Radiographic Interpretation of Dental Cariesد. شهرزاد سامي
د. شهرزاد ساميDental radiology
Dental radiology
Dental Caries
Dental caries is a unique disease affecting the hard tissues of teethThe carious process is defined as continuous phase of demineralization and remineralization of tooth surfaces with several stages, which could be reversible or irreversible.
Tooth decay or caries can be categorized depending on:
Anatomical location
Activity status
Etiology
Proximal caries
Caries found between two teeth is termed interproximal caries. On a dental image, interproximal caries is typically seen at or just below (apical to) the contact point. This area is difficult, if not impossible, to examine clinically with an explorer. As the caries progresses inward through the enamel of the tooth, it assumes a triangular configuration; the apex (or point) of the triangle is seen at the dentino-enamel junction (DEJ).
As the caries reaches the DEJ, it spreads laterally and continues into dentin. Another triangular configuration is seen in dentin; this time the base of the triangle is along the DEJ, and the apex is pointed toward the pulp chamber
Proximal caries classified according to its severity
Incipient inter proximal caries extends less than half way through the thickness of enamelModerate inter proximal caries extends more than half way through enamel


Proximal caries classified according to its severity
Advanced inter proximal caries extends to or through the dentanoenamel junction and into dentin but does not extend through the dentin more than half the distance toward the pulp (affects both enamel and dentin(Severe inter proximal caries extends through enamel and through dentin more than half distance toward the pulp (involve both enamel and dentin(
Occlusal Caries
A thorough clinically examination is the method of choices for detection of occlusal caries
Because of superimposition of dense buccal and lingual enamel cups early occlusal caries is difficult to see on a dental radiograph

Occlusal caries classified into
Incipient occlusal caries cannot be seen on a dental radiograph and must be detected clinically with dental probeModerate occlusal caries extends into dentin and appears as a very thin radiolucent line located under the enamel of the occlusal surface

Severe occlusal caries extends into dentin and appears a as large radiolucency under the enamel of occlusal surface of the tooth clinically appears as a cavitations into a tooth.
Buccal and Lingual Caries
Buccal caries involve the buccal tooth surface.
Lingual caries involve the lingual tooth surface.
Because of superimposition of the densities of normal tooth structure, they are difficult to be detected by the dental radiograph and are best detected clinically.
Radiographically these carious lesions appear as a small circular radiolucent area.
Root Surface Caries
Clinically root surface caries is easily detected on exposed root surface.The most common locations include the exposed root of the mandibular premolar and molar areas.
Radiographically the root surface caries appears as a cupped–out or crater shaped radiolucency just below the cemento-enamel junction.

Recurrent Caries
Secondary or recurrent caries occurs adjacent to a pre-existing restoration. It is occurs in this region because ofInadequate cavity preparation
Defective margins
Incomplete removal of caries prior to the placement of restoration

Rampant Caries
Advanced and severe caries that affects numerous teeth, rampant caries is seen in children with poor dietary habits or in adults with a decreased salivary flow.
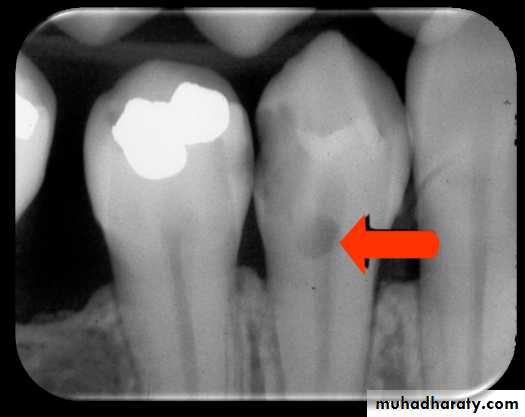
Radiolucent Cervical Burn-Out
Cervical burn-out can be explained as that the different parts of the tooth and supporting bone tissue penetrated by the same x-ray beamIn the crown-dense enamel cap and dentin
In the tooth neck-only the dentin
In the root-dentin and buccal and lingual plates of the alveolar bone.
Cervical burn out can be distinguished by the following features:
It’s located at the neck of the tooth demarcated above by the enamel cap or restoration and below by alveolar bone level.
It’s triangular in shape gradually become less apparent towards the centre of the tooth.
All the teeth on the radiograph are affected, especially in the premolars.
Radiopaque Zone beneath Amalgam Restoration
It has been shown with time, tin and zinc ions are released into the underlying demineralized dentin producing radiopaque zone which follow the S-shape of dentinal tubules. The normal dentin on either sides appear more radiolucent by contrast, this more radiolucent normal dentin may simulate the shadow of caries and lead to difficult diagnosis.

Limitations of Radiographic Diagnosis of Caries
Carious lesions are usually larger clinically than they appear radiographically and very early lesions are not evident at allTechnique variations in film and x-ray beam position can affect the image of the carious lesions (incorrect horizontal angulations make carious lesion confirm in the enamel to be progressed into dentin)
Exposure factors can affect the overall radiographic contrast and thus affect the appearance or size of carious lesion on radiograph
Superimposition and two dimensional image mean that the following features cannot always be determined:
The exact site of a carious lesion e.g. buccal or lingual
The bucco-lingual extent of a lesion
The distance between the carious lesion and pulp horn
The presence of an enamel lesion (density of the overlying enamel may obscure the zone of decalcification).
The presence of recurrent caries (existing restorations may completely overlie the carious lesion)