EMPYEMA&LUNG ABSCESS
ا.د اسامه عبيد الخفاجيM.B.Ch. B
FIBM Cardiothoracic & vascular surgey
MRCS Edn.
Empyema
accumulation of pus in the pleural space whether it is localized (encapsulated) or generalized involving the entire pleural space.Pathogenesis:
Acute or Exudative phase: Thin pus,Mobile lung(expandable),Thin pleura
Trasitional or Fibrinopurulent phase: Turbid fluid
viscus,thick pleura, Less expandable lungChronic or Organization phase: fluid is viscus,thick pleura,restricted lung
Infection of the pleural space → inflammatory changes → serous exudation → fibrin deposition on the pleural surfaces → invasion by blood vessels from adjacent lung and chest wall → granulation tissue → fibrous tissue → progressive thickening of the wall of the empyema
Secondary changes in surrounding structures as empyema continues:
Ribs drawn together & lose mobilityDiaphragm elevated and fixed
Mediastinum shifted
Lung encased in a rigid covering of fibrous tissue and is immobile and functionless
• Causes:
• 1-Pulmonary infection: Lobar pneumonia,lung abscess• 2-Trauma: Penetrating trauma,Postoperative (post-pneumonectomy ),Esophageal perforation
• 3-Extrapulmonary spread: Osteomyelitis of dorsal spine, subphrinic abscess
• 4-Aspiration of pleural effusion (done under septic technique)
• 5-Ruptured emphysematous bullae and spontaneous pneumothorax → empyema
• 6- Generalized sepsis
Microorganisms:
Most common organisms are streptococcus ,pneumococcus ,Staph aureusClinical features
constitutional symptoms of fever, malaise, tachycardia, anorexia, and weight loss in late presentation
Pleuretic chest pain and sensation of heaviness
Shortness of breath and cough with purulent sputum
On Examination: signs of infection + signs of pleural effusion
Complications:
• Invasion of the chest wall → osteomyelitis → empyema necessitans
• BPF( Bronchopleural fistula)Mediastinal abscess
• Septicemia
• Metastatic abscess
• Fibrothorax
Diagnosis:
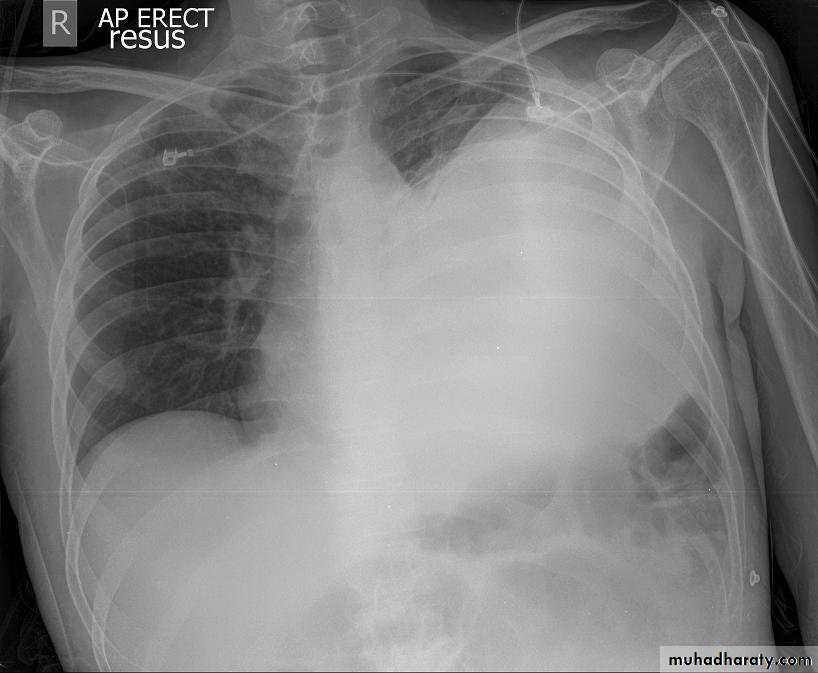
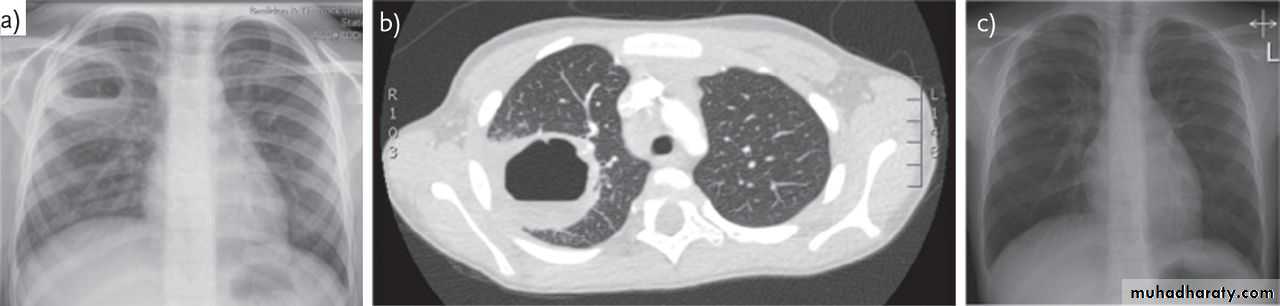
1-CXR:
PA and lateral views show effusion, air fluid level
2-Thoracocentesis and fluid analysis :
Culture and sensitivity, gram stain, pH,, glucose, protein, LDH
3-Sputum culture:
Is often helpful because organisms responsible for pneumonia are a frequent cause of empyema.
TB and fungal infection
• 4-Bronchoscopy: To exclude intrabronchial tumor or foreign body
• 5-Ultrasound
• 6-CT scan
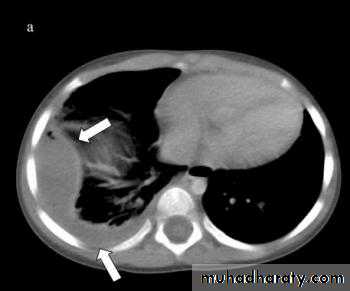
Treatment
1- Thoracocentesis : for diagnostic and therapeutic measures usualy for an early acute phase2- Tube thoracostomy : done when there is large and thick fluid
3- Image guided catheter placement with fibrinolytic agents : for those where the 2nd option failed to evacuate the pleura
4- VATS or Thoracotomy : decortications with pleurectomy
Lung Abscess
localized area of suppuration and cavitation in the lungEtiology:
1-Primary necrotizing pneumonia:Aerobic,Anaerobic
2- Aspiration pneumonia:Anesthesia,Stroke
3- Bronchial obstruction :Neoplasm,Foreign body
4-Complication of systemic sepsis 5-Complication of pulmonary trauma :Infected hematoma
6-Direct extension from extra-pulmonary infection:
Pleural empyema, subphrinic abscess
Predisposing factors :
• 1-Post-operatively• 2-Systemic illness
• 3-Malignancy (especially of lung and oropharynx)
• 4-Prolong use of corticosteroids,immunosuppressive radiotherapy or antibiotics
Clinical picture
history of upper respiratory tract infection with high fever, malaise, fatigue, and often is toxic with weight lossRecent onset of cough with copious foul smelling sputum
Chest pain
Hemoptysis
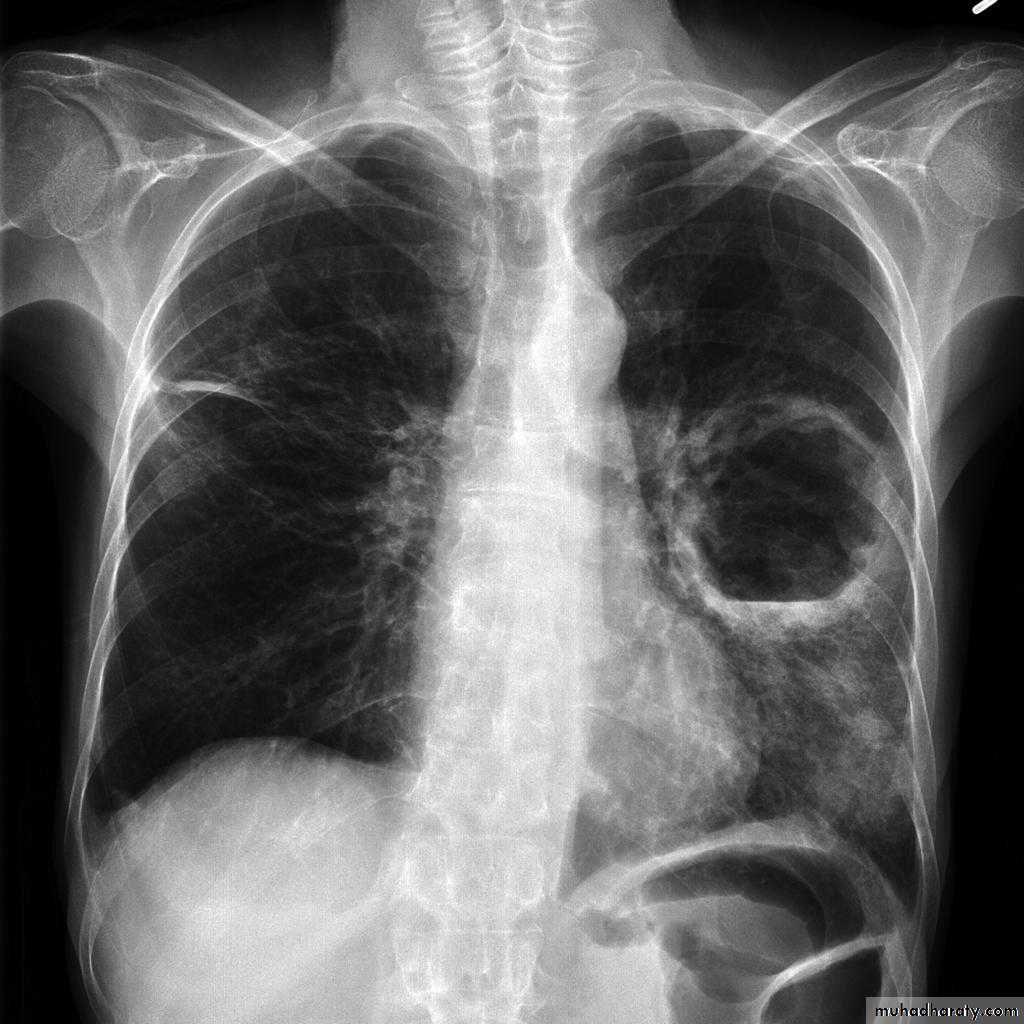
Investigations;
CXR : Air fluid level is only seen in upright film
CT san : clarify the diagnosis when the CXR is equivocal
• Bronchoscopy : To exclude or confirm Ca
• To diagnose and remove foreign bodies
• To drain an abscess
• To obtain a bronchial wash for C/S
Differential diagnosis:
1-Cavitating lung carcinoma2- Infected lung cyst or bullae
3-TB
4- Bronchiectasis
Differential diagnosis of a febrile patient with copious production of foul sputum:
Lung abscess
Bronchiectasis
Cavitating carcinoma
Treatment:
Medical :Identification of the caustic microorganism,Prolonged antimicrobial therapy Surgical :
Indications of surgical treatment:
Lack of response to medical treatment
Suspeicion of malignancy
Significant and/or recurrent hemoptysis
Complications of lung abscess : Empyema,BPF
Options of surgical treatment:
tube pneumonostomy External drainage ie.
Pulmonary resection :lobectomy,segmentectomy,wedge resection and rarely pneumonectony
Complications of lung abscess:
Massive hemoptysisEndobronchial spread to other lung portions
Septicemia
Metastatic brain abscess
Rupture into pleural cavity →
Empyema
BPF
THANKS