



Genital Ulcer
Dr. Ahmed Abdulhussein AL-Huchami

Causes:
ST causes:
Herpes genitalis
Chancre (primary syphilis)
Chancroid
Lymphogranuloma venereum (LGV)
Granuloma inguinale (Donovanosis)
Non ST causes:
Behce
t
disease
Fixed drug eruption (
t
reatment)
T
rauma
T
umor as SCC
Chronic infection as
T
B

Syphilis
Cupid
cupid :
a symbol for love in the form of a cherubic naked boy
with wings and a bow and arrow
(Roman mythology god of love)".

Mode of Transmission:
Sexual contact
Transplacentally
Blood
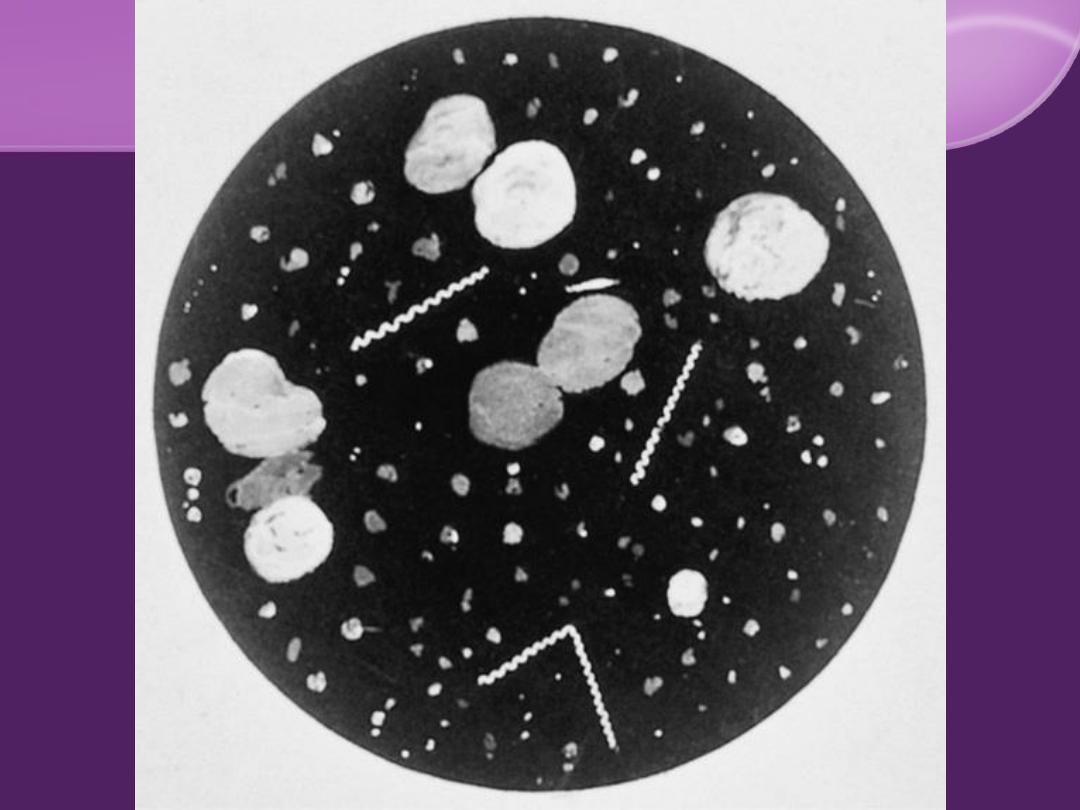
Microbiology:
T. pallidum
Spiral bacterium (spirochete)
Corkscrew rotation motility
Dark Field M
Non culturable

Classification and Stages
Congenital and Acquired.
Acquired syphilis
1- Primary
stage (chancre)
2- Secondary
stage (skin, MM, & systemic)
3- Latent
stage
(history of syphilis
+
absence of signs and
symptoms
+
positive serologic tests)
Early latent
(less than one year)
late latent
(1 year or longer).
4- Tertiary
stage (skin, MM, & visceral).
Early syphilis
(within the first 2 years, infectious).
Late syphilis
(after 2 years, less infectious).
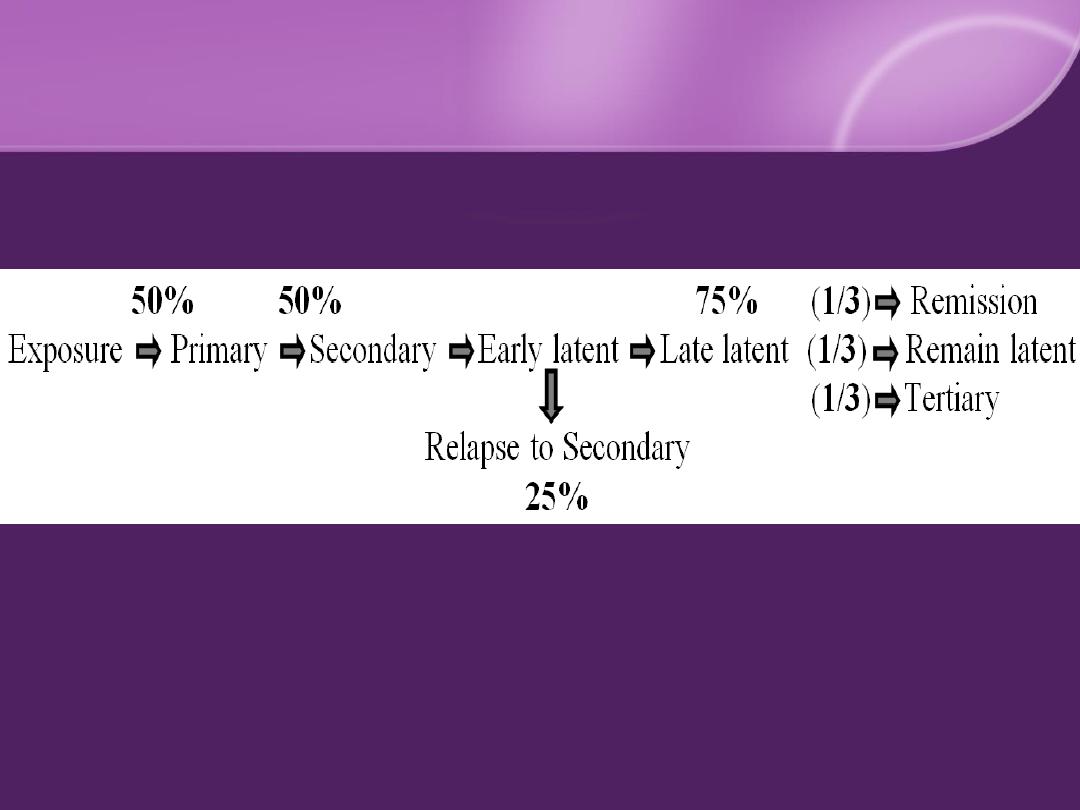
Natural Course of Syphilis

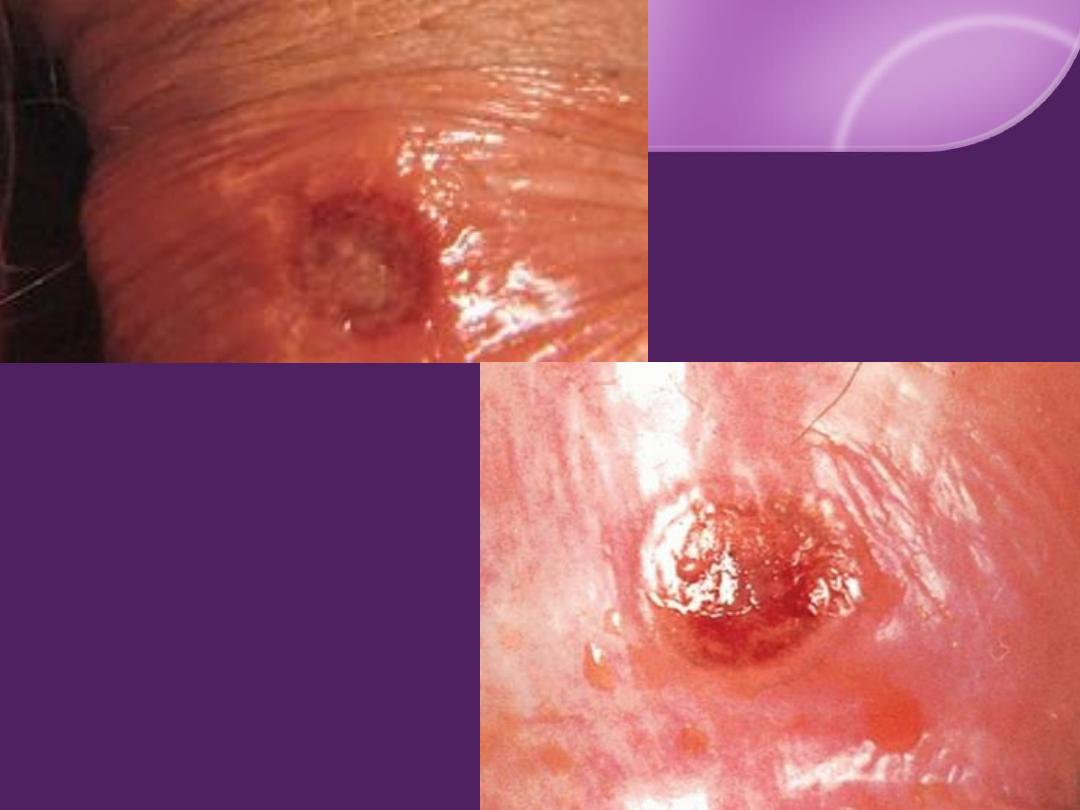
Primary Syphilis (chancre) :
The syphilitic ulcer (
chancre
)
IP: 9-90 days (3 weeks in
50%
)
Solitary
,
painless
,
hard
,
clean base (
50%
)
Painless, hard, discrete regional LN.
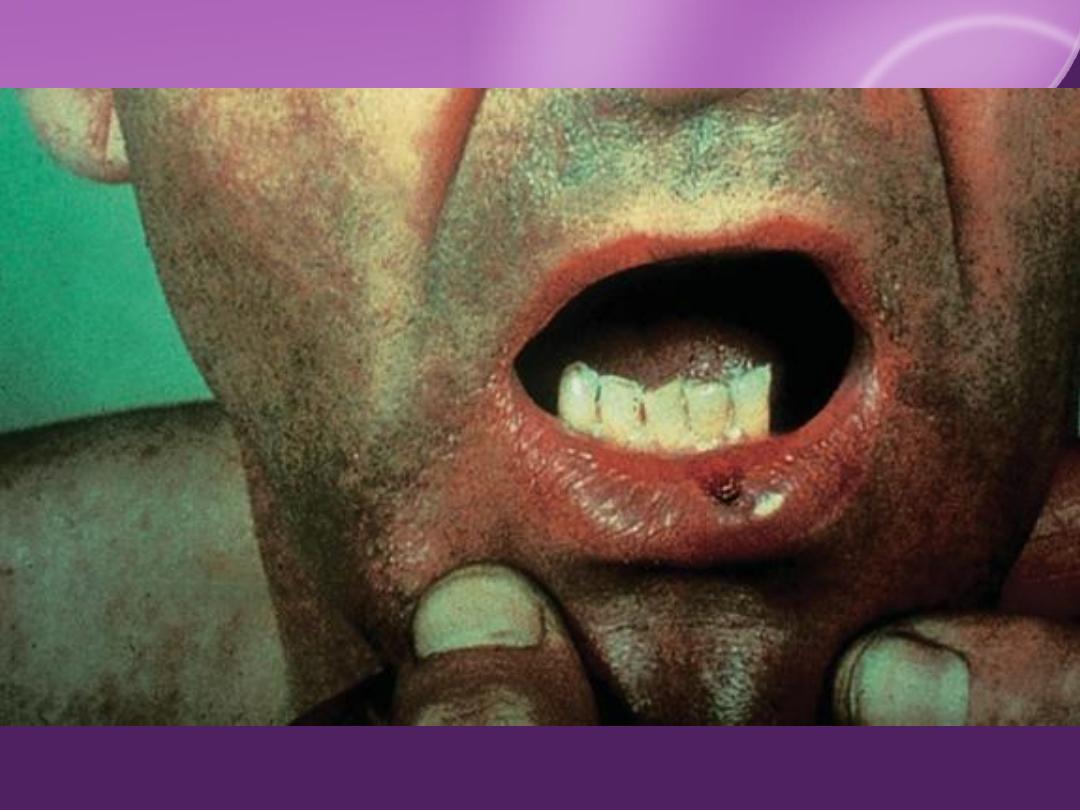

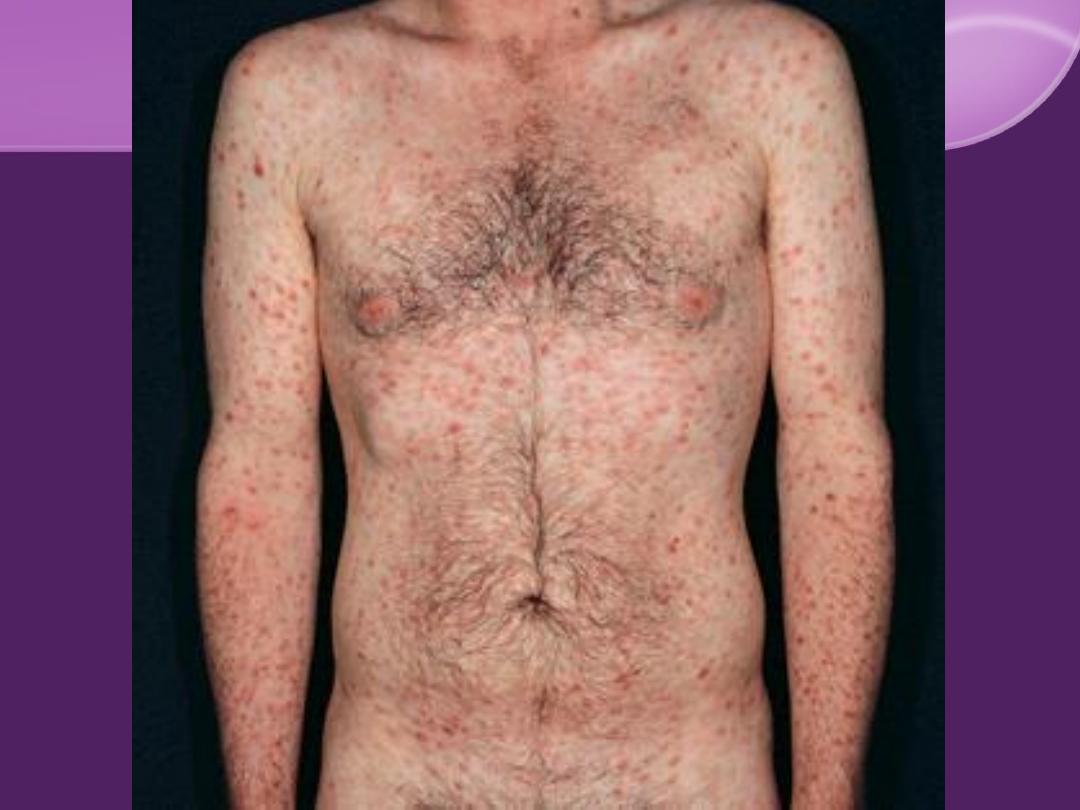
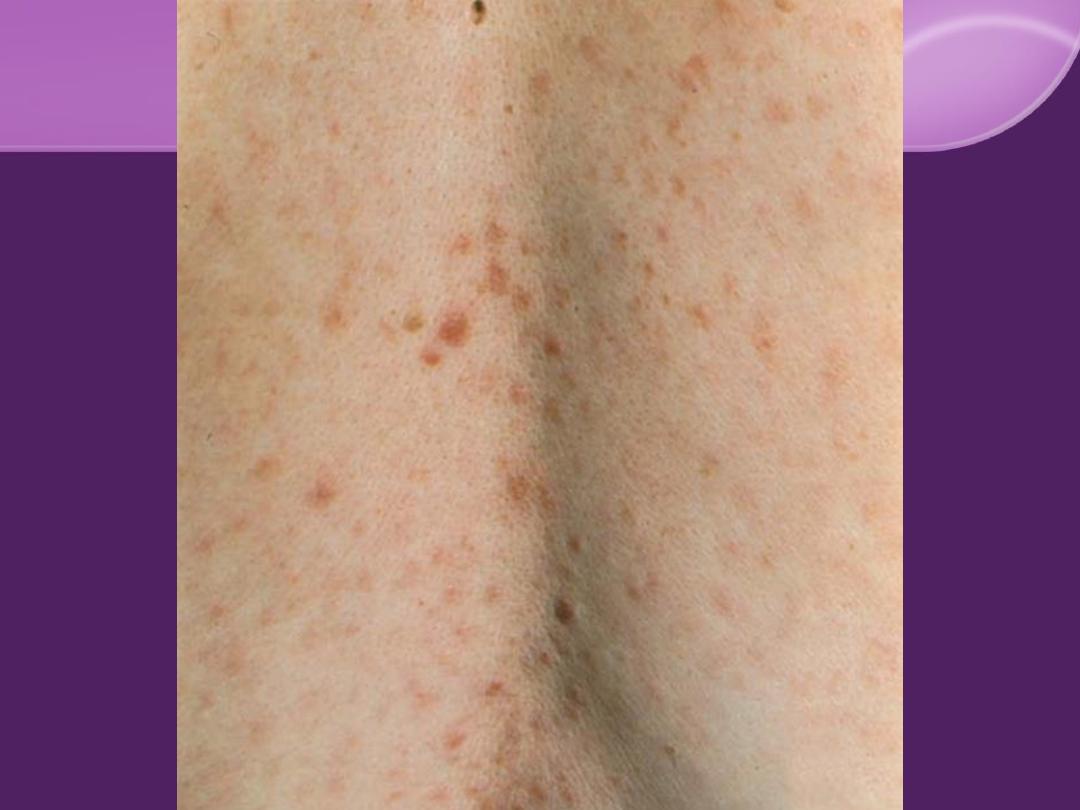
Secondary Syphilis:
Cutaneous Findings:
Flulike symptom and generalized painless
LN in 50%
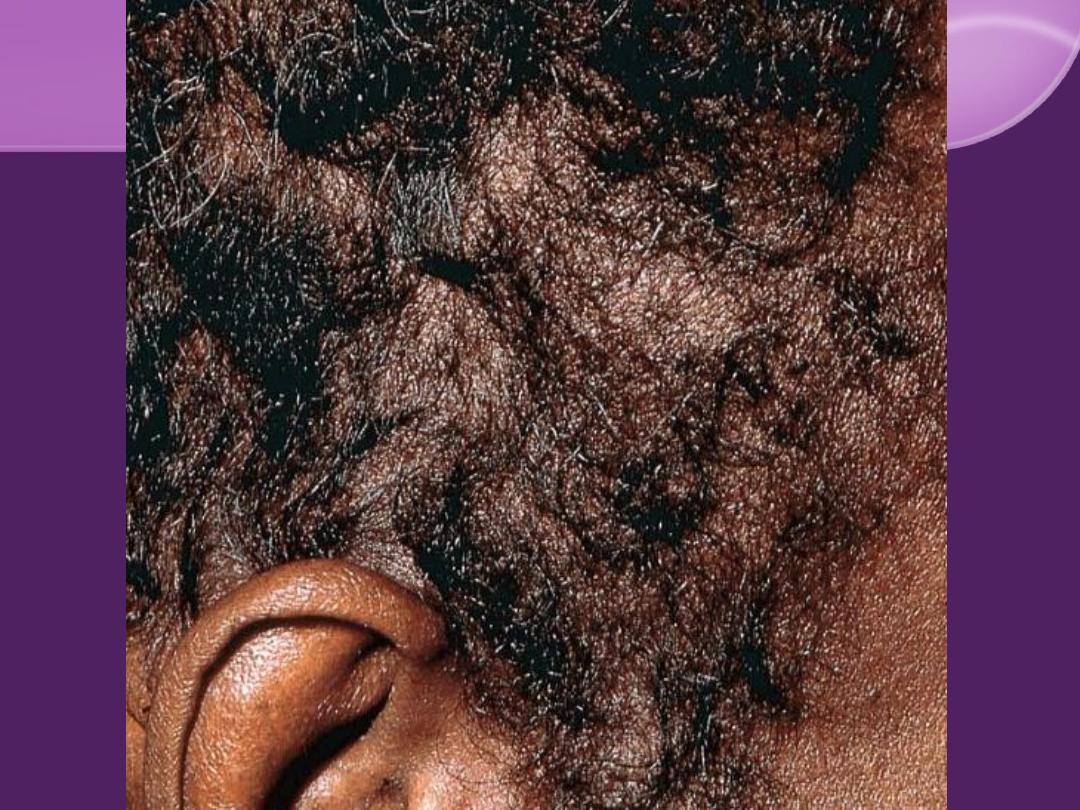
"Moth eaten" alopecia
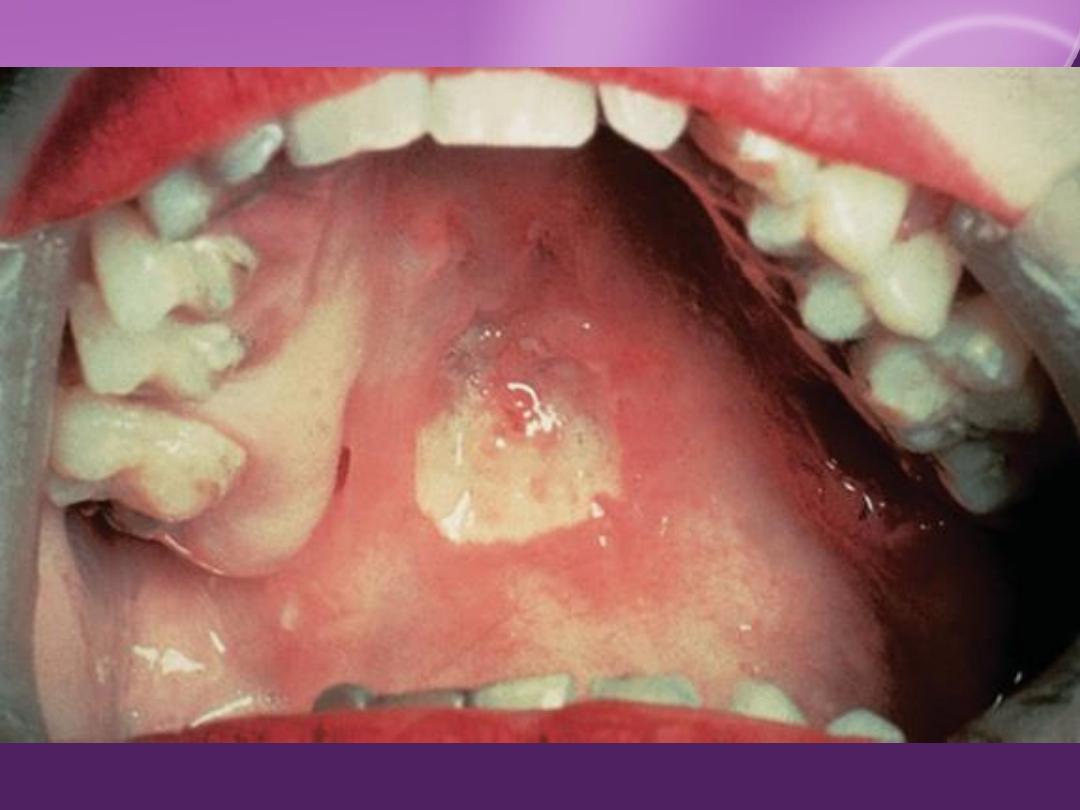
MM involvement
Extremely infectious
Genital (codylomata lata)
Oral, pharyngeal, laryngeal.
Systemic findings

DDX of Secondary Syphilis:
Great Imitator
Skin eruption
: pityriasis rosea, guttate
psoriasis, lichen planus, pityriasis versicolor,
drug eruptions, and viral eruptions.
Condylomata lata
Oral lesions
Alopecia "Moth eaten"





1.
Little or no fever at onset.
2.
Pain or itching is minimum or absent.
3.
Lesions are non inflammatory, develop
slowly.
4.
Marked tendency to polymorphism.
5.
Bilateral symmetrical, with characteristic
palms and soles involvement.
6.
The color is characteristic, resembling a
"clean-cut ham" (coppery tint).



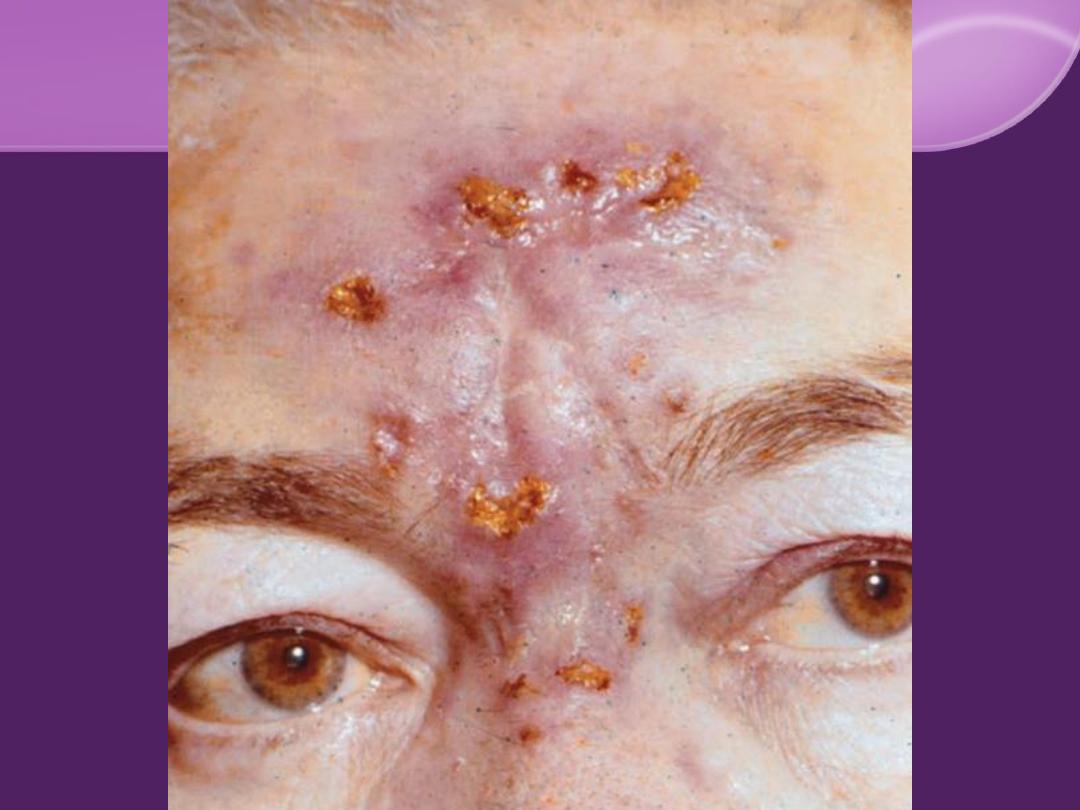
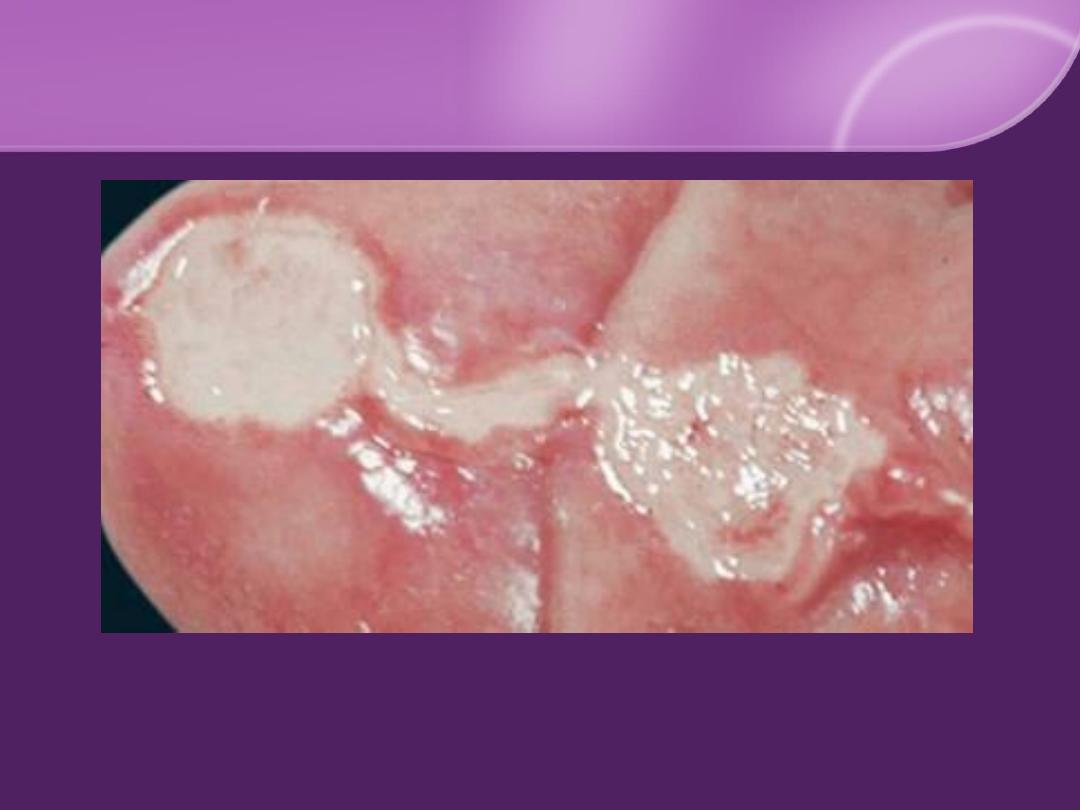
Tertiary Syphilis:
Cutaneous Lesions:
In opposite to the secondary syphilis;
few
,
few MO,
asymmetrical, slowly growing, destructive and heals
with scar.
1. Nodular and noduloulcerative lesions
2. Gummas (a form of granuloma)
Predilections sites
MM Lesions:
palate, nasal mucosa, tongue, tonsils, and pharynx
(
saddle nose
) are the disease hallmark.
Oral leukoplakia
50%
Visceral:
cardiovascular syphilis and neurosyphilis





Congenital Syphilis:
Early syphilis
Late pregnancy
25%
of infants die in utero.
75%
one-half
develop the disease.
one-forth
only seropositive.
one-forth
not infected.
Early congenital
Late congenital

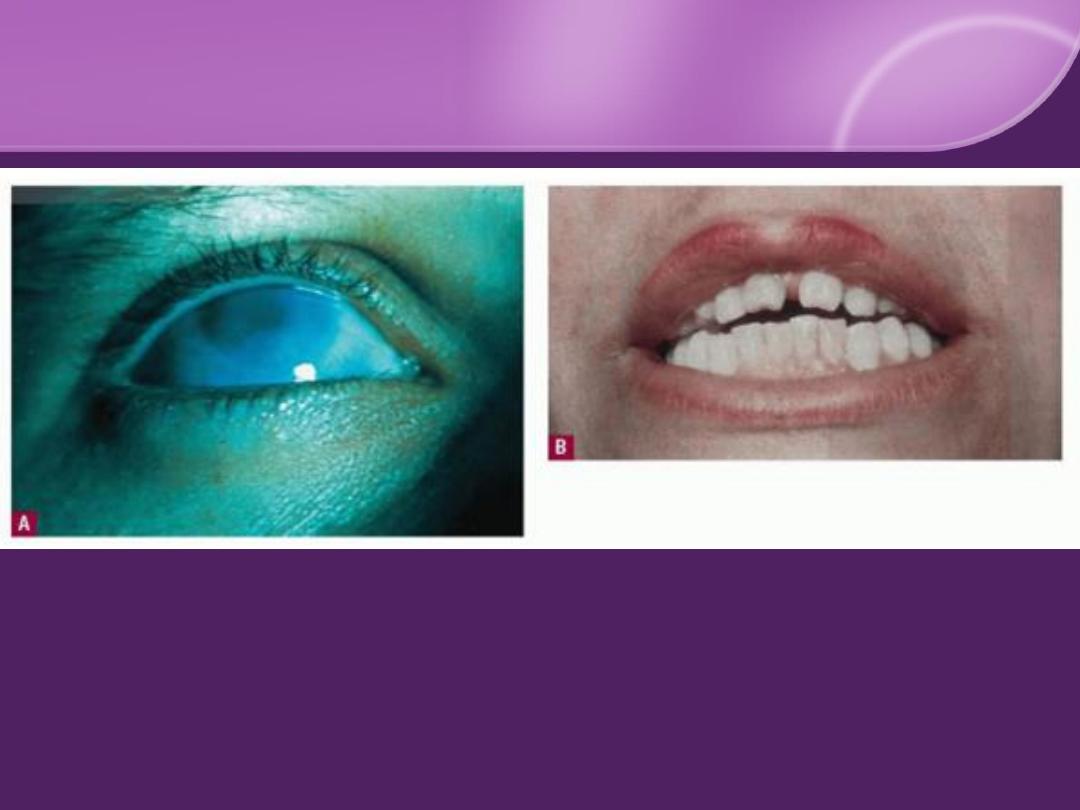
Stigmata of Congenital Syphilis
1. Ophthalmic: corneal clouding.
2. Oral: Hutchinson teeth and high-arched palate.
3. Nose: saddle nose.
4. Orthopedic: frontal bossing, saber shin, and
thickened medial clavicle.
5. Neurologic: 8
th
cranial nerve palsy.
6. Positive serology for syphilis.


Diagnosis of Syphilis:
1. History and examination.
2. Dark-field microscopy
3. Serological tests.
4. PCR.
5. Biopsy: rarely needed.

Syphilis Serology
A- Non-Specific (Lipoidal or Non Treponemal)
VDRL
RPR
.
These tests become positive 3-6 weeks after infection
(after 3 weeks in
50%
).
Remain strongly positive in the secondary phase, and
become negative after treatment ..
monitor
&
follow up.
They are used for
screening
purposes.
These tests give quantitative as well as qualitative
results, so all reactive samples are
titrated
to determine
the highest reactive dilution.
When these tests are positive, verification should be
done by the specific tests.

B- Specific (Treponemal) Tests:
TPHA
FTA/ABS
TPI
RPCF
become positive earlier than the non specific.
can not be used to assess response to treatment.
They are not used for screening purposes.
These tests cannot be titrated.

False Reactions:
False-positive reactions
False-negative reaction:
Prozone phenomenon

Treatment of Syphilis:
Penicillin
Early syphilis
: 2.4 MU BP G IM single
Late syphilis
: 2.4 MU BP G IM / W 3 times
Congenital syphilis
: CP for 10-14 days
Sexual partner
No proven alternatives to penicillin in:
1-
Neurosyphilis
2-
Congenital syphilis
3-
HIV infected patient
4-
Pregnant patient

Jarisch-Herxheimer Reaction:
a complex allergic response to antigens released
from dead microorganism can complicate the
treatment of syphilis

Follow Up : VDRL
Early syphilis
:
every 3 months in the 1
st
year,
every 6 months in the 2
nd
year,
yearly thereafter.
Late syphilis
: yearly.
Neurosyphilis
: every 6 months

Signs of Relapse:
Clinical
Serological (4 fold increase)
Transplacental infection
Infection of the partner

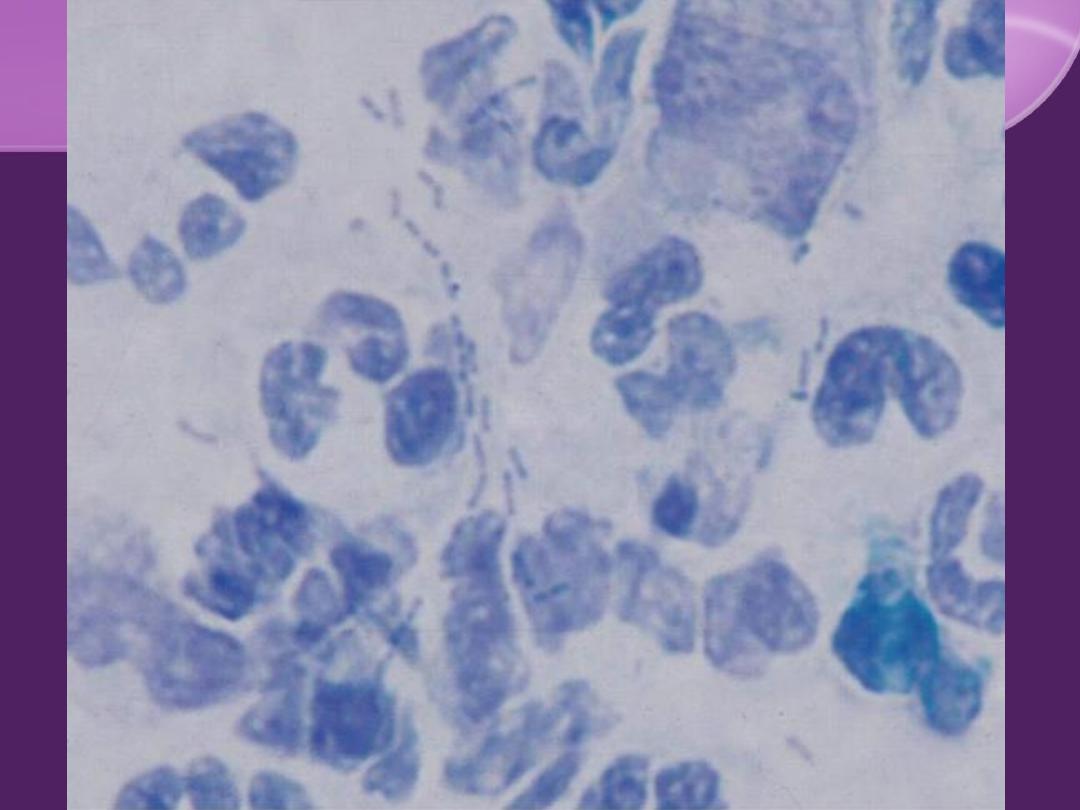
Chancroid

Rare in Iraq.
haemophilus ducreyi.
Clinical Features:
Ulcer:
in reverse to chancre ;
Multiple, painful
,
tender
,
soft
,
purulent base,
with
short IP
(3-5 days).
painful inguinal
LN
& may matted.
Investigation:
Smear: "school-of-fish" pattern.
Culture.

THANK YOU