Fifth Stage
E.N.T
Dr.Mushtaq – Lecture 18
1
Nasal Allergy
Allergy : an abnormal reaction of the tissues to certain substances ‘allergens’
‘antigens’ capable of making the body produce antibodies.
In allergic subjects, a special form of antibody (IgE,) is produced. These antibodies
easily fix on tissue cells, including those of the nasal and bronchial mucosa or the
skin.
Aetiology
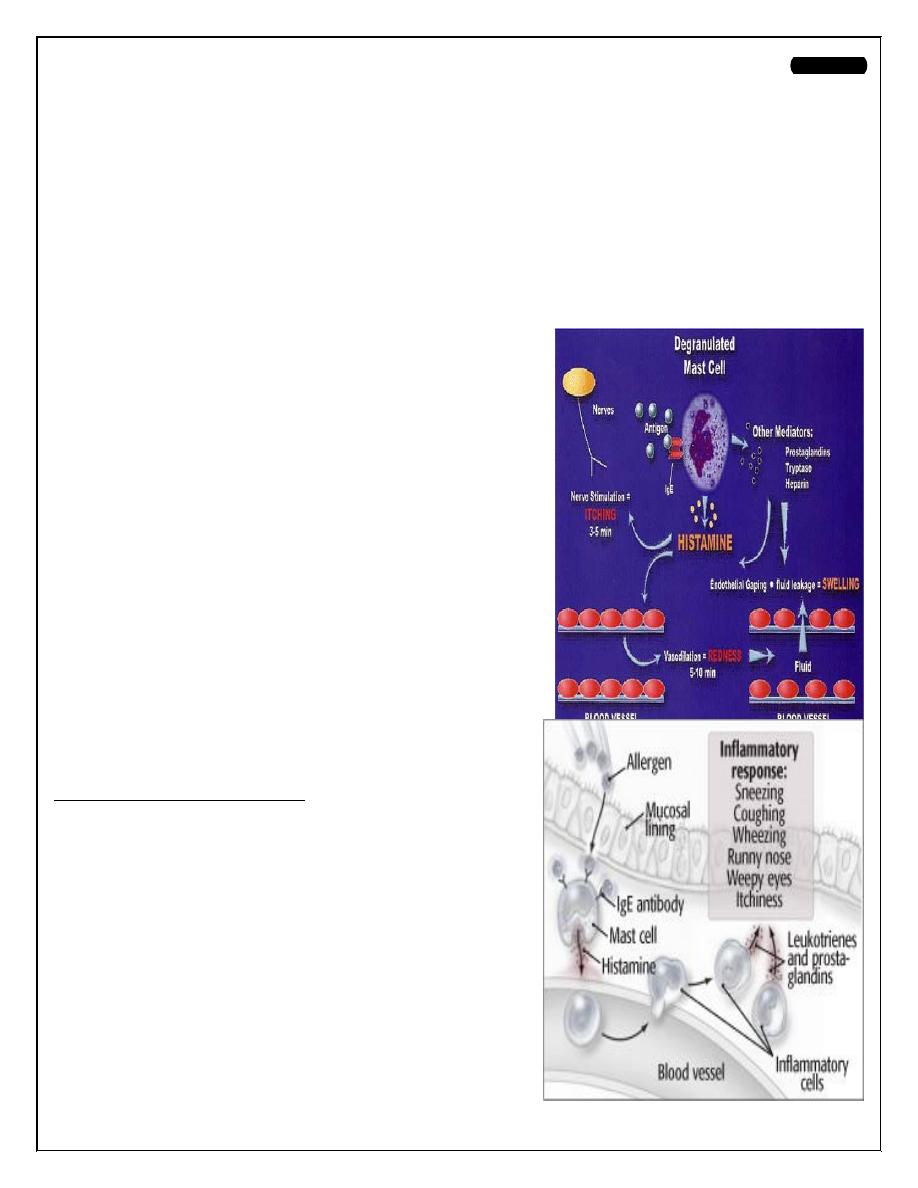
Mechanism of allergy (3phases):
1. IgE
(formed by lymphocytes in response to
allergen exposure).
2. IgE is bound
to mast and basophil cells
,
initiates
the secretion of substances such as histamine that
lead to the clinical manifestations.
3. Capillaries become permeable
,
and
oedema
occurs.
Eosinophils infiltrate
the tissues.
Serous
alveolar glands are stimulated
either directly or via
an autonomic reflex to produce excess
watery
secretion.
Predisposing factors
hereditary
.. ‘
Atopy’=inherited tendency
.
Precipitating factors
1. Exogenous
.
a.Inhalants:
,:
dusts,pollens,animal,feathers,fungal spores and
the house-dust mite
b.Ingestants;
(foods): especially in children
such as eggs, strawberries, nuts or fish .Milk or
wheat are less obvious.
c. contacts
to skin or nasal mucosa
;. Face
powders, and hair from electric razors, nasal
drops or sprays .
2
d. Drugs
; nasal symptoms may be part of a more generalized allergic response.
e. Infection
: bacterial ,fungi and parasites allergy has been suspected but never
proved.
2. Endogenous
; tissue proteins from injured tissues, transudates and exudates
) ..
Clinical types
1.Seasonal ('hay-fever': pollinosis).
2.Non-seasonal (perennial).
Age incidence
less common after 50 years of age.
Signs and Symptoms
• Sneezing
• Earache
• Itchy nose, ears, eyes and palate
•Tearing of eyes
• Red eyes
• Rhinorrhea
• Swollen eyes
Physical Examination
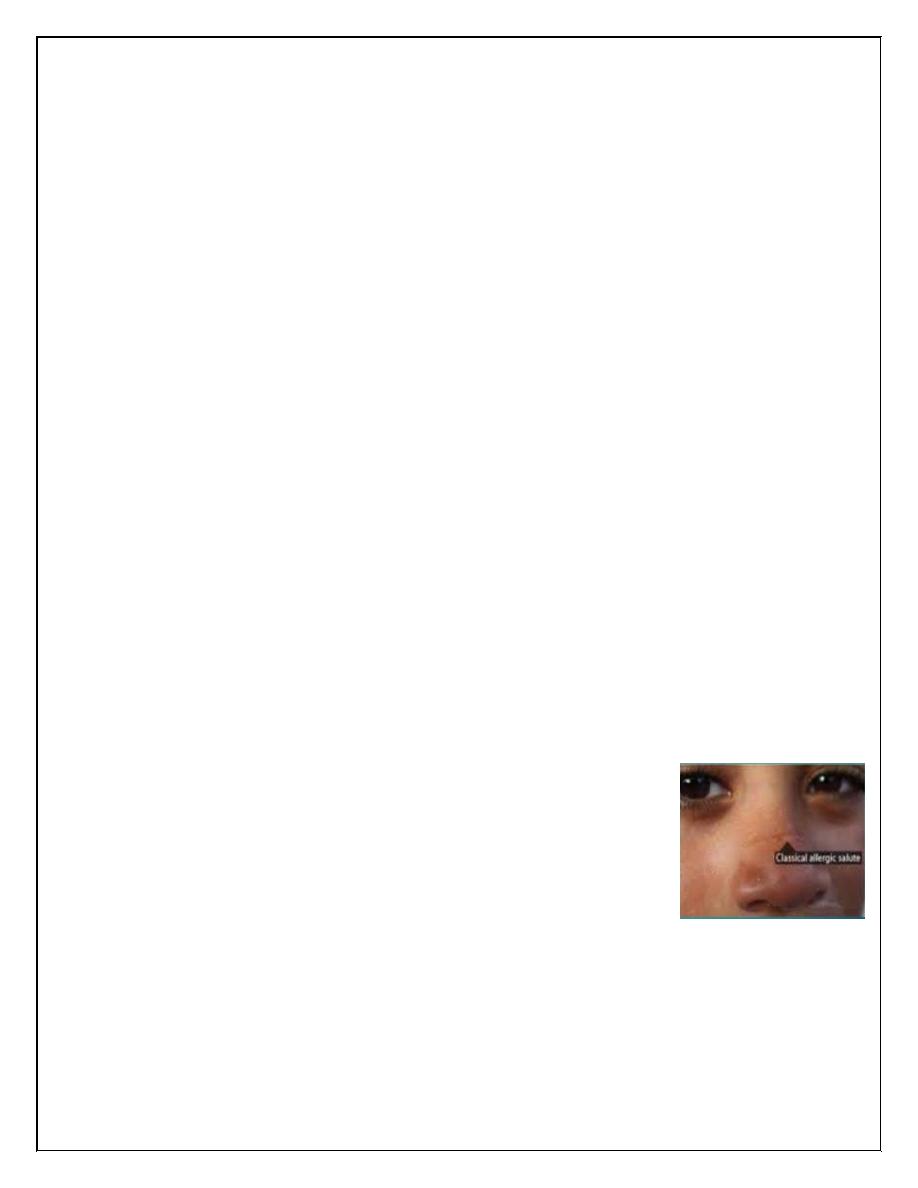
• Nasal crease
Horizontal crease across the lower half of the bridge of the
nose
• Rhinorrhoea
Thin Watery secretions
• Deviated or perforated nasal septum
• Post nasal drip
• Fatigue
• Congestion
• Drowsiness
• Anosmia
• Malaise
• Headache
3
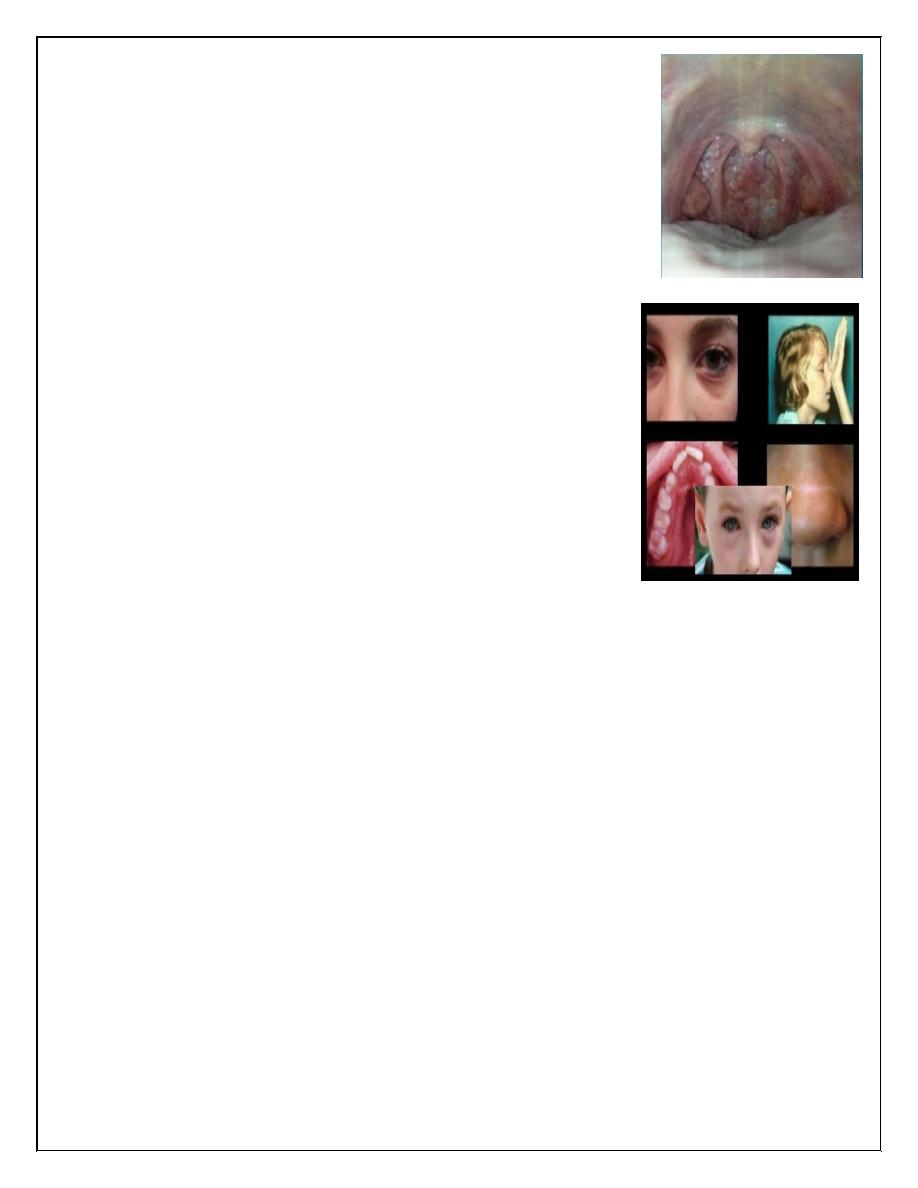
Extra Nasal Manifestation
• Retracted and abnormal flexibility of TM
• Injection and swelling of palpebral conjunctivae with excess
tearing.
• Cobblestoning on oropharynx
Classical Signs of AR
• Over bite
• High arched palate
• Allergic shiners
• Allergic salute
• Transverse crease over tip of nose and lower eye lid
• Conjunctival congestion
• Periorbital oedema
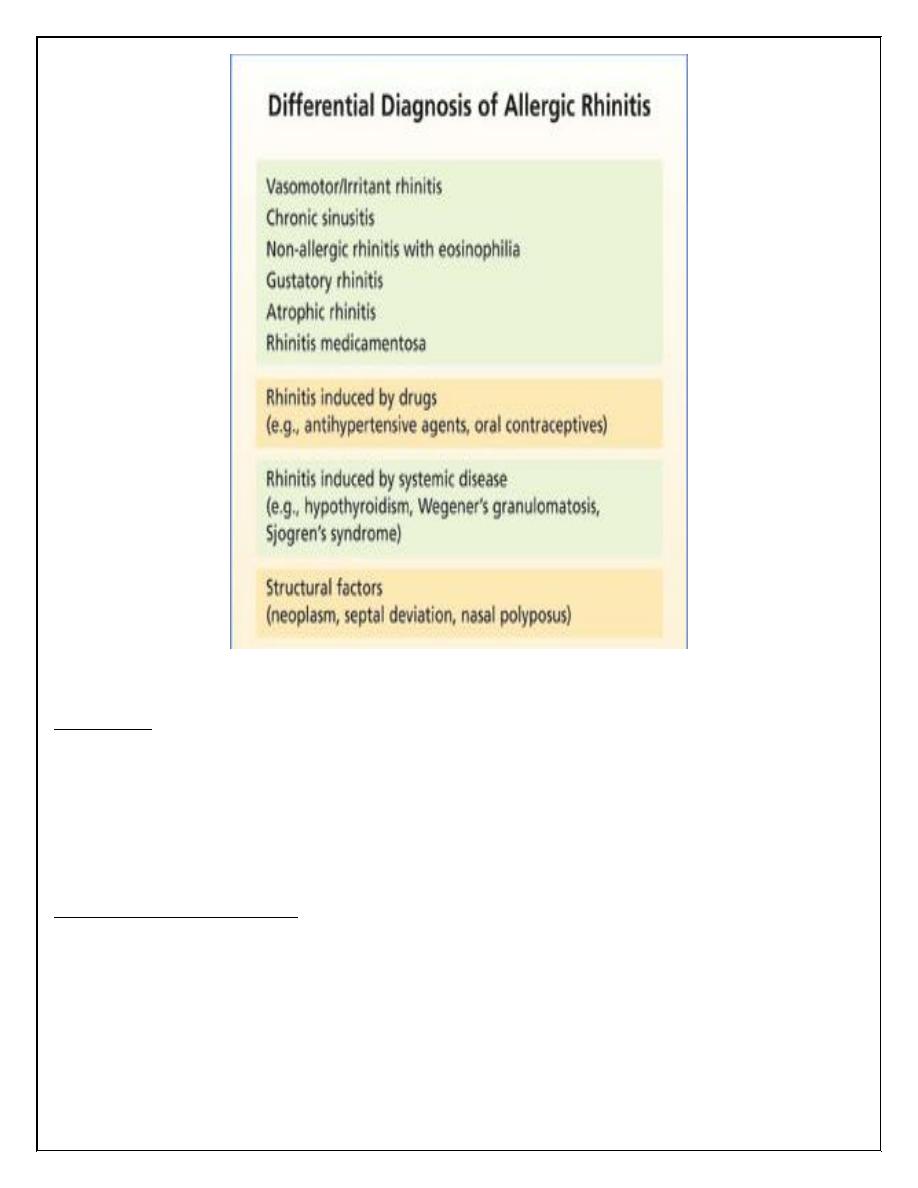
Diagnosis
1.Careful history.
2.Clinical examination..
3. Eosinophils. May be found in great numbers in the nasal secretions ,the nasal
mucosa or polypi. The eosinophil count of the blood is raised, especially in the
morning, and always in the presence of an extrinsic allergen.
4. Skin tests. These are confirmatory. Sensitivity is less than 50% of cases clinically
suggestive of a non-seasonal allergy. Nearly all patients with seasonal symptoms will
give positive responses.
5. intranasal test. A drop of test solution may promote rhinorrhea and sometimes
lacrimation - so-called 'nasal provocation' test.
6. Elimination test. may be helpful, especially in suspected food allergies.
4
Management (Avoidance, Medical, Surgical)
Avoidance
• Minimize contact with offending allergens
• Reduce dust mite exposure by encasing bed pillows and matress in allergen
proof covering
• Use of allergen proof bedding…
Acute Phase medications:
• Antihistamines effectively block histamine effects (runny nose and watery
eyes)
• Side effects : sedation, dry mouth, nausea, dizziness, blurred vision,
nervousness
• Non sedating antihistamines (cetrizine, Ioratidinelr
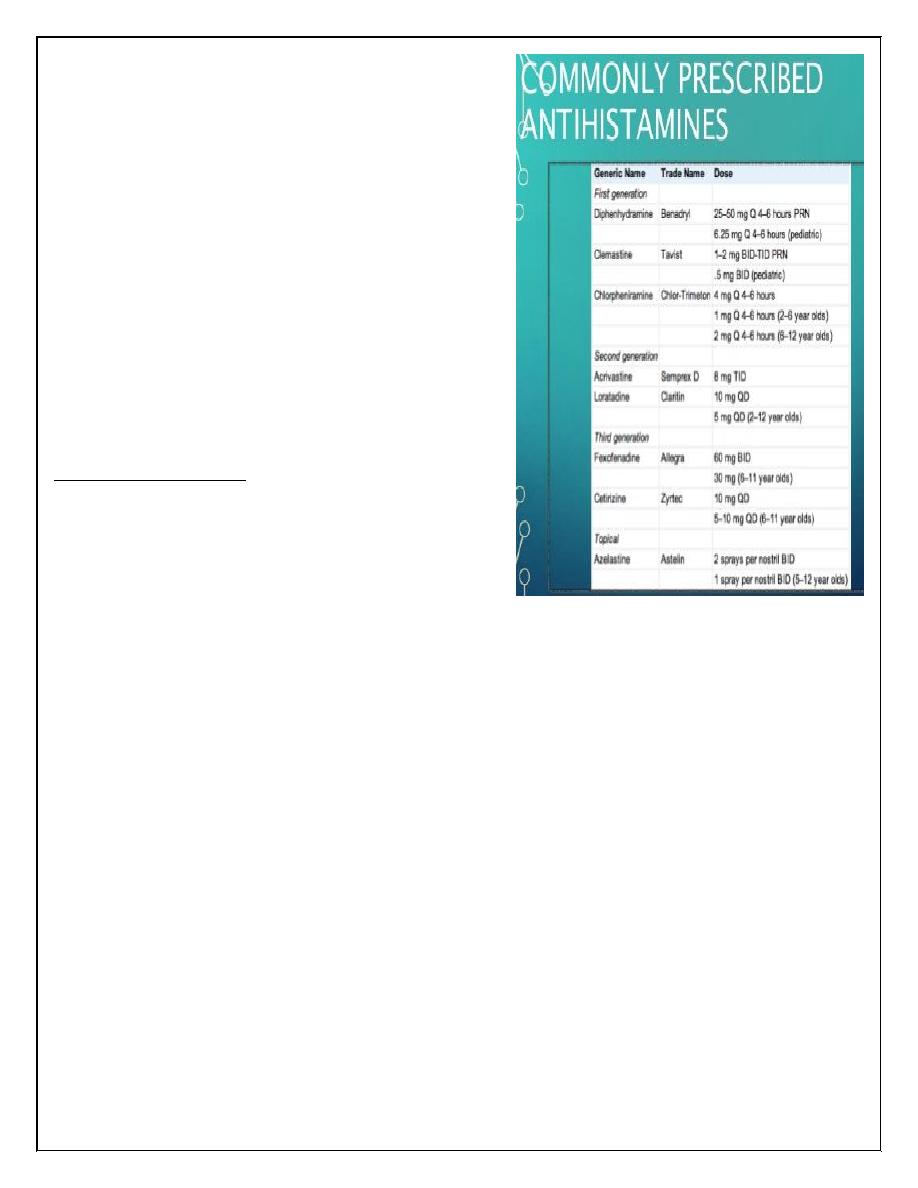
5
• Fewer side effects .
• Fexofenadine may be effective _
• Carries a lower risk of cardiac
arrythmias
• Decongestants
• Anticholinergenic agents
• inhibit mucous secretions, act as
drying agent
• Topical eye preparations
• Reduce inflammation and relieve
itching and burning, -
Prevention Therapy:
• Intranasal corticosteroids
• Reduce inflammation of mucosa
• Prevent mediator release
• Can be used safely daily
• May be given systemically for a short course during disabling attack.
• Intranasal cromolyn sodium
• Mast cell stabilizer
• Prevent release of chemical mediators
• Oral Mast cell stabilizer
• Ophthalmic solution cromolyn
• Leukotriene receptor antagonists
• Montelukast (singulair) and Zatirlukast (accolate)
• Systemic agents used for asthma
• Reduce inflammation, edema and mucous secretions of allergic rhinitis
6
Immunotherapy
• lf allergic rhinitis is refractory to pharmacotherapy or severe
• Helps in reducing the specific serum IgE level
• decreases the basophil sensitivity .
• increases IgG blocking antibody level, thus preventing allergen from
reaching mast cells and subsequent mast cell degranulation.
Surgical Therapy
•Limited
• Submucosal turbinectomy - reduces size of boggy turbinates
• Septoplasty - correction of deviation of septum
• Sinus surgery – clearance of sinuses if sinusitis is present.
Complications
• Allergic asthma
• Chronic otitis media
• Hearing loss
• Chronic nasal obstruction.
• Sinusitis
• Orthodontic malocclusion in children.
Thank you,,,