The pancreas
Dr. Ali Jaffer AlghazzawiDAdvSurg (GI)
CABS
MBChB

Anatomy
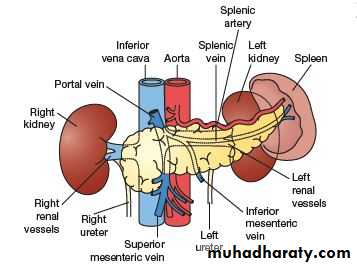
The pancreas is situated in the retroperitoneum.Head occupies 30% of the gland by mass.
Body and tail together constitute 70%.
The head lies within the curve of the duodenum, overlying the body L2 and the IVC.
The aorta and the superior mesenteric
vessels lie behind the neck of the gland.
Coming off the side of the pancreatic
head and passing to the left and behind
the superior mesenteric vein is
the uncinate process of the pancreas.
Behind the neck of the pancreas,
near its upper border, the superior
mesenteric vein joins the splenic vein
to form the portal vein.
The tip of the pancreatic tail
extends up to the splenic hilum.
Anatomy
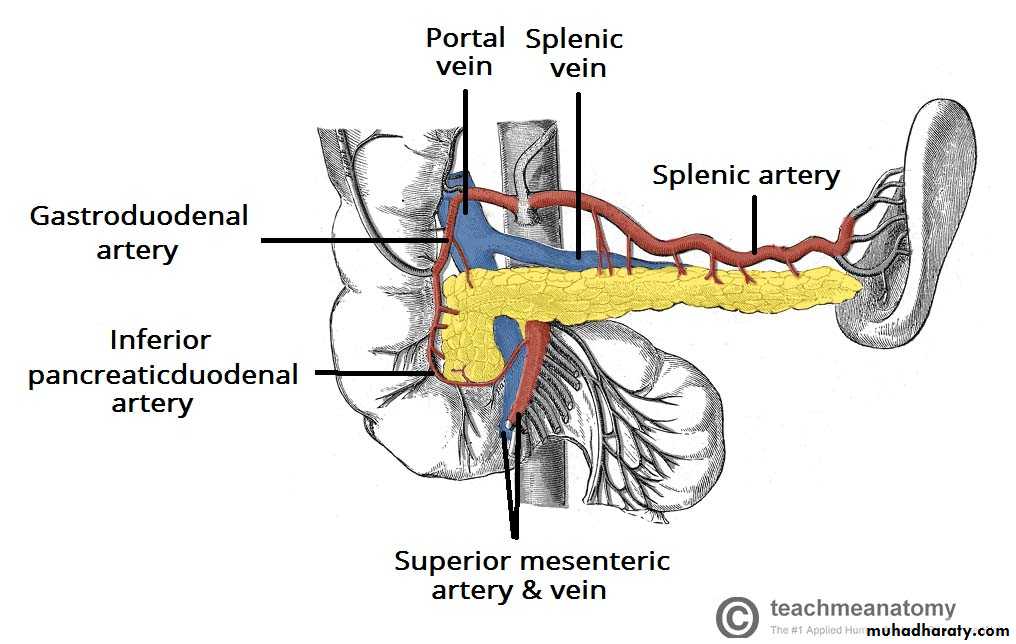
VasculatureArteries:
Splenic a., superior pancreaticoduodenal a
, inferior pancreaticoduodenal a.
Veins:
Splenic vein, superior mesenteric veinLympahatics:
The pancreas is drained by lymphaticvessels that follow the arterial supply.
They empty into the pancreaticosplenal
nodes and the pyloric nodes, which in
turn drain into the superior mesenteric and
coeliac lymph nodes.
INVESTIGATIONS
Estimation of pancreatic enzymes in body fluidsserum amylase, lipase
Pancreatic function tests
The nitroblue tetrazolium–para-aminobenzoic acid (NBT–PABA)
The pancreolauryl test
Faecal elastase
Imaging investigations
Ultrasonography
Ultrasonography is the initial investigation of choice in patients with jaundice
i. The bile duct is dilated or not.
ii. The coexistence of gallstones or gross disease within the liver such as metastases.
iii. It defines the presence or absence of a mass in the pancreas .
limitation: obesity and overlying bowel gas often make interpretation of the pancreas itself unsatisfactory.
b. Computed tomography
c. Magnetic resonance imaging
Magnetic resonance cholangiography and pancreatography (MRCP) may well replace diagnostic endoscopic cholangiography and pancreatography (ERCP) as it is non-invasive and less expensive
Invstigation
d. Endoscopic retrograde cholangiopancreatography
ERCP is performed using a side-viewing fibreoptic duodenoscope. The ampulla of Vater is intubated, and contrast is injected into the biliary and pancreatic ducts to display the anatomy radiologically.
Diagnostic and theraputic
e. Endoscopic ultrasound
* To identifying small tumours that may not show up well on CT or MRI.* To demonstrate the relationship of a pancreatic tumour to major vessels nearby.
* Transduodenal or transgastric fine needle aspiration (FNA) or Trucut biopsy performed under EUS guidance avoids spillage of tumour cells into the peritoneal cavity.
CONGENITAL ABNORMALITIES
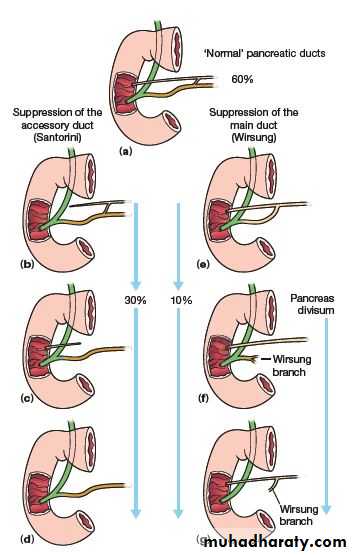
Pancreas divisum* The embryological ventral and dorsal parts of the pancreas fail to fuse.
* The dorsal pancreatic duct becomes the main pancreatic duct and drains most of the pancreas through the minor or accessory papilla.
* The incidence 5% -10% .
* Pancreas divisum found incidentally in an asymptomatic person does not warrant any intervention.* The incidence of pancreas divisum ranges from 25–50% in patients with recurrent acute pancreatitis, chronic pancreatitis and pancreatic pain. *The minor papilla is substantially smaller than the major papilla .
* A large volume of secretions flowing through a narrow papilla probably leads to incomplete drainage, which may then cause obstructive pain or pancreatitis.
* Idiopathic recurrent pancreatitis, pancreas divisum should be excluded.
The diagnosis can be arrived at by MRCP, EUS or ERCP, augmented by injection of secretin .Endoscopic sphincterotomy and stenting of the minor papilla may relieve the symptoms.
Surgical intervention.....sphincteroplasty, pancreatojejunostomy or even resection of the pancreatic head.
CONGENITAL ABNORMALITIES
Annular pancreasThis is the result of failure of complete rotation of the ventral pancreatic bud during development, so that a ring of pancreatic tissue surrounds the second or third part of the duodenum.
It is most often seen in association with congenital duodenal stenosis or atresia and is therefore more prevalent in children with Down syndrome.
Treatment is bypass (duodenoduodenostomy).
The disease may occur in later life as one of the causes of pancreatitis.
Ectopic pancreas
Islands of ectopic pancreatic tissue can be found in the submucosa in parts of the stomach, duodenum or small intestine (including Meckel’s diverticulum), the gall bladder, adjoining the pancreas, in the hilum of the spleen and within the liver.Ectopic pancreas may also be found in the wall of an alimentary tract duplication cyst.
INJURIES TO THE PANCREAS
External injuryPresentation and management
The pancreas protected location in the retroperitoneum, is not frequently damaged in blunt abdominal trauma.
If there is damage to the pancreas, it is often concomitant with injuries to other viscera, especially the liver, the spleen and the duodenum.
Pancreatic injuries may range from a contusion or laceration of the parenchyma without duct disruption to major parenchymal destruction with duct disruption (sometimes complete transection) and, rarely, massive destruction of the pancreatic head.
Blunt pancreatic trauma usually presents with epigastric Pain with the progressive development of more severe pain due to the sequelae of leakage of pancreatic fluid into the surrounding tissues.
A rise in serum amylase occurs in most cases.
A CT scan of the pancreas will delineate the damage that has occurred to the pancreas.
If there is doubt about duct disruption, an urgent ERCP should be sought. MRCP may be helpful.
INJURIES TO THE PANCREAS
Support with intravenous fluids and a ‘nil by mouth’ regimen should be instituted while these investigations are performed.
It is preferable to manage conservatively at first, investigate and, once the extent of the damage has been ascertained, undertake appropriate action.
Operation is indicated if there is disruption of the main pancreatic duct; in almost all other cases, the patient will recover with conservative management.
Penetrating trauma to the upper abdomen or the back carries a higher chance of pancreatic injury.
In penetrating injuries, especially if other organs are injured and the patient’s condition is unstable, there is a greater need to perform an urgent surgical exploration.
Sequlae
Death, in acute phase as a result of bleeding from associated injuries.Persistent drain output in 1/3 of patients
Duct stricture resulting in recurrent episodes of pancreatitis.
Pancreatic pseudocyst.
INJURIES TO THE PANCREAS
Iatrogenic injuryThis can occur in several ways:
● Injury to the tail of the pancreas during splenectomy, resulting in a pancreatic fistula.
● Injury to the pancreatic head and the accessory pancreatic duct (Santorini), which is the main duct in 7% of patients, during Billroth II gastrectomy
● Enucleation of islet cell tumours of the pancreas can result in fistulae.
● Duodenal or ampullary bleeding following sphincterotomy.
Pancreatic fistula
Management of pancreatic fistulae
Tests
● Measure amylase level in fluid
● Determine the anatomy of the fistula
● Check if the main pancreatic duct is blocked or disrupted
Measures
● Correct fluid and electrolyte imbalances
● Protect the skin
● Drain adequately
● Parenteral or nasojejunal feeding
● Octreotide to suppress secretion
● Relieve pancreatic duct obstruction if possible (ERCP andstent)
● Treat underlying cause
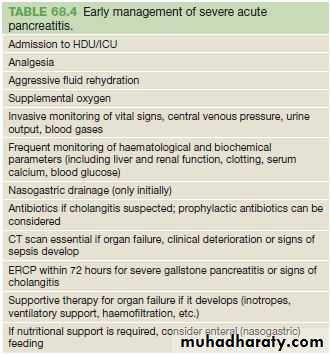
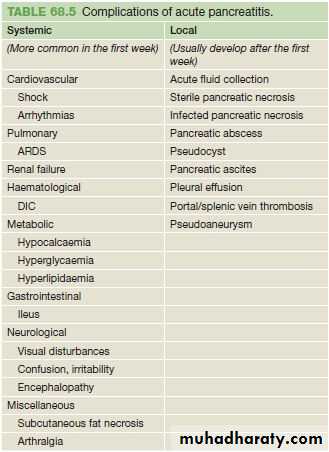
Acute pancreatitis
The mechanism of injury is thought to be premature activation of pancreatic enzymes within the pancreas, leading to a process of autodigestion.The inflammatory process can lead to pancreatic oedema, haemorrhage and, eventually, necrosis.
As inflammatory mediators are released into the circulation, systemic complications can arise, such as haemodynamic instability, bacteraemia (due to translocation of gut flora), acute respiratory distress syndrome and pleural effusions, gastrointestinal haemorrhage, renal failure and disseminated intravascular coagulation (DIC).
The majority of patients will have a mild attack of pancreatitis, the mortality from which is around 1%.
Severe acute pancreatitis 5–10% of patients, and is characterised by pancreatic necrosis, a severe systemic inflammatory response and often multi-organ failure.
Severe attack of pancreatitis, the mortality 20 - 50%.
Acute pancreatitis has an early phase that usually lasts a week. It is characterised by a systemic inflammatory response syndrome (SIRS) which – if severe – can lead to transient or persistent organ failure (deemed persistent if it lasts for over 48 hours).
About one-third of deaths occur in the early phase of the attack, from multiple organ failure.
The late phase is seen typically in those who suffer a severe attack, and can run from weeks to months. It is characterised by persistent systemic signs of inflammation, and/or local complications, particularly fluid collections and peripancreatic sepsis.
Deaths occurring after the first week of onset are often due to septic complications.
Acute pancreatitis
Possible causes of acute pancreatitis
● Gallstones
● Alcoholism 50-70%
● Post ERCP 1-3 %
● Abdominal trauma
● Following biliary, upper gastrointestinal or cardiothoracic surgery
● Ampullary tumour
● Drugs (corticosteroids, azathioprine, asparaginase, valproic acid, thiazides, oestrogens)
● Hyperparathyroidism
● Hypercalcaemia
● Pancreas divisum
● Autoimmune pancreatitis
● Hereditary pancreatitis
● Viral infections (mumps, coxsackie B)
● Malnutrition
● Scorpion bite
● Idiopathic
Acute pancreatitis
Clinical presentationPain develops quickly, reaching maximum intensity within minutes and persists for hours or even days. It is severe, constant and refractory to the usual doses of analgesics. epigastrium but may be localised to either upper quadrant or felt diffusely throughout the abdomen. There is radiation to the back in about 50% of patients, and some patients may gain relief by sitting or leaning forwards.
Nausea, repeated vomiting and retching. The retching may persist despite the stomach being kept empty by nasogastric aspiration. Hiccoughs may be due to gastric distension or irritation of the diaphragm.
On examination, the patient may be well or gravely ill.
Tachypnoea , tachycardia is usual, and hypotension .
The body temperature is often normal or even subnormal
Mild icterus can be caused by biliary obstruction in gallstone pancreatitis.
Bleeding into the fascial planes can produce bluish discolouration of the flanks (Grey Turner’s sign) or umbilicus (Cullen’s sign). Neither sign is pathognomonic of acute pancreatitis; Cullen’s sign was first described in association with rupture of an ectopic pregnancy.
Subcutaneous fat necrosis may produce small, red, tender nodules on the skin of the legs.
Abdominal examination may reveal distension due to ileus.
There is usually muscle guarding in the upper abdomen.
A pleural effusion is present in 10–20% of patients.
Pulmonary oedema and pneumonitis
Acute pancreatitis
Investigations
A serum amylase level three times above normal
serum levels lipase
contrast- enhanced CT.
ASSESSMENT OF SEVERITY
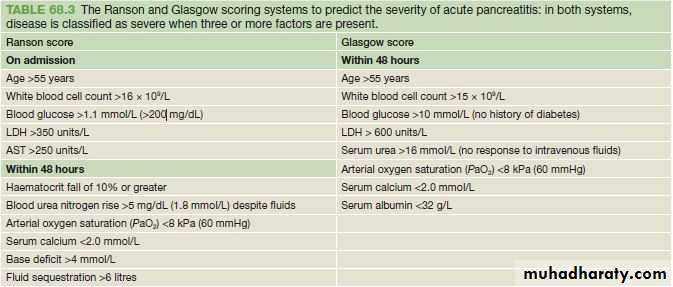
Severity stratification assessments should be performed in patients at 24 hours, 48 hours and 7 days after admission.The Ranson and Glasgow scoring systems are specific for acute pancreatitis, and a score of 3 or more at 48 hours indicates a severe attack
Regardless of the system used, persisting organ failure indicates a severe attack. A serum C-reactive protein level >150 mg/L at 48 hours after the onset of symptoms is also an indicator of severity.
Mild acute pancreatitis:
no organ failure;
no local or systemic complications.
Moderately severe acute pancreatitis:
organ failure that resolves within 48 hours (transient organ failure); and/or
local or systemic complications without persistent organ failure.
Severe acute pancreatitis:
persistent organ failure (>48 hours);
single organ failure;
multiple organ failure.
Acute pancreatitis
ASSESSMENT OF SEVERITY
Acute pancreatitis
Acute pancreatitis
Acute pancreatitis
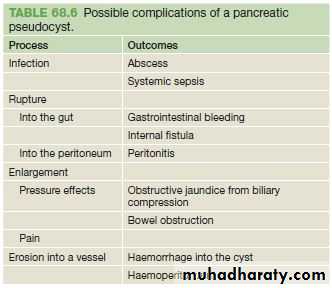
PSEUDOCYSTIt is a collection of amylase-rich fluid enclosed in a well-defined wall of fibrous or granulation tissue. Formation of a pseudocyst requires 4 weeks or more from the onset of acute pancreatitis.
It is usually identified on ultrasound or a CT scan.
EUS and aspiration of the cyst fluid. The fluid should be sent for measurement of carcinoembryonic antigen (CEA) levels, amylase levels and cytology.
Fluid from a pseudocyst typically has a low CEA level, and levels above 400 ng/mL are suggestive of a mucinous neoplasm.
Pseudocyst fluid usually has a high amylase level, but that is not diagnostic, as a tumour that communicates with the duct system may yield similar findings.
Cytology typically reveals inflammatory cells in pseudocyst fluid.
Pseudocysts will resolve spontaneously in most instances,
but complications can develop .
Pseudocysts that are thick-walled or large (over 6 cm in diameter), have lasted for a long time (over 12 weeks), or have arisen in the context of chronic pancreatitis are less likely to resolve spontaneously.
Therapeutic interventions are advised only if the pseudocyst causes symptoms, if complications develop, or if a distinction has to be made between a pseudocyst and a tumour.
Acute pancreatitis
PSEUDOCYST
Percutaneous drainage to the exterior under radiological guidance should be avoided. It carries a very high likelihood of recurrence.It is not advisable unless one is absolutely certain that the cyst is not neoplastic and that it has no communication with the pancreatic duct (or else a pancreaticocutaneous fistula will develop).
Endoscopic drainage usually involves puncture of the cyst through the stomach or duodenal wall under EUS guidance, and placement of a tube drain with one end in the cyst cavity and the other end in the gastric lumen.
Surgical drainage involves internally draining the cyst into the gastric or jejunal lumen
Acute pancreatitis
STERILE AND INFECTED PANCREATIC NECROSISRefers to a diffuse or focal area of non-viable parenchyma.
Acute necrotic collection (ANC). This is typically an intra or extrapancreatic collection containing fluid and necrotic material, with no definable wall.Gradually, over a period of over 4 weeks, this may develop a well-defined inflammatory capsule, and evolve into what is termed walled-off necrosis (WON).
Collections associated with necrotising pancreatitis are sterile to begin with but often become subsequently infected, probably due to translocation of gut bacteria.
Infected necrosis is associated with a mortality rate of up to 50%.
Sterile necrotic material should not be drained or interfered with. But if the patient shows signs of sepsis, then one should determine whether the collection is infected
Dx: aspiration under Ct scan guidance. (the needle should never pass through hollow viscera)
Rx: if the aspirated is purulent, the patient should be kept on antibiotics according to sensitivity and drain inserted for drainage. The drain should be with larger size when the aspirate is thick content.
if sepsis persist this need pancreatic necrosectomy
Patients with peripancreatic sepsis are ill for long periods of time, and may require management in an intensive care unit. Nutritional support is essential. The parenteral and nasojejunal approaches are more popular (on the assumption that they rest the pancreas).
Chronic pancreatitis
Chronic pancreatitis is a progressive inflammatory disease in which there is irreversible destruction of pancreatic tissue. Its clinical course is characterised by severe pain and, in the later stages, exocrine and endocrine pancreatic insufficiency.
Aetiology and pathology
Alcoholism 60-70%
Duct obstruction due to trauma, acute pancreatitis or pancreatic cancer
Congenital anomalies
Hereditary pancreatitis
Cystic fibrosis
Hyperlipidemia
Hypercalcemia
Autoimmune pancreatistis (IgG4 phenomena)
Idioathic
*** At the onset of the disease, the pancreas may appear normal. Later, the pancreas enlarges and becomes hard as a result of fibrosis. The ducts become distorted and dilated with areas of both stricture formation and ectasia. Calcified stones form within the ducts. The ducts may become occluded with a gelatinous proteinaceous fluid and debris, and inflammatory cysts may form. Histologically, the lesions affect the lobules, producing ductular metaplasia and atrophy of acini, hyperplasia of duct epithelium and interlobular fibrosis.
Chronic pancreatitis
Clinical featuresPain; the site of the pain is depend on the site of the disease. Head of pancreas; the pain felt in the epigastric and right subcostal region, whereas if the disease is limited to the body and tail, the pain felt in the left subcostal region and back.
Nausea is common, vomiting may develop.
Weight loss
The patient’s lifestyle is gradually destroyed by pain, analgesic dependence, weight loss and inability to work.
Loss of exocrine function leads to steatorrhoea in more than 30% of patients with chronic pancreatitis.
Loss of endocrine function and the development of diabetes
Infection
Chronic pancreatitis
Investigations
Only in the early stages of the disease will there be a rise in serum amylase.Tests of pancreatic function merely confirm the presence of pancreatic insufficiency or that more than 70% of the gland has been destroyed.
Pancreatic calcifications may be seen on abdominal X-ray
CT or MRI scan will show the outline of the gland, the main area of damage and the possibilities for surgical correction, An MRCP will identify the presence of biliary obstruction and the state of the pancreatic duct
ERCP is the most accurate way of elucidating the anatomy of the duct
EUS
Chronic pancreatitis
Medical treatment of chronic pancreatitisTreat the addiction
Stop alcohol consumption and tobacco smoking
Involve a dependency counsellor or a psychologist
Alleviate abdominal pain
Eliminate obstructive factors (duodenum, bile duct, pancreatic duct)
Escalate analgesia in a stepwise fashion
Refer to a pain management specialist
For intractable pain, consider CT/EUS-guided coeliac axis block
Nutritional and pharmacological measures
Diet: low in fat and high in protein and carbohydrates
Pancreatic enzyme supplementation with meals
Correct malabsorption of the fat-soluble vitamins and vitaminB12
Micronutrient therapy with methionine, vitamins C & E, selenium (may reduce pain and slow disease progression)
Steroids (only in autoimmune pancreatitis, for relief of symptoms)
Medium-chain triglycerides in patients with severe fat malabsorption (they are directly absorbed by the small intestine without the need for digestion)
Reducing gastric secretions may help
Treat diabetes mellitus
Chronic pancreatitis
Endoscopic, radiological or surgical interventions are indicated mainly to relieve obstruction of the pancreatic duct, bile duct or the duodenum, or in dealing with complications (e.g. pseudocyst, abscess, fistula, ascites or variceal haemorrhage).
Prognosis
Chronic pancreatitis is a difficult condition to manage. Patients often suffer a gradual decline in their professional, social and personal lives.
The pain may abate after a surgical or percutaneous intervention, but tends to return over a period of time.
In a proportion of patients, the inflammation may gradually burn out over a period of years, with disappearance of the pain, leaving only the exocrine and endocrine insufficiencies.
Development of pancreatic cancer is a risk in those who have had the disease for more than 20 years.
New symptoms or a change in the pattern of symptoms should be investigated and malignancy excluded.
CARCINOMA OF THE PANCREAS
Risk factors for the development of pancreatic cancer.Demographic factors
Age (peak incidence 65–75 years)Male gender
Black ethnicity
Environment/lifestyle
Cigarette smokingGenetic factors /medical conditions
Family historyGermline BRCA2 mutations in some rare high-risk families
Hereditary pancreatitis (50- to 70-fold increased risk)
Chronic pancreatitis (5- to 15-fold increased risk)
Lynch syndrome (HNPCC)
Ataxia telangiectasia
Peutz–Jeghers syndrome
Familial breast–ovarian cancer syndrome
Familial atypical multiple mole melanoma
Familial adenomatous polyposis – risk of ampullary/duodenal carcinoma
Diabetes mellitus
CARCINOMA OF THE PANCREAS
Pathology of pancreatic tumours
85% ductal adenocarcinomaIntense desmoplastic reaction (extensive fibrosis), difficult to differentiate from ch pancreatitis
Spread; locally… nerve sheath, blood vessels and lymphatic
liver and peritoneal spread
Cystic tumours ; serous and mucinous
Serous : benign, old female, small and multiple
Mucinous : potential for malignant transformation
it is either Mucinous cystic neoplasm (MCNs)
or intraductal papillary mucinous neoplasms (IPMNs)
Adenomas of ampulla of Vater; premalignant lesion, may harbour invasive adenocarcinoma, it is common in patients with FAP, need endoscopic surveillance
Ampullary adenocarcinoma
Ampullary neuroendocrine tumours
CARCINOMA OF THE PANCREAS
Clinical featuresPainless jaundice, pruritus, dark urine, pale stool, steatorrhoea
Vague symptoms, weight loss , poor appitite
Recent onset DM over 50 with non specific symptms
Attacks of pancreatitis
Body and tail of pancreas tumours usually preset late as a big tumour with backache
Examination; jaundice, weight loss, palpable liver and gall bladder, Courvoisier sign, sings of advance disease (acites, supraclavicular LN, pelvic metastasis …etc)
Investigation
blood test; abnormal liver function test, anemia, tumour markers CA19-9
Ultrasound; dilated CBD, pancreatic mass liver metastasis, peritoneal mass
Contrast enhanced CT scan; site of tumour, relation to the arteries vein, duodenum, stomach, bowel, peritoneum lymphnodes
MRI
ERCP; mainly therapeutic ( stenting)
EUS, tissue to confirm the Dx (ch. Pancreatitis, Mucinous tumours)
Diagnostic laparoscopy
CARCINOMA OF THE PANCREAS
Management85% unrespectable at time of diagnosis palliative treatment
Operable surgical resection
1. head of pancreas and periampullary tumours: pancreaticoduodenectomy – whipple’s operation ( resection of gastric antrum, duodenum, head of pancreas, CBD& gall bladder) or pylorus preserving pancreaticodudenectomy
2. body and tail of pancreas ; distal pancreatectomy and splenectomy
3. total pancreatectomy; a multifocal tumour (e.g. a main duct IPMN), or the body and tail of the gland are too inflamed or too friable to achieve a safe anastomosis with the bowel.
CARCINOMA OF THE PANCREAS
Palliation of pancreatic cancerRelieve jaundice and treat biliary sepsis
Surgical biliary bypass
Stent placed at ERCP or percutaneous transhepaticcholangiography
Improve gastric emptying
Surgical gastroenterostomy
Duodenal stent
Pain relief
Stepwise escalation of analgesia
Coeliac plexus block
Transthoracic splanchnicectomy
Symptom relief and quality of life
Encourage normal activities
Enzyme replacement for steatorrhoea
Treat diabetes
Consider chemotherapy
Questions
