Patent Ductus Arteriosus
Normally, the ductus arteriosus closes before the 4th week of lifeFailure of closure of the ductus is more common in females

1
PDA: Pathophysiology
Pressure gradient between the aorta & PA occurs throughout the cardiac cycleThis leads to continuous flow of blood from the aorta to PA
2
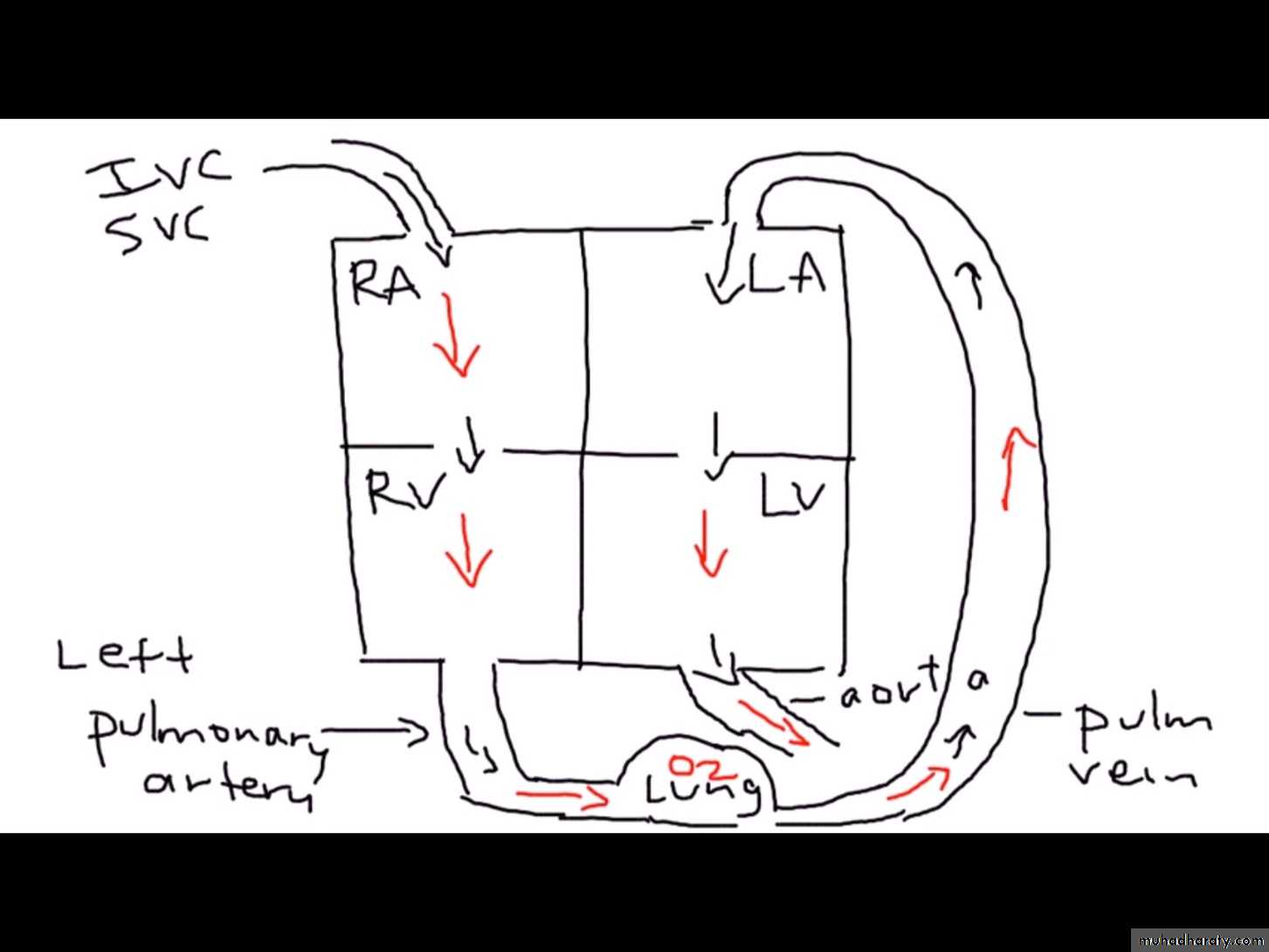
Adult life
3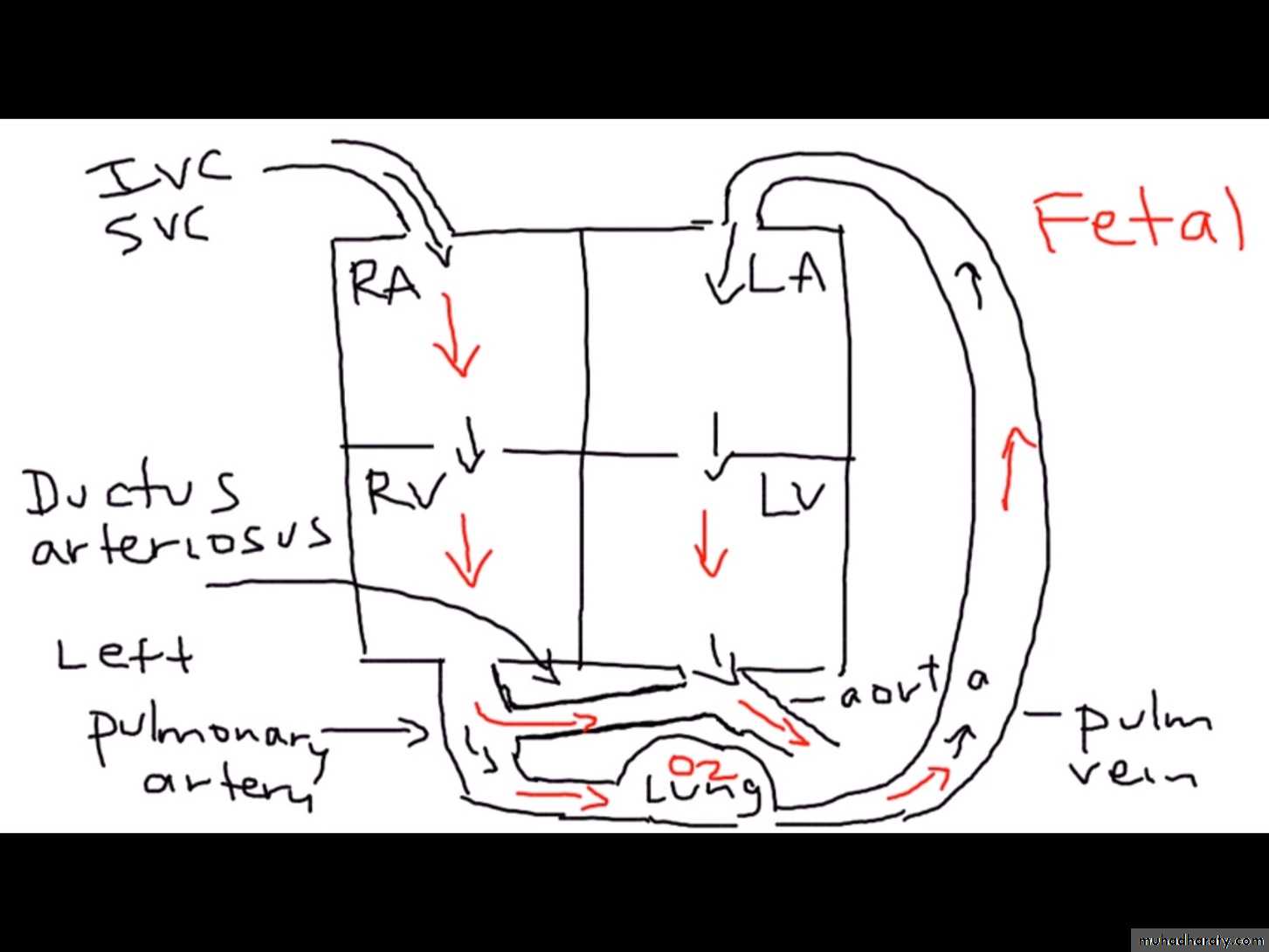
Fetal Life
4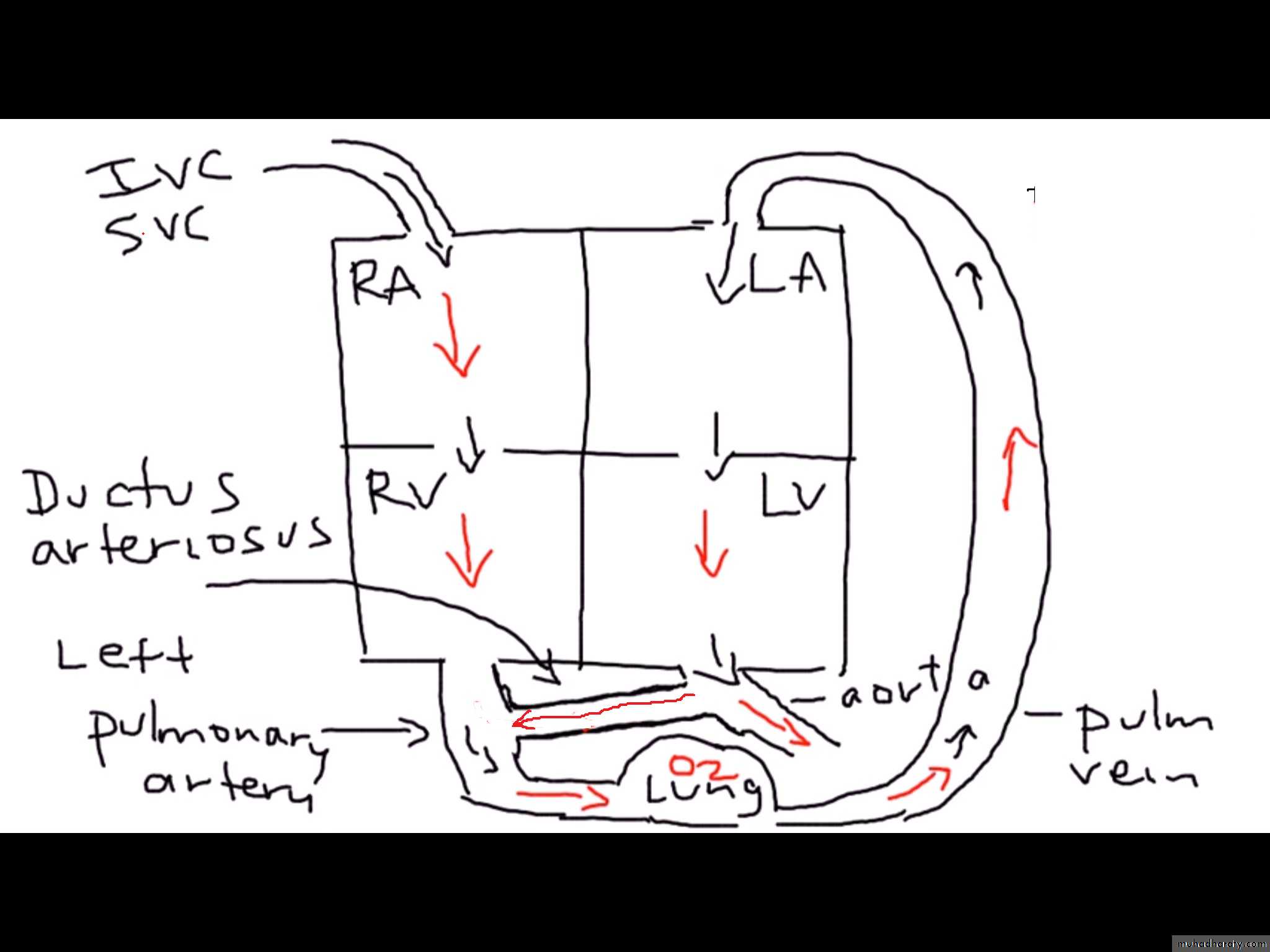
Adult with PDA
Adult5
PDA: Pathophysiology
The shunt involves PA, LA, LV, & aortaThe RV and RA are not involved in the shunt
6
PDA: Pathophysiology
The magnitude of the shunt depends on the size of the communicationUsually there is LV volume overload and increased flow through the mitral valve
7PDA: Clinical Presentation
Exertional dyspneaRecurrent chest infections
Congestive heart failure
8
PDA: Physical Findings
Large volume pulseLeft ventricular dilatation (displaced apex beat)
Systolic & diastolic thrills in the pulmonary area
Palpable systolic expansion of the pulmonary artery
9
PDA: Physical Findings
Left parasternal heave (RVH due to PHT)Auscultation: continuous murmur in the pulmonary area (machinery murmur)
10
PDA: Clinical Presentation
Eisenmenger syndrome with differential cyanosis:Cyanosis of the toes but not the fingers
The right to left shunt bypasses the cerebral and upper limb vessels & flows directly into the aorta
11

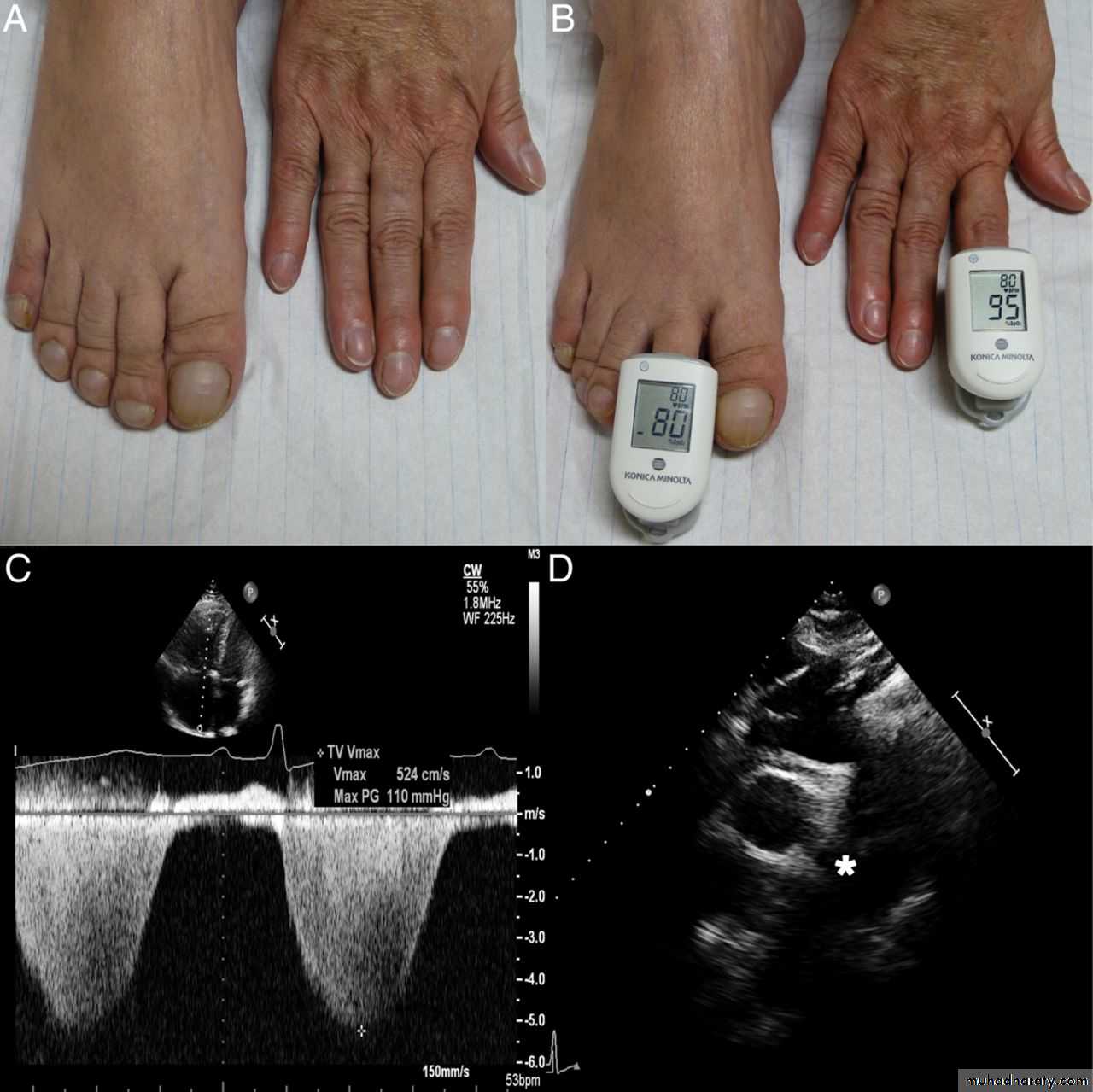
Moccetti F et al. Eur Heart J 2014;35:1410
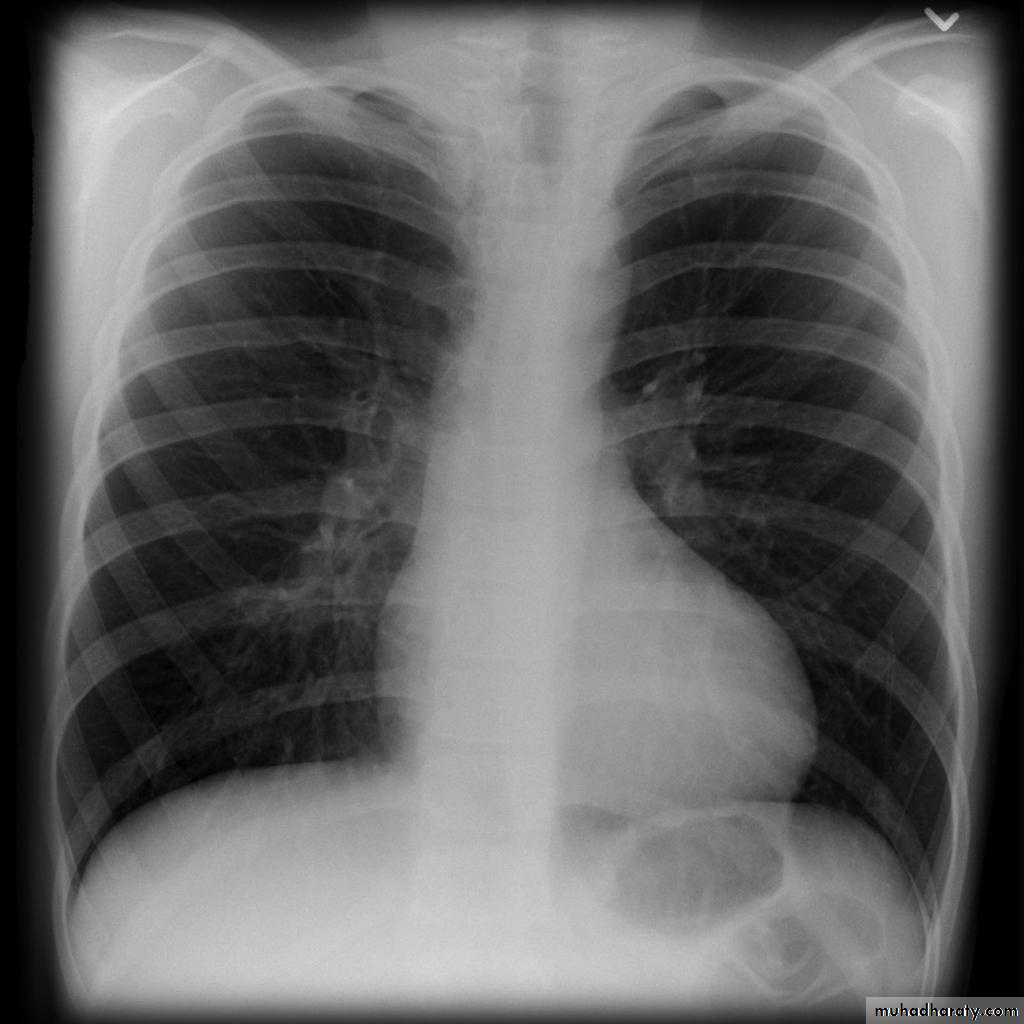
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions please email: journals.permissions@oup.comPDA: Investigations: CXR
LV & LA dilatationProminent main pulmonary artery
Plethoric lungs (increased pulmonary vascular markings: arterial and venous)
Prominent aorta
In older patients: the ductus may be calcified
13
14
PDA: Investigations
ECG: LVHtall R waves in chest leads V5 & V6
Deep S waves in chest leads V1 & V2
Echocardiography & Doppler: Demonstrates the site of the ductus and the continuous flow by Doppler
15
PDA: Management
Closure of the ductus whatever the sizeUsually closed through catheterization
Large ducts are closed surgically
16
Valvular Pulmonary Stenosis
Increased resistance for RV ejectionPressure gradient between RV & PA
This leads to right ventricular hypertrophy
The forceful jet into the PA leads to dilatation of the main pulmonary artery
17
Valvular PS: Clinical Picture
Raised JVPRVH: left parasternal heave
Systolic thrill in the pulmonary area
Faint pulmonary second sound
Systolic ejection murmur at the pulmonary area
18
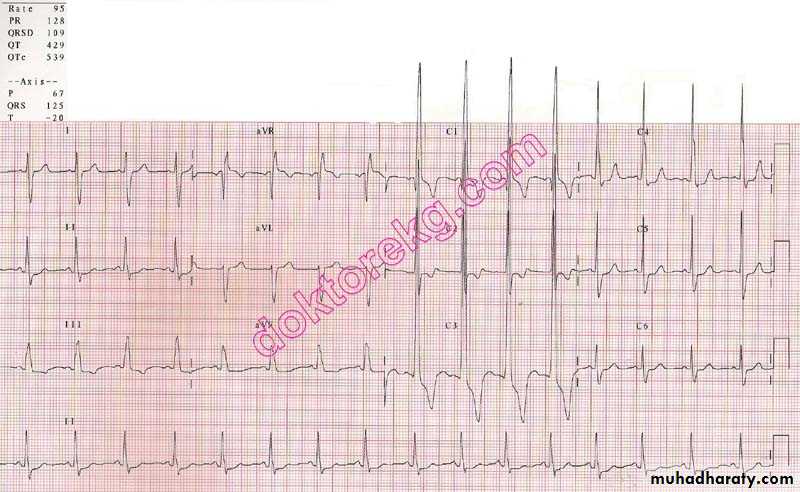
Valvular PS: Investigations
ECG:RVH: tall R waves in V1 & V2
CXR:
Oligemic lungs: reduced pulmonary blood flow
Prominent main pulmonary artery (post-stenotic dilatation)
19
ECG in PS
20
21
Valvular PS: Investigations
Echocardiography:Reduced pulmonary valve motion
Doppler: estimation of the gradient across the pulmonary valve
22
Valvular PS: Treatment
Transcatheter dilatation of the stenotic pulmonary valve using a balloon inflated at the pulmonary valveIf this fails: surgery
23
Coarctation of the Aorta
Narrowing of the aorta just distal to the origin of the left SCA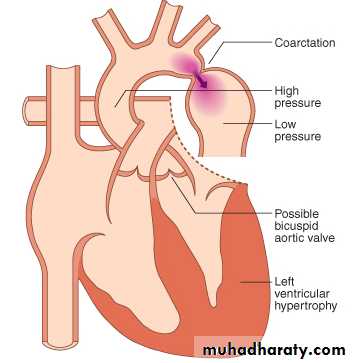
24
Coarctation of the Aorta
With age, collaterals form around the narrowing to bridge the proximal & distal parts25
Coarctation of the Aorta
Usually associated with bicuspid aortic valveMore common in males
26
Coarctation of the Aorta: Clinical
Co A is an important cause of congestive heart failure in neonatesOften undetected during physical examination
27
Coarctation of the Aorta: Clinical
The hallmark is radio-femoral delay of the pulse
28
Hypertension may cause headache
Leg cramps: reduced circulation in the lower limbs29
Coarctation of the Aorta: Clinical
BP is raised in the arms, normal in the legsAuscultation:
systolic murmur over the coarctation (heard over the back)
Systolic ejection click (dilated aorta, bicuspid aortic valve)
Continuous murmur from flow into collaterals: heard best over the spine
30
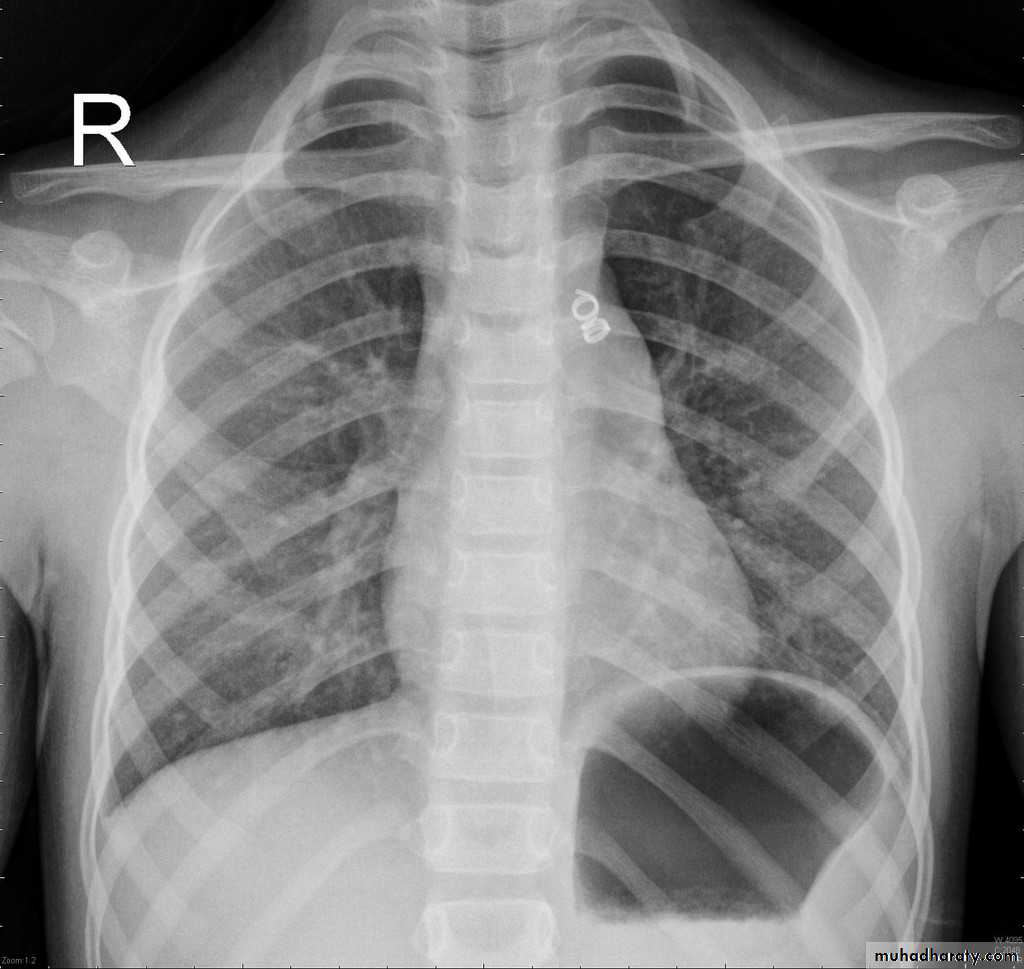
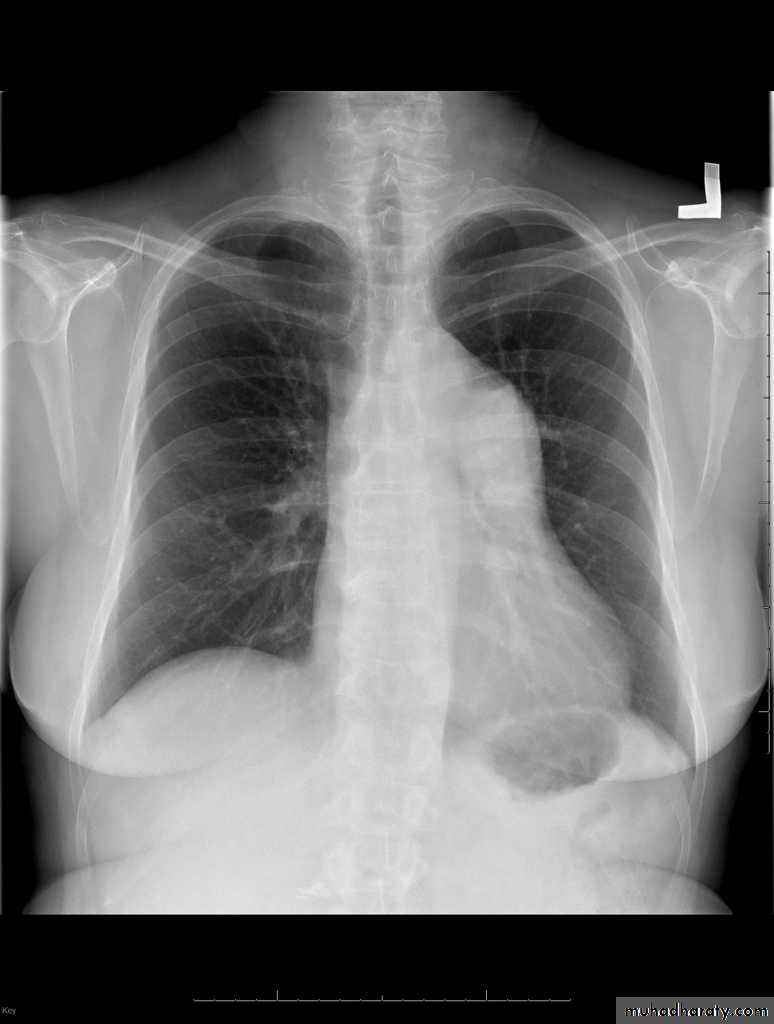
Coarctation of the Aorta: Investigations
CXR:Rib notching: from enlarged collaterals
Prestenotic and post-stenotic dilatation form the “3 sign” of the descending aorta
31
32
33
Coarctation of the Aorta: Investigations
Echocardiography:Shows the site of stenosis & pressure gradient across it
CT & MRI: can show the entire extent of the aorta
34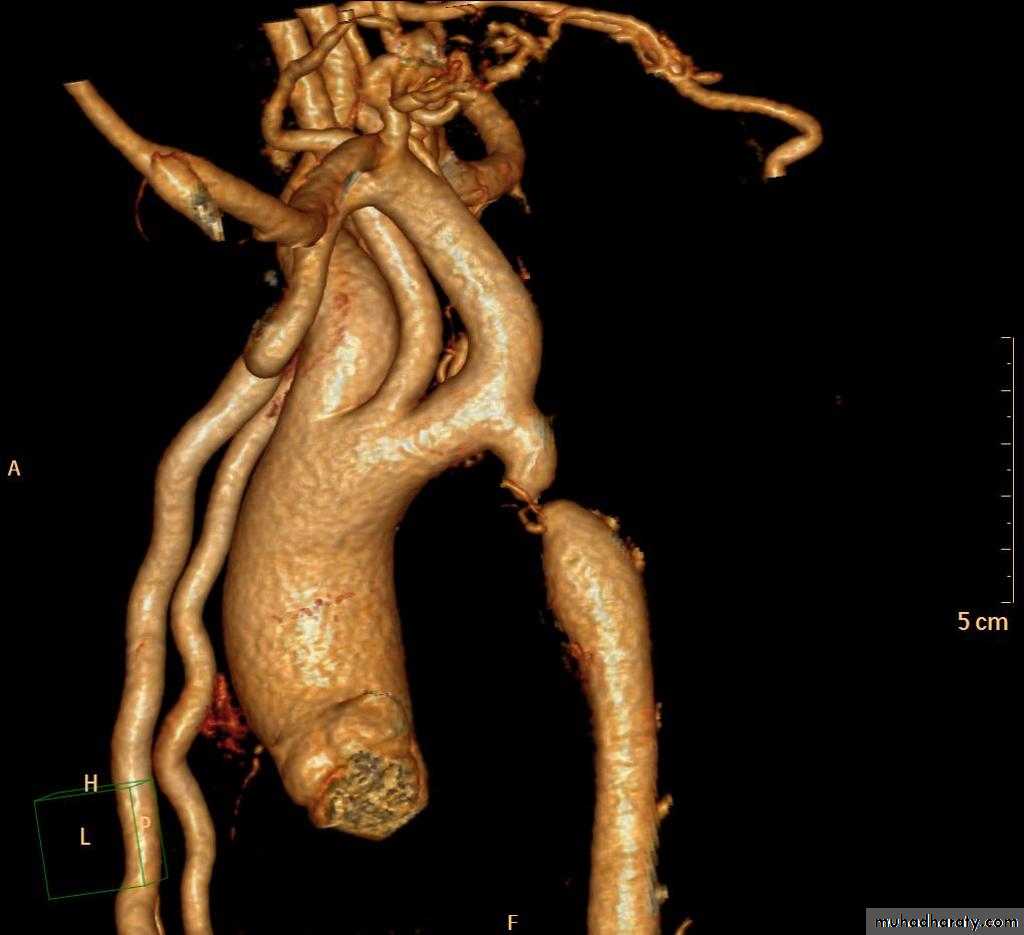
35
Coarctation of the Aorta: treatment
Early relief of obstruction: by surgery or catheter-based interventionBP returns to normal
If intervention is delayed, HT may persist
36
Tetralogy of Fallot (TOF)
The four components of TOF are:Ventricular septal defect
Over-riding aorta
Pulmonary stenosis, RV outflow tract obstruction
Right ventricular hypertrophy
37
38
TOF: Clinical Picture
Cyanosis & clubbingSquatting: sudden assumption of the sitting position in the upright patient:
This increases the LV afterload and reduces the magnitude of right -to-left shunt
39
TOF: Clinical Picture
Cyanotic spells: sudden lethargy and weakness with increased depth of cyanosis:Fever
Crying
Exertion
Cause: Reduced pulmonary blood flow & increased shunting of blood to the left side
40
TOF: Physical findings
ClubbingCyanosis
Prominent RV impulse
No thrill (≠ valvular PS): reduced pulmonary blood flow
41
TOF: Physical findings
Auscultation:
single second heart sound
Faint systolic ejection murmur at the pulmonary area
42
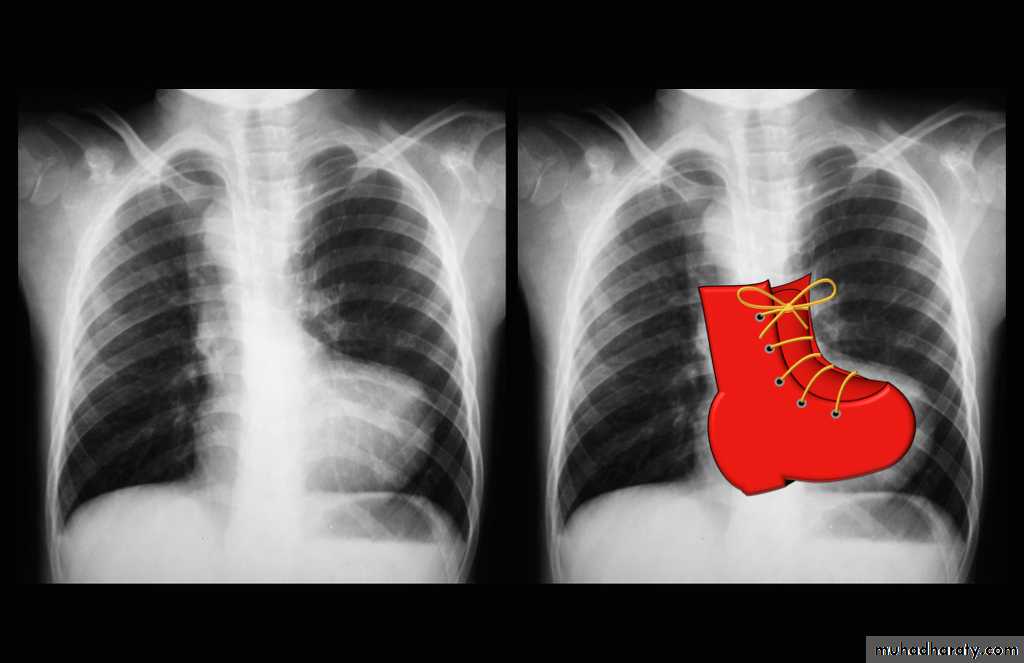
TOF: investigation
ECG:Right ventricular hypertrophy
Chest X ray:
Right ventricular enlargementPulmonary bay (underdeveloped pulmonary artery)
The combination of these findings gives the “boot-shaped heart”
43

44
45
TOF: Treatment
Surgical correctionIf the PA is very small & underdeveloped: the aorta is anastomosed to the pulmonary arteries to enhance their growth before total correction ( Blalock-Taussig shunt)
46