Inflammatory Bowel Disease (IBD)
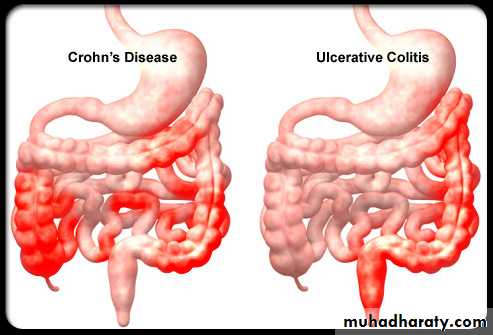
IBD disorders of idiopathic chronic intestinal inflammation: Crohn disease and ulcerative colitis.
Both disorders are characterized by unpredictable exacerbations and remissions. The onset is during adolescence and young adulthood. IBD is more common in urban areas than in rural areas.
Both genetic and environmental influences are involved in the pathogenesis of IBD.
• Cigarette smoking is a risk factor for Crohn disease but paradoxically protects against ulcerative colitis.• Men are slightly more likely to acquire ulcerative colitis than are women; the reverse is true for Crohn disease.
.
Chronic Ulcerative Colitis
It is localized to the colon and spares the upper gastrointestinal tract. Disease usually begins in the rectum and extends proximally . When it is localized to the rectum, the disease is ulcerative proctitis, whereas disease involving the entire colon is pancolitis.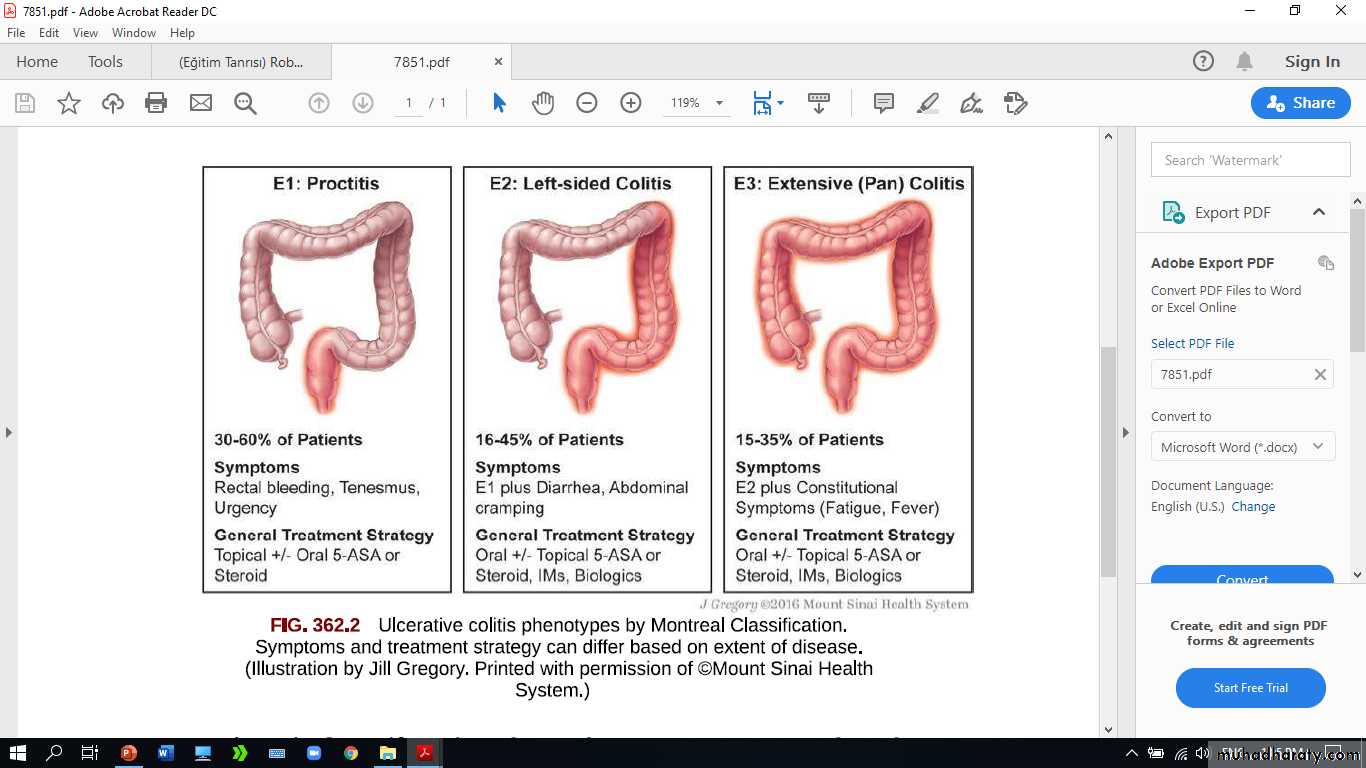
Clinical Manifestations
Blood, mucus, and pus in the stool as well as diarrhea are the typical presentation of ulcerative colitis.Constipation may be observed in those with proctitis. Tenesmus, urgency, cramping abdominal pain.
Fulminant colitis defined as Fever, severe anemia, hypoalbuminemia, leukocytosis, and greater than five bloody stools per day for 5 days.
Anorexia, weight loss, and growth failure may be present.
The clinical course of ulcerative colitis is marked by exacerbations.
The use of nonsteroidal anti-inflammatory drugs is predispose to exacerbation.
The risk of colon cancer begins to increase after 8-10 yr of disease.Extraintestinal manifestations
1. pyoderma gangrenosum,2. sclerosing cholangitis & chronic active hepatitis
3. ankylosing spondylitis.
4. Iron deficiency may result from chronic blood loss as well as decreased intake.

5.Folate deficiency.
6. Anemia of chronic disease.
7. Secondary amenorrhea.
Diagnosis
1. Typical presentation2. Laboratory studies
CBP: anemia (either iron deficiency or the anemia of chronic disease), WBC ↑ with more severe colitis.
• ↑ ESR & C-reactive protein .
• Hypoalbuminemia.3. Plain radiographs of the abdomen: may demonstrate loss of haustral markings in an air-filled colon or marked dilatation with toxic megacolon.
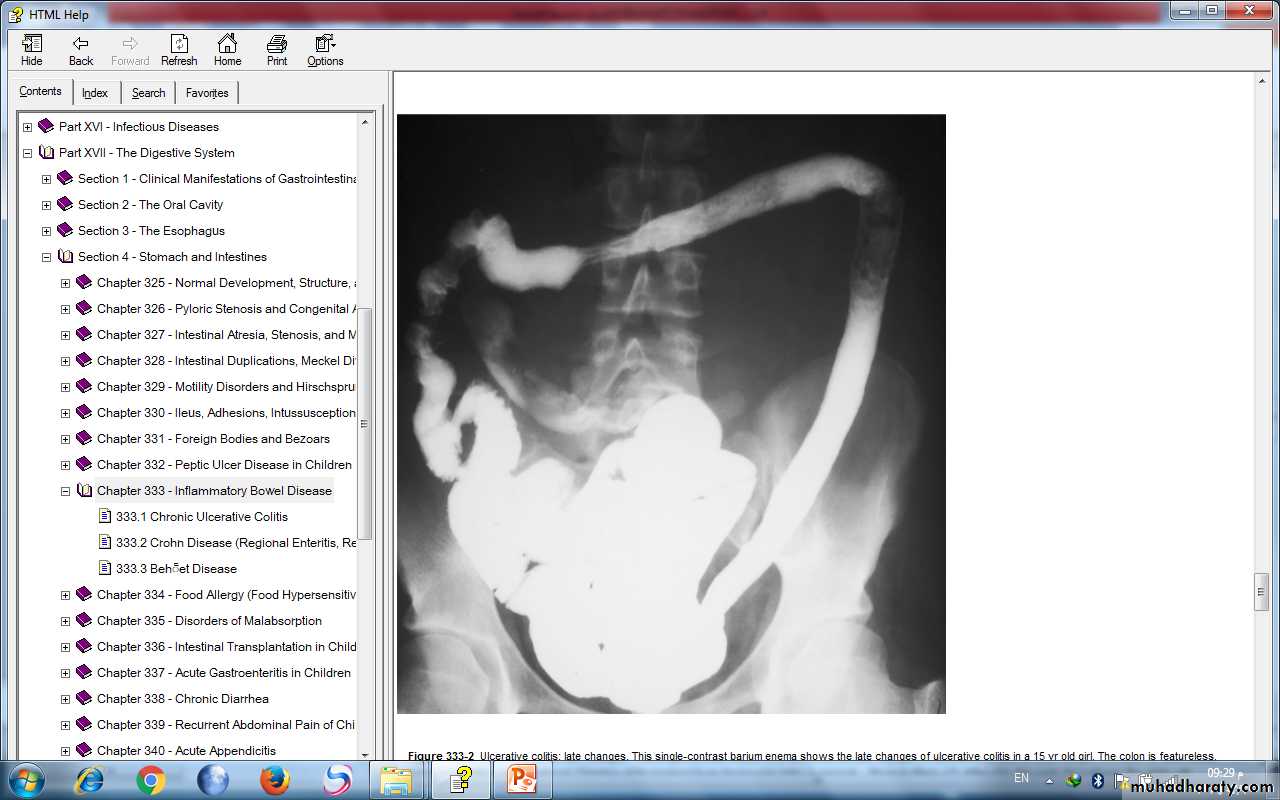
4. Barium enema.
Small ulcerations are distributed uniformly about the colonic circumference and continuously from the rectum to the proximal transverse colon
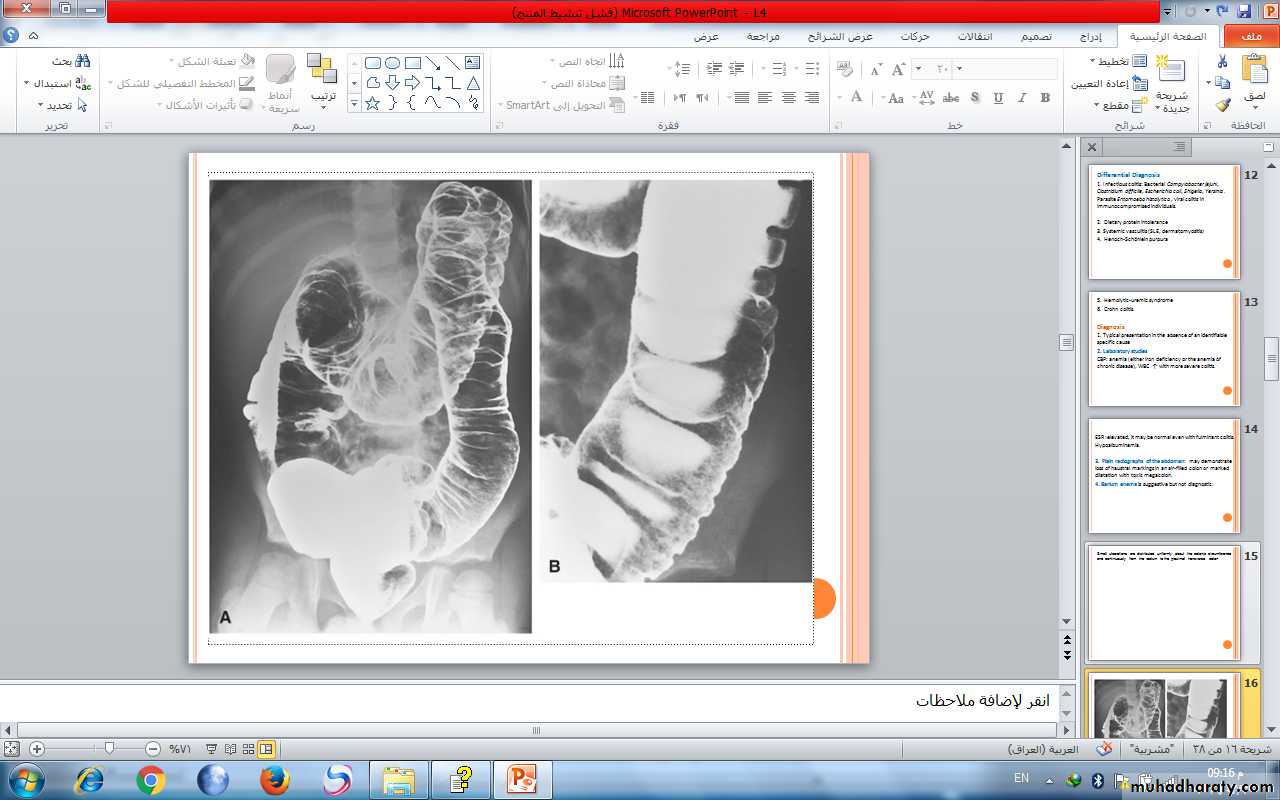
late changes:The colon is featureless, reduced in caliber, and shortened.
5. Sigmoidoscopy & colonoscopy with biopsy : characterized by erythema, edema, loss of vascular pattern, and friability.
The endoscopic findings of ulcerative colitis result from microulcers. With very severe chronic colitis, pseudopolyps may be seen.
Biopsy→ Typical findings are
cryptitis, & crypt abscesses
Treatment
A medical cure for ulcerative colitis is not available; treatment is aimed at controlling symptoms and reducing the risk of recurrence.1. In mild colitis :
* Aminosalicylate
1. Sulfasalazine: 50-75 mg/kg/24 hr (divided into 2-4 doses) PO.
• Onset of action may take several weeks.
2. Mesalamine: 40-60 mg/kg/day.
Hydrocortisone enemas (100 mg) are used to treat proctitis , once a day (usually bedtime) for 2-3 wk.2. I n moderate to severe pancolitis or colitis that is unresponsive to 5-aminosalicylate therapy treated with oral corticosteroids
Prednisone: 1-2 mg/kg/24 hr, taper to an alternate-day dose within 1-3 mo.
Children who requiring frequent corticosteroid therapy are started on immunomodulators such as azathioprine or 6-mercaptopurine.
Infliximab, a monoclonal antibody may use in fulminant colitis.
Surgical treatment(Colectomy):
Performed for intractable disease, complications of therapy, and fulminant disease that is unresponsive to medical management.
Crohn Disease (Regional Enteritis, Regional Ileitis, Granulomatous Colitis)
Involves any region of the alimentary tract from the mouth to the anus. Gastrointestinal involvement in Crohn disease is transmural.• Most commonly
• involves ileum and• colon (ileocolitis).
Clinical Manifestations
Small bowel disease: The patient have right lower quadrant pain with fibrostenosis.Those with colonic disease are more likely to have symptoms resulting from inflammation (diarrhea, bleeding, cramping)
Systemic signs and symptoms include:
Fever, malaise, and easy fatigability.Growth failure with delayed bone maturation and delayed sexual development may precede other symptoms by 1 or 2 yr.
Children may present with growth failure as the only manifestation of Crohn disease.
Primary or secondary amenorrhea.Perianal disease is common (tags, fistula, abscess).
Enteroenteric or enterocolonic fistulas→ malabsorption.• Enterovesical fistulas (between bowel and urinary bladder)→ signs of urinary infection, or fecaluria.
Intra-abdominal abscess, Hepatic or splenic abscess , Anorectal abscesses, Perianal abscess.
Extraintestinal manifestations oral aphthous ulcers, arthritis, erythema nodosum, digital clubbing, episcleritis, renal stones (uric acid, oxalate), and gallstones.

Diagnosis
1.History : any combination of abdominal pain (especially right lower quadrant), diarrhea, vomiting, anorexia, weight loss, growth retardation, and extraintestinal manifestations.2. physical examination: Children often appear chronically ill, pale, have weight loss and malnourished, Digital clubbing.
3. laboratory studies:
*CBP→ anemia, elevated platelet count (>600,000/mm3), WBC normal or mildly elevated.*Low serum albumin level
*ESR & C-reactive protein → elevated
*Stool α1-antitrypsin level may be elevated
*Anti-Saccharomyces antibodies are identified in 55% of children with Crohn
4. Endoscopic and radiologic findings
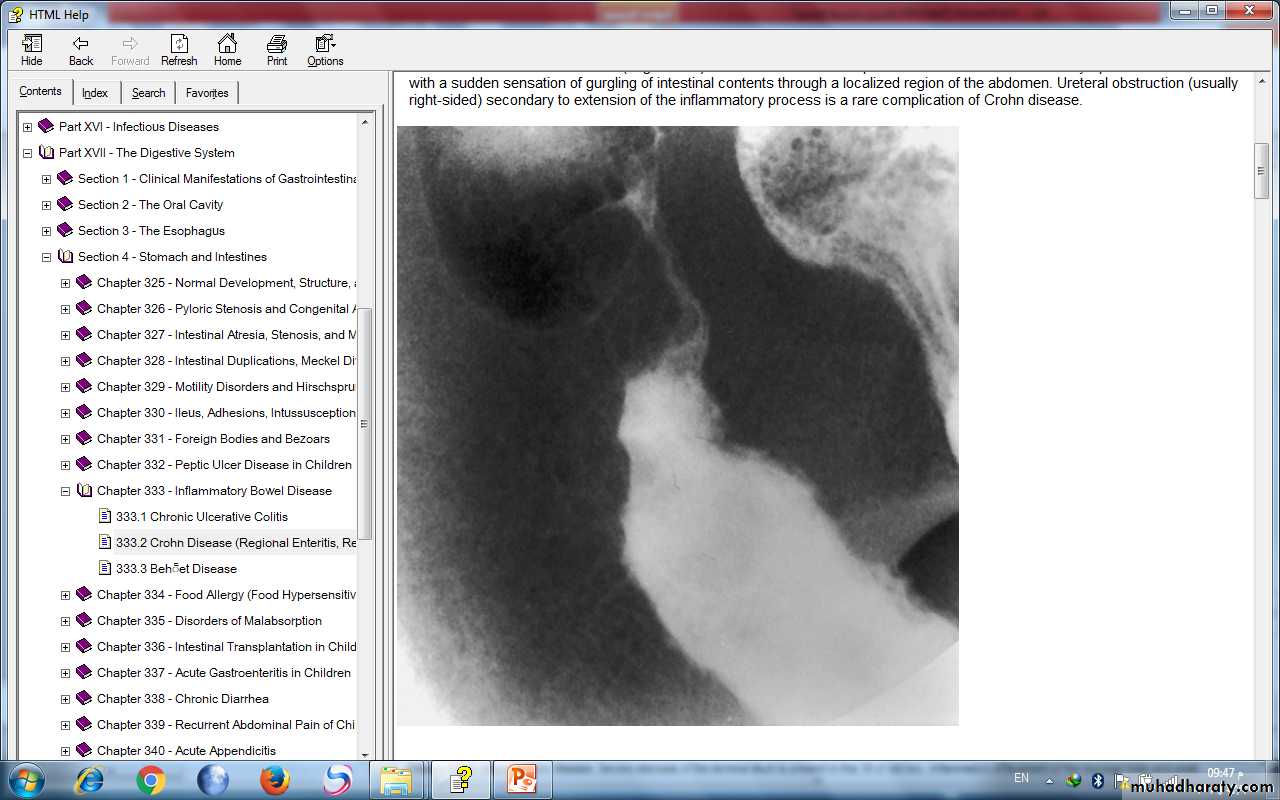
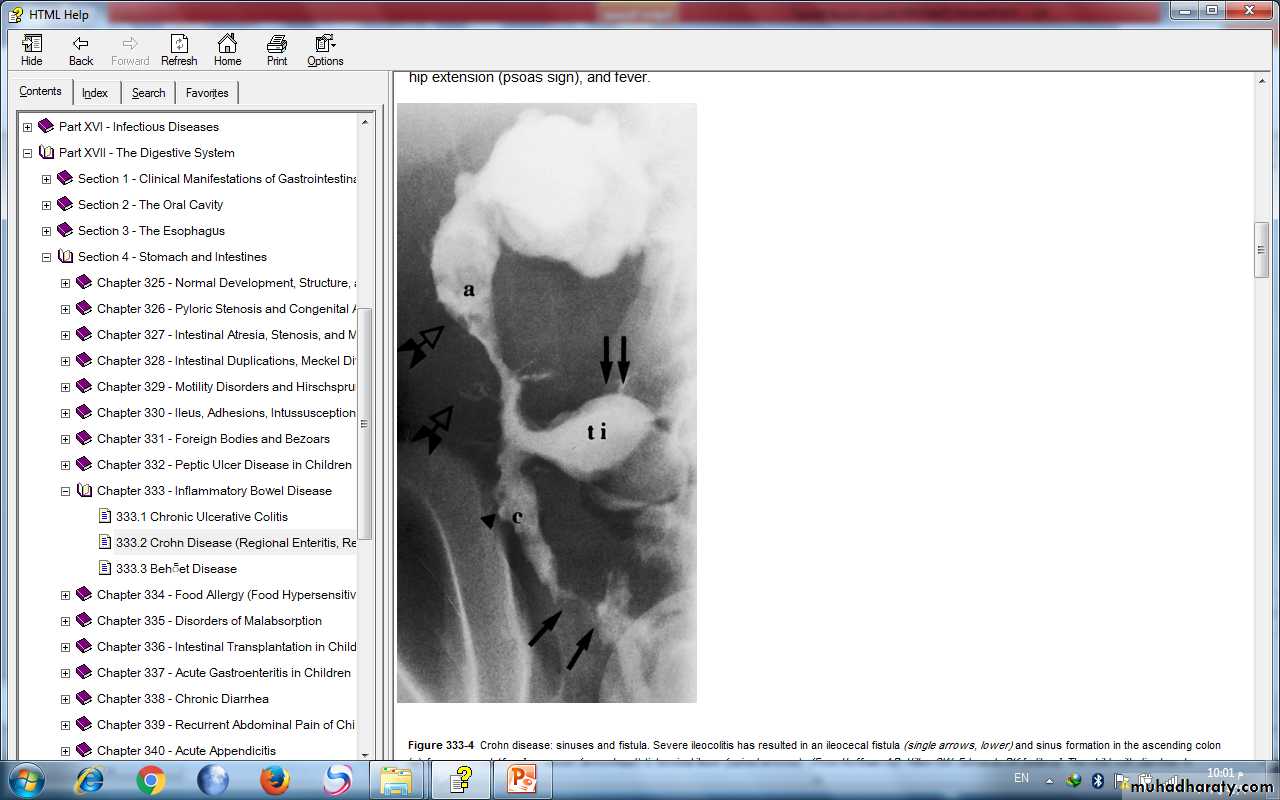
*Small bowel follow-through: show aphthous ulceration and thickened, narrowing of the lumen. Linear ulcers may give a cobblestone appearance to the mucosal surface.Other radiologic findings are fistulas ,sinus tracts, and strictures.
Double-contrast barium enema examination in Crohn's colitis demonstrates numerous aphthous ulcers (the tiny spots on the lining of the intestine).

Stricture, terminal ileum - colonoscopy

Severe stenosis of the terminal ileum. Inflammatory effacement of the mucosal folds and small ulcerations characterize the proximal nonstenotic segment.
*Ultrasonography and contrast CT : identifying intra-abdominal abscess.
*MRI: It is useful during pregnancy.*Colonoscopy with biopsy: Findings on colonoscopy include aphthous ulcers, linear ulcers, and strictures. Findings on biopsy → noncaseating granulomas.
Treatment
1.For mild terminal ileal disease or mild Crohn disease of the colon:mesalamine
Sulfasalazine
2. For more extensive or severe small bowel or colonic disease:
Corticosteroids (prednisone, 1-2 mg/kg/day).
Steroid enemas → used for distal colon disease.Children who become refractory to corticosteroid therapy or become dependent on daily dosing→ Immunomodulators such as azathioprine, 6-mercaptopurine, or Methotrexate .
A beneficial effect of these drugs may be delayed for 3-6 mo after starting therapy.
Infliximab serve as a bridge until the immunomodulators take effect.
3. For perianal disease and perirectal fistula→ Metronidazole , Azathioprine and 6-mercaptopurine.• 4. For children with growth failure → Nutritional therapy: enteral nutritional approach administered via a nasogastric or gastrostomy infusion, usually overnight.
High-calorie oral supplements.
• Pubertal delay→ sex steroids.
• Short stature→ growth hormone.Deficits in bone mineral density & osteopenia→ calcium, vitamin D therapy.
• 5. Psychologic counseling & Social support.
Surgical therapy
Indications:*unresponsive to medical treatment
*bowel perforation
*fibrosed stricture with obstruction
* intractable bleeding.
Intra-abdominal or liver abscess treated by ultrasonographic or CT-guided catheter drainage and concomitant intravenous antibiotic treatment.