
Congenital Malformations Of Central Nervous System (CNS)
Neural tube defectsNeural tube defects (NTDs) are commonest congenital anomalies of the CNS and result from failure of the neural tube to close spontaneously between the 3rd and 4th wk of in utero development.
Etiology
UnknownHyperthermia
Drugs (valproic acid)
Malnutrition
Low red cell folate levels
Maternal obesity or diabetes
Genetic determinants (mutations in Folate-responsive or folate-dependent enzyme pathways)
Abnormal maternal nutritional state
Exposure to radiation before conception.
Prenatal screening
Prenatal screening of maternal serum for AFP
(alfa fetoprotein ) in the 16th-18th wk of gestation is an effective method for identifying pregnancies at risk for fetuses with NTDs in utero.
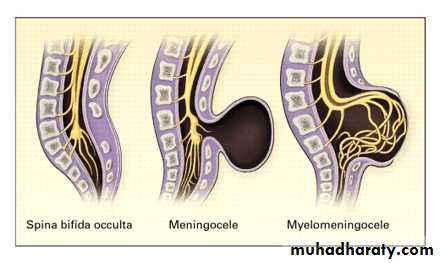
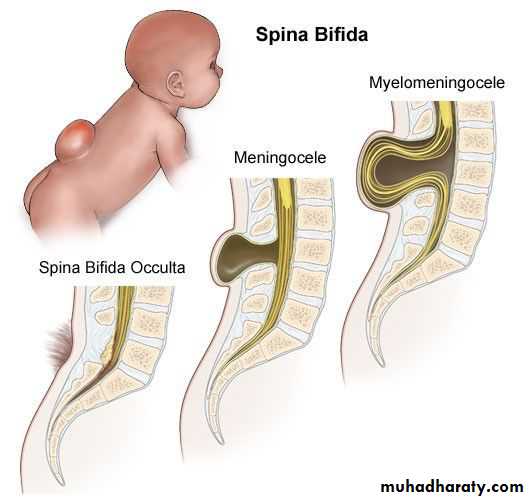
Spina bifida occulta
is a common anomaly
consisting of a midline
defect of the vertebral
bodies without protrusion
of the spinal cord or meninges.
Most patients are asymptomatic and lack
neurologic signs.
This simple defect does not have an associated spinal cord malformation but there are cutaneous manifestations such as hemangioma, discoloration of the skin, pit, lump , dermal sinus, or hairy patch.
All cases of occult spinal dysraphism are best investigated with MRI



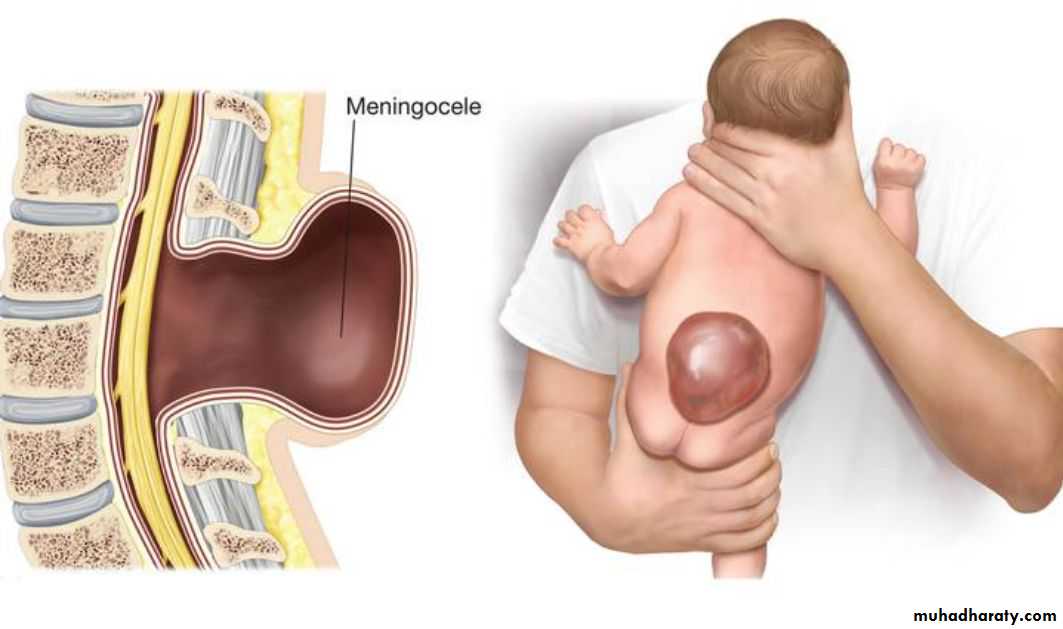
Meningocele
A meningocele is formedwhen the meninges herniate
through a defect in the
posterior vertebral arches
or the anterior sacrum.
Most meningoceles are well
covered with skin .Carefulneurologic examination is mandatory.


Orthopedic and urologic examination should also be considered.
asymptomatic children with normal neurologic findings and full-thickness skin covering the meningocele surgery may be delayed .Prognosis
Children with meningocele generally have a goodprognosis
But if meningocele associated with hydrocephalus have
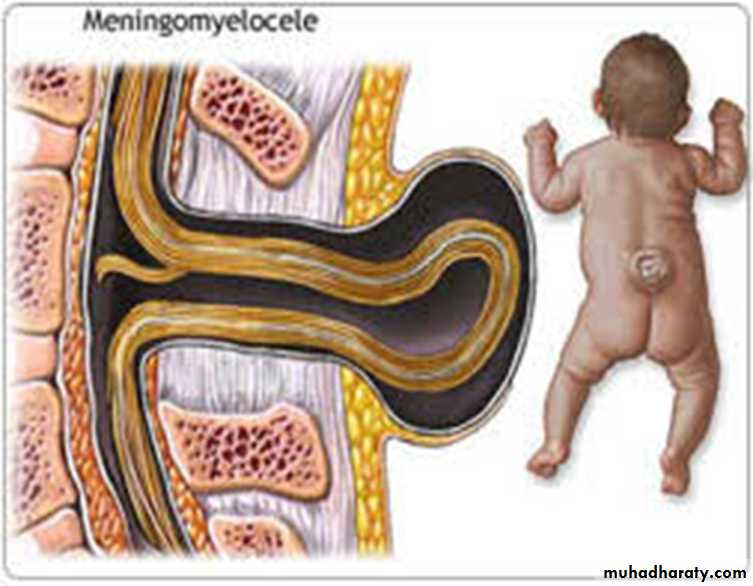
the poorest prognosis.Myelomeningocele
Myelomeningocelerepresents the most
severe form of dysraphism
so-called open form,
involving the vertebral
column and spinal cord.
CLINICAL MANIFESTATIONS
Myelomeningocele produces dysfunction of skeleton,skin, gastrointestinal , genitourinary tracts, peripheral
nervous system and the CNS.
A myelomeningocele located in lumbosacral region
accounts for 75% of the cases.
A lesion in the low sacral
region causes bowel and
bladder incontinence

Examination of the infant shows a flaccid paralysis of
the lower extremities, an absence of deep tendonreflexes , a lack of response to touch and pain, and
a high incidence of lower-extremity deformities
(clubfeet, ankle and/or knee contractures, and
subluxation of the hips).
Patients with a myelomeningocele in
the upper thoracic or the cervical
region usually have a very minimal
neurologic deficit in most cases .

TREATMENT
1-Surgery : repair of a myelomeningocele is often done within a day of birth 2-Shunting procedure for hydrocephalus if present.3-Clubfeet may require casting.
4-Careful evaluation of the genitourinary system, & regularly catheterize a neurogenic bladder to prevents urinary tract infections and refluxPROGNOSIS
A child who is born with a myelomeningocele and who is treated aggressively, the mortality rate is 10-15%, and most deaths occur before age 4 yr.At least 70% of survivors have normal intelligence, but learning problems and seizure disorders are more common.
Renal dysfunctioncomnon cause of mortality
PREVENTION
Folic acid supplementation should be initiated before conception and continued until at least the 12th wk of gestation . All women of child bearing age take 0.4 mg of folic acid daily.
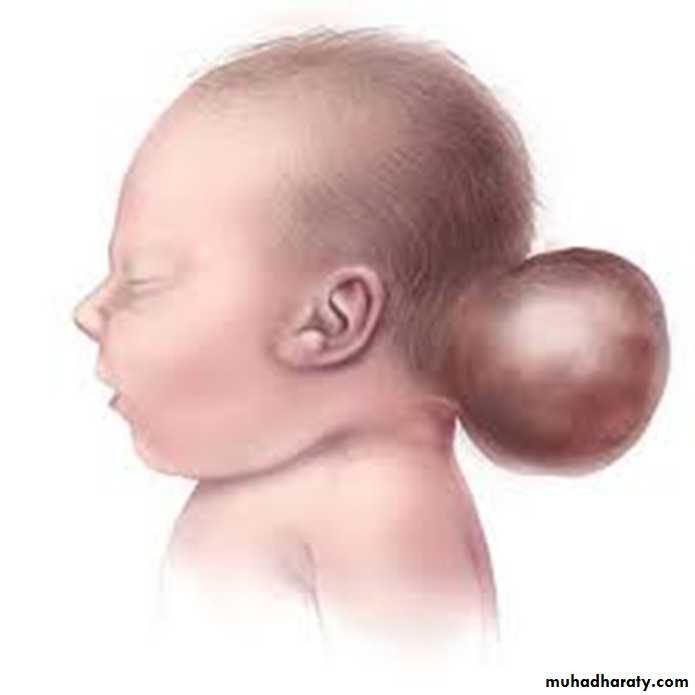
Encephalocele
Protrusion of tissue througha bony midline defect
(commonly in the occipital region).
a cranial encephalocele contains
the sac contain cerebral cortex,
cerebellum, or portions of the brainstem.
Infants with a cranial encephalocele are at increased risk
for developing hydrocephalus.patients with an encephalocele are at risk for vision problems,
microcephaly, intellectual disability, and seizures.
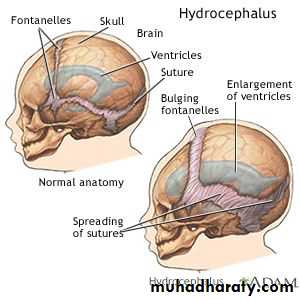
Hydrocephalus
Hydrocephalus is not a specific disease; that result from impaired circulation and absorption of CSF .
Physiology:
The CSF is formed primarily in the ventricular system by the choroid plexus, which is situated in the lateral, 3rd, and 4th ventricles.
The total volume of CSF approximates 50 mL in an infant and 150 mL in an adult. Intraventricular pressure is 180 mm H2O.
Hydrocephalus resulting from obstruction within the ventricular system is called obstructive or non communicating hydrocephalus.
The CSF then circulates from the basal cisterns over the convexities of the cerebral hemispheres & absorbed by the arachnoid villi.
Hydrocephalus resulting from obliteration of the subarachnoid cisterns or malfunction of the arachnoid villi is called nonobstructive or communicating hydrocephalus.
Etiology
Obstructive hydrocephalus( non communicating) :1-Aqueductal stenosis
– Infectious (meningitis)
– neurofibromatosis.
2-Lesions or malformation of posterior fossa like tumor, Chiari malformation, Dandy-Walker malformation.
3-Mass lesions ( Abscess, Hematoma and neurocutaneous disorders, Vein of Galen malformation).
Communicating hydrocephalus:
1-Meningitis (Pneumococcal and tuberculous meningitis thick CSF)2- Subarachnoid hemorrhage
3- Leukemic infiltrates.
4- Choroid plexus papilloma.
5- Achondroplasia.
Clinical manifestations
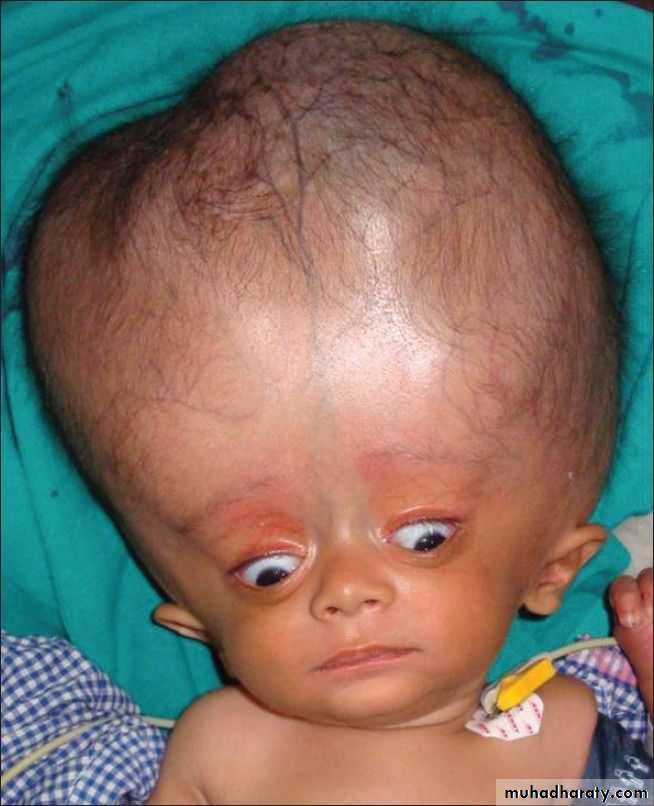
It is variable and depends on many factors, including the age at onset, the nature of the lesion causing obstruction, duration and rate of increase intracranial pressure (ICP).In infants:
Accelerated rate of enlargement of the head .
The anterior fontanel is wide open and bulging, and the scalp veins are dilated.
The forehead is broad, and the eyes deviate downward, producing the setting-sun sign.
Long-tract signs including brisk tendon reflexes, spasticity, and + ve Babinski sign.

In older child
The cranial sutures are partially closed so that the signs of hydrocephalus become difficult.Headache is a prominent symptom in older patients.
Irritability, lethargy, poor appetite,and vomiting are common .
A gradual change in personality and a deterioration in academic productivity
Examination:
1-Serial measurements ofthe head circumference(OFC)
3-Fundoscopy (Papilledema), abducens nerve palsy, and pyramidal signs mainly in the lower extremities
• 2-Percussion of the skull may
• produce a cracked pot sound,
• indicating separation of the sutures.

Chiari malformation:
• consists of two major subgroups.Type I typically produces symptoms during adolescence or adult life and is usually not associated with hydrocephalus. Patients complain of recurrent headache, neck pain, urinary frequency, and progressive lower extremity spasticity. The deformity consists of displacement of the cerebellar tonsils into the cervical canal.
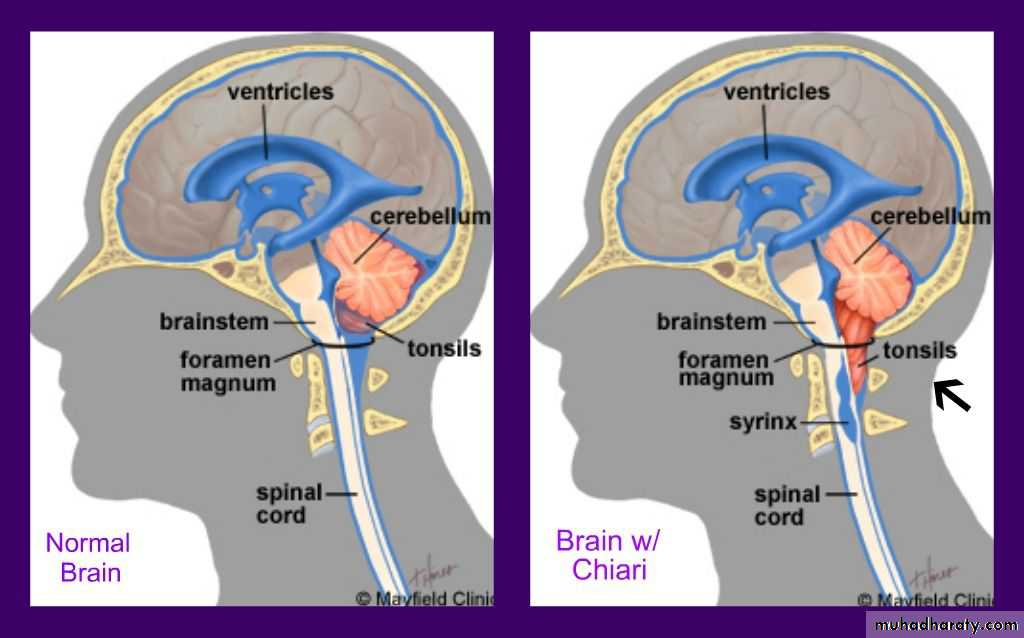
Type II Chiari malformation
• This lesion represents an elongation of the 4th ventricle• and kinking of the brainstem , with displacement of the
• pons, and medulla into the cervical canal.
• Symptoms during infancy consisting of
• stridor, weak cry, and apnea.
Dandy-Walker malformation consists
• of a cystic expansion of the 4th ventricle
• in the posterior fossa. 90% of patients
• have hydrocephalus

Anencephaly
Large defect of the calvarium,meninges, and scalp associated
with a rudimentary brain.
The cerebral hemispheres and cerebellum are usually absent, and only a residue of the brainstem can be identified.
Most anencephalic infants die within several days of birth.

Q1. To be effective for preventing myelomeningocele, administration of folic acid needs to begin:
• By 3 months of gestation
• At the first missed period
• Before conception
• By 30 days of gestation
• At 3 months prior to delivery
• Q2. Enumerate causes of Communicating hydrocephalus?
