1
Anatomy of female pelvis and fetal head
Maternal Pelvis anatomy
Bony pelvis
The bony pelvis is made of 4 bones: the sacrum, coccyx, and 2 innominate bones which are
(composed of the ilium, ischium, and pubis). These are held together by the SIJ, and the SCJ
joints.
The anterior superior edge of the 1
st
sacral vertebra is called the promontory which is an
important land mark in obstetrics.
The anterior aspect of the sacrum is usually concave.
The pelvis is divided into the false and true pelvis.
The true pelvis is important in obstetrics, it is a bony canal is formed by the sacrum and
coccyx posteriorly and by the ischium and pubis laterally and anteriorly, the true pelvis
dimensions are of concern in obstetrics because sometimes these are inadequate to permit
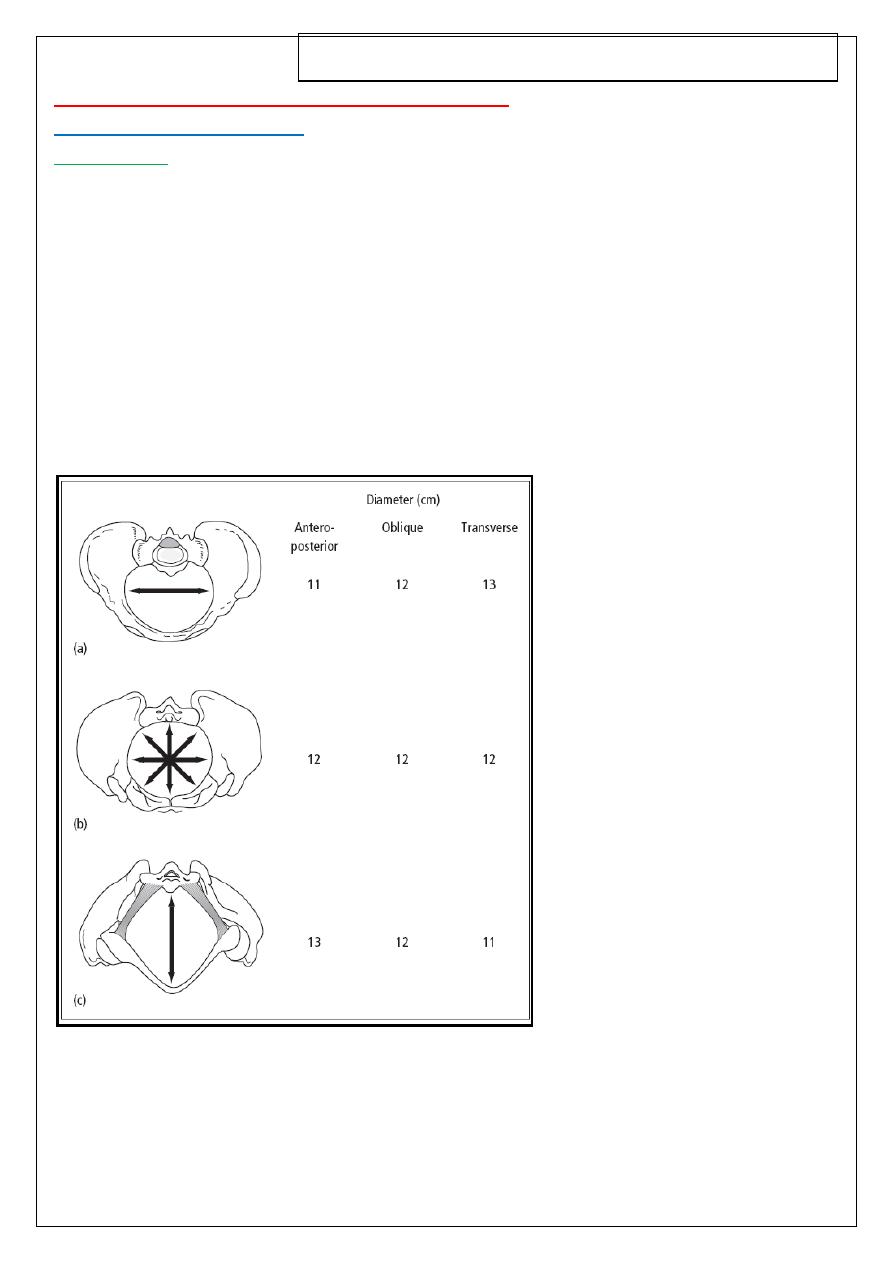
passage of the fetus. the false pelvis is not important. Diameters are shown in Figure below:
Figure The bony pelvis.
(a) Inlet: Bean shaped.
(b) Mid-cavity: Circular.
(c) Outlet: Diamond shaped
.
Fourth Stage / Obstetrics / Dr.Nadia / Lecture 4
2
Pelvic diameters:
These represent the space available for the fetal head when it passes through the pelvis
during labour
1- the obstetric conjugate of the pelvic inlet: 11 cm
2- the bispinous diameter: 10.5 cm in the midcavity.
3- the bituberous diameter 11 cm in the pelvic outlet
4- the curve and length of the sacrum
5- and finally the subpubic angle
The female bony pelvis is divided into:
False pelvis: above the pelvic brim and has no obstetric importance.
True pelvis: below the pelvic brim and related to the child -birth.
THE TRUE PELVIS
It is composed of inlet, cavity, and outlet.
The Pelvic Inlet (Brim)
Boundaries
Sacral promontory,
alae of the sacrum,
sacroiliac joints,
iliopectineal lines,
iliopectineal eminencies,
upper border of the superior pubic rami,
pubic tubercles,
pubic crests and
upper border of symphysis pubis.
Diameters of pelvic inlet
*Antero -posterior diameters:
Anatomical antero-posterior diameter (true conjugate) = 11cm : from the tip of the sacral
promontory to the upper border of the symphysis pubis.
Obstetric conjugate = 10.5 cm :from the tip of the sacral promontory to the most bulging
point on the back of symphysis pubis which is about 1 cm below its upper border. It is the
shortest antero-posterior diameter.
3
Diagonal conjugate = 12.5 cm : i.e. 1.5 cm longer than the true conjugate. From the tip of
sacral promontory to the lower border of symphysis pubis.
External conjugate = 20 cm : from the depression below the last lumbar spine to the upper
anterior margin of the symphysis pubis measured from outside by the pelvimeter . It has
not a true obstetric importance.
*Transverse diameters:
Anatomical transverse diameter =13cm: between the farthest two points on the
iliopectineal lines, It lies 4 cm anterior to the promontory and 7 cm behind the symphysis. It
is the largest diameter in the pelvis.
Obstetric transverse diameter: It bisects the true conjugate and is slightly shorter than the
anatomical transverse diameter.
* Oblique diameters:
Right oblique diameter =12 cm :from the right sacroiliac joint to the left iliopectineal
eminence.
Left oblique diameter = 12 cm :from the left sacroiliac joint to the right iliopectineal
eminence.
Sacro-cotyloid diameters = 9-9.5 cm : from the promontory of the sacrum to the right and
left iliopectineal eminence, so the right diameter ends at the right eminence and vice versa.
The Pelvic Cavity
It is a segment, the boundaries of which are:
the roof is the plane of pelvic brim,
the floor is the plane of least pelvic dimension,
anteriorly the shorter symphysis pubis,
posteriorly the longer sacrum.
The Pelvic Outlet
Anatomical outlet
It is lozenge-shaped bounded by;
the lower border of symphysis pubis,
pubic arch,
ischial tuberosities,
sacrotuberous and sacrospinous ligaments and,
4
tip of the coccyx.
Obstetric outlet
It is a segment, the boundaries of which are:
the roof is the plane of least pelvic dimension,
the floor is the anatomical outlet,
anteriorly the lower border of symphysis pubis,
posteriorly the coccyx.
laterally the ischial spines.
Diameters of pelvic outlet
*Antero - posterior diameters:
Anatomical antero-posterior diameter =11cm :from the tip of the coccyx to the lower
border of symphysis pubis.
Obstetric antero-posterior diameter = 13 cm : from the tip of the sacrum to the lower
border of symphysis pubis as the coccyx moves backwards during the second stage of
labour.
Transverse diameters:
Bituberous diameter = 11 cm : between the inner aspects of the ischial tuberosities.
Bispinous diameter = 10.5 cm : between the tips of ischial spines.
Pelvic Planes
These are imaginary planes lie as follow:
Plane of pelvic inlet:
passing with the boundaries of pelvic brim and making an angle of 55o with the horizon
(angle of pelvic inclination).
Plane of mid cavity:
(plane of greatest pelvic dimensions)
pass between the middle of the posterior surface of the symphysis pubis and the junction
between 2nd and 3rd sacral vertebrae. Laterally, it passes to the centre of the acetabulum
and the upper part of the greater sciatic notch.
It is a round plane with diameter of 12.5 cm.
5
Internal rotation of the head occurs when the biparietal diameter occupies this wide pelvic
plane while the occiput is on the pelvic floor i.e. at the plane of the least pelvic dimensions.
Plane of obstetric outlet
: (plane of least pelvic dimensions):
passes from the lower border of the symphysis pubis anteriorly, to the ischial spines
laterally, to the tip of the sacrum posteriorly.
Plane of anatomical outlet:
passes with the boundaries of anatomical outlet and consists of 2 triangular planes with
one base which is the bituberous diameter.
Anterior sagittal plane: its apex at the lower border of the symphysis pubis.
Posterior sagittal plane: its apex at the tip of the coccyx.
Anterior sagittal diameter: 6-7 cm : from the lower border of the symphysis pubis to
the centre of the bituberous diameter.
Posterior sagittal diameter: 7.5-10 cm : from the tip of the sacrum to the centre of
the bituberous diameter.
Pelvic Axes
Anatomical axis (curve of Carus)
It is an imaginary line joining the centre points of the planes of the inlet, cavity and
outlet.
It is C shaped with the concavity directed forwards.
It has no obstetric importance.
Obstetric axis
It is an imaginary line represents the way passed by the head during labour.
It is J shaped passes downwards and backwards along the axis of the inlet till the
ischial spines where it passes downwards and forwards along the axis of the pelvic
outlet.
Pelvic shapes (types):
We have 4 types or shapes of the bony pelvis and these are: the gynecoid, android,
anthropoid, and finally the platypelloid.
The fetal head enters the pelvic inlet in the transverse position then the head rotates in the
pelvic cavity to the anterior position.
Inside the pelvic cavity there is a plane of least diameters which is formed by lower edge of
the pubis anteriorly, ischial spines and sacrospinous ligaments laterally and the lower
6
sacrum posteriorly this plane is the most important from a clinical point of view and deep
transverse arrest generally occurs in this plane.
Each type of the pelvises has certain diameters and we have to know the characteristic of
each type and its compatibility for vaginal delivery of the fetus:
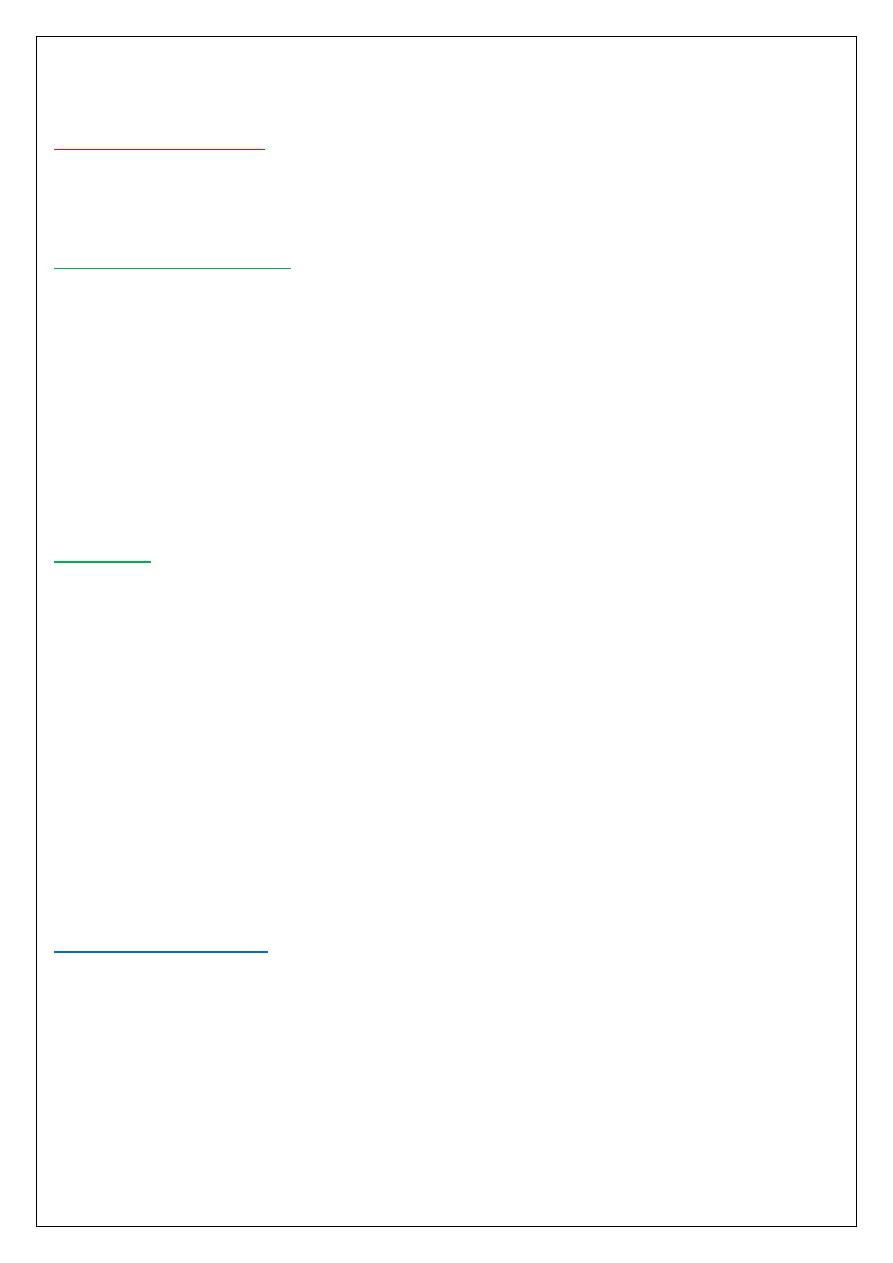
The gynecoid pelvis:
it is the classic female pelvis and is seen in about 50% of all the women and characterized
by the following:
Rounded bean shape inlet, side walls are straight, ischial spines are of average prominence,
well curved sacrum, wide subpubic arch.
It is the best shape suitable for normal vaginal delivery because the fetal head rotate easily
into the occipito-anterior position.
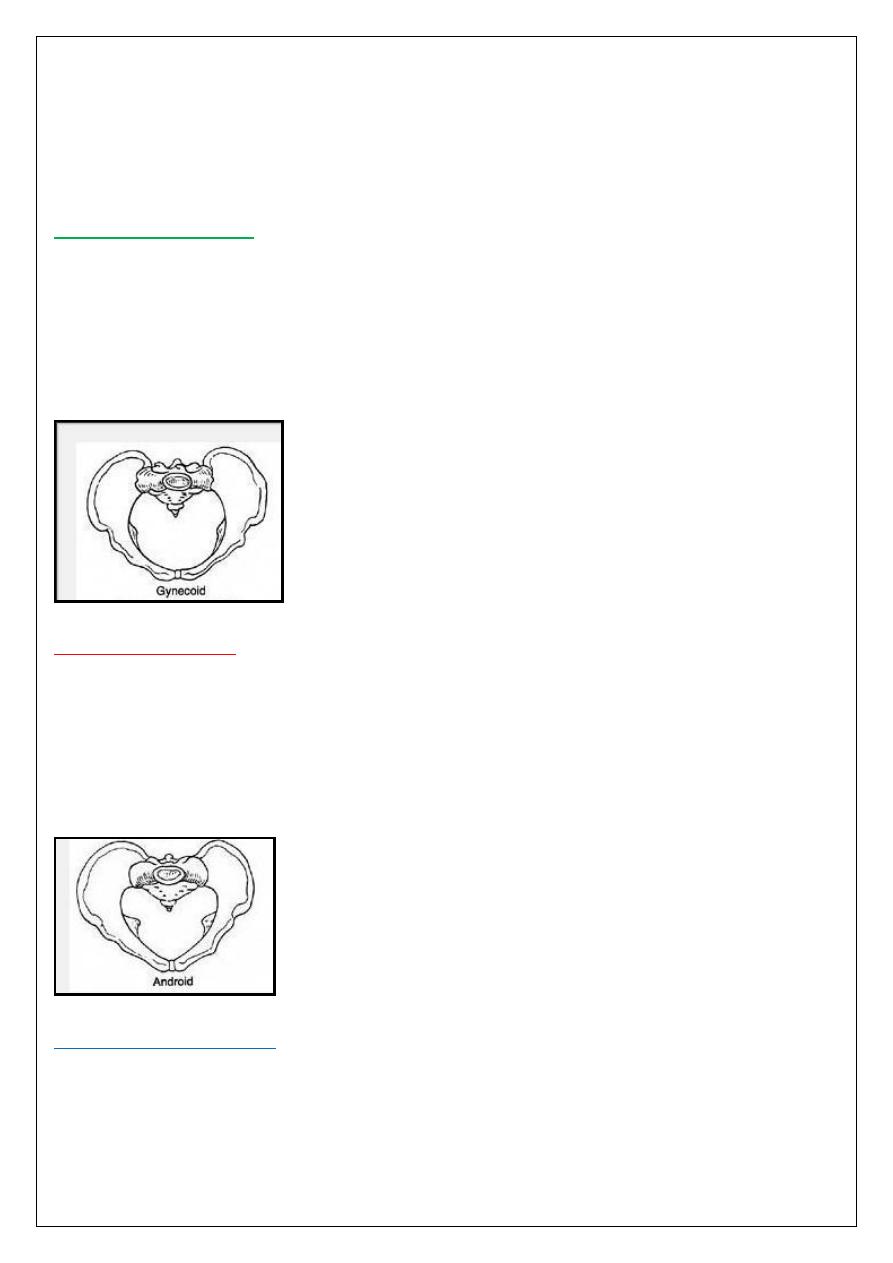
The android pelvis
:
which is the typical male pelvis and found in < than 30% of women and characterized by:
Heart shape inlet (triangular), convergent side wall (funnel shape) with prominent spines,
straight sacrum, and narrow subpubic arch.
This type is not suitable for vaginal delivery for the average size fetus unless the fetus is
very small or immature because this pelvis is narrow from the inlet and progressively
downward.
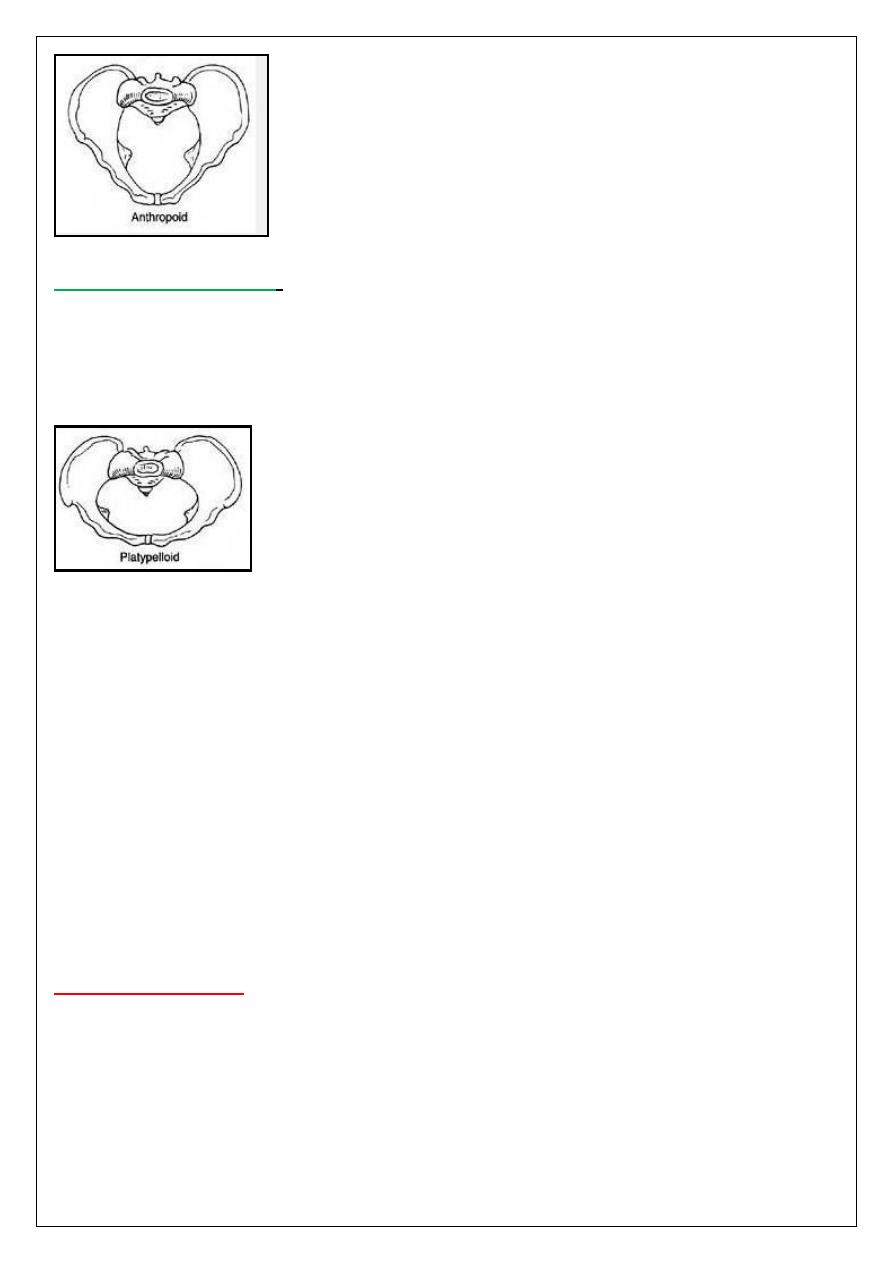
The anthropoid pelvis:
is found in 20% of women and characterized by:
A long and narrow oval shaped inlet, straight side walls, non prominent ischial spines,
variable sacrum, and narrow subpubic arch. The fetal head can engages in this type but
usually in the occipito-posterior position.
7
The platypelloid pelvis
:
which is a flattened gynecoid pelvis and seen in 3% of women and characterized by:
Oval shaped inlet which has wider transverse diameter, straight or divergent side walls,
posterior inclination of a flat sacrum, wide bispinous diameter and subpubic arch. The fetal
head has to engage in the transverse diameter.
N.B. At the Level of Ischial Spines:
The plane of obstetric outlet (plane of the least pelvic dimensions) is at this level.
The levator ani muscles are situated at this level and its ischio-coccygeous part is
attached to the ischial spines.
The obstetric axis of the pelvis changes its direction.
The head is considered engaged when the vault is felt vaginally at or below this level.
Internal rotation of the head occurs when the occiput is at this level.
Forceps is applied only when the head at this level (mid forceps) or below it (low and
outlet forceps).
Pudendal nerve block is carried out at this level.
The external os of the cervix is located normally.
The vaginal vault is located nearly.
The ring pessary should be applied above this level for treatment of prolapse.
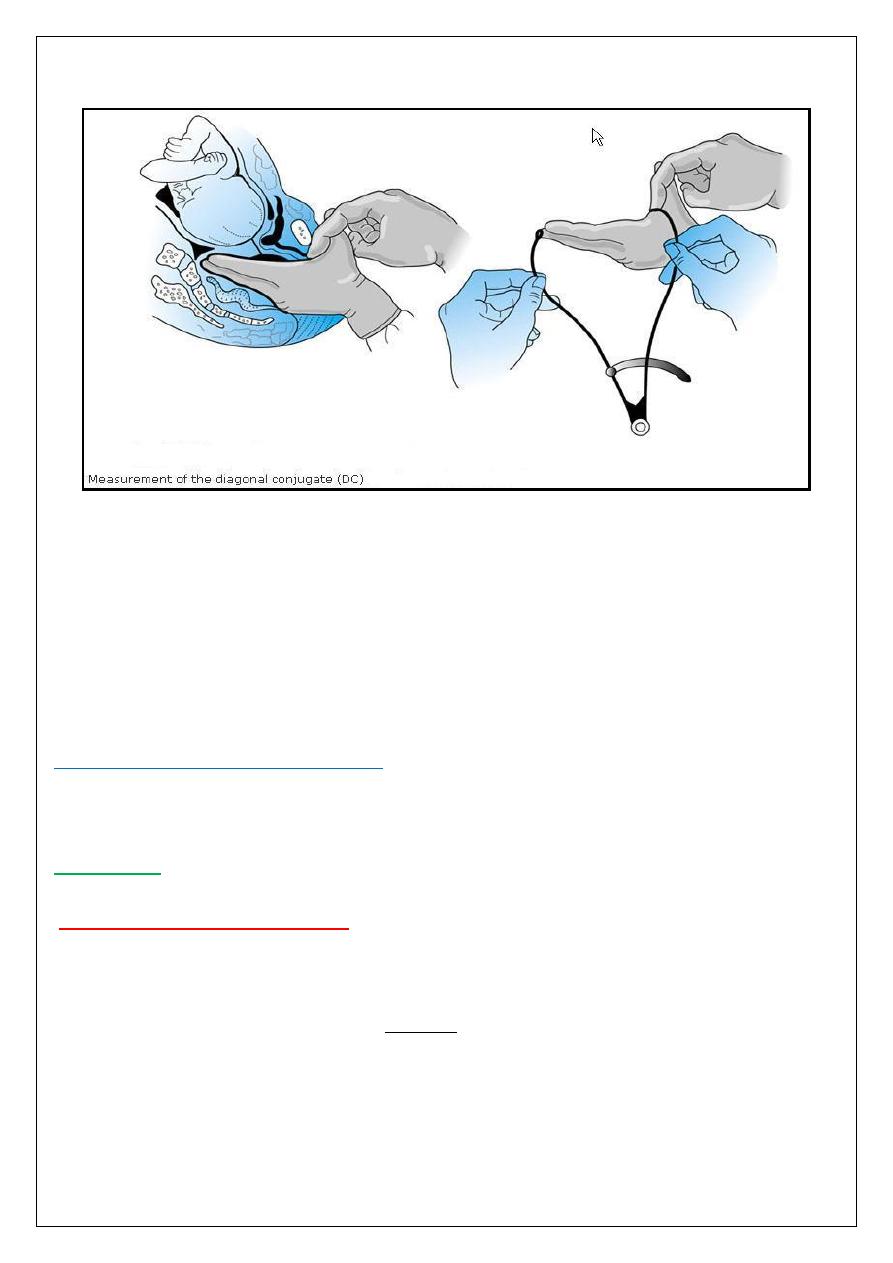
Clinical pelvimetry:
The diameters that can be assessed clinically are: the obstetric conjugate of the inlet by
clinical assessment of the diagonal conjugate when 2 fingers (index and middle) are passed
in the vagina and the index finger meets the pubis, the tip of the middle finger cannot meet
the promontory of the sacrum then we subtract 1.5-2 cm will corresponds the obstetric
conjugate (which is said to be adequate inlet).
8
Then the curvature of the sacrum is assessed by palpating its anterior surface.
Then the midpelvis is assessed but it is difficult to do it clinically unless the pelvic side walls
are apparently convergent which indicate narrow pelvic cavity, the bispinous dimension
also can be assessed by palpating the prominence of the spines, in addition the width of the
sacrosiatic notch should be assessed.
And the final step is the assessment of the outlet by placing a fist between the ischial
tuberosities, a dimension of 8.5 cm is adequate transverse diameter. And the subpubic arch
of less than 90 degrees usually associated with narrow midcavity and outlet.
Radiological assessment of the pelvis:
Is indicated when there is history of pelvic trauma or there is suspicion of pelvic
abnormalities, and the MRI is more preferable than XR.
Fetal skull:
Dimensions of the fetal skull:
The fetal head is the largest and the least compressible part of the fetus
The fetal skull consists of a base and a vault (cranium) which consists of the occipital,
parietal, frontal and temporal bones; these are easily compressible and interconnected by
membranes and these features allow molding to occur which means the overlap of these
bones under pressure and changing their shape to conform to maternal pelvis during
vaginal delivery.
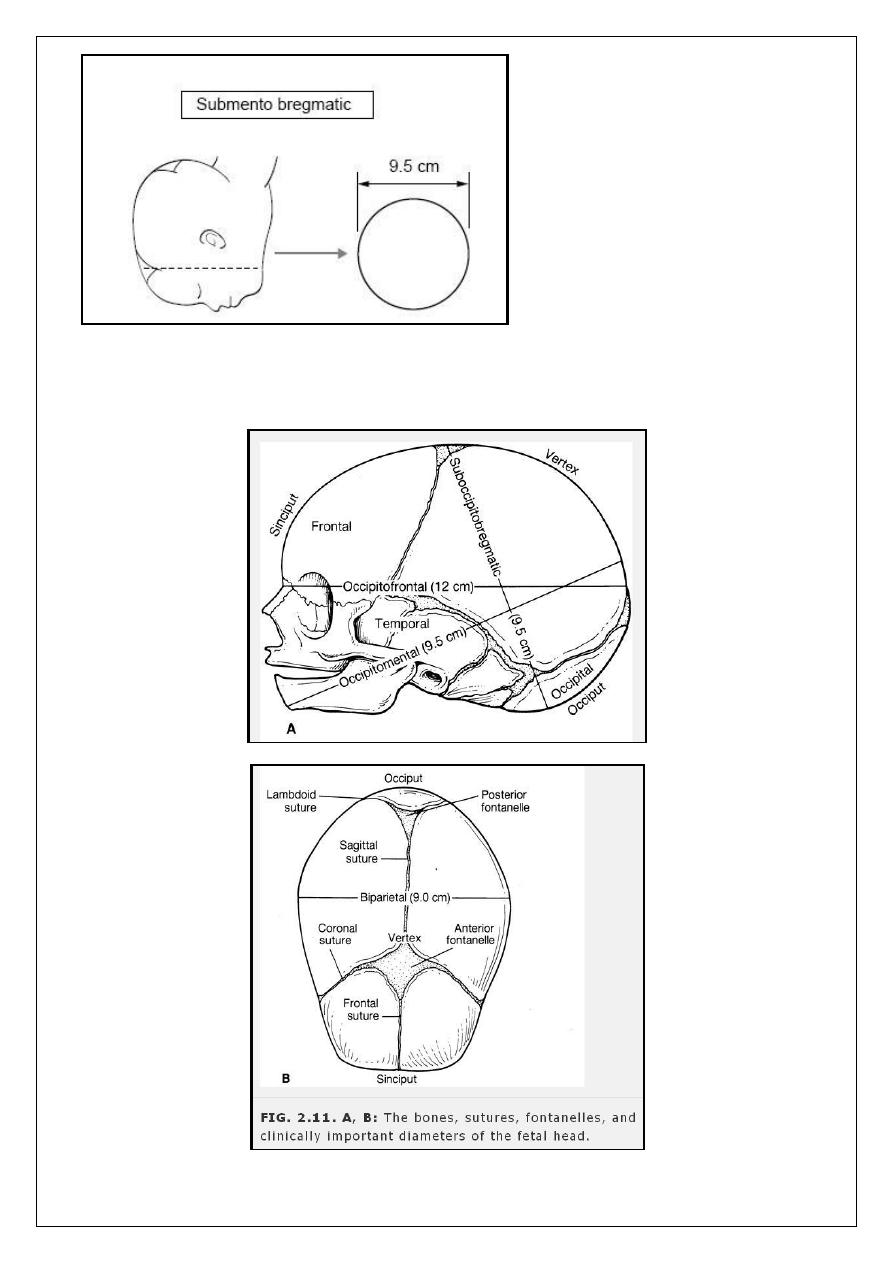
You have to know many terms: fontanelle [anterior (bregma) and posterior (lambda)],
nasion, glabella, vertex, and the occiput
9
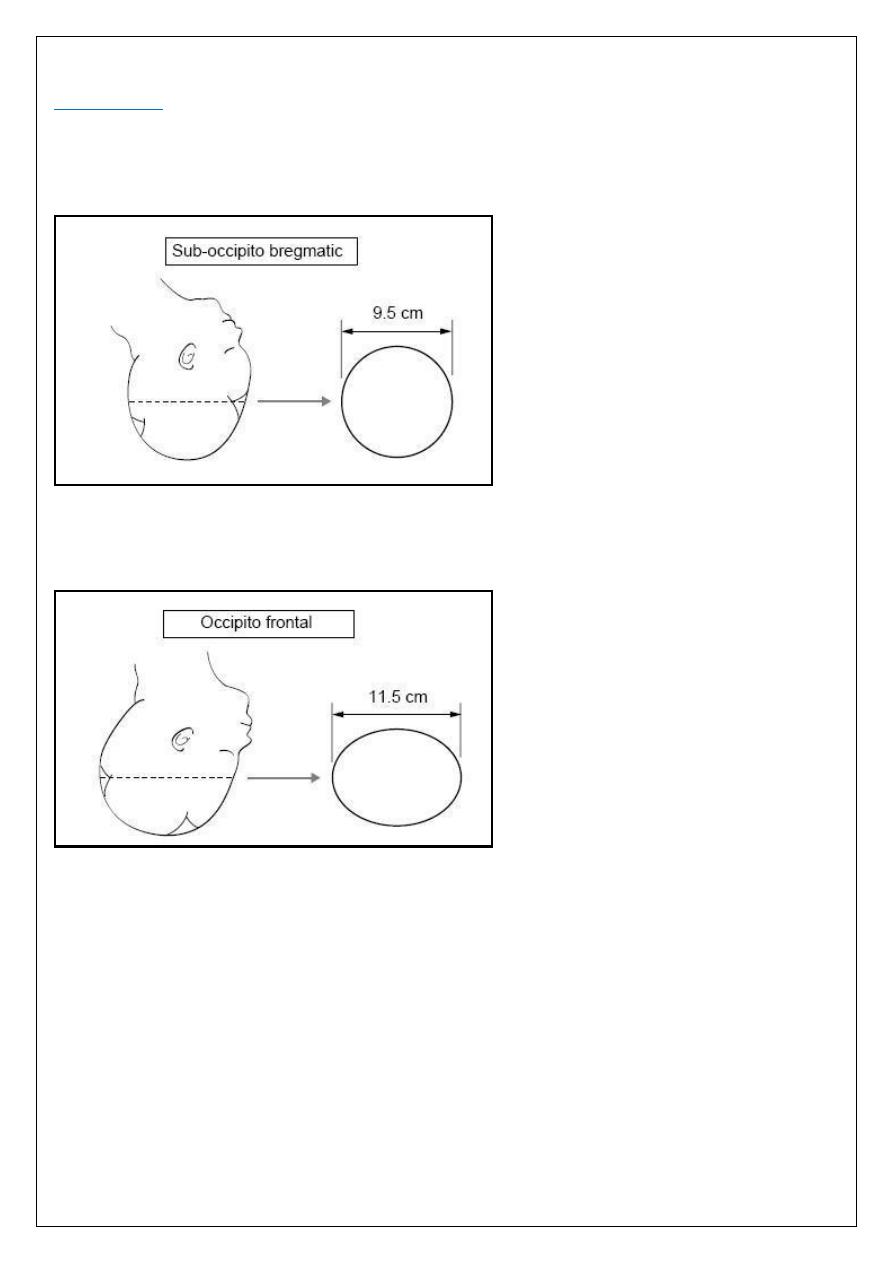
Diameters:
1*suboccipitobregmatic (9.5) cm this is the presenting anteroposterior diameter when the
head is well flexed. It extends from the undersurface of the occipital bone to the center of
the bregma.
2*Occipitofrontal (11-12) cm: when the head is deflexed. Extend from the external
protuberance of the occipital bone to the glabella.
3*Mentovertical (13.5) cm when the head is extended in brow presentation. It extends
from the vertex to the chin.
4*Submentobregmatic (9.5) cm when hyper extended head in the face presentation.it
extends from below the chin to the bregma.
10
The transverse diameters:
The biparietal (9.5) cm, and the bitemporal (8) cm diameters.