Approach to Anemia
TUCOM
Dep. of Medicine
5
th
year
Dr. Hasan I. Sultan
2- 10- 2018
Learning objectives
1. Review the normal structure and function of red blood
cell
2. Recognize the normal values for red blood cell
measurements and indices
3. Define anemia
4. Review the causes of anemia
5. Clarify the clinical assessment of anemic patient
6. Explain the investigations of anemia
7. List the types of anemia according to mean cell volume
(MCV) and low reticulocyte count
Normal red blood cell structure and function
The red blood cells (RBCs, erythrocytes) deliver oxygen to all
the tissues in the body and carry carbon dioxide back to the
lungs for excretion. The erythrocyte is uniquely adapted to
these functions.
Normal mature red cell circulate for about 120 days. It is a 8
μm non-nucleated, non-dividing cell, a biconcave disk shape
that maximizes the membrane surface area for gas
exchange, and it has a cytoskeleton and membrane
structure that allow it to deform sufficiently to pass through
the microvasculature.
About 98% of the cytoplasmic protein of the mature
erythrocyte is hemoglobin. The remainder is mainly
enzymatic proteins, such as those required for anaerobic
metabolism and the hexose monophosphate shunt.
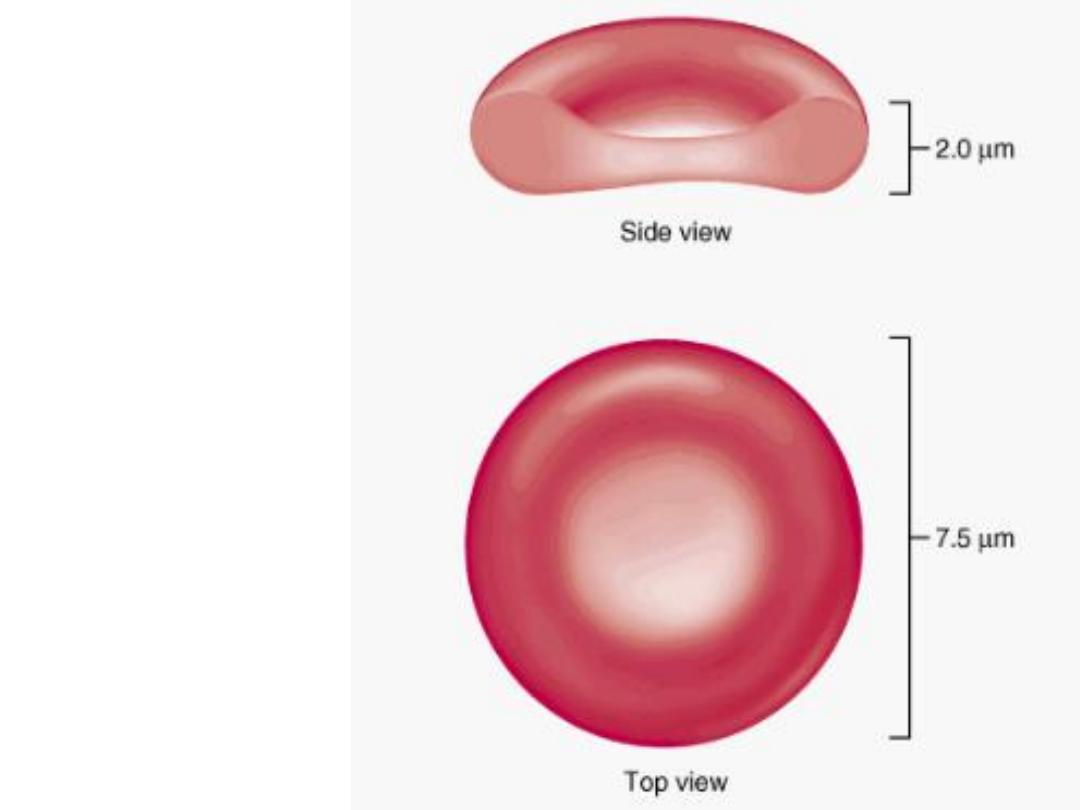
Normal shape of a
red blood cell
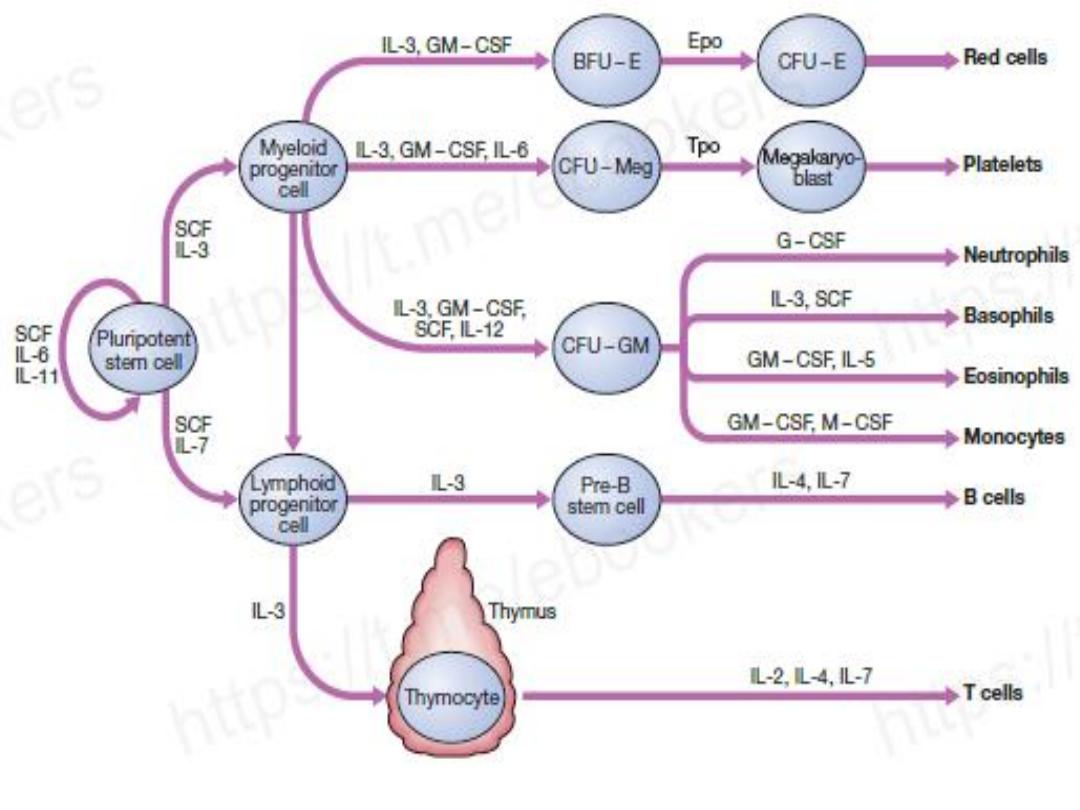
Stem cells and growth factors in haematopoietic cell development.
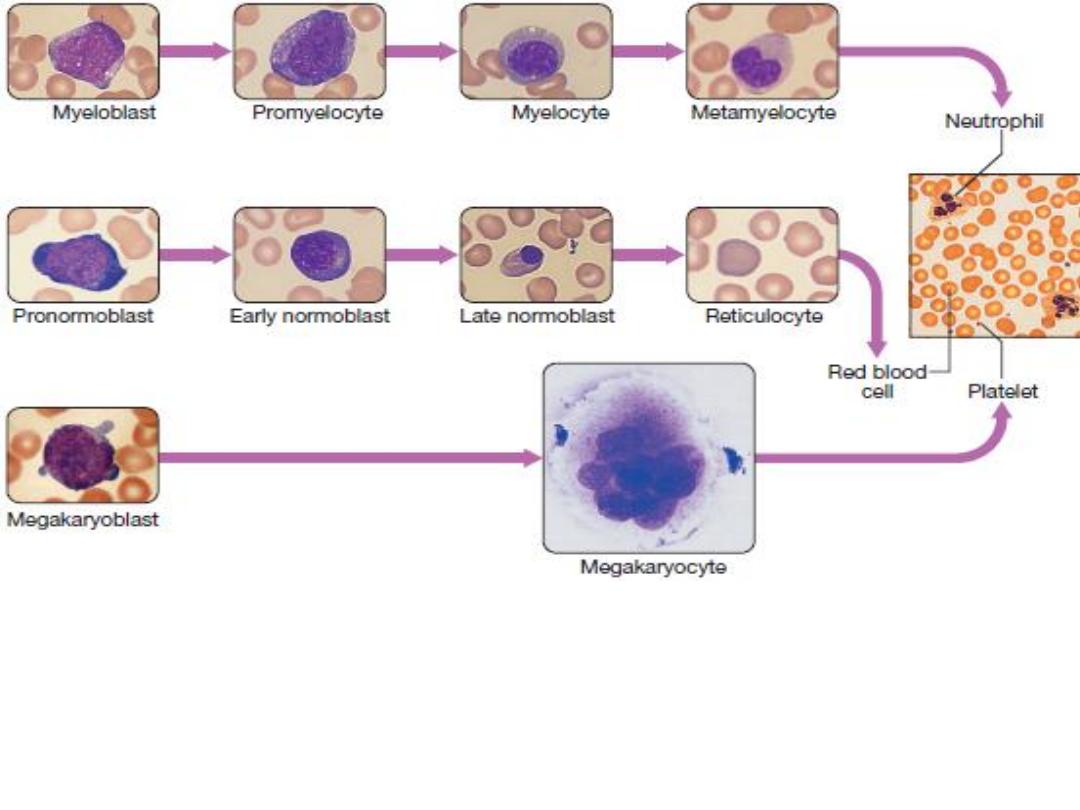
Red cell precursors formed in the bone marrow from the erythroid (CFU–E)
progenitor cells are called erythroblasts or normoblasts. The first non-nucleated red
cell is a reticulocyte, which still contains ribosomal material in the cytoplasm, giving
these large cells a faint blue tinge (‘polychromasia’). Reticulocytes lose their
ribosomal material and mature over 3 days, during which time they are released into
the circulation.
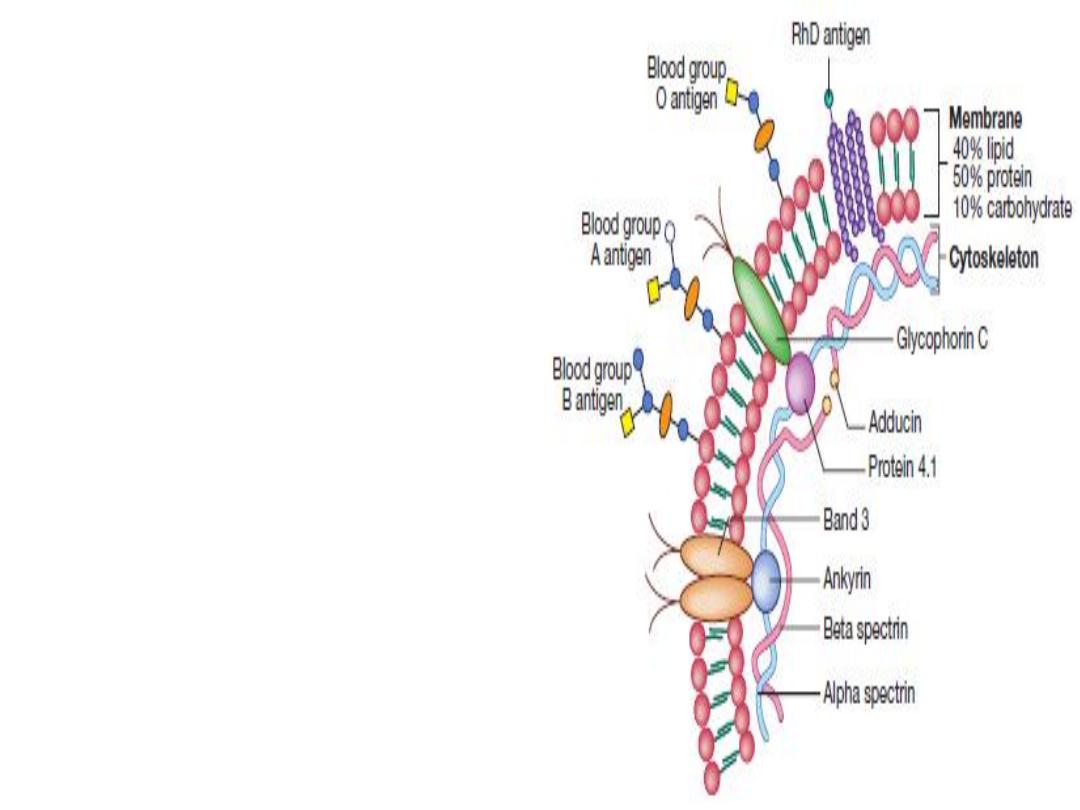
Red cell membrane (lipid bilayer)
flexibility is conferred by
attachment of cytoskeletal
proteins, in order to:
• Pass through the smallest
capillaries
• Prevent osmotic destruction in
the pulmonary and renal
circulation
Red cell membrane also carry the
antigens for ABO blood group and
Rhesus system.
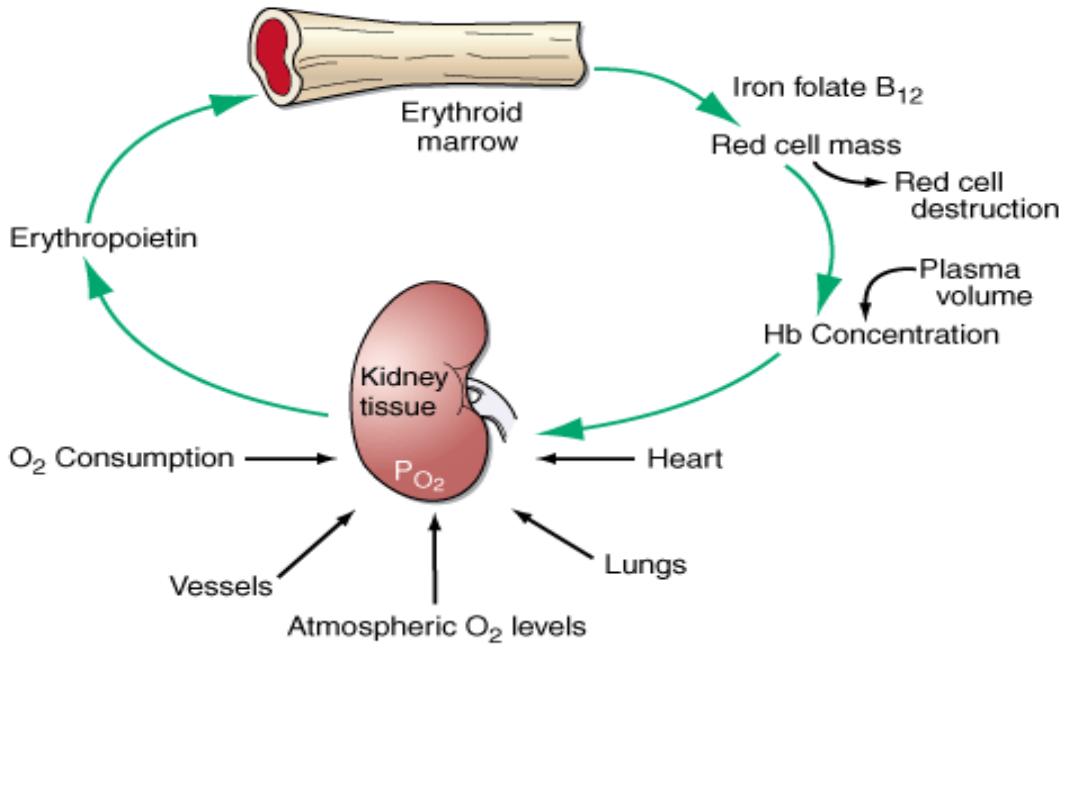
Proliferation and differentiation of red cell precursors is stimulated by
erythropoietin, a polypeptide hormone produced by renal interstitial
peritubular cells in response to hypoxia.
Anemia
Anemia refers to a state in which the level of hemoglobin in
the blood is below the reference range appropriate for age
and sex. It is not a disease but it is an important sign of
different underlying diseases.
Causes of anemia
Decreased or ineffective
marrow production
• Lack of iron, vitamin B12 or
folate
• Hypoplasia/myelodysplasia
• Invasion by malignant cells
• Renal failure
• Anemia of chronic disease
Normal marrow production
but increased removal of
cells
• Blood loss
• Hemolysis
• Hypersplenism
Measurement
Unit
Normal Range
Hemoglobin
g/dL
Males: 13.5–17.5
Females: 12–16
Hematocrit
%
Males: 40–52
Females: 36–48
Red blood cell (RBC) count
× 10
6
/μL of blood Males: 4.5–6.0
Females: 4.0–5.4
Mean cell volume (MCV)
fL
78–98
Mean cell hemoglobin (MCH)
pg
29–33
Mean cell hemoglobin concentration
(MCHC)
g/dL
30–36
Red blood cell size distribution width
RDW-CV
%
12–14
RDW-SD
fL
37–47
Reticulocyte count (absolute number) No./μL of blood
40,000–100,000
Reticulocyte percentage
% of RBCs
0.5–1.5
Normal values for red blood cell measurements
Age/Sex
Hemoglobin g/dL
Hematocrit %
At birth
17
52
Childhood
12
36
Adolescence
13
40
Adult man
16 (±2)
47 (±6)
Adult woman
(menstruating)
13 (±2)
40 (±6)
Adult woman
(postmenopausal)
14 (±2)
42 (±6)
During pregnancy
12 (±2)
37 (±6)
Changes in Normal Hemoglobin/Hematocrit Values with Age
and Pregnancy
Clinical presentation
The clinical presentation of anemia depend on its severity
and the underlying cause.
• Acute anemia: due to acute hemorrhage or massive
hemolysis may exhibit symptoms of hypovolemic shock.
• Chronic anemia: most common, patients complaints are
fatigue, pallor, dizziness, headache, decreased exercise
tolerance, dyspnea, and palpitations. In patients with
coronary artery disease, anemia may precipitate angina.
History:
• Gastrointestinal history, menstrual history or recent
pregnancy are to important to looking for iron deficiency
anemia (which is the most common type of anemia
worldwide).

• A dietary history should assess the intake of iron and
folate, which may become deficient e.g. in pregnancy or
during periods of rapid growth.
• Past medical history: such as rheumatoid arthritis
(anaemia of chronic disease), chronic diarrhea or previous
surgery (e.g. resection of the stomach or small bowel,
which may lead to malabsorption of iron and/or vitamin
B12).
• Family history and ethnic background: such as the
haemoglobinopathies and hereditary spherocytosis.
• A drug history may reveal the ingestion of drugs which
cause blood loss (e.g. aspirin and antiinflammatory
drugs), haemolysis (e.g. sulphonamides) or aplasia (e.g.
chloramphenicol).
• Recent significant weight loss.

On examination:
General physical findings of anemia
• Pallor: of mucous membranes and conjunctiva (Hb < 9 g/dl) or skin
creases (Hb < 7 g/dl)
• Tachycardia, systolic flow murmur, wide pulse pressure or features
of heart failure
• Rectal digital examination to look for GI bleeding.
Specific findings related to the aetiology of the anemia, for
example:
• Spooning of the fingernails (koilonychia) due to iron deficiency
anemia. Glossitis due to iron, folate and vitamin B12 deficiency.
• Right iliac fossa mass due to an underlying caecal carcinoma.
• Hemolytic anemia can cause jaundice.
• Vitamin B12 deficiency may be associated with neurological signs,
including peripheral neuropathy, dementia and signs of subacute
combined degeneration of spinal cord.
• Sickle-cell anemia may result in leg ulcers, stroke or features of
pulmonary hypertension.
• Splenomegaly, lymphadenopathy and hemorrhagic skin rash due to
hematological diseases.
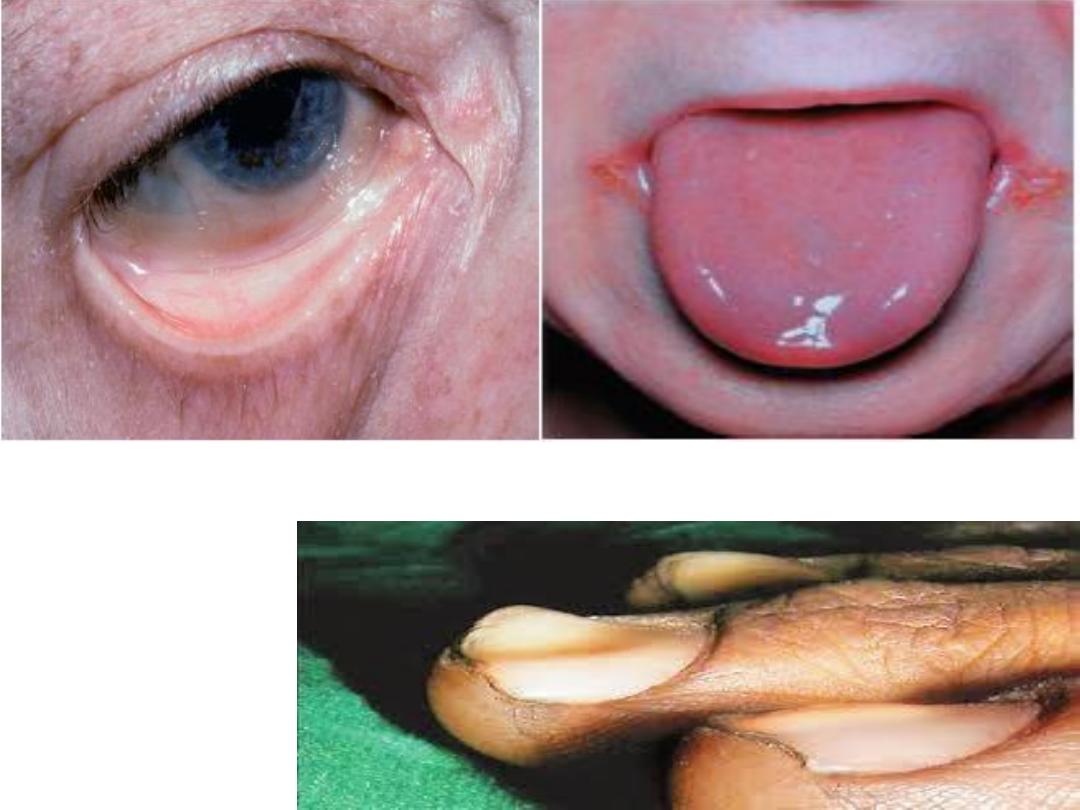
Smooth red tongue and angular
stomatitis
koilonychia
Conjunctival pallor

Chronic anemia. Pallor of the hand in anemia is obvious in this patient, especially
when compared with the physician's hand on the right. The patient's hemoglobin
concentration was 7 g/dL. The hand also shows that the patient was a heavy smoker.
His anemia resulted from chronic blood loss from a carcinoma in the esophagus, a
site where the risk for carcinoma is increased in smokers.
Investigations
1- Complete Blood Counts:
Hemoglobin level and
hematocrit, RBC indices and RDW, WBC count and
differential, platelet count, and reticulocyte count and
percentage.
A- Red blood cell indices:
Index
Normal Value
Mean cell volume (MCV) = (hematocrit x 10)/(red cell
count x 10
6
)
78- 98 fL
Mean cell hemoglobin (MCH) = (hemoglobin x
10)/(red cell count x 10
6
)
29- 33 pg
Mean cell hemoglobin concentration (MCHC) =
(hemoglobin x 10)/hematocrit, or MCH/MCV
30- 36 g/dL

Microcytosis is reflected by a lower than normal MCV (<78
fl), whereas high values (>98 fl) reflect macrocytosis.
Decrease in MCH and MCHC reflect defects in hemoglobin
synthesis (hypochromia).
B- Red cell distribution width (RDW):
is the measurement of
variability of red cell volume or size (anisocytosis). RDW can
be reported statistically as coefficient of variation (CV)
and/or standard deviation (SD), RDW-CV and/or RDW-SD,
respectively.
• It aids in distinguishing between iron deficiency anemia
(elevated RDW, low MCV) and thalassemia (normal RDW,
low MCV); however, definitive tests are required.
• It can also help distinguish between megaloblastic anemia
such as folate or vitamin B12 deficiency anemia (elevated
RDW, high MCV) and other causes of macrocytosis (often
normal RDW, high MCV).

C- The reticulocyte count:
allows the critical distinction
between anemia arising from a primary failure of red cell
production (reticulocyte count not elevated) and anemia
resulting from increased red cell destruction or bleeding
(reticulocyte count more than 2%).
2- Peripheral Blood Smear:
it is complementary to the red
cell indices, it may reveals variations in cell size
(anisocytosis) and shape (poikilocytosis) and polychromasia
(increase reticulocytes). The appearance of nucleated red
cells, Howell-Jolly bodies, target cells, sickle cells, and others
may provide clues to specific disorders. In addition,
examination of myeloid cells and platelets may also be
helpful. Hypersegmented neutrophils and large platelets
support the diagnosis of megaloblastic anemia, and the
presence of immature blast forms may be diagnostic of
leukemia.
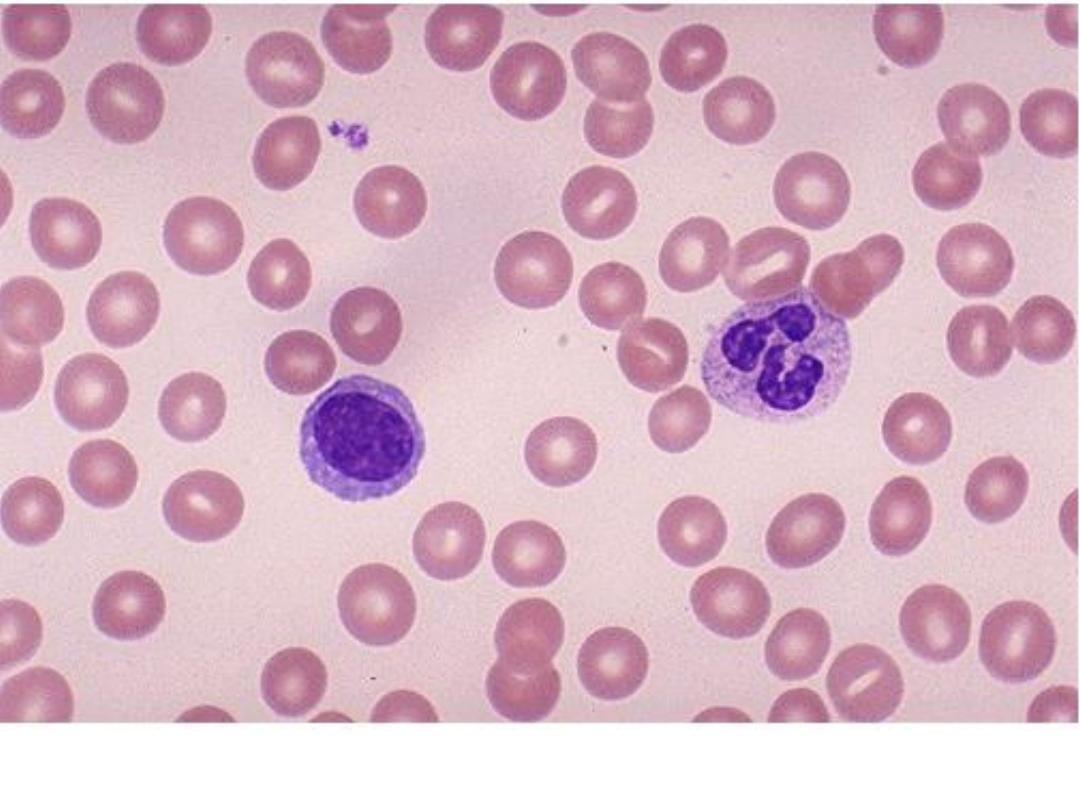
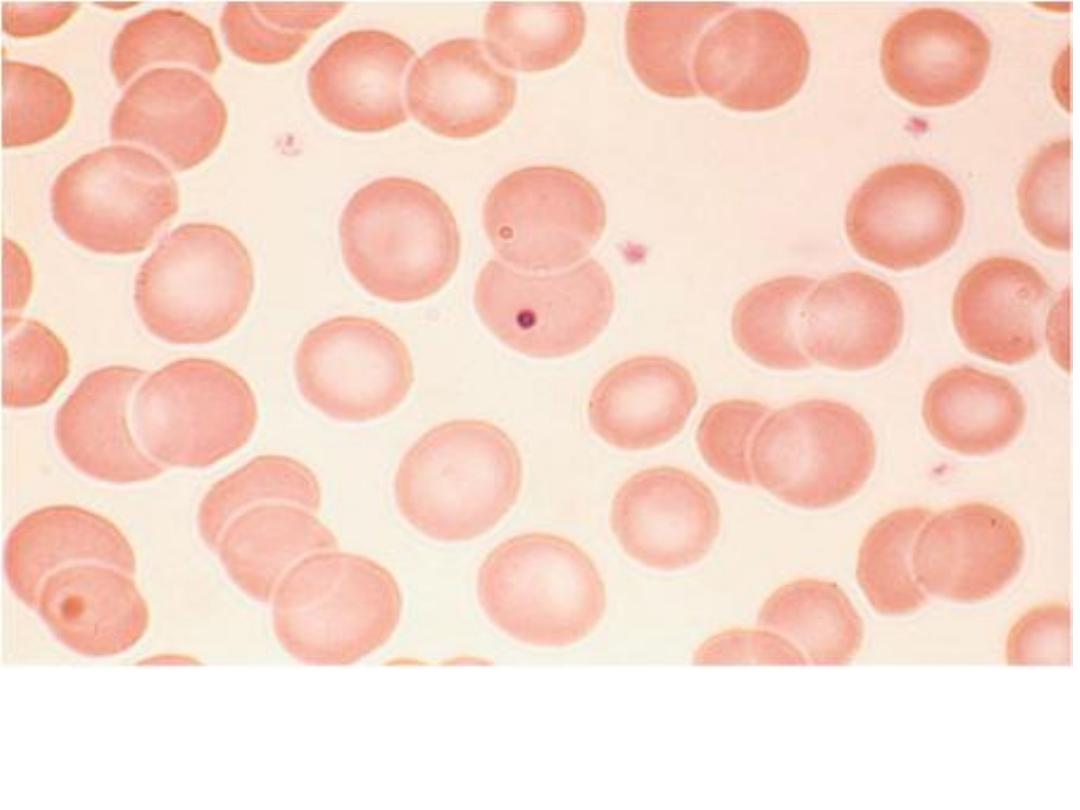
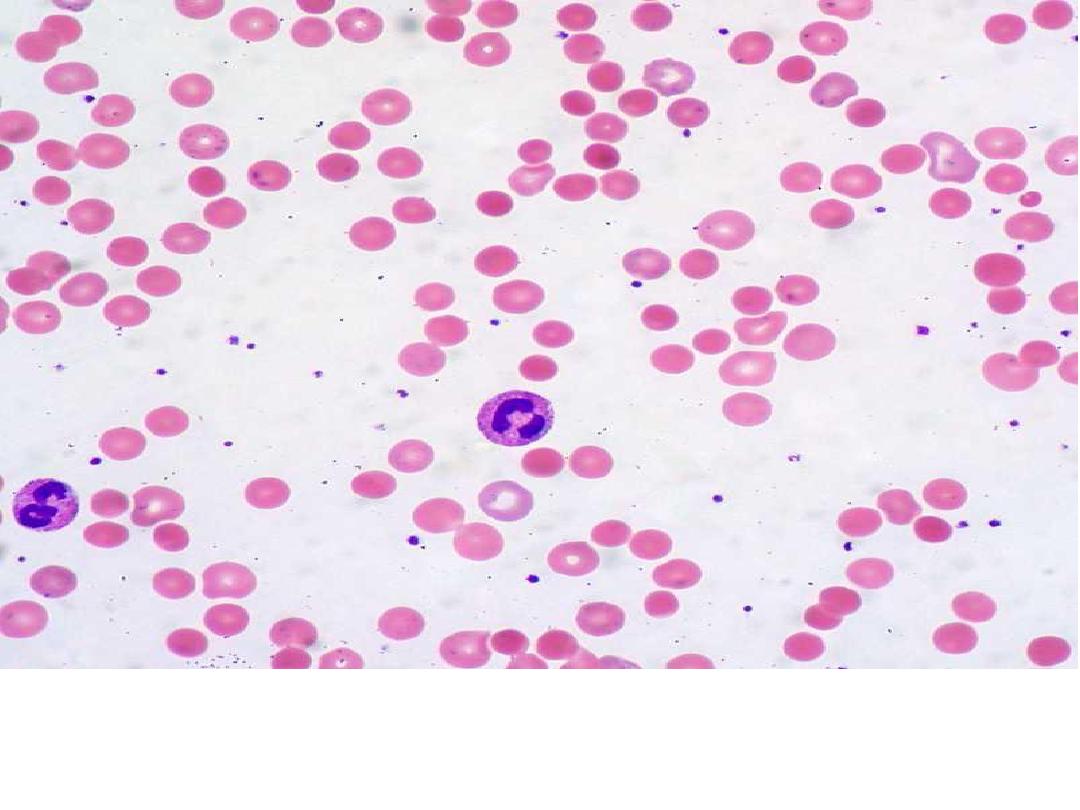
A normal peripheral blood smear indicates the appropriate appearance of red blood
cells, with a zone of central pallor occupying about 1/3 of the size of the RBC.

Normal blood smear (Wright's stain). High-power field showing normal
red cells, a neutrophil, and a few platelets.
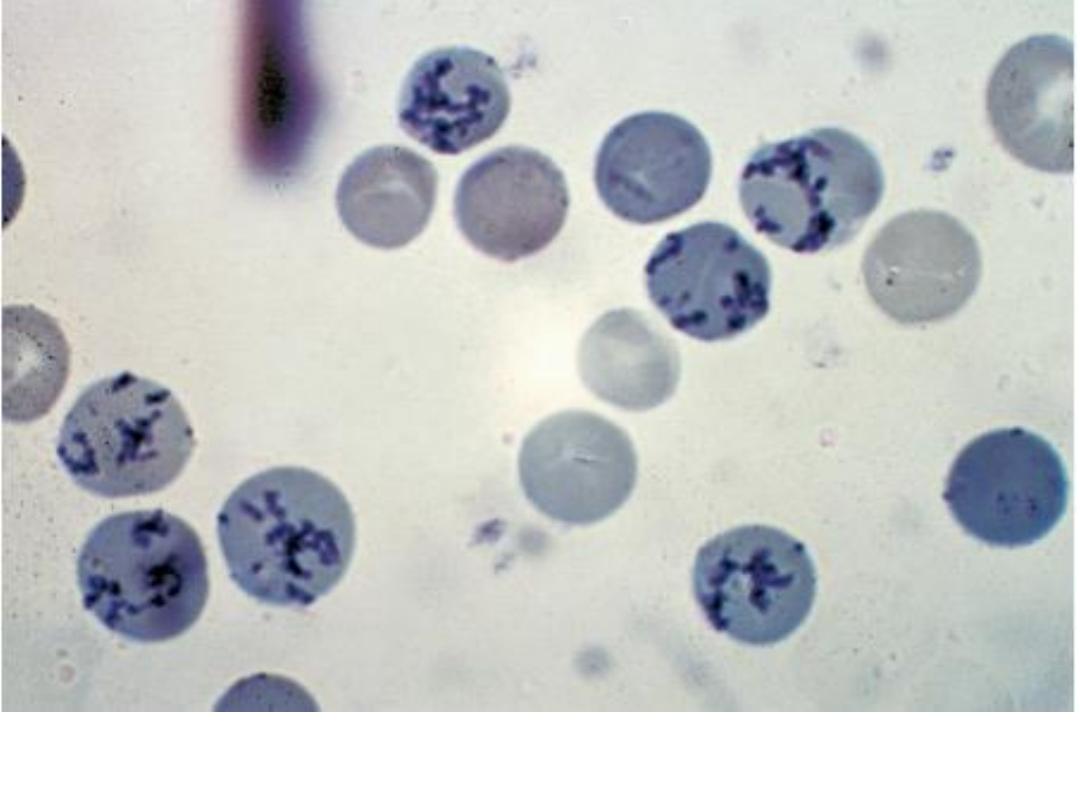
Reticulocytes. Methylene blue stain demonstrates residual RNA in
newly made red cells.
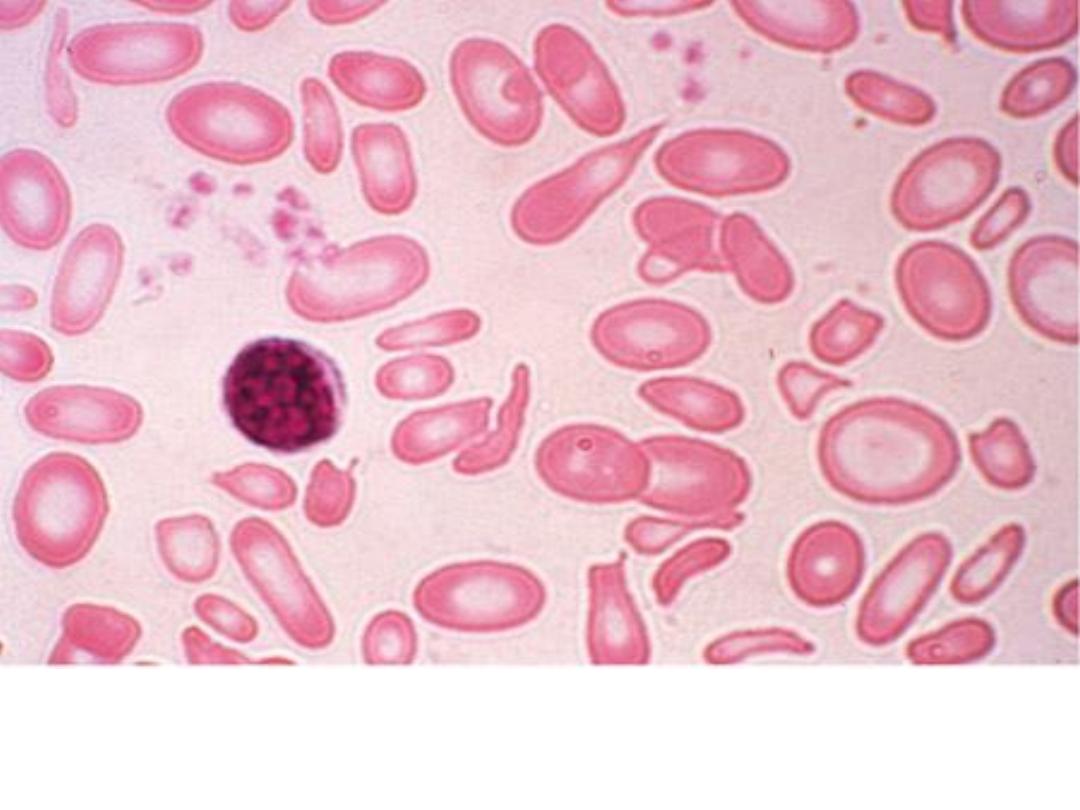
Severe iron-deficiency anemia. Microcytic and hypochromic red cells
smaller than the nucleus of a lymphocyte associated with marked
variation in size (anisocytosis) and shape (poikilocytosis).
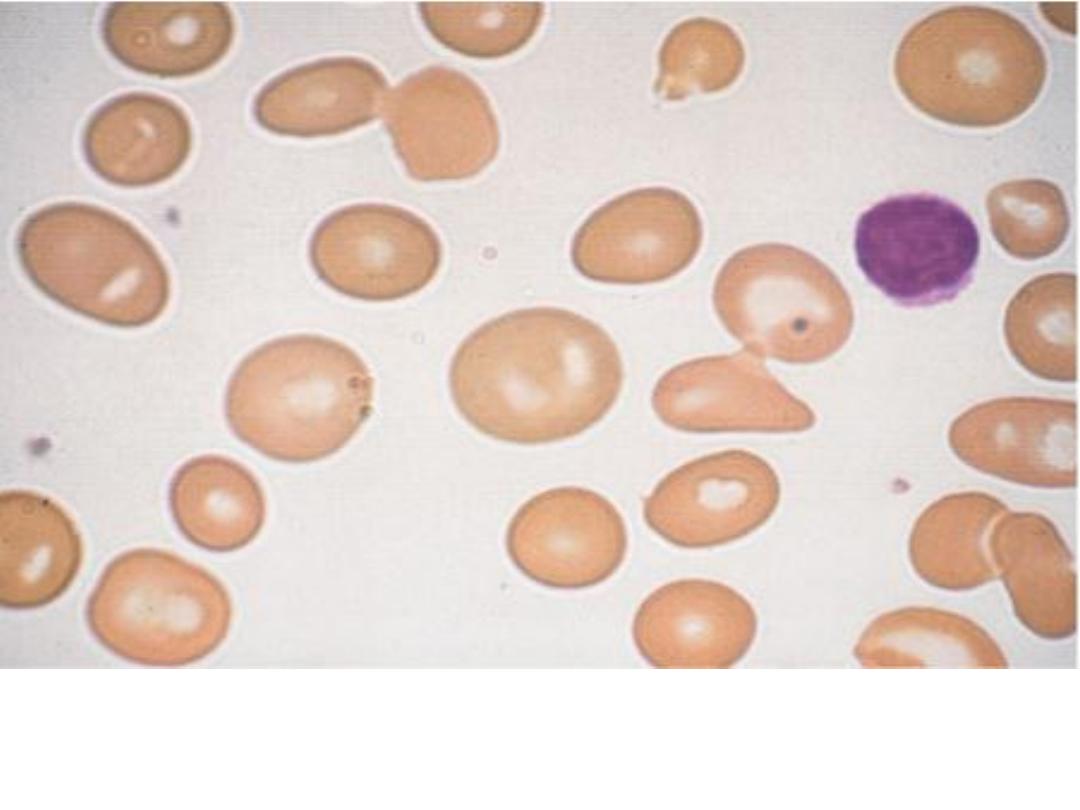
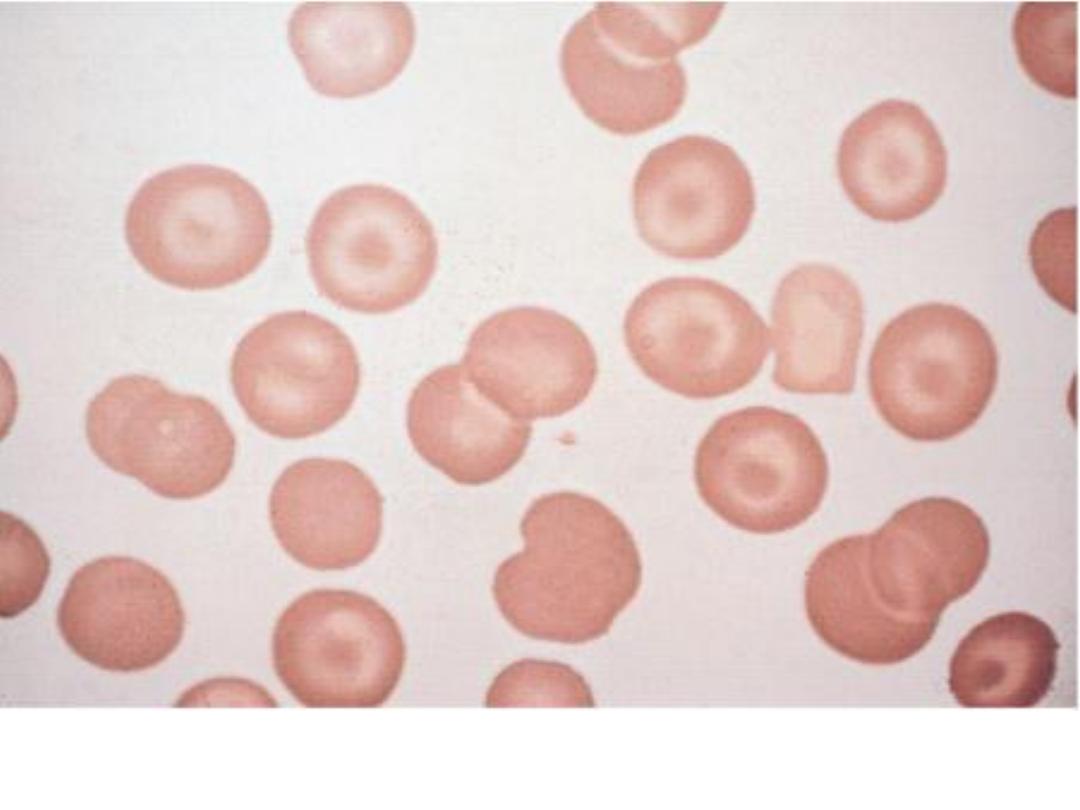
Macrocytosis. Red cells are larger than a small lymphocyte and well
hemoglobinized. Often macrocytes are oval-shaped
(macroovalocytes).
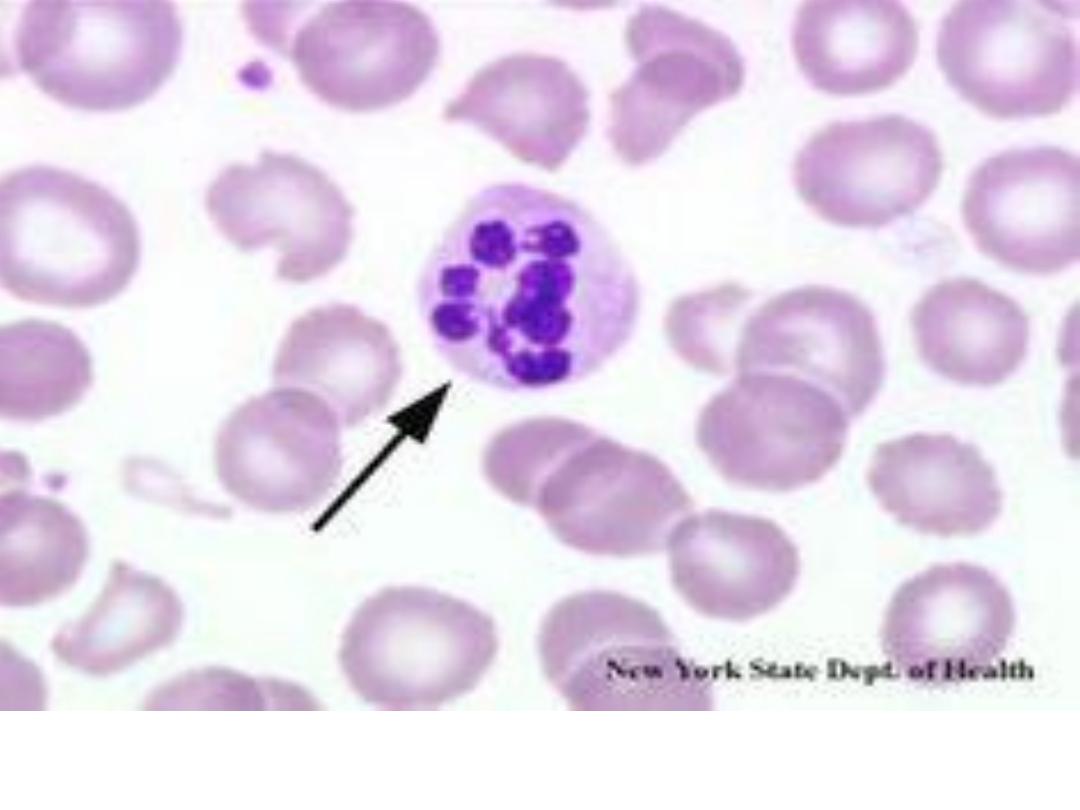
Peripheral blood smear showing hypersegmented neutrophils,
characteristic of megaloblastic anemia.
Howell-Jolly bodies. In the absence of a functional spleen, nuclear
remnants are not culled from the red cells and remain as small
homogeneously staining blue inclusions on Wright stain.
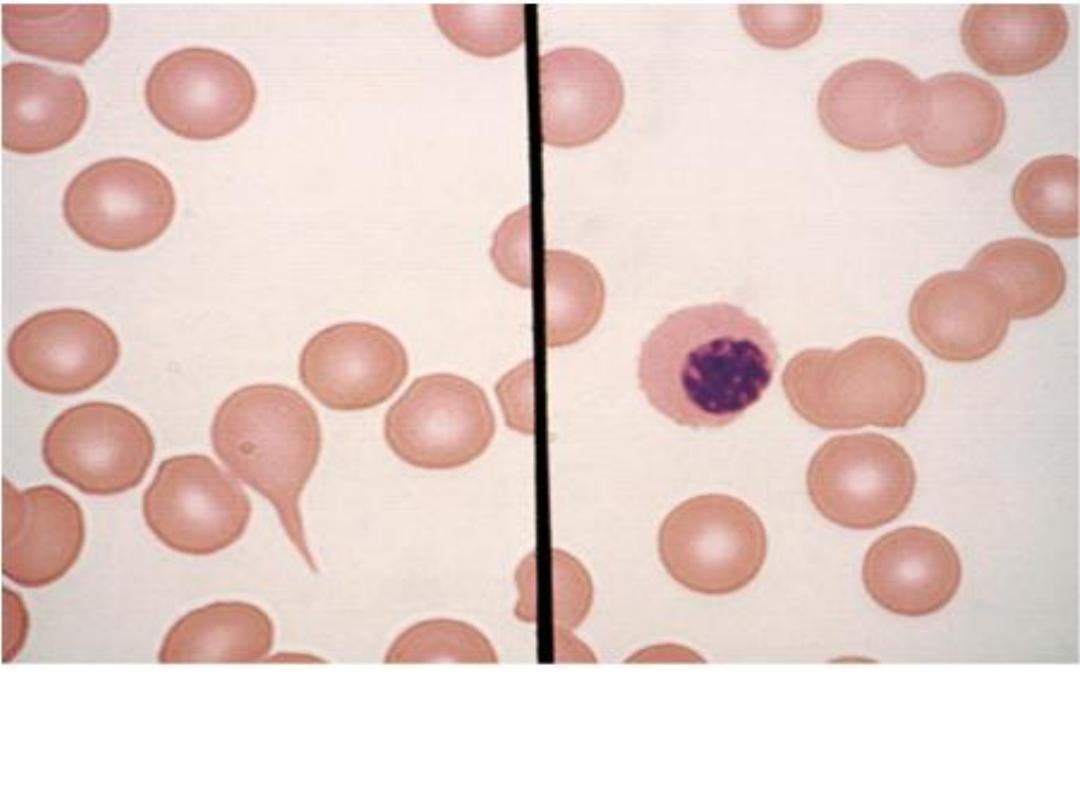
Red cell changes in myelofibrosis. The left panel shows a teardrop-
shaped cell. The right panel shows a nucleated red cell. These forms
are seen in myelofibrosis with extramedullary hematopoiesis.
Target cells. Target cells have a bull's-eye appearance and are seen in
thalassemia and in liver disease.
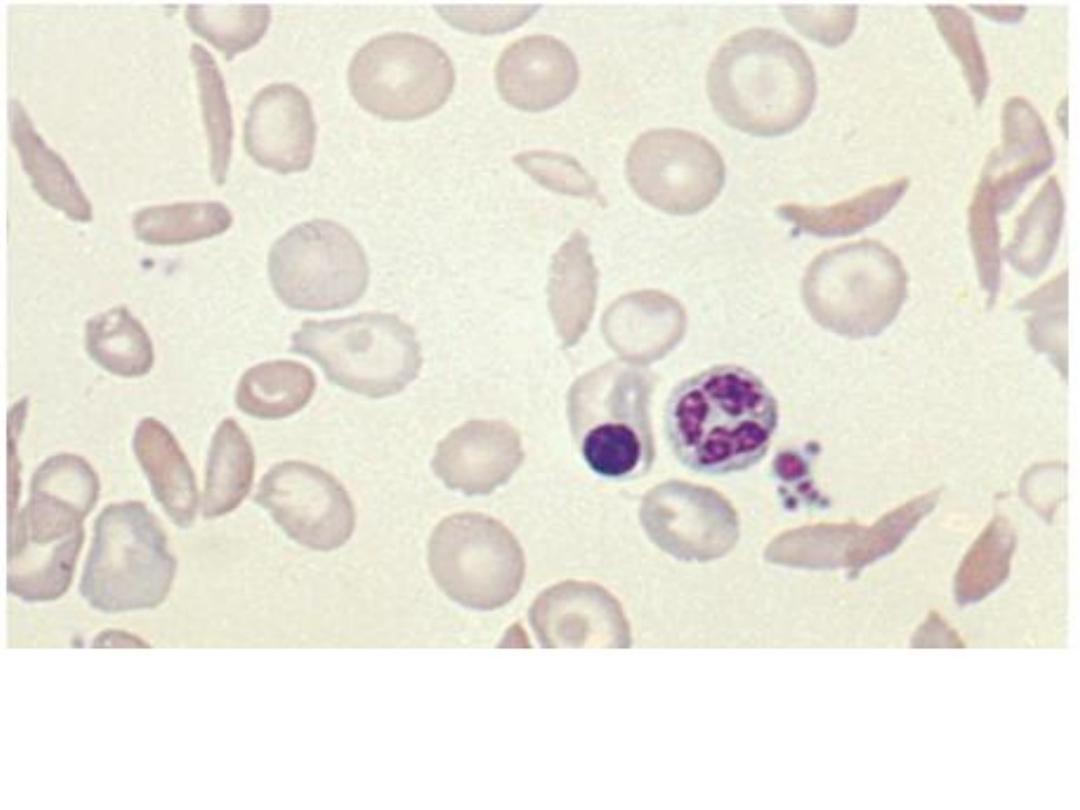
Sickle cell anemia. The elongated and crescent-shaped red blood cells
seen on this smear represent circulating irreversibly sickled cells.
Target cells and a nucleated red blood cell are also seen.
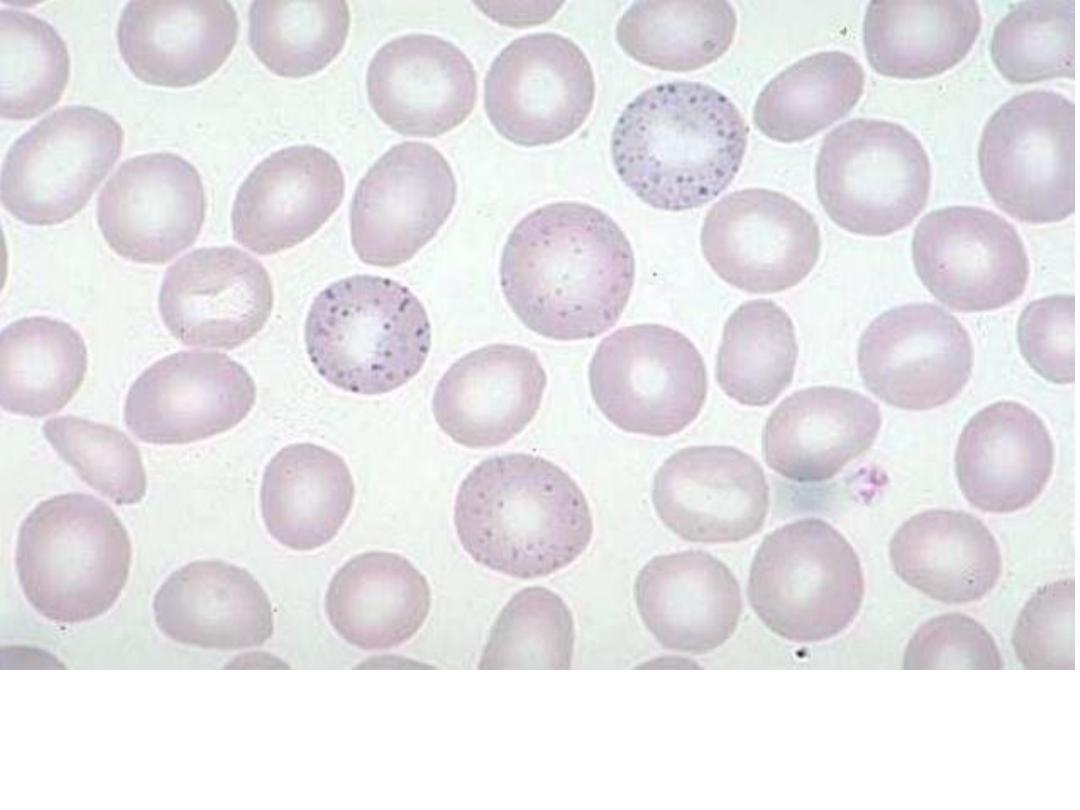
Basophilic stippling: refers to erythrocytes display small dots at the
periphery (visualized ribosomal aggregates) seen in lead poisoning and
thalassemia.
Spherocytosis: the red blood cells (RBCs) are sphere-shaped, rather
than bi-concave disk shaped. Spherocytes are found in hereditary
spherocytosis and autoimmune hemolytic anemia
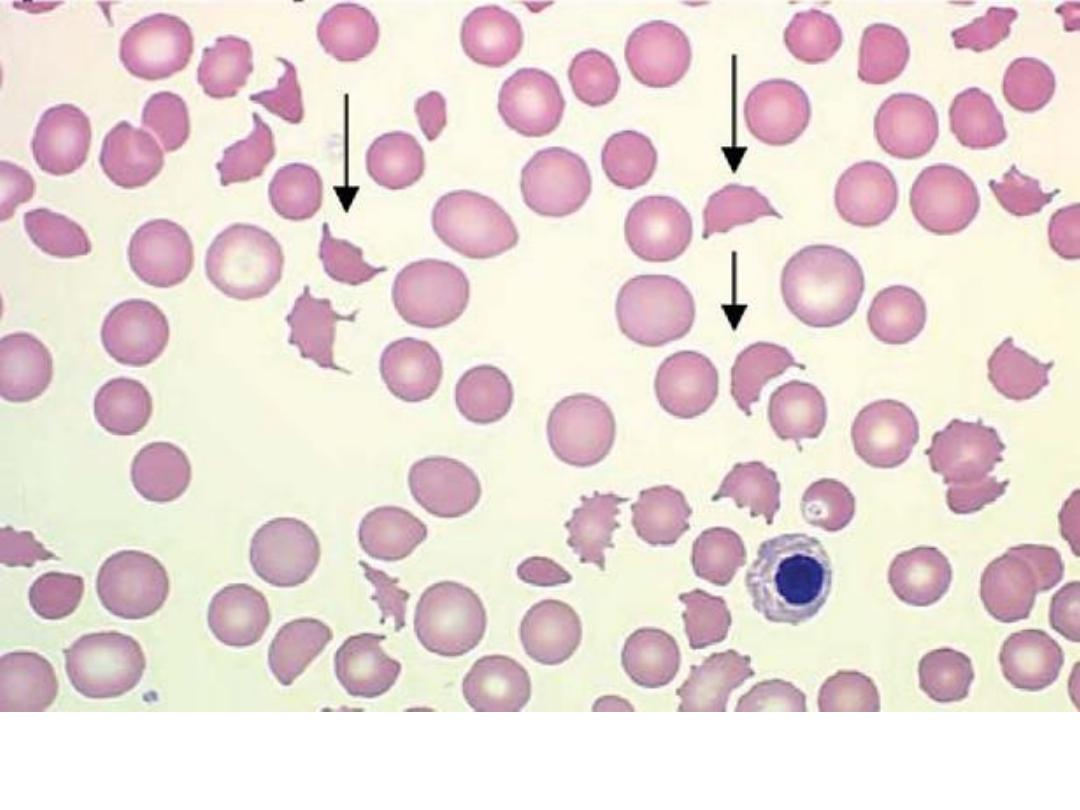
Microangiopathic hemolytic anemia: A nucleated red blood cell is seen
with the fragmented red cells and spherocytes.

3- Other blood tests for:
• Iron: serum iron, the TIBC, the percent transferrin saturation
and serum ferritin.
• Vitamin B12 and folate serum levels.
• Indirect bilirubin.
• Direct Coomb’s test.
• Haptoglobin levle.
• Osmotic fragility test.
• Hemoglobin electrophoresis.
• RBC enzyme studies
4- Occult blood in stool.
5- Bone Marrow Examination:
Marrow examination can diagnose primary marrow disorders
such as myelofibrosis, a red cell maturation defect, or an
infiltrative disease. Marrow biopsy can be stained for the
presence of iron stores.
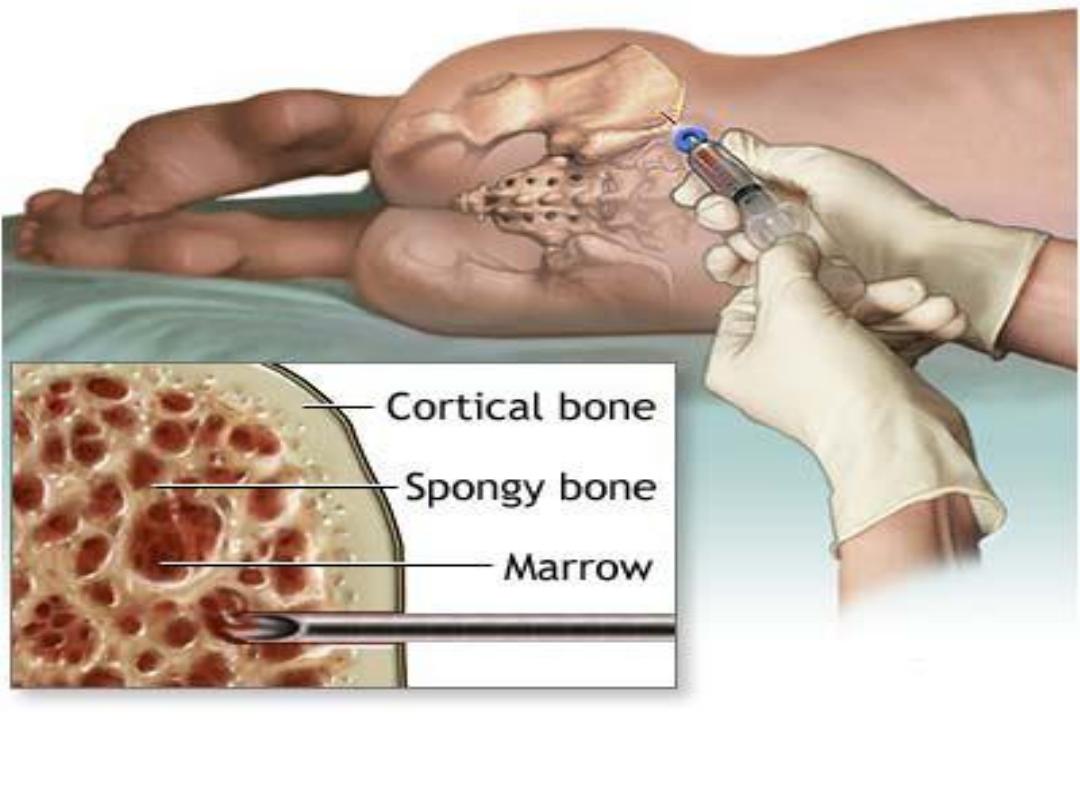
Bone marrow aspiration and trephine biopsy are usually performed on
the back of the hip bone on posterior iliac crest.
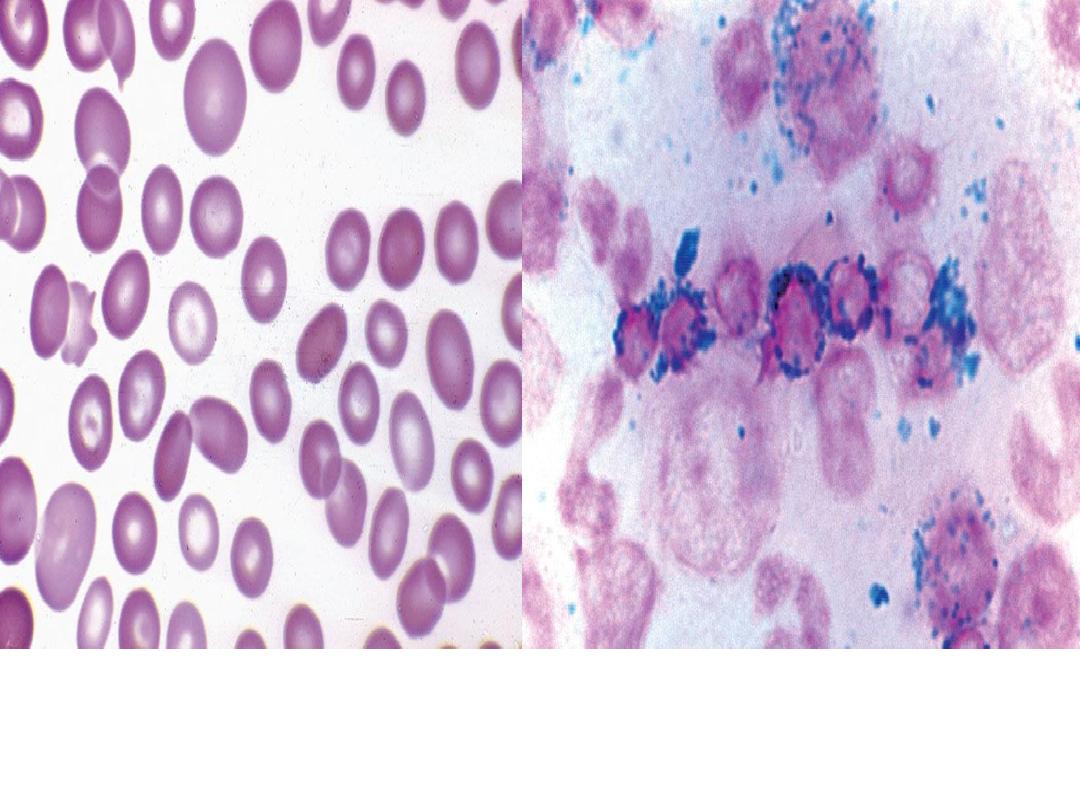
Refractory anaemia with ring
sideroblasts. Blood smear with
dimorphic red blood cells and
macrocytes
Refractory anaemia with ring sideroblasts.
Iron stain of bone marrow aspirate
showing numerous ring sideroblasts
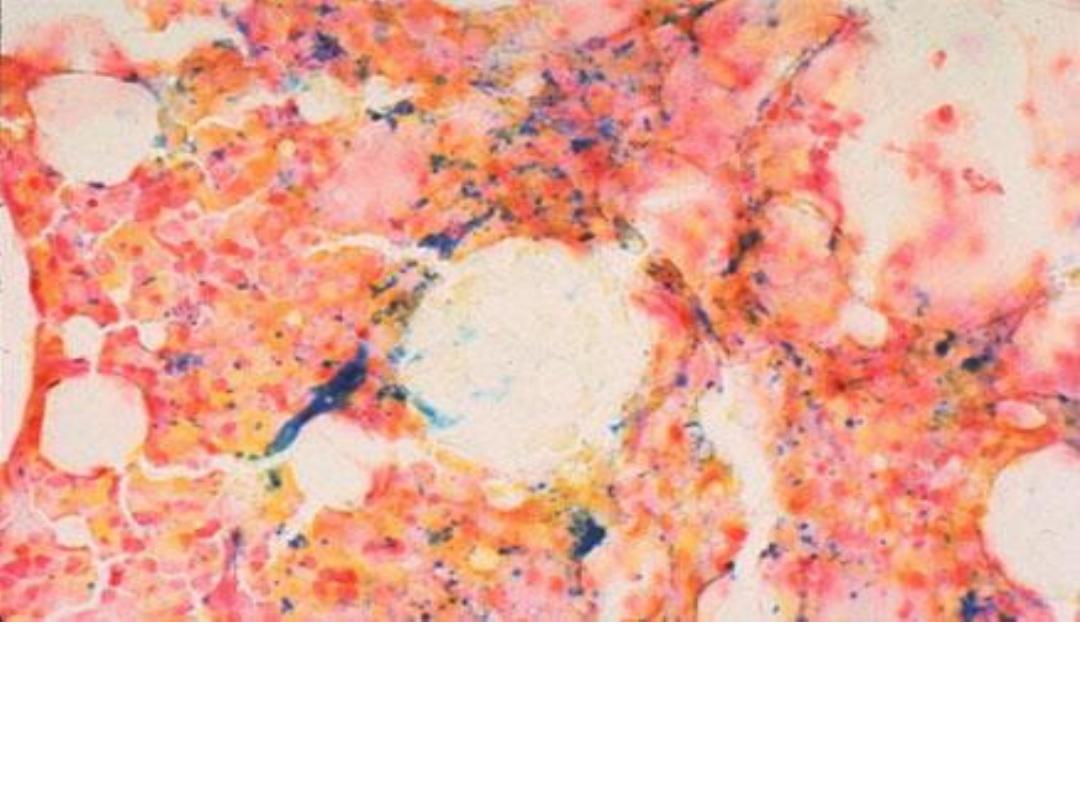
Prussian blue stain for iron in a normal bone marrow (the blue staining
material is iron within the reticuloendothelial cells in bone marrow).
Iron deficiency anemia will develop following depletion of iron stores
from the bone marrow.
Differential diagnosis of anemia according to MCV with low
reticulocyte count
Microcytic Anemia (MCV <
78 fl)
• Iron deficiency
• Thalassemia minor
• Anemia of chronic disease
• Sideroblastic anemia
• Lead poisoning
Macrocytic Anemia (MCV > 98
fl)
Megaloblastic Anemias
• Folate deficiency
• Vitamin B12 deficiency
• Drug-induced megaloblastic
anemia
• Myelodysplasia
Nonmegaloblastic Macrocytosis
• Liver disease
• Hypothyroidism
• Reticulocytosis
Normocytic Anemia (MCV 78-
98 fl)
• Early iron deficiency
• Aplastic anemia
• Endocrinopathies
• Anemia of chronic disease
• Anemia of renal failure
• Mixed nutritional deficiency
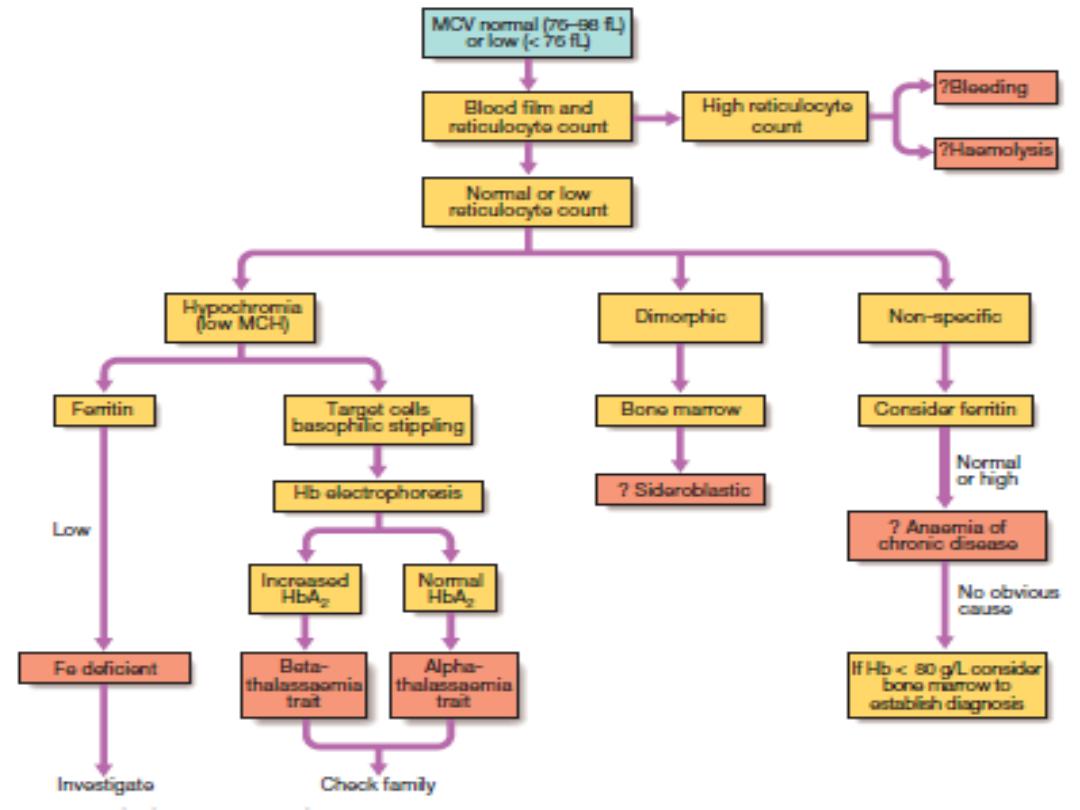
Investigation of anemia with
normal or low MCV.
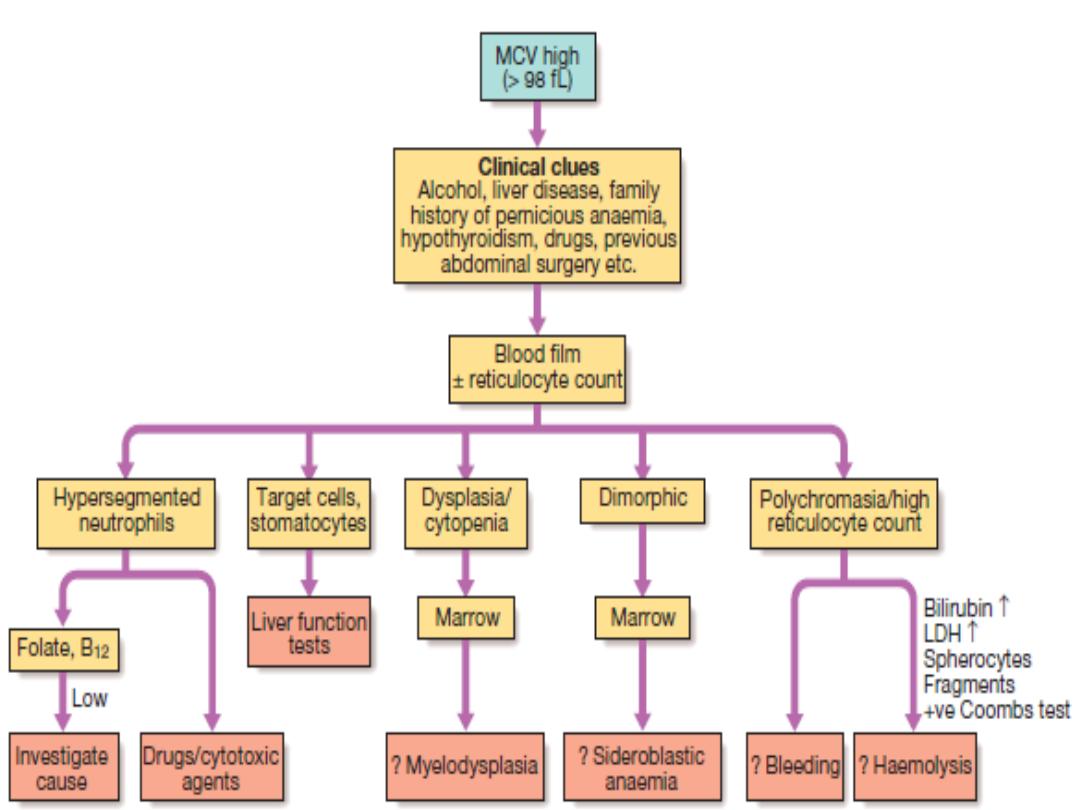
Investigation of anaemia with
high MCV. (LDH = lactate
dehydrogenase)

Thanks