Venous Thromboembolism
Deep Venous Thrombosis
And
Pulmonary Embolism
D o n e b y :
D R . M A R W A N M I B R A H I M
C A B M I N T E R N A L M E D I C I N E
F I C M R E S P I R A T O R Y M E D I C I N E

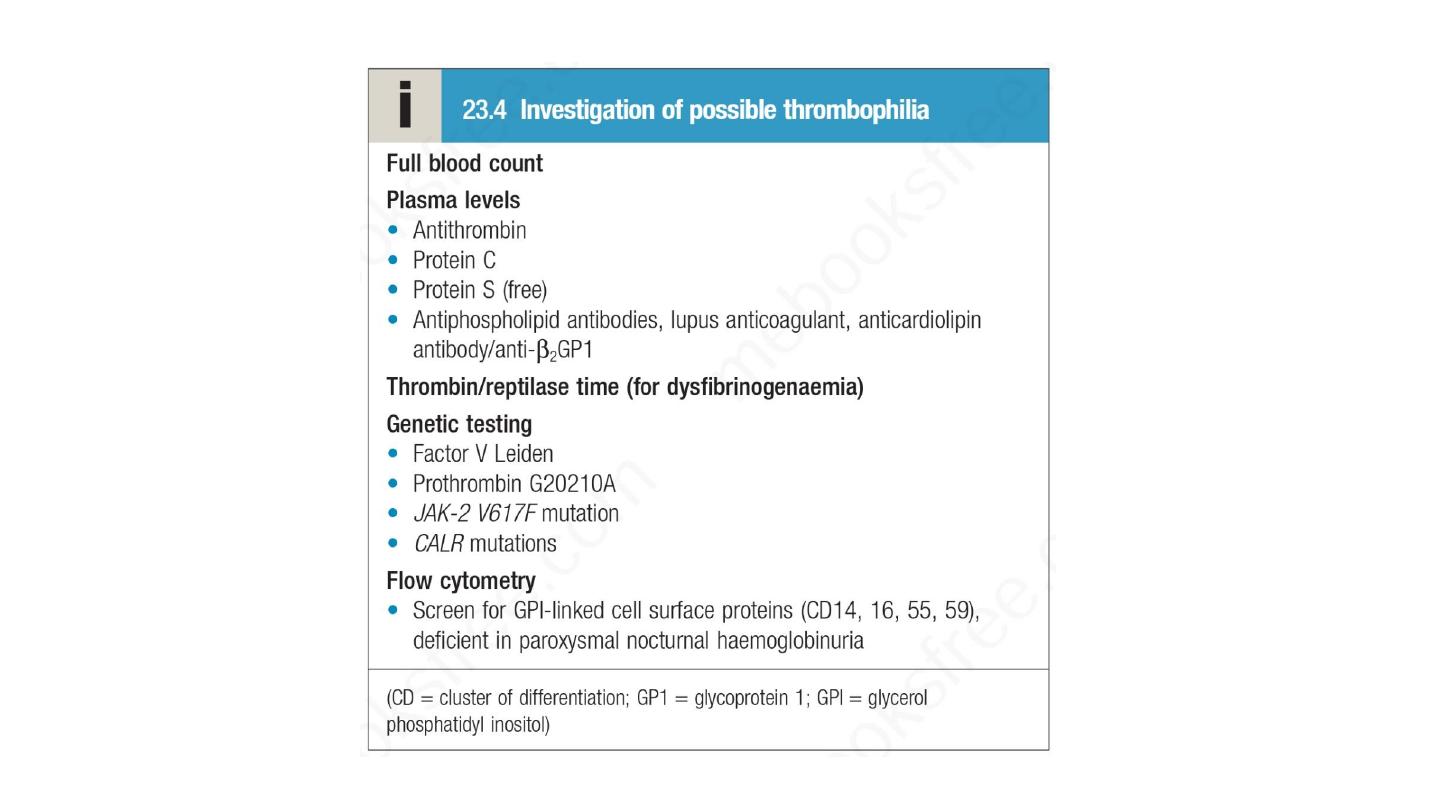
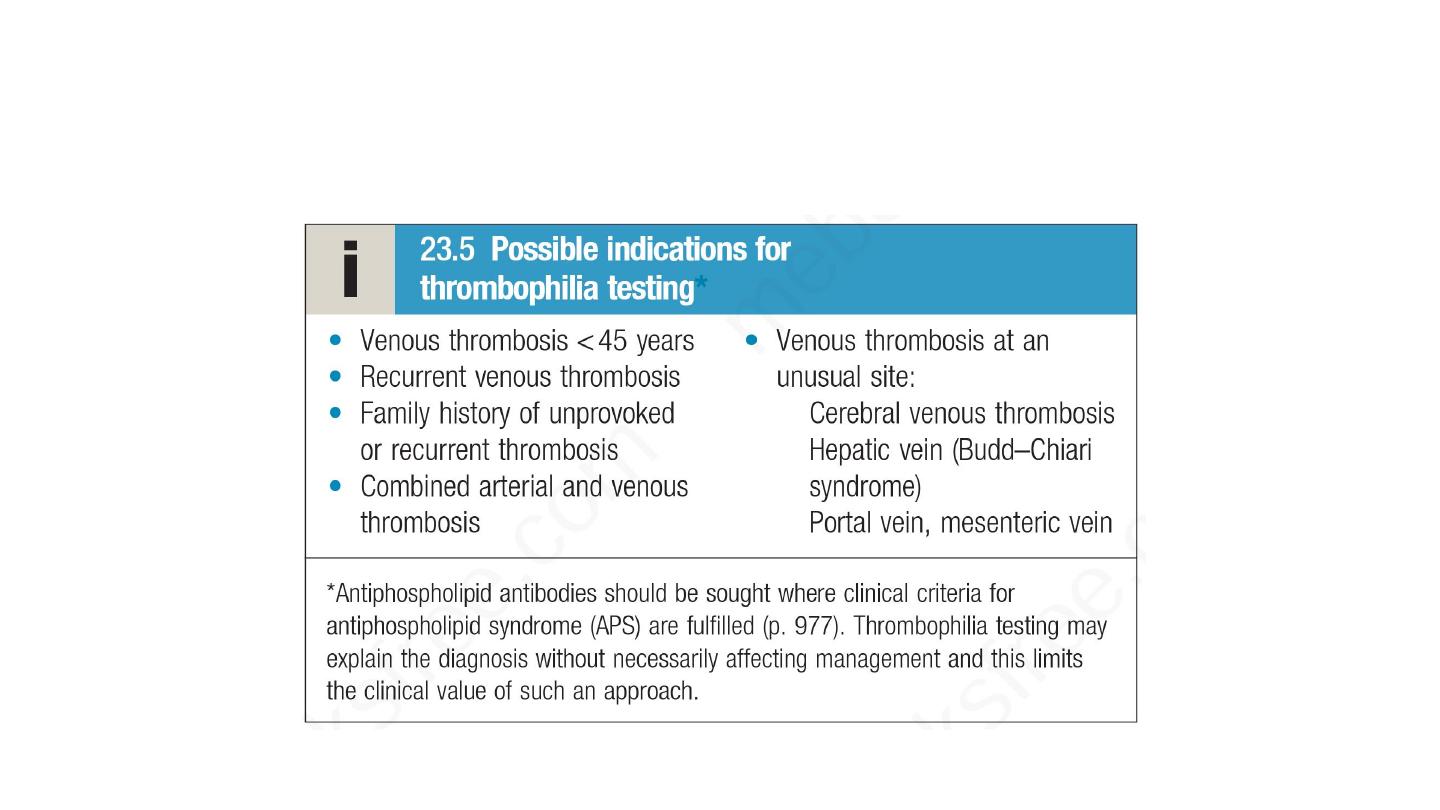
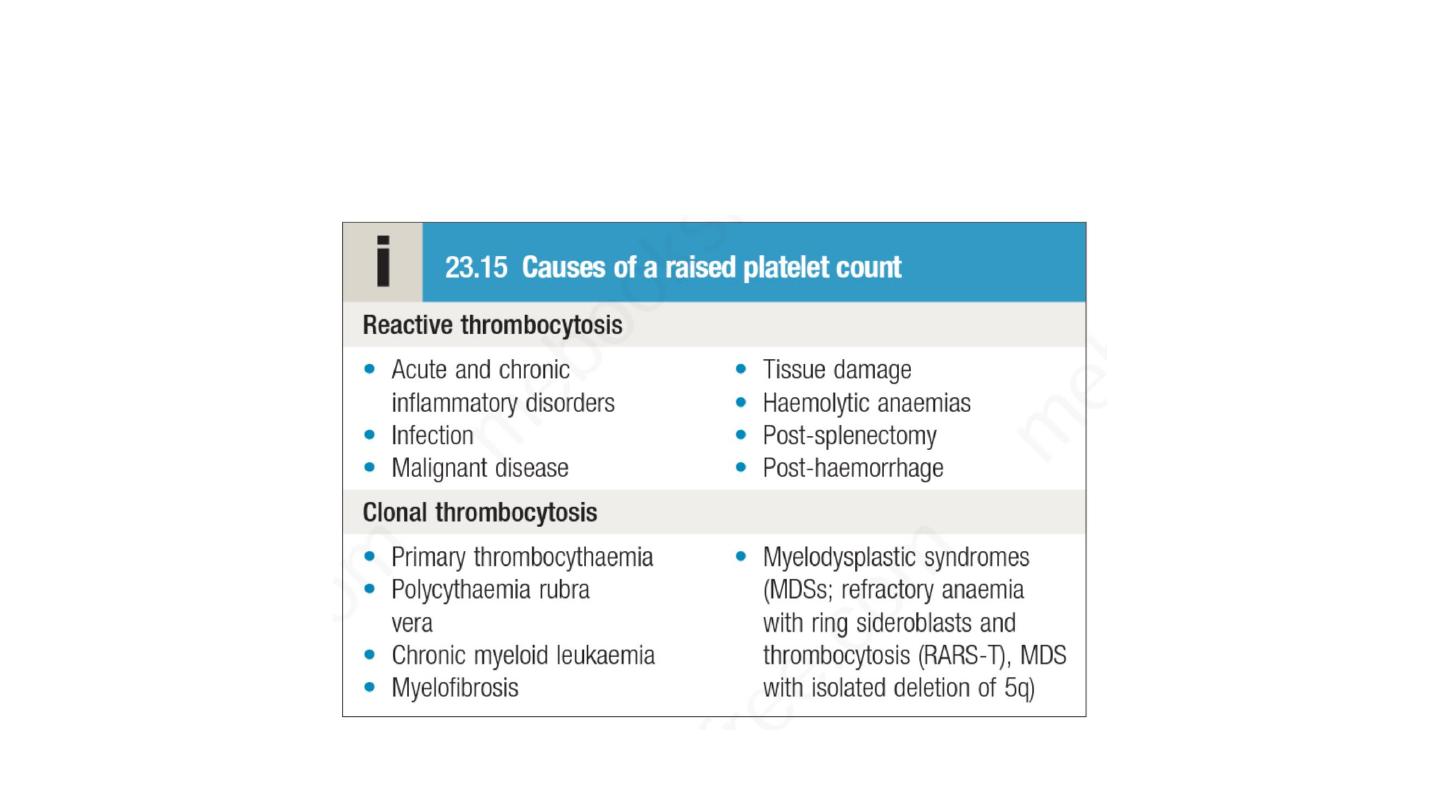
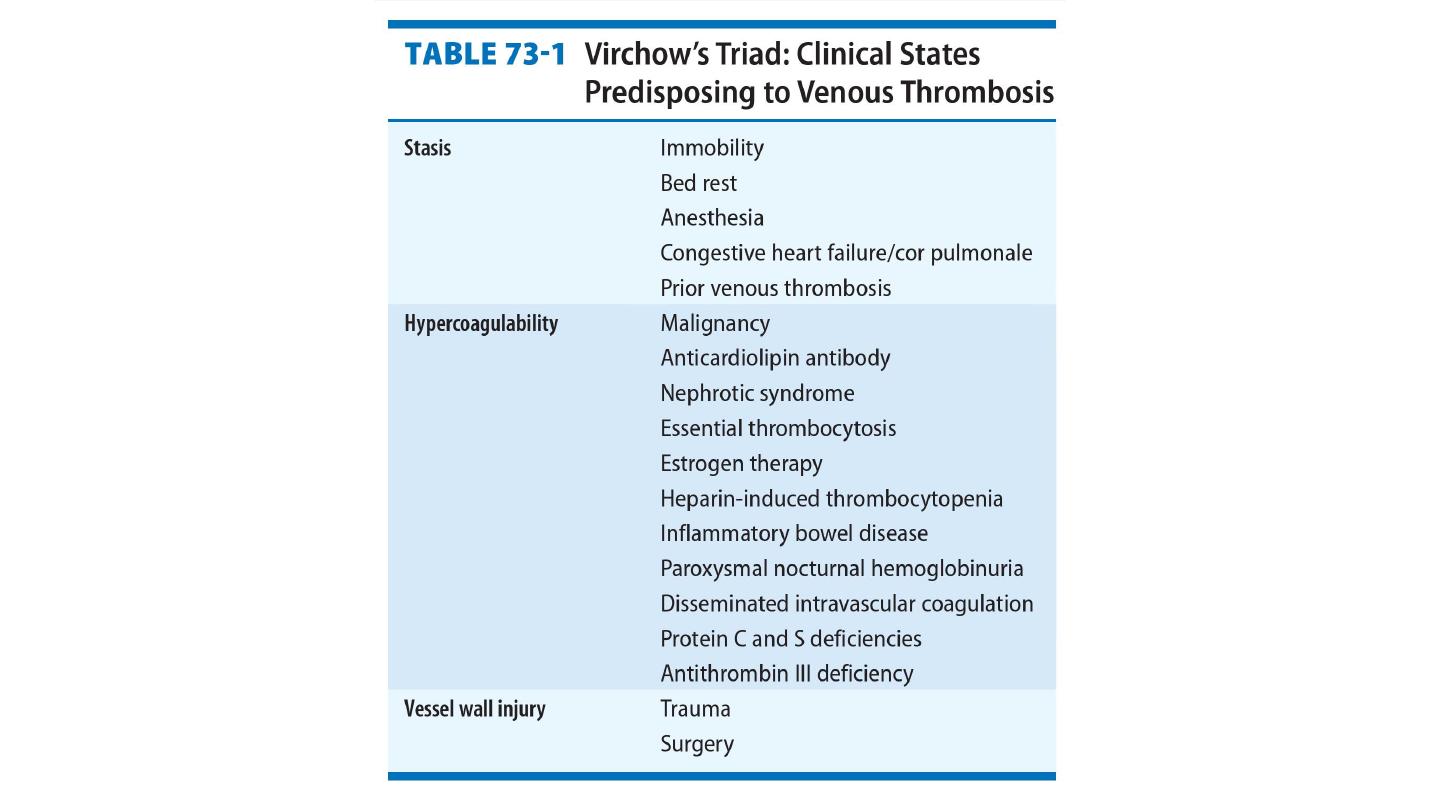
Thrombophilia is a state of hypercoagulability that can be inherited or
acquired.
It can result in venous or arterial thrombosis and even embolic
phenomena.

• While the most common presentations of venous thromboembolism
(VTE) are deep vein thrombosis (DVT) of the leg and/or pulmonary
embolism
,
similar
management
principles
apply
to
rarer
manifestations such as jugular vein thrombosis, upper limb DVT,
cerebral sinus thrombosis and intra-abdominal venous thrombosis
(e.g. Budd–Chiari syndrome)
• Incidence of approximately 1 : 1000 in Western populations. The
relative incidence of DVT:PE is approximately 2 : 1. Mortality 30 days
after DVT is approximately 10%, compared to 15% for PE

Management of VTE
• The mainstay of treatment for all forms of VTE is anticoagulation
.
This can be achieved in several ways. One option is to use LMWH
followed by a coumarin anticoagulant, such as warfarin. Treatment of
acute VTE with LMWH should continue for a minimum of 5 days.
Patients treated with warfarin should achieve a target INR of 2.5
(range 2–3) with LMWH continuing until the INR is above 2.
Alternatively, patients may be treated with a NOAC. Rivaroxaban
and apixaban may be used immediately from diagnosis without the
need for LMWH, while the licences for dabigatran and edoxaban
include initial treatment with LMWH for a minimum of 5 days
before commencing the NOAC.

• In patients with active cancer and VTE, there is evidence that
maintenance anticoagulation with LMWH is associated with a lower
recurrence rate than warfarin. Patients who have had VTE and have a
strong contraindication to anticoagulation and those who continue to
have new pulmonary emboli despite therapeutic anticoagulation
should have an inferior vena cava (IVC) filter inserted to prevent life-
threatening PE.
• The optimal initial period of anticoagulation is between 6 weeks and
6 months.

Indications for IVC filter:
• Contraindication for anticoagulation
• Recurrent PE in spite of anticoagulation
• Anticoagulation-related complication
• PE and limited cardiac reserve
• Prophylaxis in patients with severe trauma, spinal cord injury, or
paraplegia

• Patients with a
provoked VTE
in the presence of a temporary risk
factor, which is then removed, can usually be treated for short
periods (e.g
. 3 months
), and indeed anticoagulation for more than
6 months does not alter the rate of recurrence following
discontinuation of therapy. If there are ongoing risk factors that
cannot
be
alleviated,
such
as
active cancer,
long-term
anticoagulation is usually recommended, provided that the risk of
bleeding is not deemed excessive.
• Many patients who have had
unprovoked episodes of VTE will
benefit from long-term anticoagulation

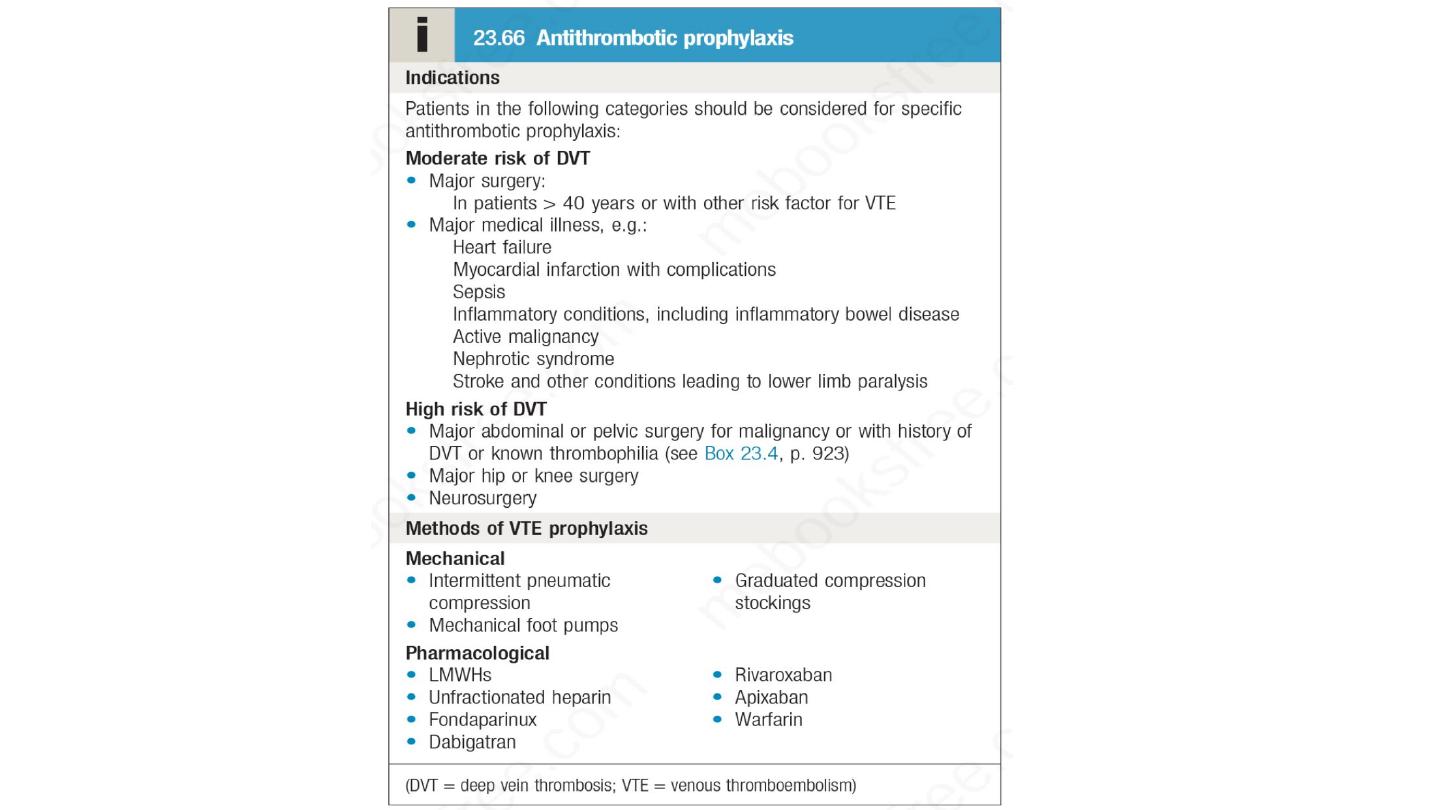
Prophylaxis of VTE
• All patients admitted to hospital should be assessed for their
risk of developing VTE and appropriate prophylactic measures
should be put in place. Both medical and surgical patients are
at increased risk. Early mobilization of patients is important to
prevent DVT, and those at medium or high risk require additional
antithrombotic measures;
these
may
be
pharmacological
or
mechanical.

Unilateral leg swelling
• Most leg swelling is caused by oedema, the accumulation of
fluid within the interstitial space. Unilateral swelling usually
indicates a localised pathology in either the venous or the
lymphatic
system,
while bilateral
oedema
often
represents
generalised fluid overload combined with the effects of gravity.
However, all causes of unilateral leg swelling may present
bilaterally, and generalised fluid overload may present with
asymmetrical (and therefore apparently unilateral) oedema.

Presentation
Any patient who presents with unilateral leg
swelling should be assessed with the possibility of deep vein
thrombosis
(DVT)
in mind
. The pain and swelling of a DVT is
often fairly gradual in onset, over hours or even days. Sudden-
onset pain in the posterior aspect of the leg is more consistent
with gastrocnemius muscle tear (which may be traumatic or
spontaneous) or a ruptured Baker’s cyst. Leg swelling and pain
associated with paraesthesia or paresis, or in the context of lower
limb injury or reduced conscious level, should always prompt
concern regarding the possibility of compartment syndrome .
Cellulitis is other cause of unilateral leg swelling.

• Clinical assessment
• Lower limb DVT characteristically starts in the distal veins,
causing an increase in temperature of the limb and dilatation of
the superficial veins. Often, however, symptoms and signs are
minimal.
• Cellulitis is usually characterised by erythema and skin warmth
localised to a well-demarcated area of the leg and may be
associated with an obvious source of entry of infection (e.g. leg
ulcer or insect bite). The patient may be febrile and systemically
unwell. Superficial thrombophlebitis is more localised; erythema
and tenderness occur along the course of a firm, palpable vein.

Examination of any patient presenting with leg swelling should
include assessment for malignancy (evidence of weight loss, a
palpable mass or lymphadenopathy).
Malignancy is a risk factor for DVT, but pelvic or lower abdominal
masses can also produce leg swelling by compressing the pelvic
veins or lymphatics.
Early lymphoedema is indistinguishable from other causes of
oedema. More chronic lymphoedema is firm and non-pitting, often
with thickening of the overlying skin, which may develop a
‘cobblestone’ appearance

Chronic venous insufficiency is a cause of long-standing oedema
that, particularly when combined with another cause of leg
swelling,
may
acutely
worsen.
Characteristic
skin
changes
(haemosiderin deposition, hair loss, varicose eczema, ulceration)
and prominent varicosities are common, and sometimes cause
diagnostic confusion with cellulitis.
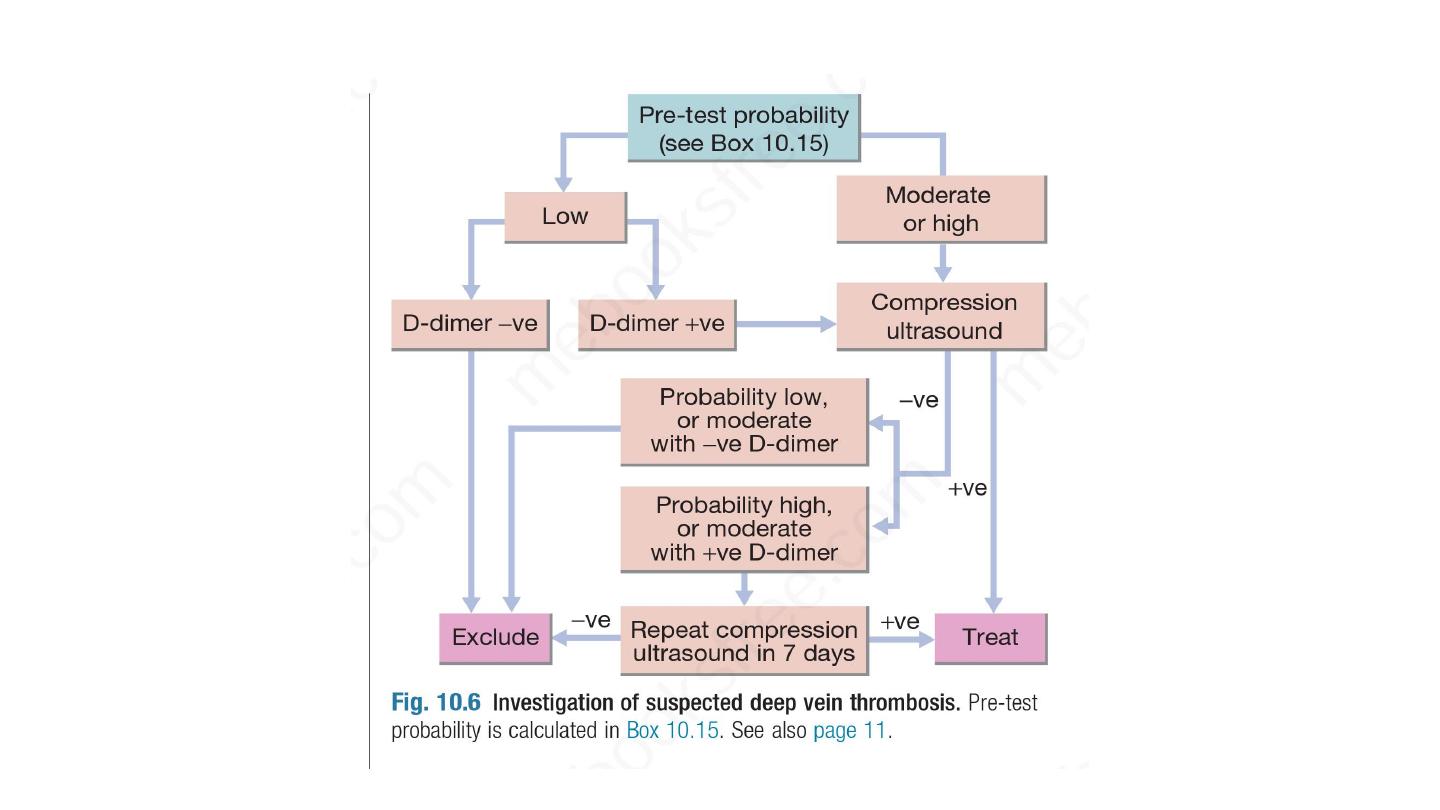
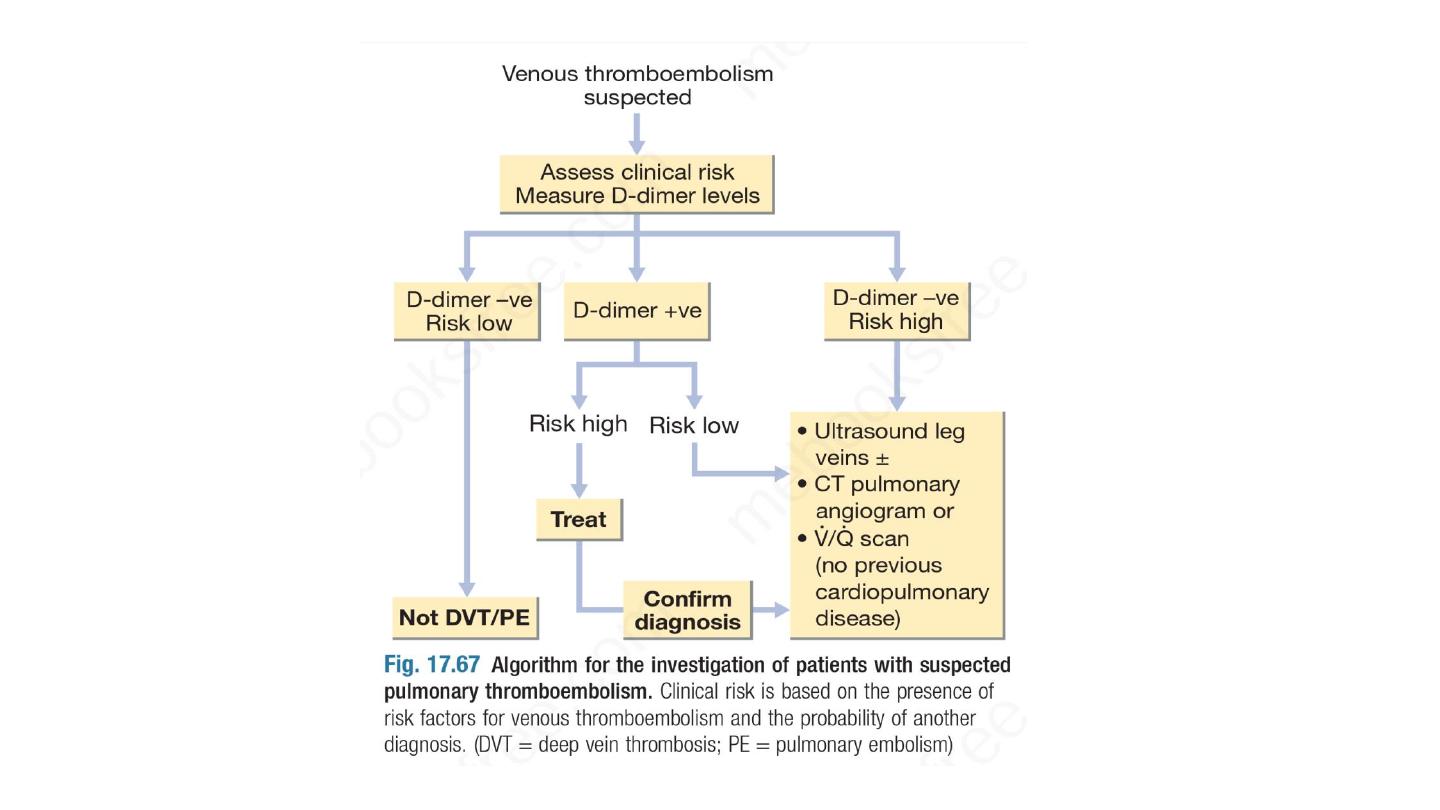
Initial investigations
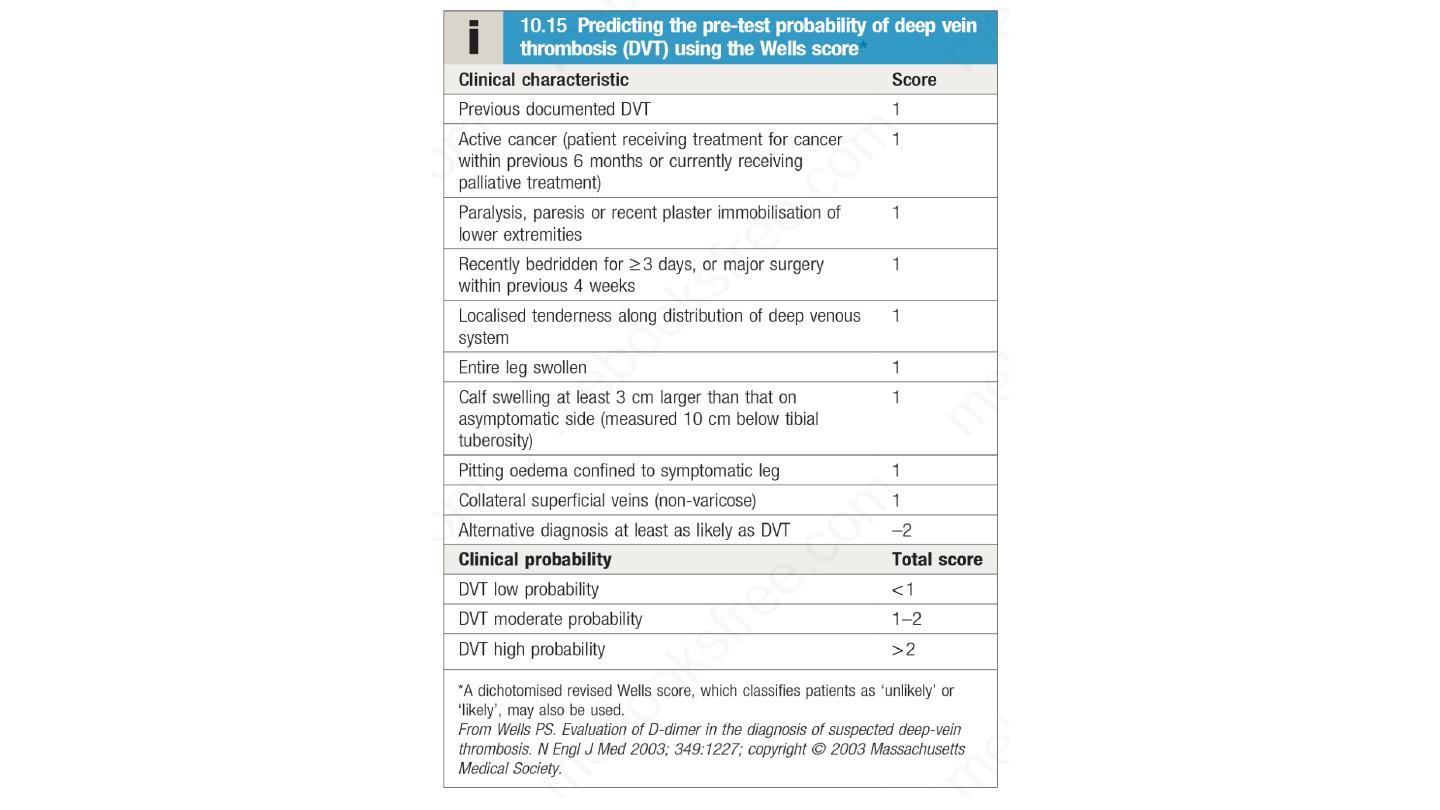
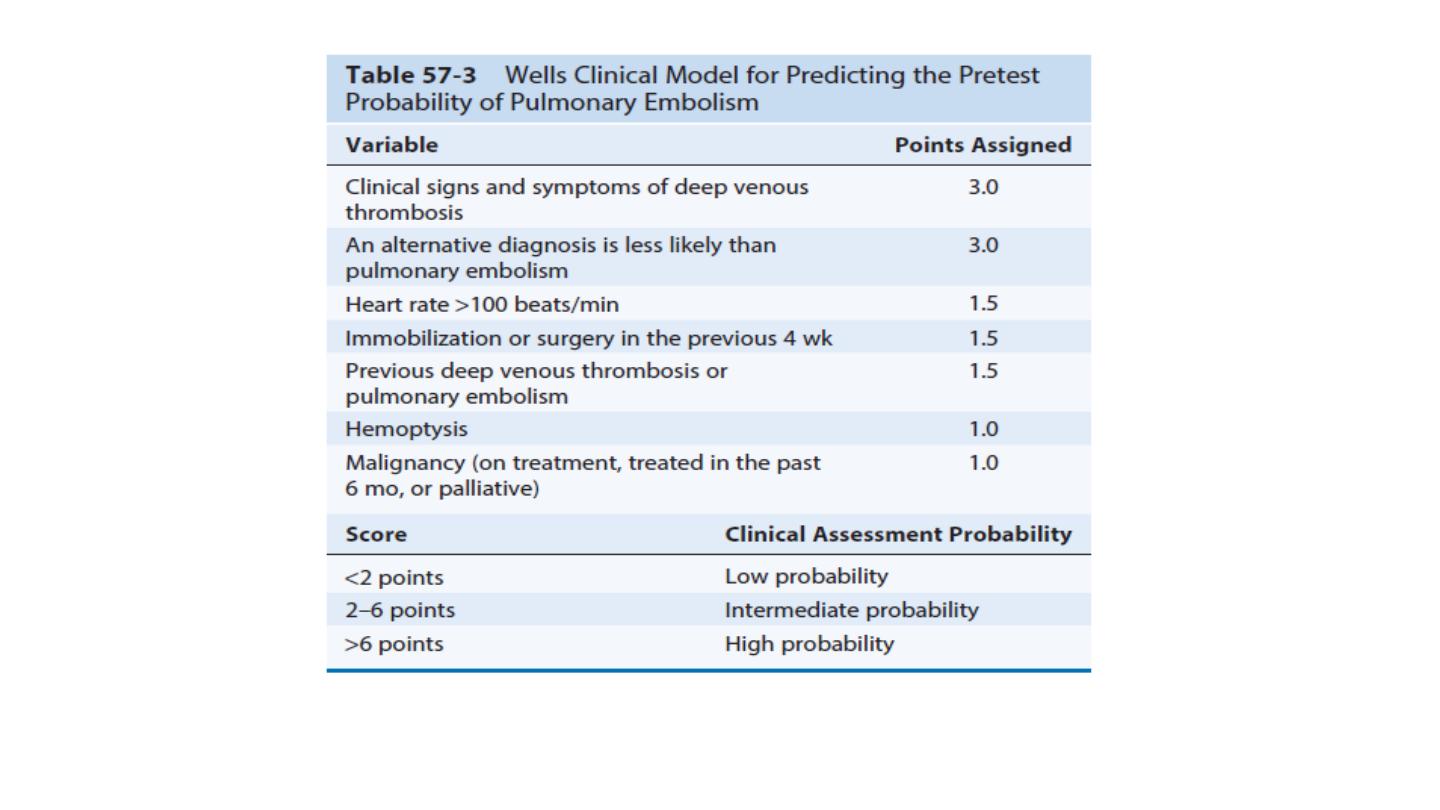
Clinical criteria can be used to rank patients according to their
likelihood of DVT, by using scoring systems such as the Wells score .
Investigation of suspected DVT based on initial Wells score. In
patients with a low (‘unlikely’) pre-test probability of DVT, D-dimer
levels can be measured; if these are normal, further investigation for
DVT is unnecessary. In those with a moderate or high (‘likely’)
probability of DVT or with elevated D-dimer levels, objective diagnosis
of DVT should be obtained using appropriate imaging, usually a Doppler
ultrasound scan. The investigative pathway for DVT, therefore, differs
according to the pre-test probability of DVT. For low-probability DVT,
the negative predictive value of the D-dimer test (the most important
parameter in this context) is over 99%; if the test is negative, the
clinician can discharge the patient with confidence.

• If cellulitis is suspected, serum inflammatory markers, skin swabs
and blood cultures should be sent.
• Ruptured Baker’s cyst and calf muscle tear can both be readily
diagnosed on ultrasound. If pelvic or lower abdominal malignancy
is suspected, a prostate-specific antigen (PSA) level should be
measured in males and appropriate imaging with ultrasound
(transabdominal or transvaginal) or CT should be undertaken.

Pulmonary embolism
The majority of pulmonary emboli arise from the propagation of lower
limb deep vein thrombosis. Rare causes include septic emboli (from
endocarditis affecting the tricuspid or pulmonary valves), tumour
(especially choriocarcinoma), fat following fracture of long bones such
as the femur, air, and amniotic fluid, which may enter the mother’s
circulation following delivery

Clinical features The diagnosis of pulmonary embolism (PE) may be aided by
asking three questions:
• Is the clinical presentation consistent with PE?
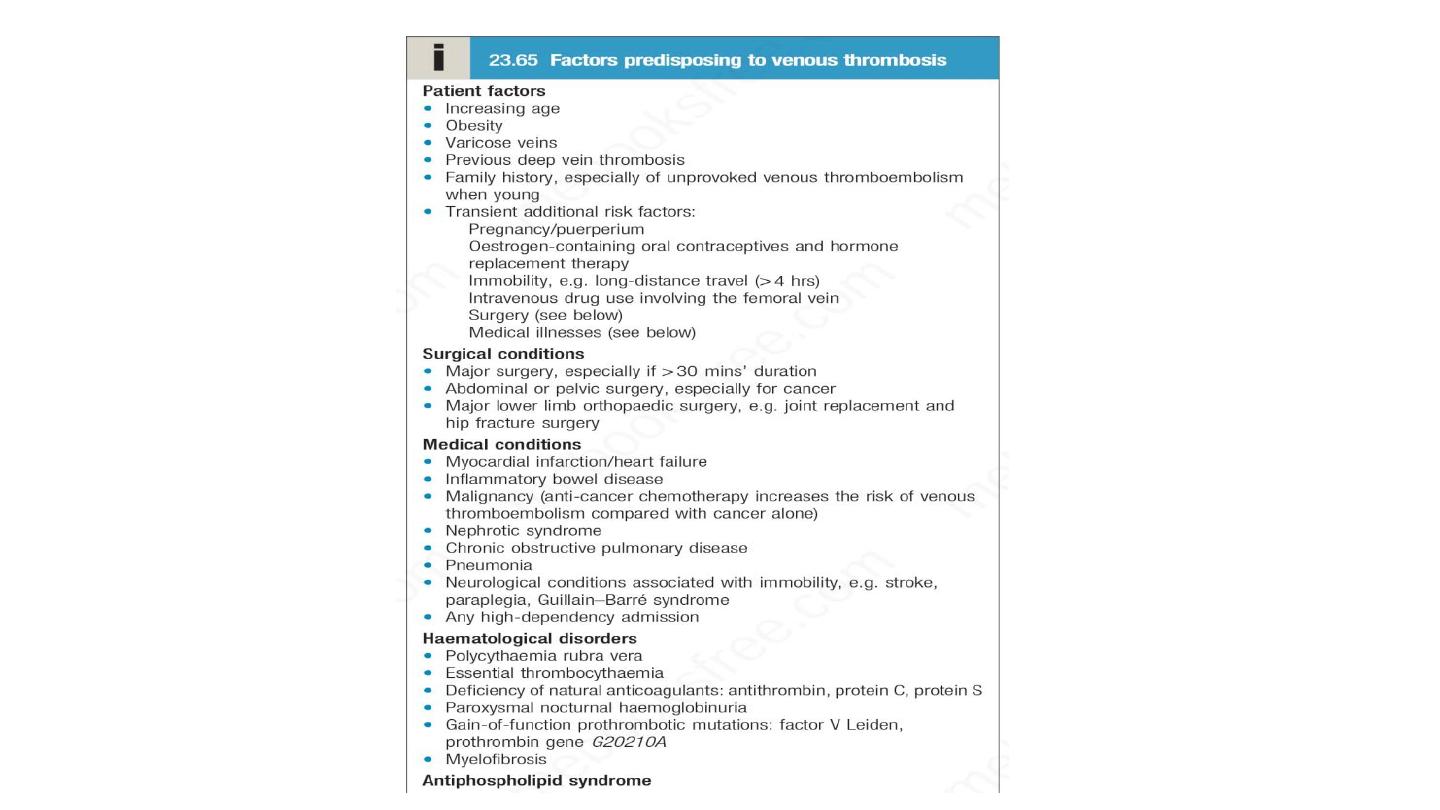
• Does the patient have risk factors for PE?
•
Are there any alternative diagnoses that can explain the patient’s
presentation?
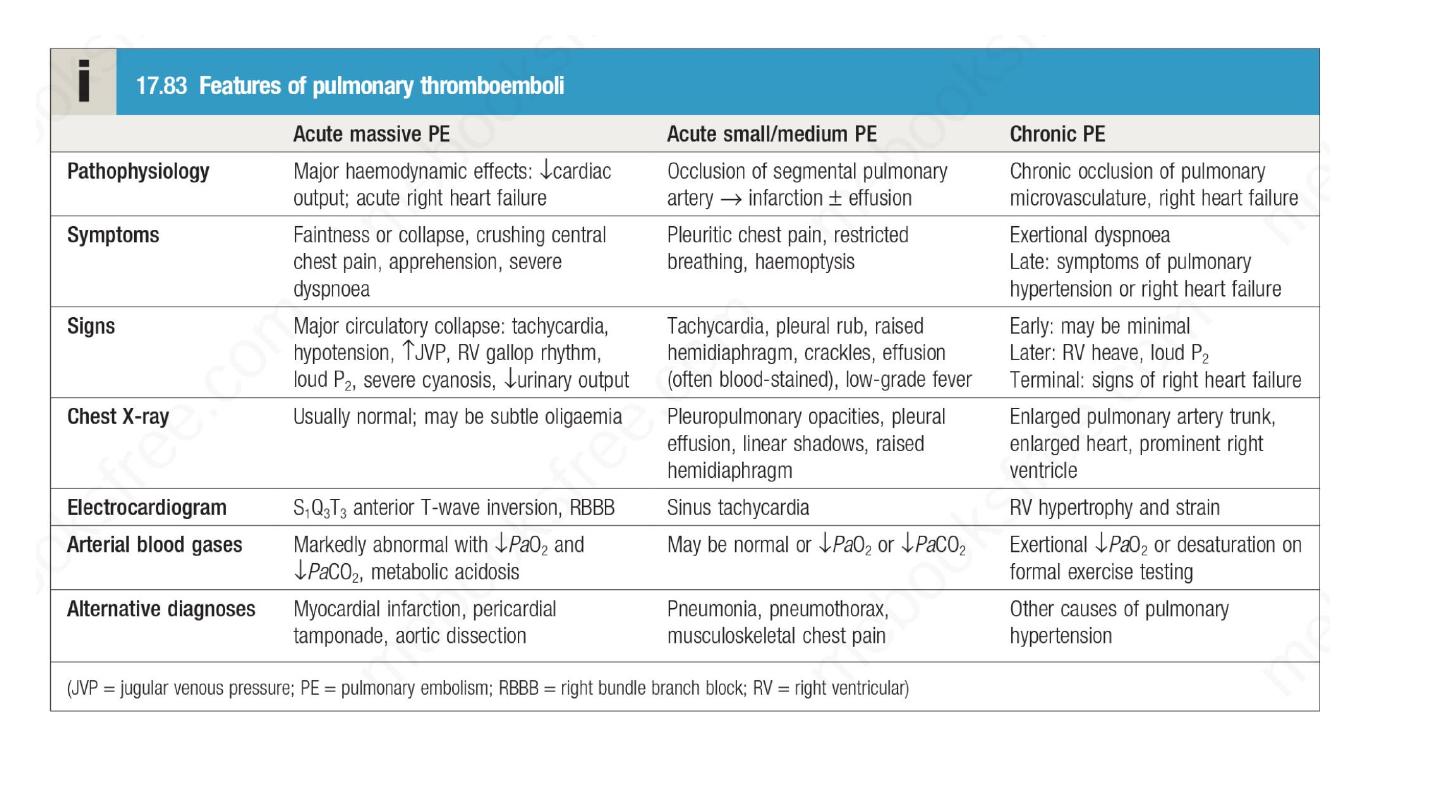
Clinical presentation varies, depending on number, size and distribution of
emboli and on underlying cardiorespiratory reserve. A recognised risk factor
is present in 80–90% . The presence of one or more risk factors increases the
risk further still.

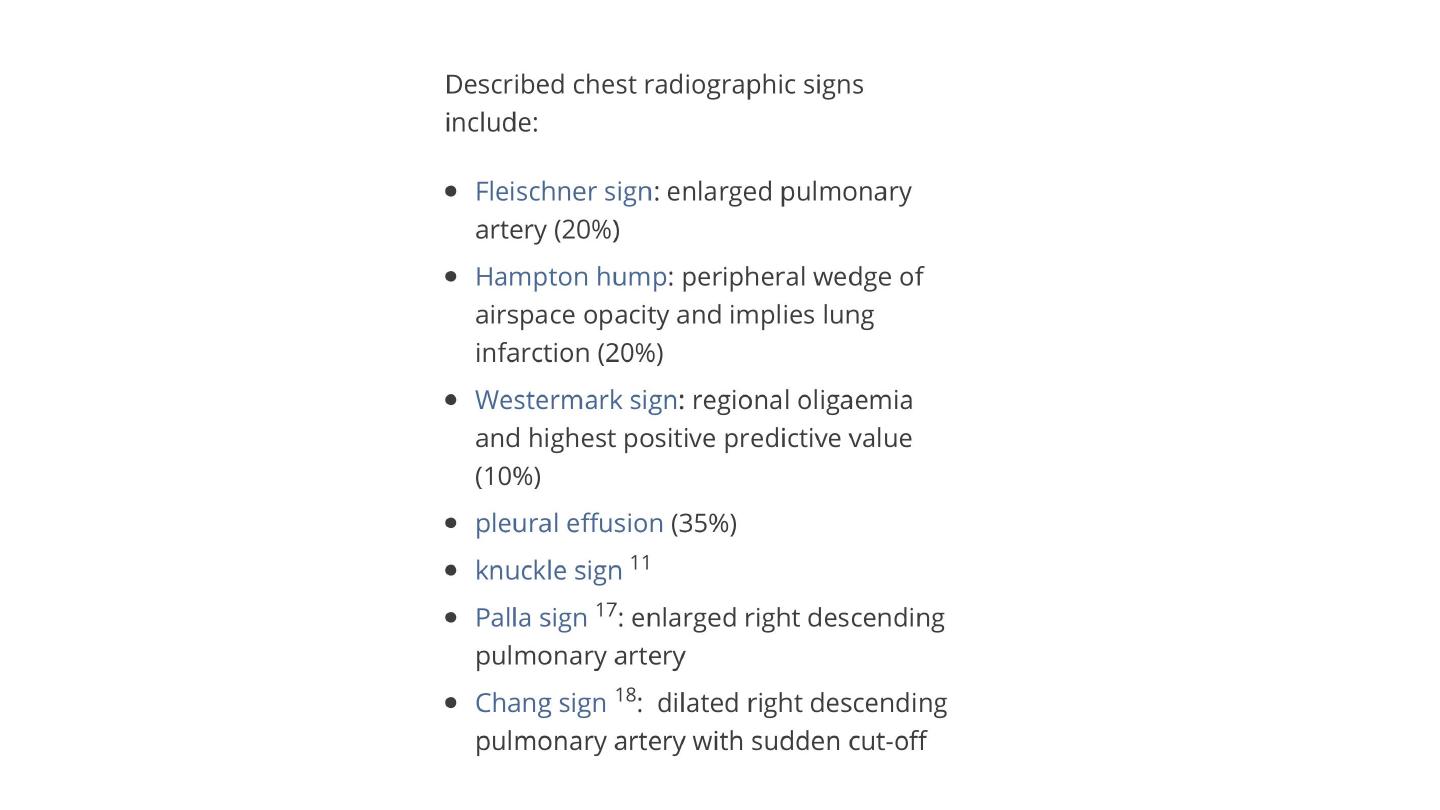
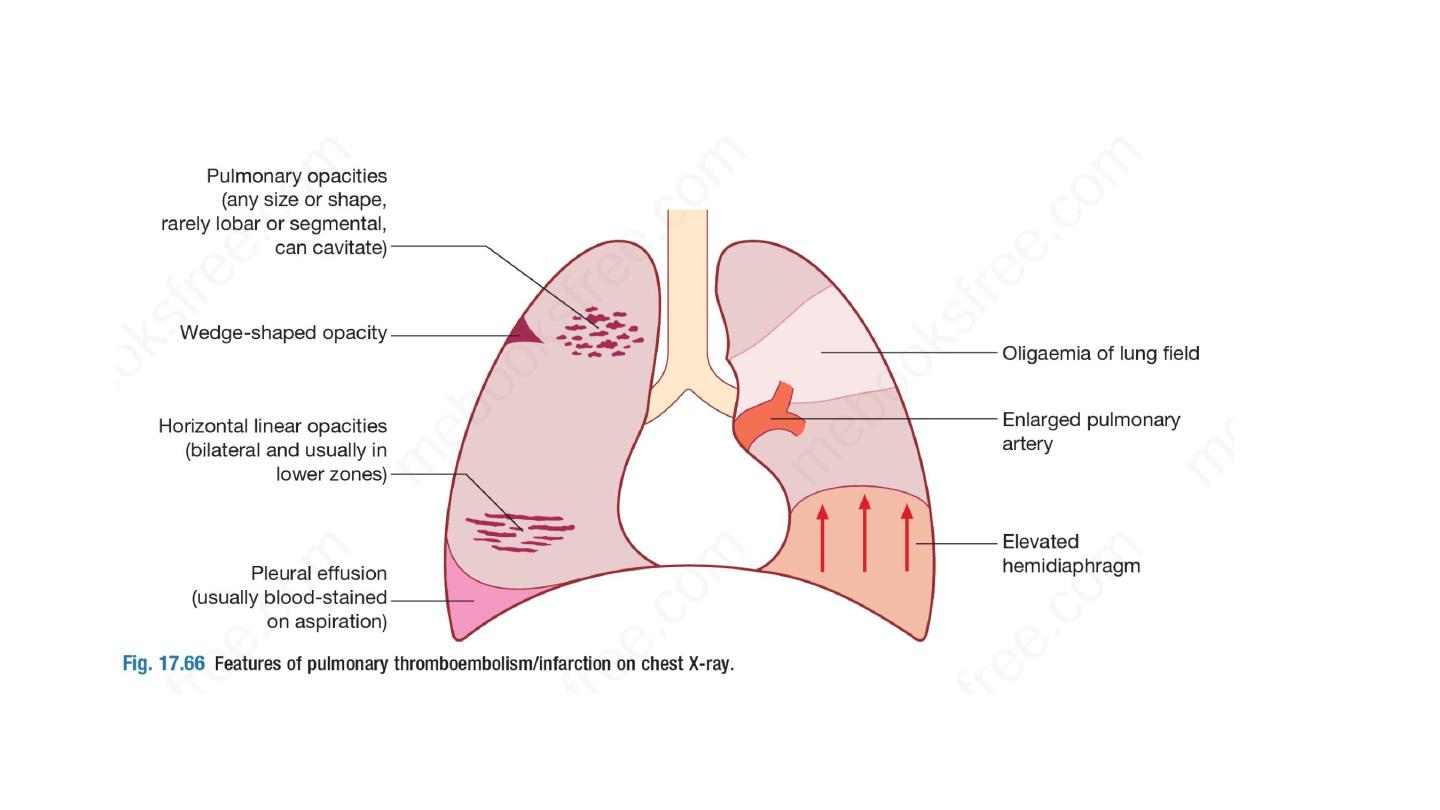
Investigations
A variety of non-specific radiographic appearances have been
described but the chest X-ray is most useful in excluding
key
differential diagnoses, e.g. pneumonia or pneumothorax.
Normal
appearances in an acutely breathless and hypoxaemic patient
should raise the suspicion of PE
, as should bilateral changes in
anyone presenting with unilateral pleuritic chest pain.

ECG is often normal but is useful in excluding other important
differential diagnoses, such as acute myocardial infarction and
pericarditis.
The most common findings in PE include sinus
tachycardia and anterior T-wave inversion
but these are non-
specific; larger emboli may cause right heart strain revealed by an
S1Q3T3
pattern,
ST-segment
and
T-wave
changes, or
the
appearance of right bundle branch block.
Arterial blood gases typically show a reduced PaO2 and a normal
or low PaCO2, and an increased alveolar–arterial oxygen gradient,
but may be normal in a significant minority. A metabolic acidosis
may be seen in acute massive PE with cardiovascular collapse

An elevated D-dimer is of limited value, as it may be raised in a
variety
of
other
conditions,
including myocardial
infarction,
pneumonia and sepsis. However, low levels, particularly in the
context of a low clinical risk, have a high negative predictive
value and further investigation is usually unnecessary . The result
of the D-dimer assay should be disregarded in high-risk patients,
as further investigation is mandatory even when normal. The
serum troponin I may be elevated, reflecting right heart strain.

• CTPA is the first-line diagnostic test.
It has the advantage of
visualising
the
distribution
and
extent
of
the
emboli or
highlighting an alternative diagnosis, such as consolidation,
pneumothorax or aortic dissection. As the contrast media may be
nephrotoxic,
care
should
be
taken in
patients
with
renal
impairment, and CTPA avoided in those with a history of allergy
to iodinated contrast media.
• In these cases, either V/Q scanning or ventilation/perfusion single
photon emission computed tomography (V/Q SPECT) may be
considered

• Colour Doppler ultrasound of the leg veins may be used in
patients with suspected PE, particularly if there are clinical signs
in a limb, as many will have identifiable proximal thrombus in
the leg veins.
• Bedside echocardiography is extremely helpful in the differential
diagnosis and assessment of acute circulatory collapse. Acute
dilatation of the right heart is usually present in massive PE,
and thrombus (embolism in transit) may be visible. Important
differential diagnoses, including left ventricular failure, aortic
dissection and pericardial tamponade, can also be identified.

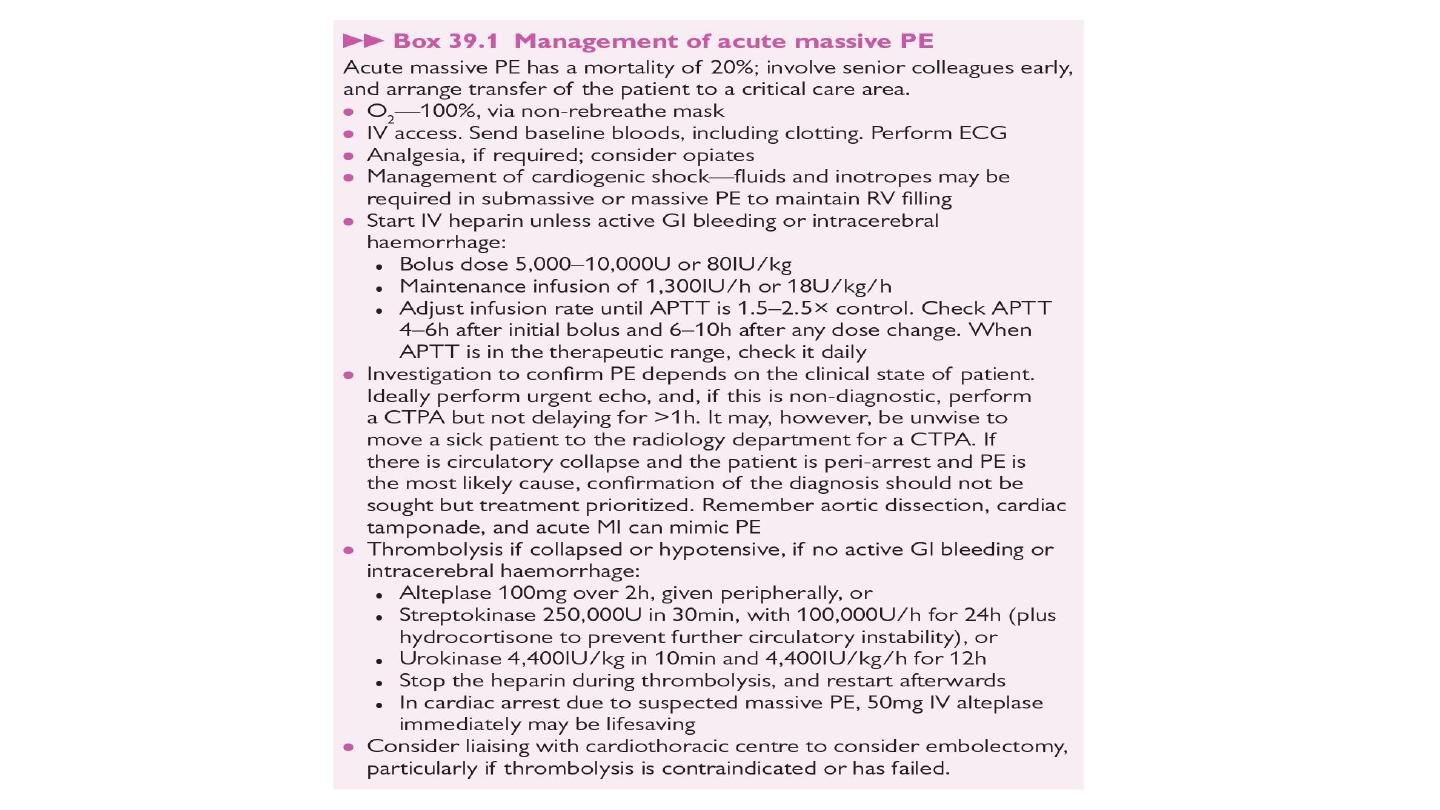
Management
General measures
Prompt recognition and treatment are potentially life-saving.
Sufficient oxygen should be given to hypoxemic patients to
maintain arterial oxygen saturation above 90%. Circulatory shock
should be treated with intravenous fluids or plasma expander,
but inotropic agents are of limited value as the hypoxic dilated
right ventricle is already close to maximally stimulated by
endogenous catecholamines. Diuretics and vasodilators should also
be avoided, as they will reduce cardiac output. Opiates may be
necessary to relieve pain and distress.

• Anticoagulation : The main principle of treatment for PE is
anticoagulation, which is discussed for PE and other forms of VTE.
• Thrombolytic and surgical therapy : Thrombolysis is indicated in any
patient presenting with acute massive PE accompanied by cardiogenic
shock. In the absence of shock, the benefits are less clear but
thrombolysis may be considered in those presenting with right
ventricular dilatation and hypokinesis or severe hypoxaemia. Patients
must be screened carefully for haemorrhagic risk, as there is a high
risk of intracranial haemorrhage. Surgical pulmonary embolectomy
may be considered in selected patients but carries a high

• External cardiac massage may be successful in the moribund patient
by dislodging and breaking up a large central embolus.
• Caval filters : A patient in whom anticoagulation is contraindicated,
who has suffered massive haemorrhage on anticoagulation, or
recurrent VTE despite anticoagulation, should be considered for an
inferior vena caval filter. Retrievable caval filters are particularly useful
in individuals with temporary risk factors. The caval filter should be
used only until anticoagulation can be safely initiated, at which time
the filter should be removed if possible.

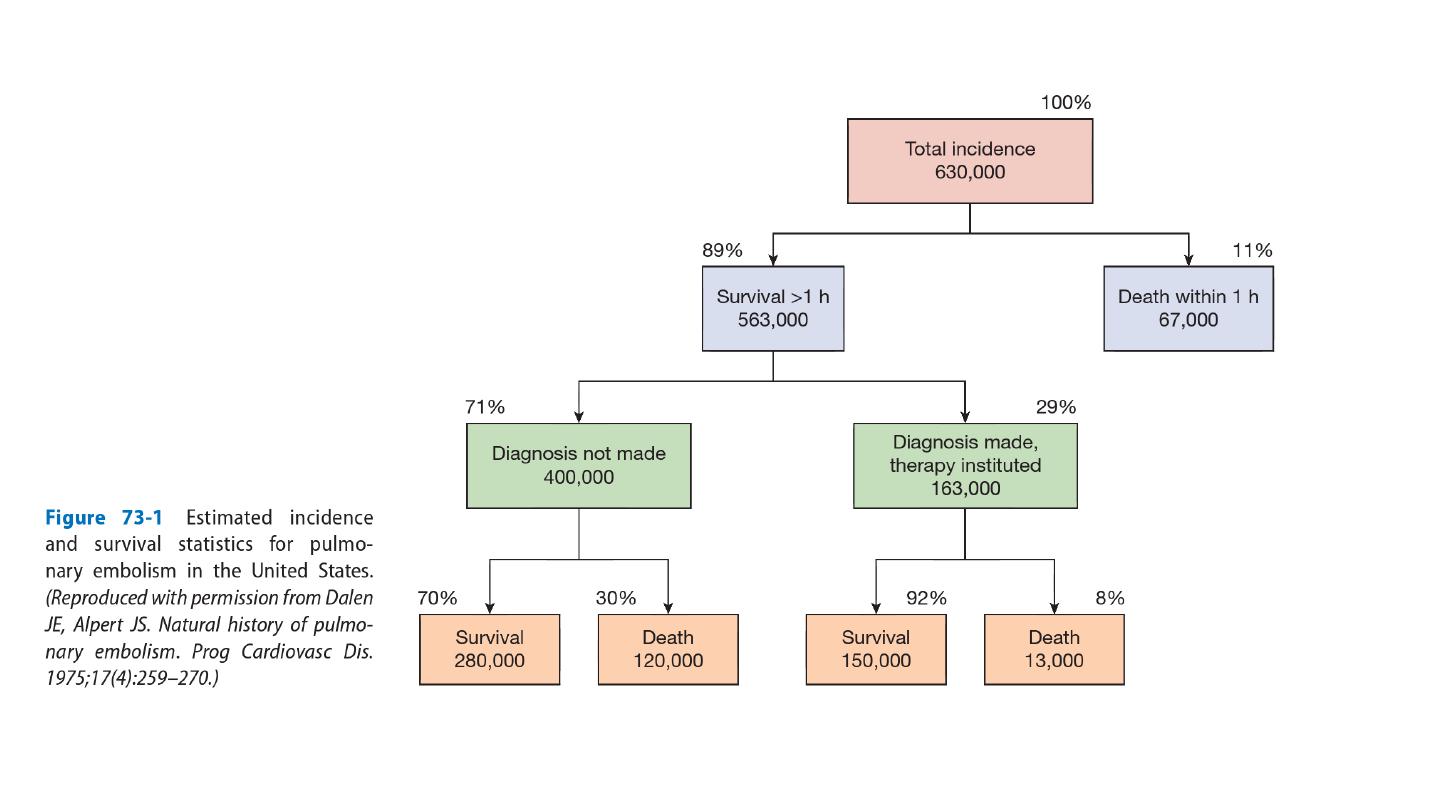
Prognosis
Immediate
mortality
is
greatest
in
those
with
echocardiographic evidence of right ventricular dysfunction or
cardiogenic shock. Once anticoagulation is commenced, however, the
risk of mortality rapidly falls. The risk of recurrence is highest in the first
6–12 months after the initial event, and at 10 years around one-third of
individuals will have suffered a further events.