Authors: Ass. Professor Baha Diaa Moohee
Alosy, DCH, FICMSP Departments of
Pediatrics- Collage of Medicine. University
of Tikrit -IRAQ.
Etiology:
Specific RNA virus. Only one serotype is
known (life long immunity after infection).
Essentials of Diagnosis:
-History of exposure 10-12 days previously.
onjunctivitis,
c
days prodroma (fever,
5
-
3
-
ough).
c
oryza and
c
-Koplik's spots (Pathognomonic)
-Maculopapular confluent rash.

Mode of Transmission:
-Contact with secretions or droplets of an infected child.
Period of Infectivity:
-4 days prior to and 5 days after appearance of the rash.
Clinical Manifestations
: An incubation
stage 10-12 days
stage 10-12 days
Prodromal stage with an exanthem (Koplik's spots),
usually lasts 3-5 days.
Koplik's spots
are grayish
white dots on an erythematous base on the anterior
portion of the buckle mucosa. With appearance of rash,
Koplik's spots start to disappear.

Final stage starts with a maculopapular rash
accompanied by high fever. The rash starts behind
the ears, and along the hairline. Then the rash
spreads on the face, neck, upper arms, and upper
part of the chest within the first 24 hours.
On 2
nd
day. The rash appears on the back,
abdomen, arms and thighs.
On 3
rd
day. It reaches the feet and begins to fade
On 3
rd
day. It reaches the feet and begins to fade
on the face.
An abrupt drop in temperature to normal. The rash
fades downward in the same sequence in which it
appeared


Diagnosis:
Clinical features but Laboratory tests is
rarely needed.
Leukocytic count tends to be low with a relative
lymphocytosis. Leucocytosis is indicative of secondary
bacterial infection.
Complications:
*The main complications of measles
are otitis media and pneumonia. *Encephalitis;
*Diarrhea and dysentery.
*Diarrhea and dysentery.
*Corneal ulcer and stomatitis. *Activation of a
tuberculous focus.
Supportive therapy: -
Antipyretics
(paracetamol)
Bed rest and an adequate fluid intake are indicated.

A nourishing easily digested diet and proper
cleanliness.
Vitamin A: A single dose of 50,000 to 200,000
IU.
A broad spectrum antibiotic in presence of
infections.
Prevention:
*Isolation should be maintained
Prevention:
*Isolation should be maintained
from the 7
th
day after exposure until 5 days
after the rash has appeared.
*Measles vaccine. *Post-exposure
prophylaxis.
- Hemorrhagic measles - PEM
GERMAN MEASLES (Rubella)
Etiology
: Rubella virus (an RNA virus).
Incubation Period: 2-3
weeks.
Mode of Transmission:
Droplet infection or direct contact with a case
Transplacental congenital infection from infected mother.
Prodromal stage: Very short and mild that it goes
unnoticed.
Prodromal stage: Very short and mild that it goes
unnoticed.
Contagiousness
:
Not as contagious as measles.
◦
Virus is present in nasopharyngeal secretions, blood,
feces and urine.
◦
Virus has been recovered from the nasopharynx 7 days
before exanthema and 7-8 days after its disappearance.
◦
Infants with congenital rubella are contagious for at least
10-12 months.
Clinical Manifestations
:
Age: Any age, peak incidence 5-14 years
Lymphadenopathy is evident at least 24hr before the rash
appears.
The exanthem begins on the face and spreads quickly on
the first day.
the first day.
2
nd
day.The rash is confluent and pinpoint like that of
scarlet fever with mild itching.
3
rd
day.The rash generally disappears with minimal
desquamation and no scaring.
Rubella without rash may occur as fever with enlarged
tender lymphadenopathy which may persist for a week or
more.


Complications:
Complications are relatively uncommon in
childhood.
Encephalitis similar to that seen with measles
Polyarthritis
• Congenital rubella
syndrome
Prophylaxis:
Prophylaxis:
Active immunization (MMR vaccine)
-MMR vaccine should not be given to pregnant
women; vaccinated women should avoid
pregnancy for 3 months after vaccination. Natural
infection gives life- long immunity.

Passive immunization. It is not indicated except in
non-immune pregnant women. Immune serum
globulin (ISG) in big doses is given I.M within one
week of exposure.
Treatment:
1- Antipyretics for fever. 2- Treatment of
complications
complications
Congenital Rubella
If rubella develops during the first trimester of
pregnancy, (which is the period of organogenesis).

Features of congenital rubella syndrome:
1-Intrauterine growth retardation, small for
gestational age and failure to thrive
2-Nerve deafness
3- Microcephaly and mental retardation
3- Microcephaly and mental retardation
4- Congenital heart disease (PDA, VSD)
5- Cataract, glaucoma, and cloudy cornea
6- Thrombocytopenic purpura,
hepatosplenomegaly, and osteopathy
This is a highly contagious infection characterized
by a pleomorphic rash.
Etiology:
Varicella-zoster virus which cause
Chicken pox in a non immune and Herpes
zoster in a partially immune individual.
Mode of Infection:
1-Direct contact. 2-Droplet
Mode of Infection:
1-Direct contact. 2-Droplet
infection. 3-Air borne.
Period of Infectivity:
Extends from one day
before the onset of rash till crusted.
Incubation Period:
2-3 weeks.
Clinical Manifestations:
Age:
Any age , the most
common from 5-10 years.
Prodromal stage
: very mild and short.
Eruption stage
: (pleomorphic rashes), all
forms of lesions being present.
The rash appears
as crops of macules which within
hours pass through a papular stage, then progress to develop
hours pass through a papular stage, then progress to develop
vesicles and pustules.
Pruritus
may be intense. -The rash may appear on mucous
membranes with ulceration in the mouth.

Complications:
Secondary bacterial infection of skin
lesions.
Hemorrhagic complications:
thrombocytopenia, purpura, hematuria,
and gastrointestinal hemorrhage.
and gastrointestinal hemorrhage.
Encephalitis and cerebellar ataxia.
Reye syndrome: encephalopathy and
hepatic dysfunction
.

Differential Diagnosi
s:
1 -Herpes zoster: Unilateral rash occurs along one
or more dermatome of peripheral nerves.
2-Impetigo: It is pyogenic infection of the skin
caused by staphylococci or streptococci.
3- Papulo-vesicular urticaria:
- Allergic reaction, mostly to an insect bite. -
- Allergic reaction, mostly to an insect bite. -
The lesions are mainly distributed over the
extensor surfaces of the extremities.
4-Scabies: -There is history of contact with a
case. -Itching is more by night. -Thread-like
burrows in interdigital spaces of fingers and
toes.

Varicella rash
Treatment:
Local and systemic antihistaminic to alleviate
itching.
Non- aspirin antipyretics (e.g. paracetamol).
Local application of calamine lotion.
Patients at risk of severe chickenpox should receive
acyclovir (antiviral agent).
Treatment of complications.
Treatment of complications.
RESEOLA INFANTUM
RESEOLA INFANTUM
Roseola (exanthem subitum) is a mild febrile
exanthematous illness occurring almost exclusively in
infants and young children. It is characterized by:
High fever for 3-5 days followed by
Precipitous drop to normal temperature with a
Precipitous drop to normal temperature with a
generalized maculopapular rash.
Etiology: Human herpes virus 6 and 7 (Sixth disease)
Mode of Transmission: Droplet infection
Incubation Period: 1 - 2 weeks

Clinical Manifestations:
• Season: mainly spring
• Prodrome of mild rhinorrhea, and mild redness of
conjunctiva and pharynx.
• Age: Most cases occur from 6 months to 3 years of
age,
(peak at 6-15 mons).
(peak at 6-15 mons).
• Fever: Sudden high fever lasts 3-4 days without
any localizing signs. It may be associated with
febrile convulsions.
•
Maculopapular Rash Appears On The 4
th
Day With
The Drop Of Fever. It Starts On The Trunk And
Rapidly Spreads Over The Arms And Neck, Leaving
The Face Minimally Involved, And Lasts Only 24
Hours.
•
This Occurrence Of Rash Is Described As A "Rainbow
Following The Storm".
Diagnosis
: This Is Only Clinical.
Diagnosis
: This Is Only Clinical.
Treatment:
- No Need For Antiviral Therapy
- Antipyretics
Such As Paracetamol.
- Supportive Treatment For Febrile Convulsions.
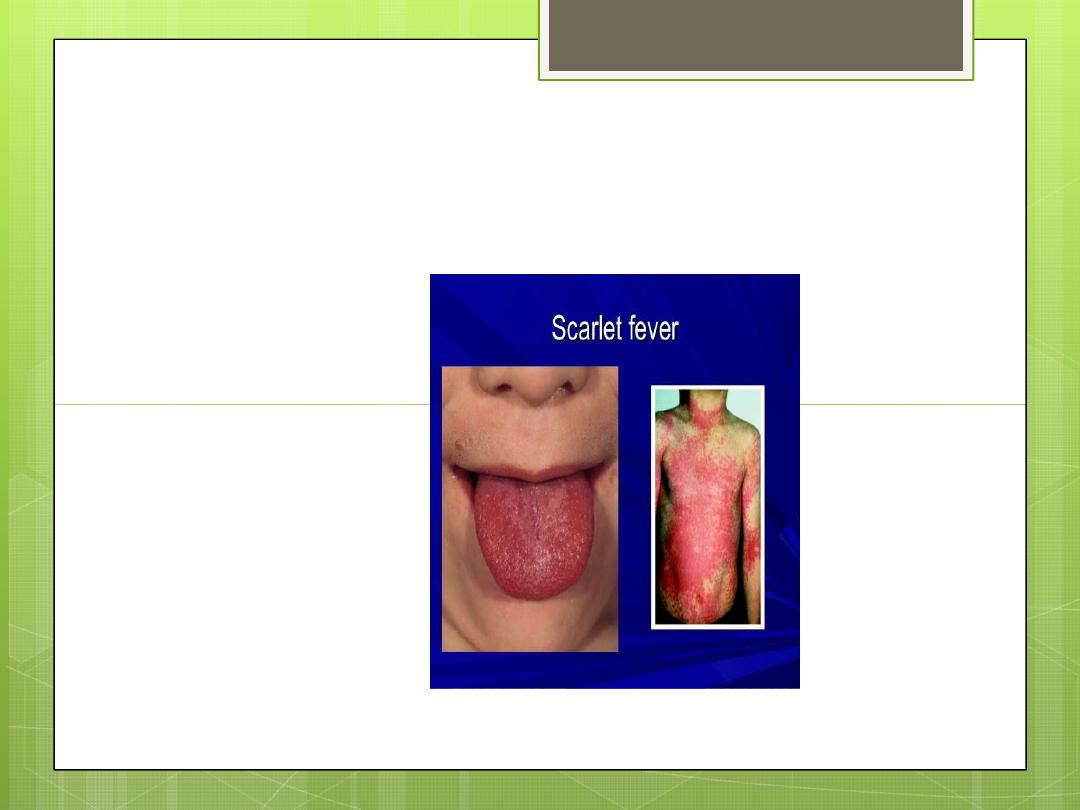
Scarlet fever
Incubation period is usually 3-6 days.
The onset is abrupt with fever, headache, dysphagia,
vomiting, with approximately 3 days duration.
Exanthem – Characteristic:
Filatov’s mask
Pastia’s lines
The erythema abates in 7-9 days.
Enanthem consists of:
Characteristic appearance of tongue
Exudative or erythematous pharyngitis and
tonsillitis, and very rarely, ulcerative aspect of
tonsillitis.
Descuamation period starts after 7-14 days of illness
Differential diagnosis
Other infectious causes of tonsillitis
Different eruptive disease
Kawasaki
Complications of scarlet fever
Complications of scarlet fever
Suppurative complications
Non suppurative complications: acute
rheumatic fever, acute glomerulonephritis
Laboratory features
Throat culture - positive for group A streptococci.
Rapid antigen detection tests in throat swab.
White blood cell count reveals leukocytosis,
White blood cell count reveals leukocytosis,
hypereosinophilia, neutrophilia.
Increased ESR.
Intracutaneous administration of erythrogenic
toxin elicits local erythema (positive Dick test – not
used at the present time).
Treatment
To prevent primary attacks of rheumatic fever, treatment
To prevent primary attacks of rheumatic fever, treatment
should ensure penicillin levels for at least 10 days.
This can be achieved by 7 days of penicillin G (2-4 million
IU/day) followed by 3 administration of benzathine
penicillin (every 7 days).
If penicillin allergy is suspected, the drug of choice is
erythromycin (30-40 mg/kg/day).