Acute Abdomen
Bowel Obstruction in Focus
Tikrit University
College of Medicine
Department of Radiology

Definition
Acute abdominal pain: defined as acute
abdominal pain unrelated to trauma
It is one of the most common conditions in in
the hospital emergency department.
It is a syndrome characterized by the sudden
onset of severe abdominal pain, requiring early
medical or surgical treatment
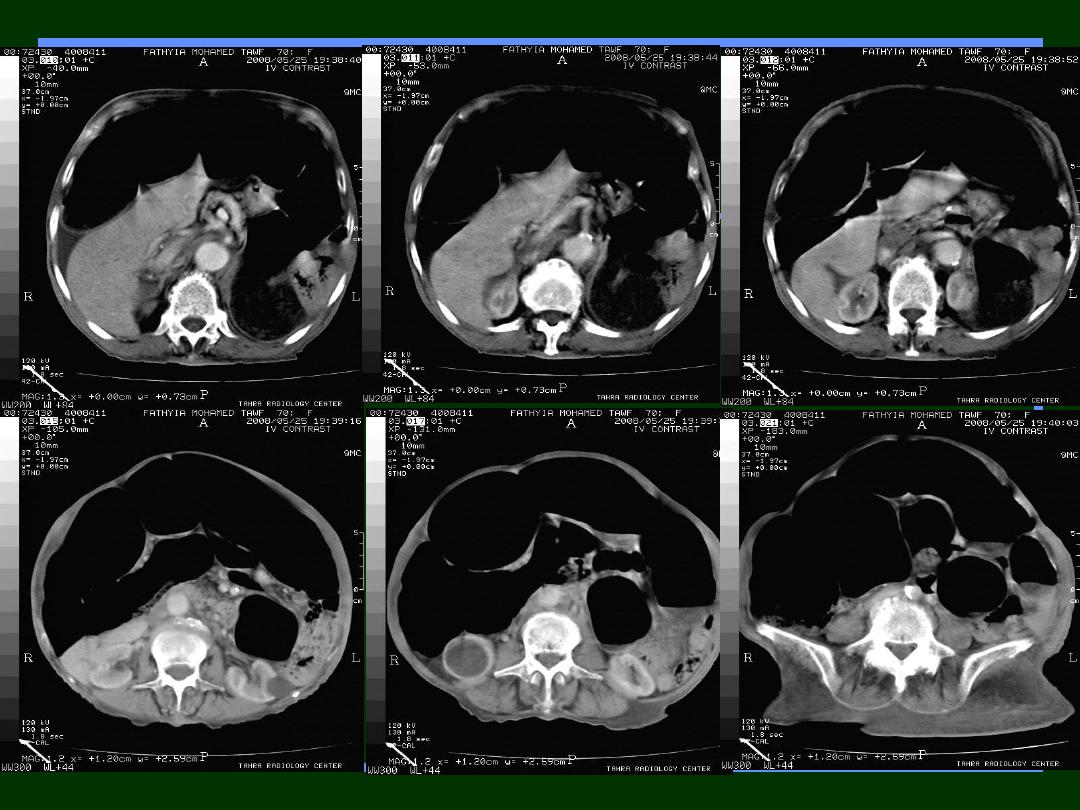
GB:
Acute cholecystitis & biliary colic - US
Pancreas:
Acute pancreatitis - US & CT
Stomach & Duodenum:
Gastritis & Peptic Ulcer
Spleen:
Spleenic infarction
– US & CT
Liver:
Amebic liver abscess. Spontaneous rupture of
hepatic neoplasm - US & CT
Renal :
Renal colic & Stones
–US & CT
Ovaries:
ovarian cyst, torsion - US
Bowel:
Acute appendicitis - US & CT
Bowel obstruction
–
X-ray
, US & CT
Acute diventricular disease - CT
Causes
Common causes of acute pain in
an abdominal quadrant
Right upper quadrant:
Acute calculous / non calculous
Cholecystitis.
Amebic liver abscess.
Spontaneous rupture of hepatic
neoplasm.
Myocardial infarction.
Common causes of acute pain in
an abdominal quadrant
Left upper quadrant:
Splenic infarction.
Splenic abscess.
Gastritis.
Gastric ulcer.
Common causes of acute pain in
an abdominal quadrant
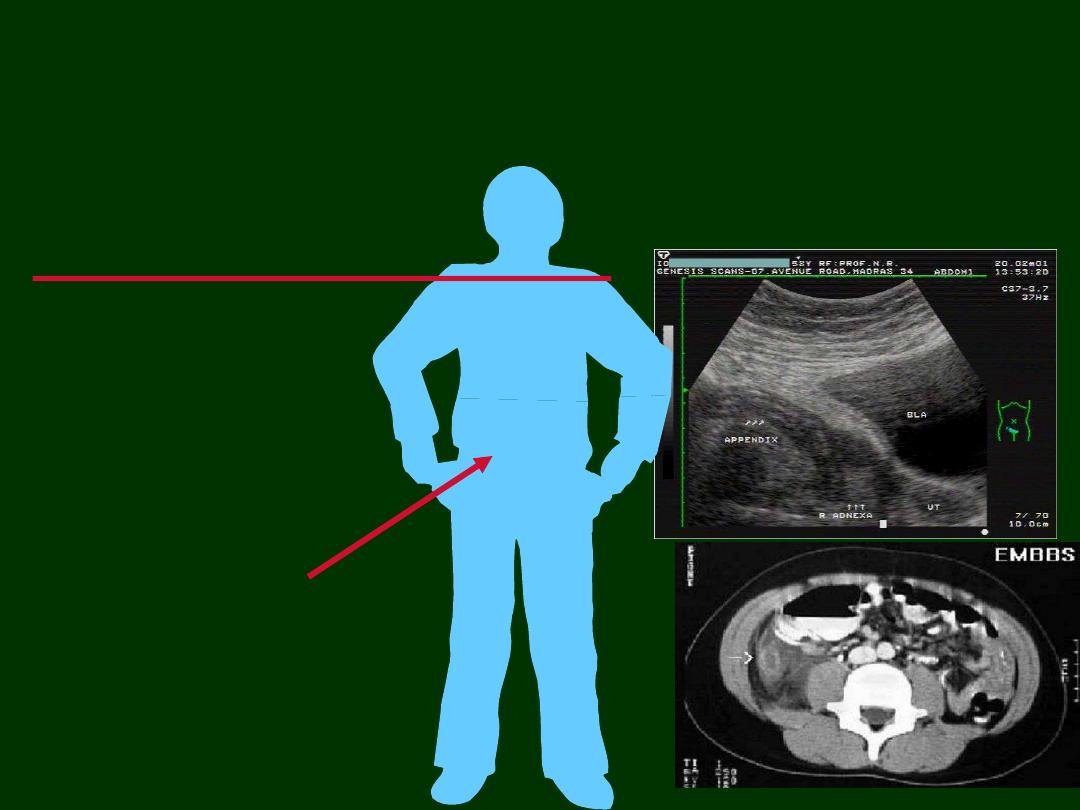
Right lower quadrant
:
Acute appendicitis.
Acute terminal ileitis.
Acute typhlitis.
Pelvic inflammatory disease.
Complications of overian cyst.
Endometriosis.
Ectopic pregnancy.
Common causes of acute pain in
an abdominal quadrant
Left lower quadrant
:
Diverticulitis.
Epiploic appendagitis.
Pancreatitis
Ulcer
Diverticulitis
Cholecystitis
Appendicitis
Approach
Detailed History..
Physical Examination..
Investigations..
Hematological, Serological, chemicals, etc
Radiological
X-ray
US
CT
General Considerations
Clinical assessment is often difficult.
Laboratory investigations are often non
specific.
Clinical presentation
Abdominal pain, distension & constipation.
Nausea & Vomiting
Failure to pass flatus
On examination:
Negative bowel sound
Tenderness
Systemic symptoms.
General Considerations
Imagining Modalities
Plain X-ray
Ultra sonography
CT examinations
Contrast studies
Plain Radiograph
Plain Abdominal X-Ray
Plain radiographs of the abdomen
is the initial radiological
approach, but had a significant diagnostic limitations
(may confirm the diagnosis but lack of specificity
–
cannot detect the cause in most of cases).
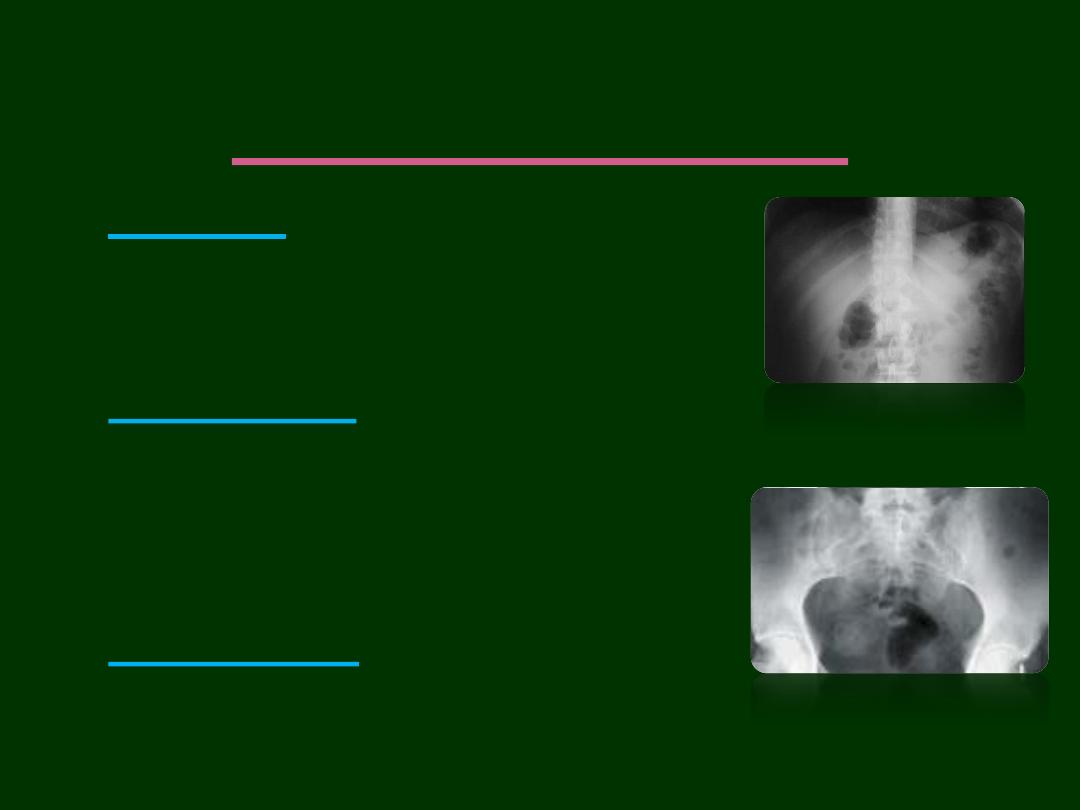
X-ray in general:
Cheap
Easy and rapid
Widely available
Good diagnostic value
CT is clearly superior to plain radiography
CT can:
Confirming the
diagnosis (site and level)
Revealing the
cause of bowel obstruction
Detecting
pneumoperitoneum
Identifying
ureteric stones
.
Examining
solid organs.
The major obstacle of CT vs plain abdominal
radiography appears to be regarding:
Cost
Availability
Radiation dose
Value of CT

How to examine the X-ray
Firstly, you should know that:
There are 5 basic radiographic
densities
1.
Black
—gas
2.
Dark gray
—fat
3.
Gray
—soft tissues
4.
White
—calcified structures & Bones
5.
Dense white
—metallic objects

Gas pattern
Air fluid level
Extra-luminal air
Soft tissue masses
Calcular shadows
Calcifications
Skeletal pathology
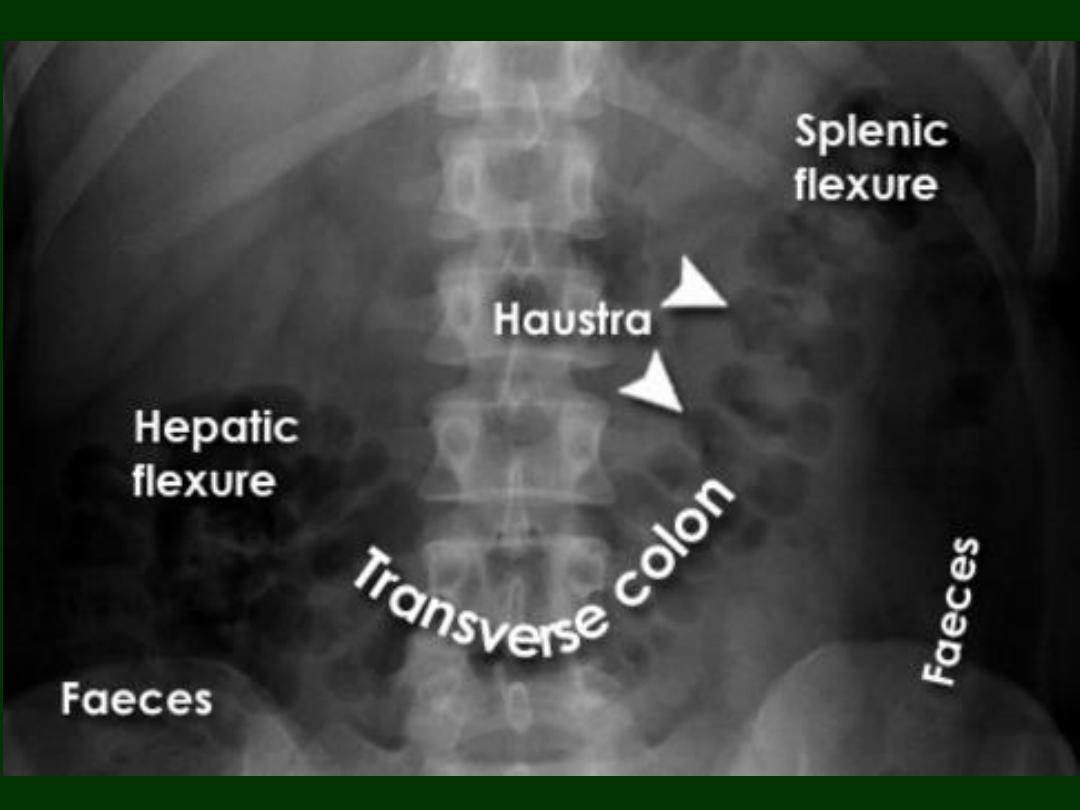
How to examine the X-ray
Normal Gas Pattern
Stomach
Always
Small Bowel
Two or three loops of non-distended bowel
Normal diameter = 2.5 cm
Large Bowel
In rectum or sigmoid
– almost always

Gas in
stomach
Gas in a few
loops of
small bowel
Gas in
rectum or
sigmoid
Normal Gas Pattern
Normal Fluid Levels
Stomach
Always (except supine film)
Small Bowel
Two or three levels possible
Large Bowel
None normally

Erect Abdomen
Always
air/fluid level
in stomach
A few
air/fluid
levels in
small bowel
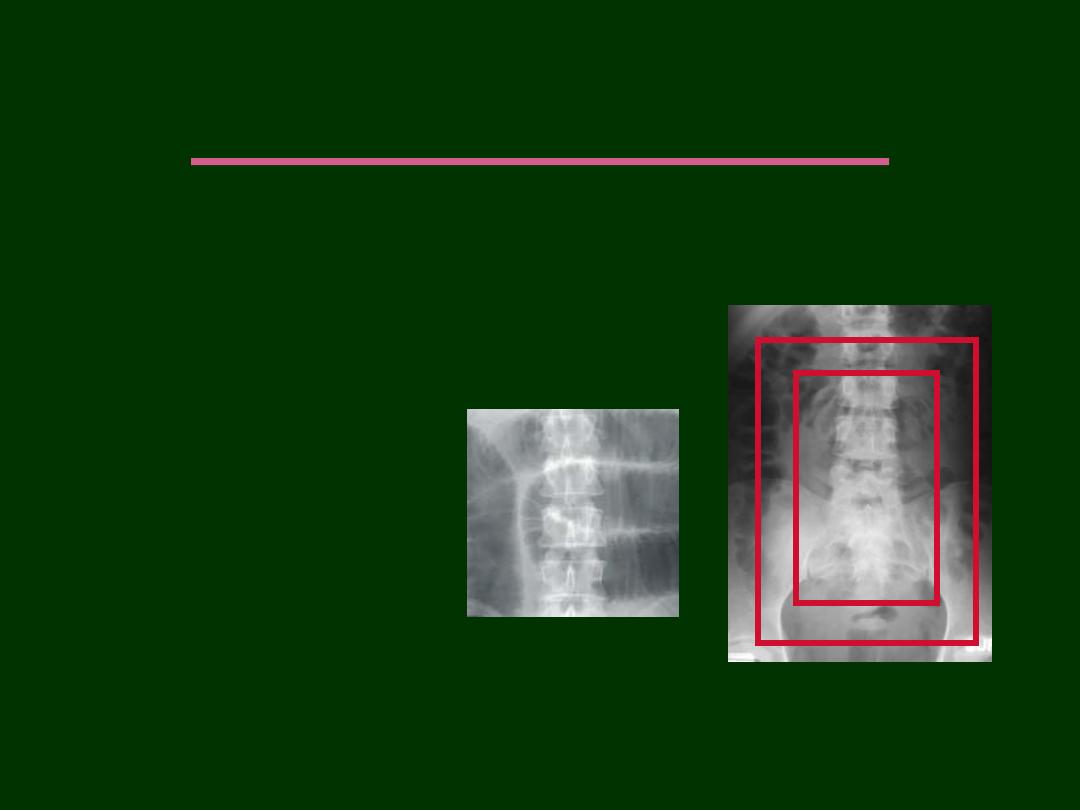
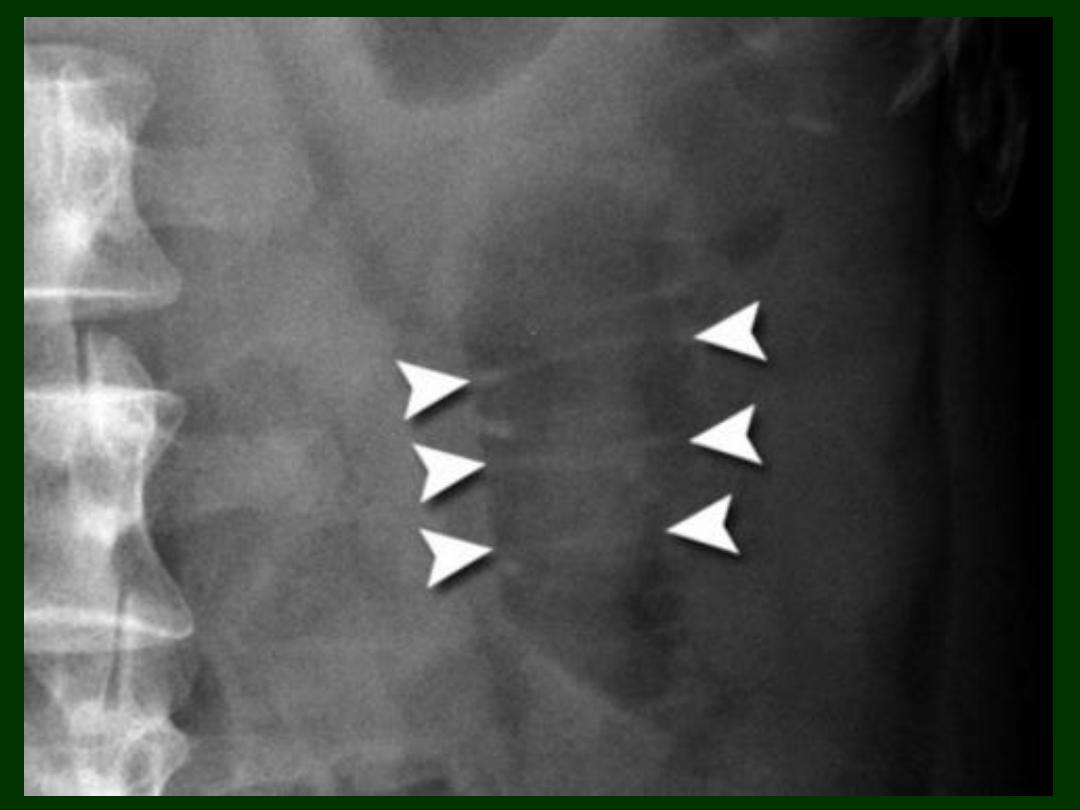
Large vs. Small Bowel
Large Bowel
Peripheral
Haustral markings are thick
don't extend from wall to wall
Small Bowel
Central
Valvulae are thin & extend
across lumen
Bowel obstructions
Bowel obstructions
are common and
account for 20% of admissions with
surgical abdomens.
Radiology is important in confirming the
diagnosis and identifying the underlying
cause.
Bowel Obstruction
1.
Functional Obstruction
Sentinel loop
Post operative ileus
Adynamic (paralytic) ileus
2.
Mechanical Obstruction
SBO
LBO
Functional
Obstruction
Functional Obstruction
(Sentinel loop, Post operative ileus, Adynamic (paralytic) ileus)
Failure of passage of enteric contents through
small bowel and colon that is not mechanically
obstructed.
Occur due to the paralysis of intestinal motility.
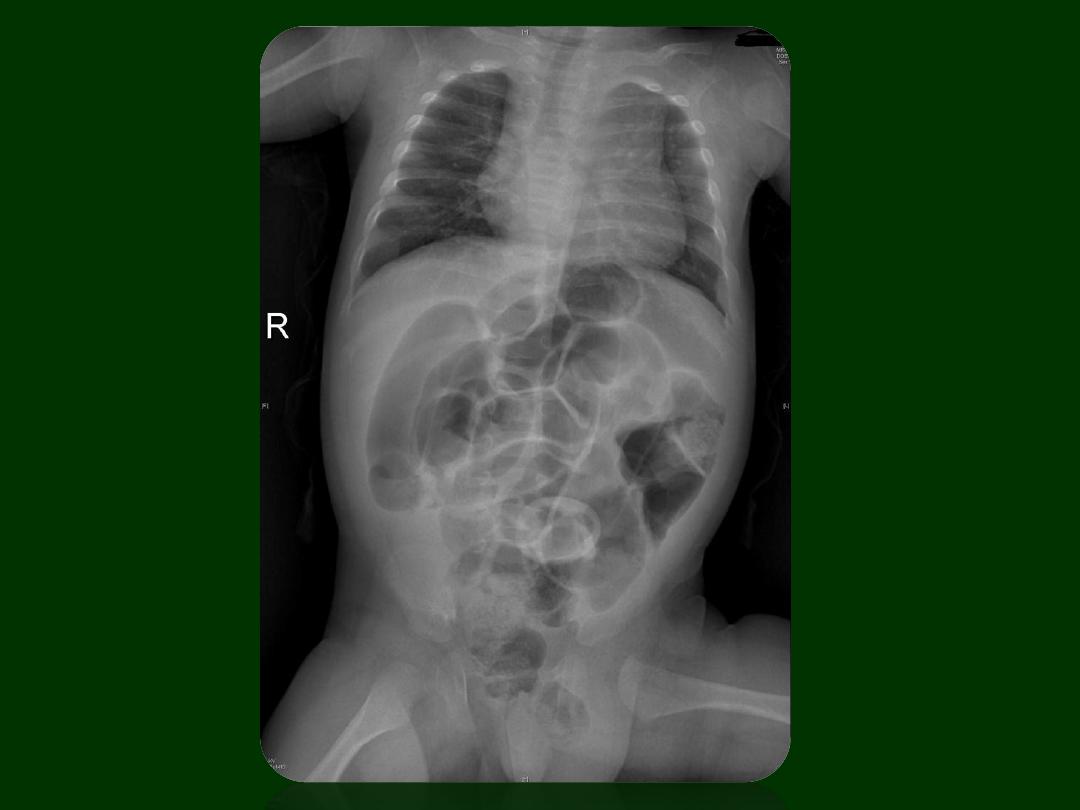
Radiographic Features
Gas in dilated small bowel and large bowel to rectum
(Generalized , uniform, gaseous distension of the
large
and
small
bowel).
involvement of large bowel and
lack
of a transition point
help distinguish it from
small bowel obstruction
Long air-fluid levels
Functional Obstruction
(Sentinel loop, Post operative ileus, Adynamic (paralytic) ileus)
when localized, it will be:
sentinel loop
Post operative ileus
is normal and expected
finding after abdominal surgery.
Recovery times have been reported at:
small intestine: 0-24 hours
stomach: 24-48 hours
colon: 48-72 hours
Prolonged postoperative ileus (>72 hours) has
been termed "
paralytic
" ileus by some and is
concerning for small bowel obstruction, bowel
perforation, peritonitis and intra-abdominal
abscess.
Sentinel Loops
Supine
Prone
One or two persistently dilated loops of
large or small bowel
Gas in rectum or sigmoid
Localized Ileus Key Features

Localized Ileus
Pitfalls
May resemble early
mechanical SBO
Clinical course
Get follow-up
Gas in dilated small bowel and large bowel to rectum
Long air-fluid levels
Only post-op patients have generalized ileus
Other causes:-
Peritonitis
Hypokalemia
Metabolic disorder as hypothyroidism
Vascular occlusion
Generalized Ileus
Key Features
Generalized Adynamic Ileus
Supine
Erect

Is It An Ileus?
Is the patient immediately post-op?
Are the bowel sounds absent or hypoactive?
Mechanical
Obstruction
SBO & LBO
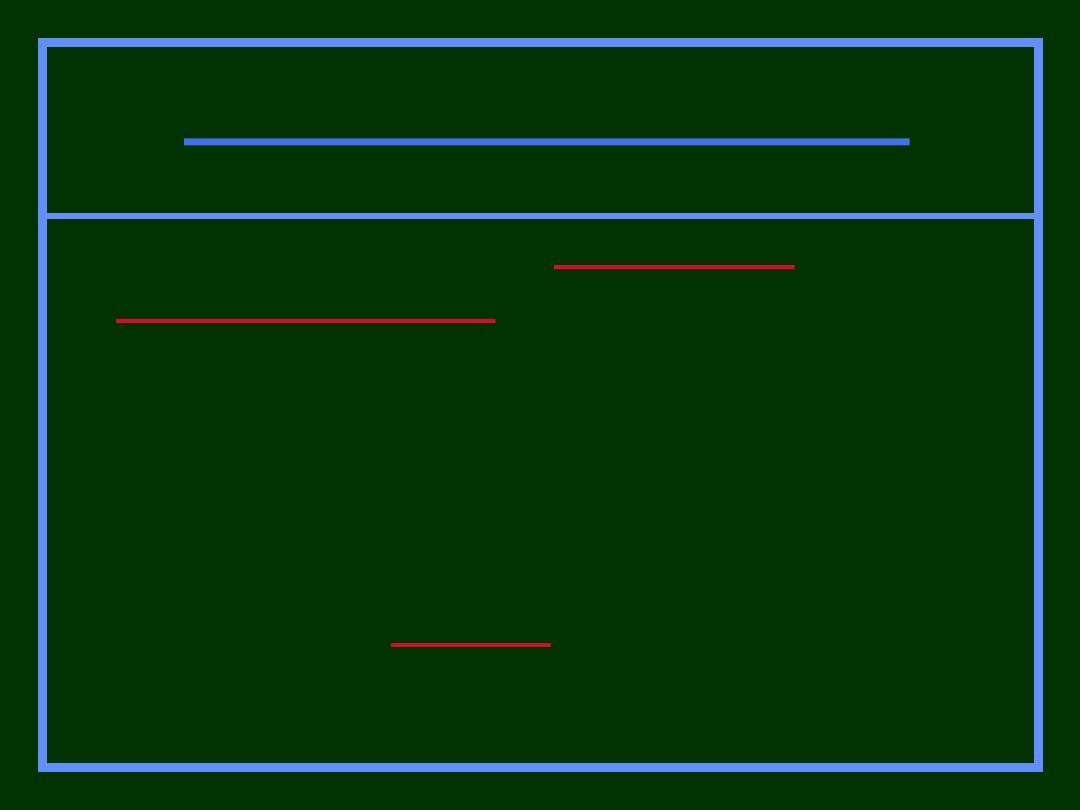
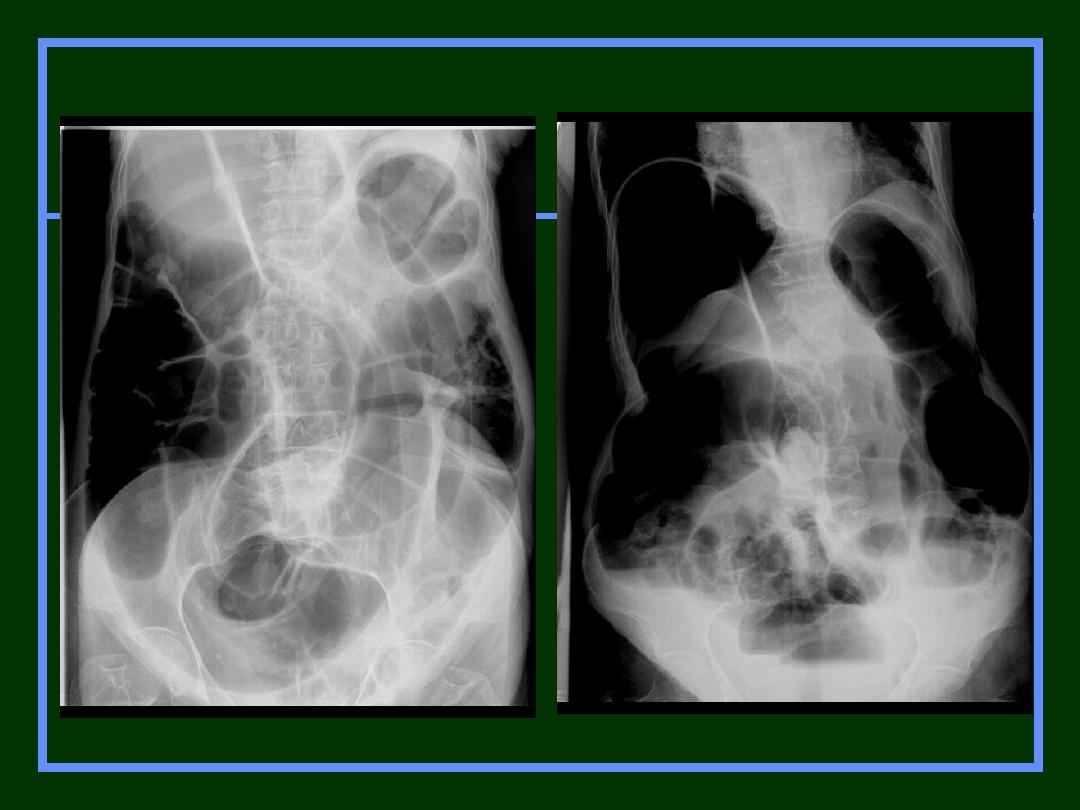
Small bowel obstruction
Small bowel obstruction (SBO)
accounts for
80% all
mechanical intestinal obstruction
; the
remaining 20% result from
large bowel
obstruction
.
It has a mortality rate of 5.5%.
Clinical presentation
Classical presentation is constipation, increasing
abdominal distension with nausea and vomiting.
Radiograph features of SBO
Abdominal radiographs are only 50-60% sensitive for
small bowel obstruction.
In most cases, the abdominal radiograph will have the
following features:
dilated small bowel loops proximal to the obstruction.
predominantly central dilated loops.
three instances of dilatation over 3 cm.
are visible.
fluid levels if the study is erect.
Fighting loops.
Little gas in colon, especially rectum.



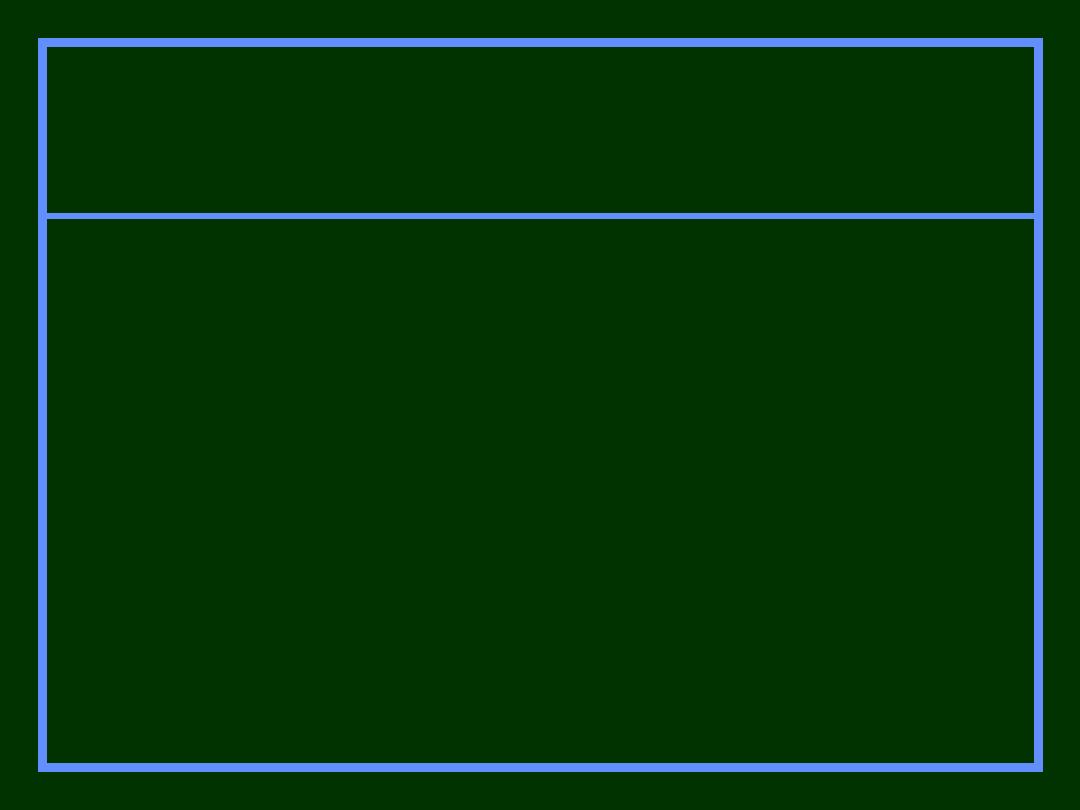
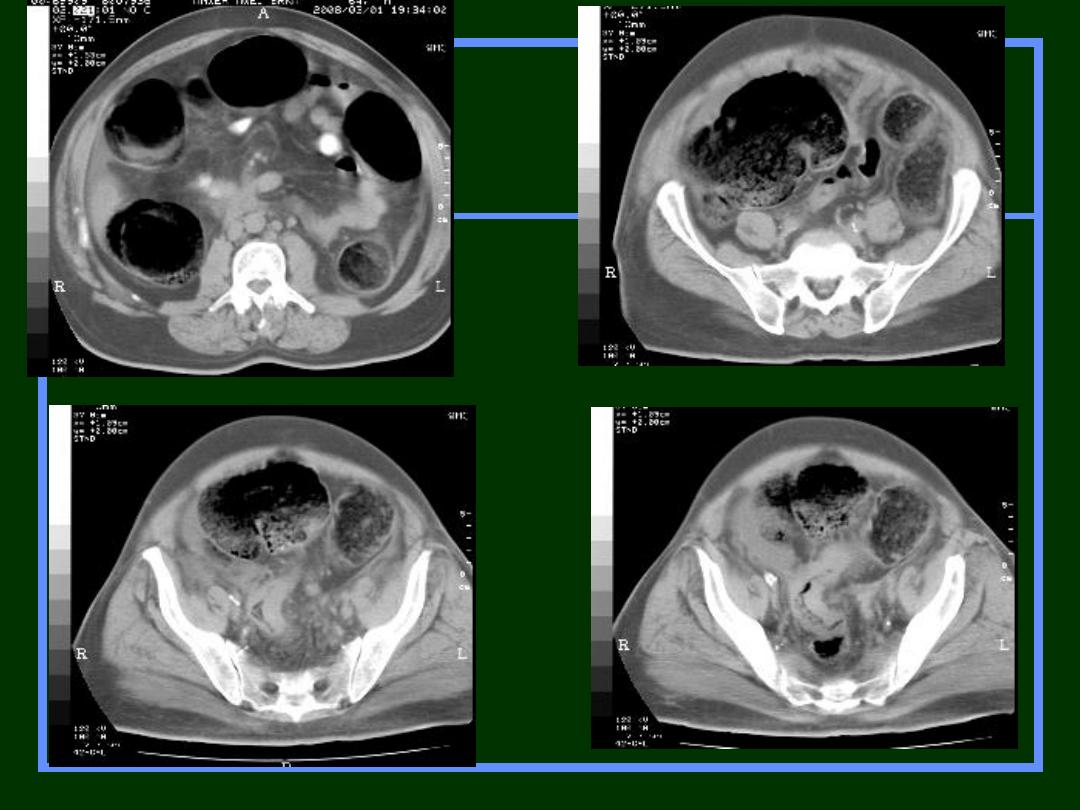
CT
CT is more sensitive than radiographs and
will demonstrate the cause in ~80% of
cases.
There are variable criteria for maximal
small bowel obstruction, but 3.5 cm is a
conservative estimate of dilated bowel.

Mechanical SBO
Causes
Adhesions
Hernia*
Volvulus
Gallstone ileus*
Intussusception
*Cause may be visible on plain film

Mechanical SBO
Pitfalls
Early SBO may
resemble localized
ileus -get F/O
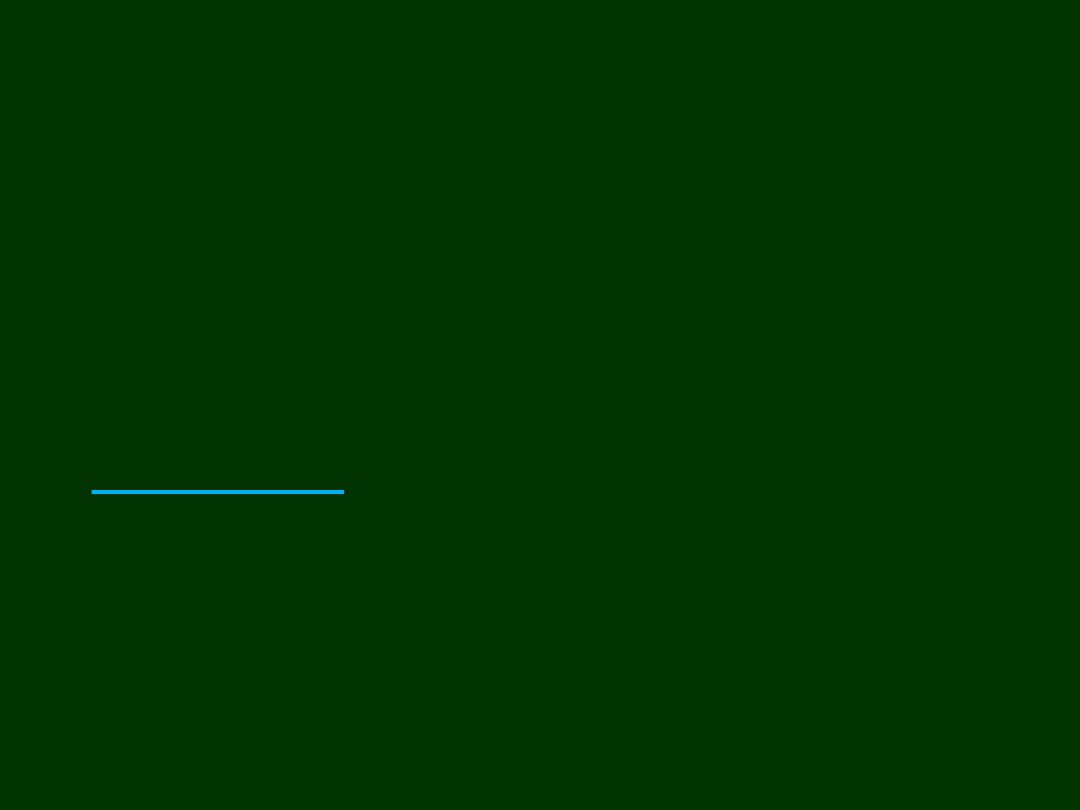
Large bowel obstruction
Large bowel obstructions
are far less common
than small bowel obstructions, accounting for only
20% of all bowel obstructions
.
Clinical presentation
Presentation is typically with abdominal pain,
distension and failure of passage of flatus & stool.
Eventually signs of peritonism, sepsis and shock
develop, when
perforation occurs
.
•colonic distension: gaseous secondary to gas-
producing organisms in faeces
•collapsed distal colon
•small bowel dilatation, depends on
•duration of obstruction
•incompetence of the ileocaecal valve
•In advanced cases one may see the signs of an
ischemic colon:
•intramural gas (
)
•free intra-abdominal gas (
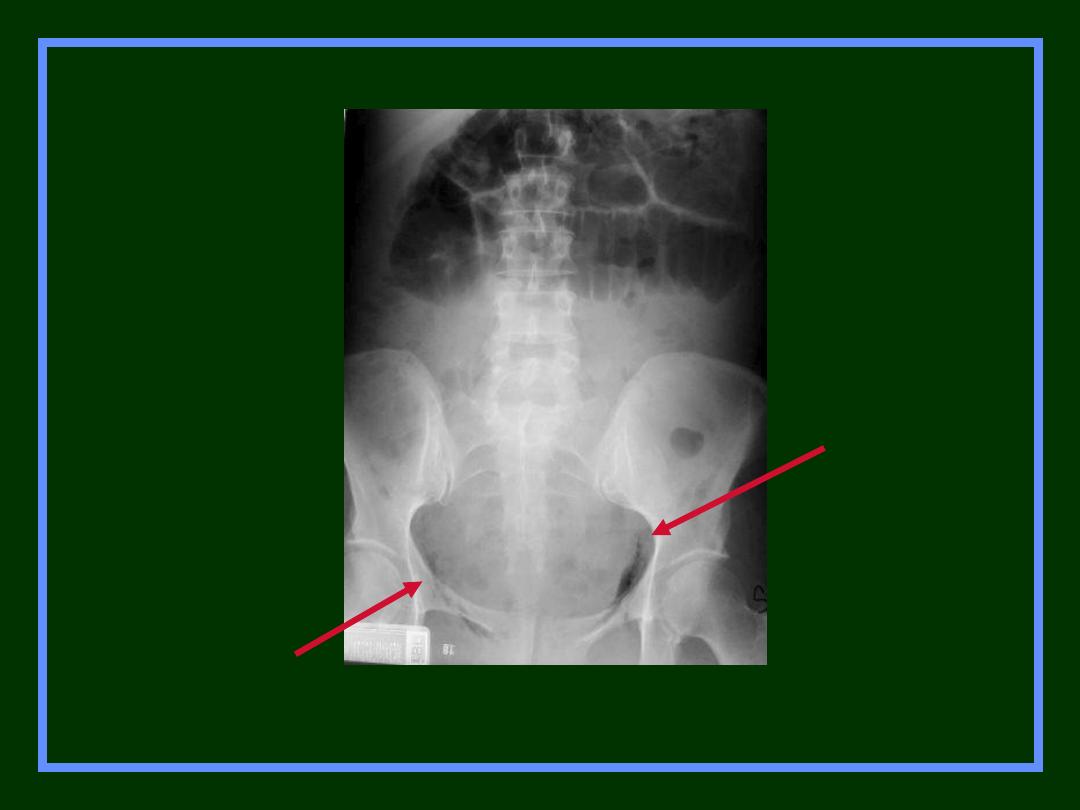
Radiograph features of LBO
LBO
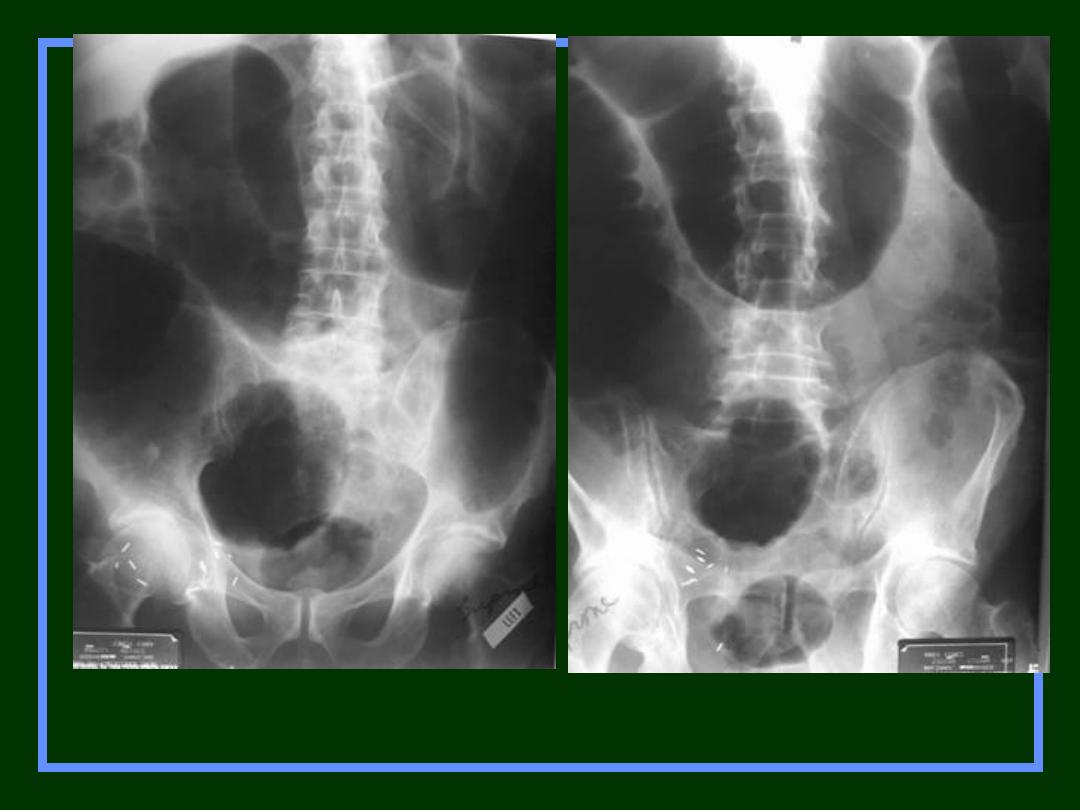
LBO
Supine
Prone

Mechanical LBO
Causes
Tumor
Volvulus
Hernia
Diverticulitis
Intussusception

Carcinoma of Sigmoid
– LBO –
Decompressed into SB
Prone
Supine
Air in Rectum
or sigmoid
Air in Small
Bowel
Air in Large
Bowel
Localized
Ileus
Yes
2-3 distended
loops
Air in rectum or
sigmoid
Generalized
Ileus
Yes
Multiple
distended loops
Yes-
Distended
SBO
No
Multiple dilated
loops
No
LBO
No
None-unless
ileocecal valve
incompetent
Yes-
Dilated
The goals of imaging in a patient with suspected
intestinal obstruction have been defined and are as
follows:
1.
To confirm that it is a true obstruction and to
differentiate it from an ileus.
2.
To determine the level of obstruction.
3.
To determine the cause of the obstruction.
4.
To look for findings of strangulation.
5.
To allow a good management either medically or
surgically by laparoscopy or laparoscopy).

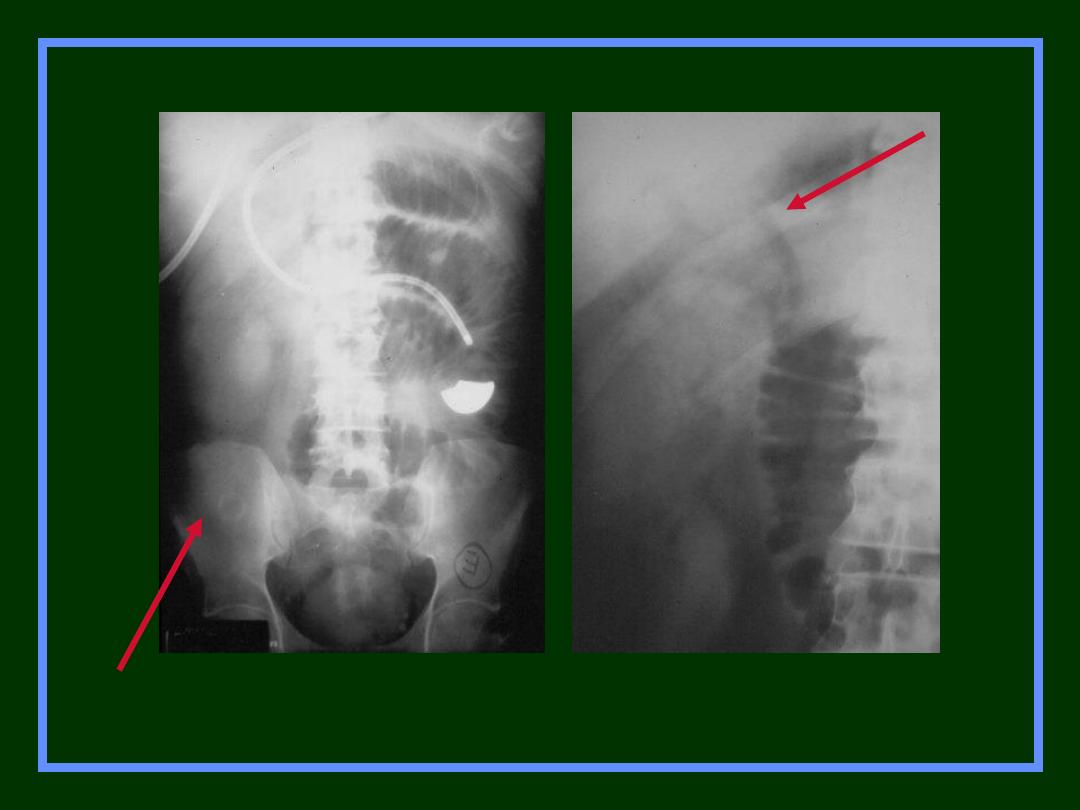
Air in
biliary
tree
Gallstone
Gallstone Ileus

Post-op C-section
Adynamic Ileus
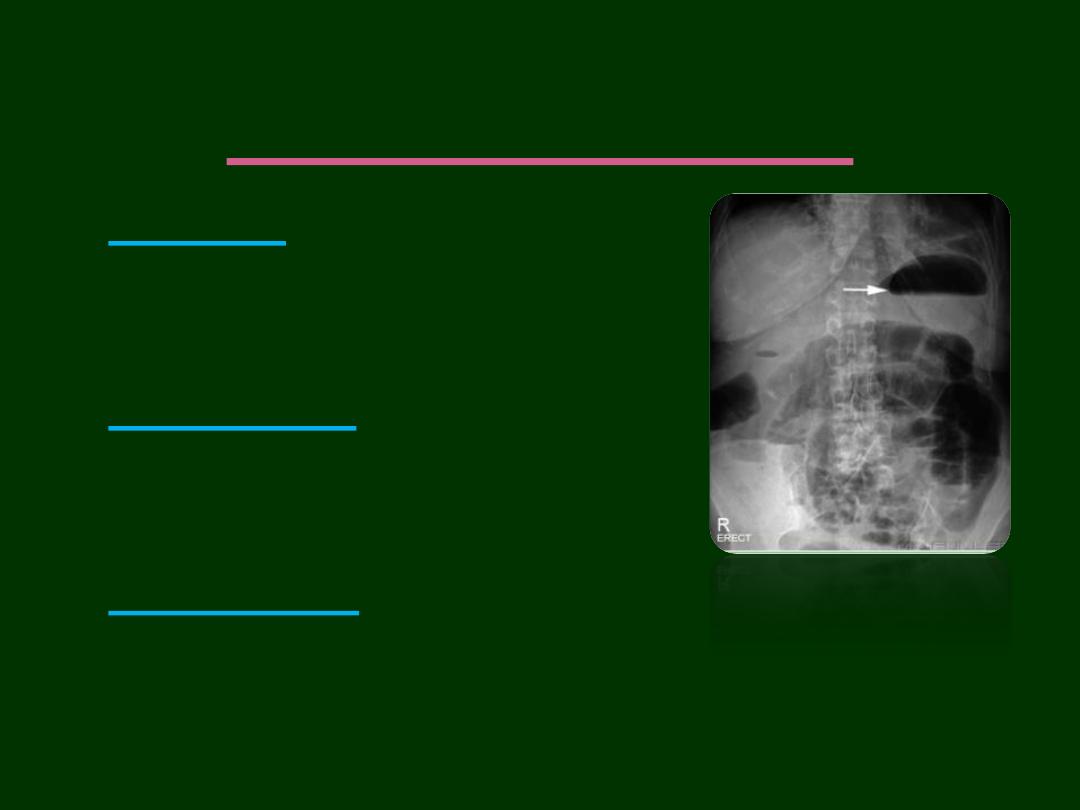
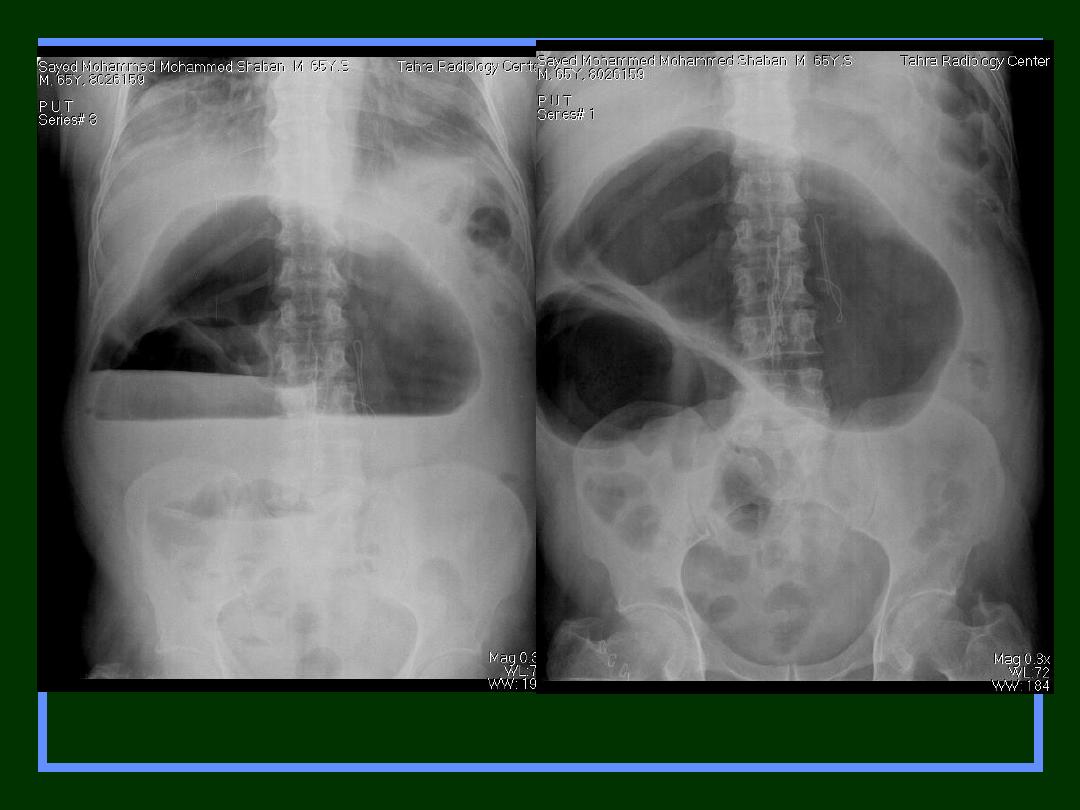
Extra-luminal Air
Free Intra-peritoneal Air
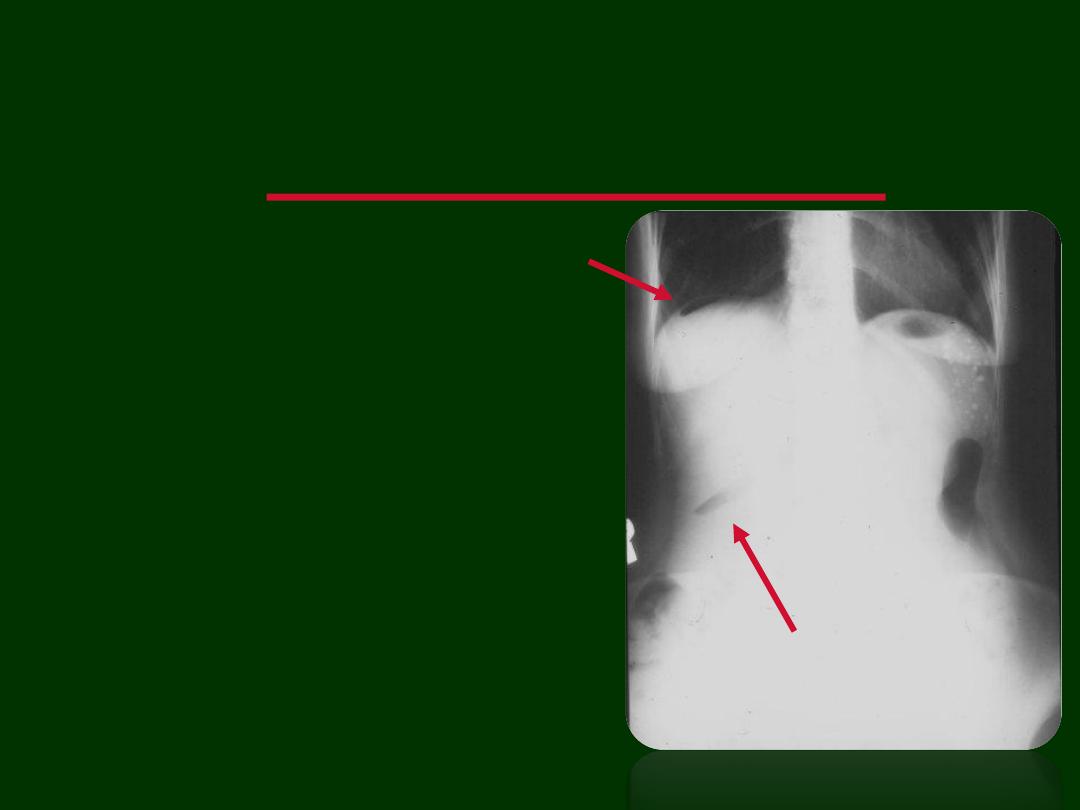
Signs of Free Air-
Pneumoperitoneum
1.
Air under diaphragm
2.
Rigler sign: Air on both
sides of bowel wall
3.
Falciform ligament sign
4.
Air In the biliary system
Crescent
sign
Free Intraperitoneal Air
Rigler sign
The
Rigler sign
, also known as the
double wall
sign
, is seen on an x-ray of the abdomen when
air is present on both sides of the intestine, i.e.
when there is air on both the luminal and
peritoneal side of the bowel wall.
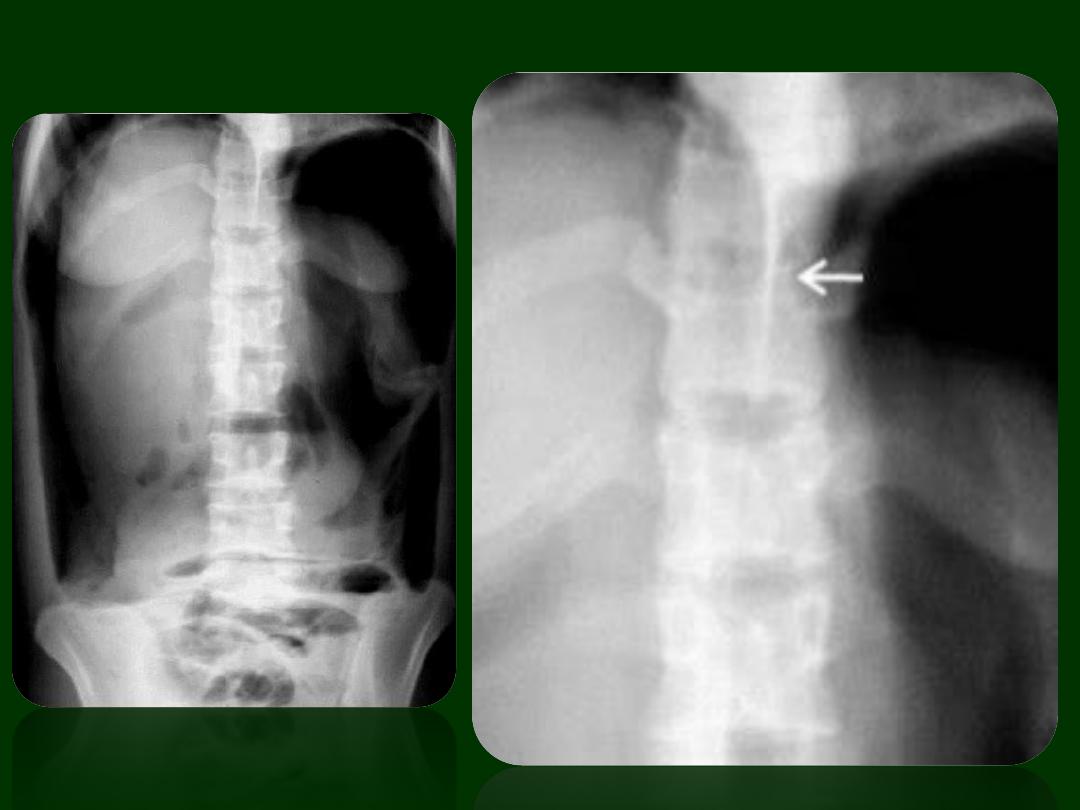
Falciform ligament sign
The
falciform ligament sign
is a sign seen with a
pneumoperitoneum.
It is almost never seen in isolation. If there is enough free
air to outline the falciform ligament, there is usually
enough air to also provide at least a
Rigler's sign
.
The falciform ligament connects the anterior abdominal
wall to the liver. The ligament continues to extend
inferiorly beyond the liver where it becomes the round
ligament (white arrow). Given that the falciform ligament
is situated against the anterior abdominal wall, it is not
surprising that it becomes outlined with air in a supine
patient with free abdominal gas.

Free Air
Causes
Rupture of a hollow viscus
Perforated ulcer
Perforated diverticulitis
Perforated carcinoma
Trauma or instrumentation
Post-op 5
–7 days
Extraperitoneal Air
thank you