
Urticaria (hives, ‘nettle-rash’)
Is common
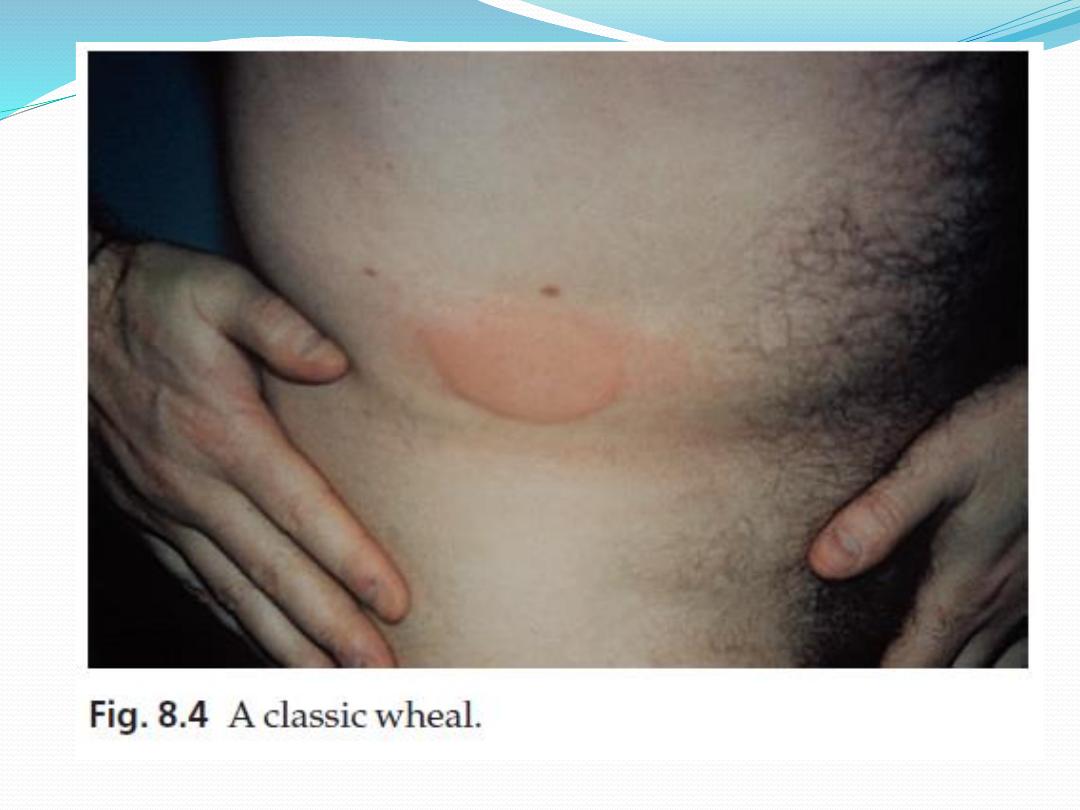
pink, itchy or ‘burning’ swellings (wheals) can occur
anywhere on the body.
Individual wheals do not last longer than 24 h, but new
ones may continue to appear for days, months or even
years.
urticaria is divided into acute less than 6 weeks, and
chronic forms, for more than 6 weeks.
Most patients with chronic urticaria, other than those with
an obvious physical cause, have what is often known as
‘ordinary urticaria’.
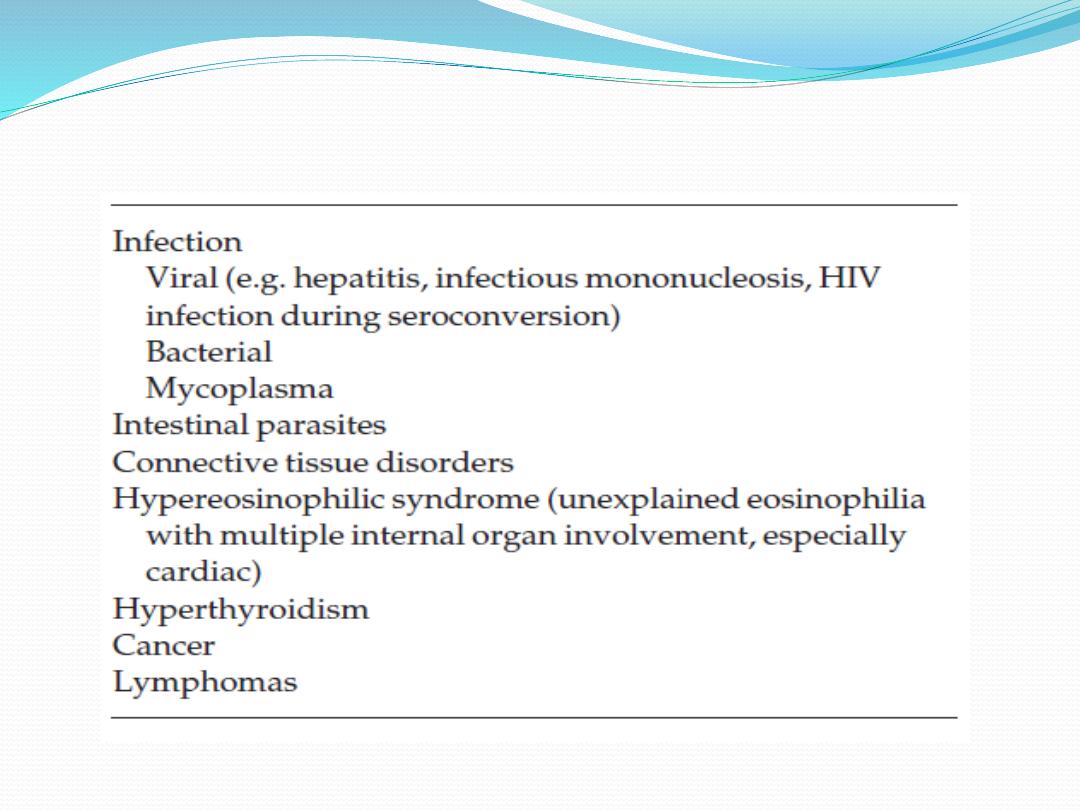
Causes-endogenous
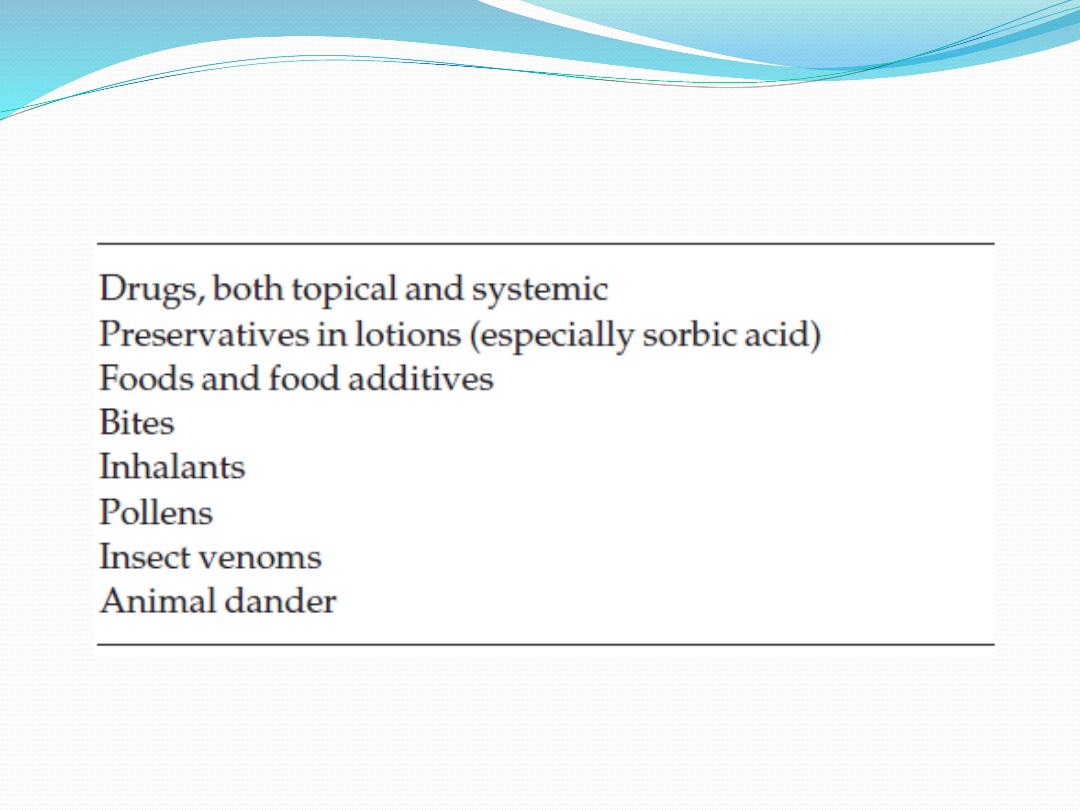
Causes, Exogenous

Pathophysiology
The signs and symptoms of urticaria are caused by
mast cell degranulation, with release of histamine,
increased capillary permeability leading to transient
leakage of fluid into the surrounding tissue and
development of a wheal
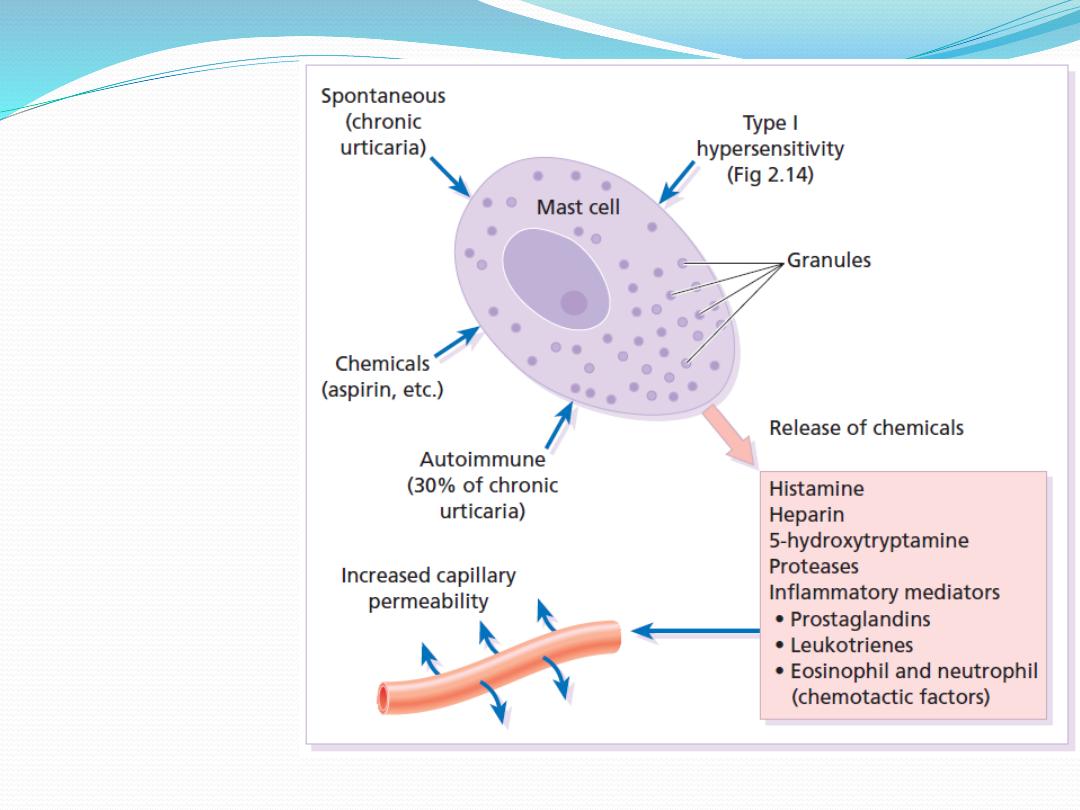
Ways in which
a mast cell
can be
degranulated
and the
ensuing
reaction.
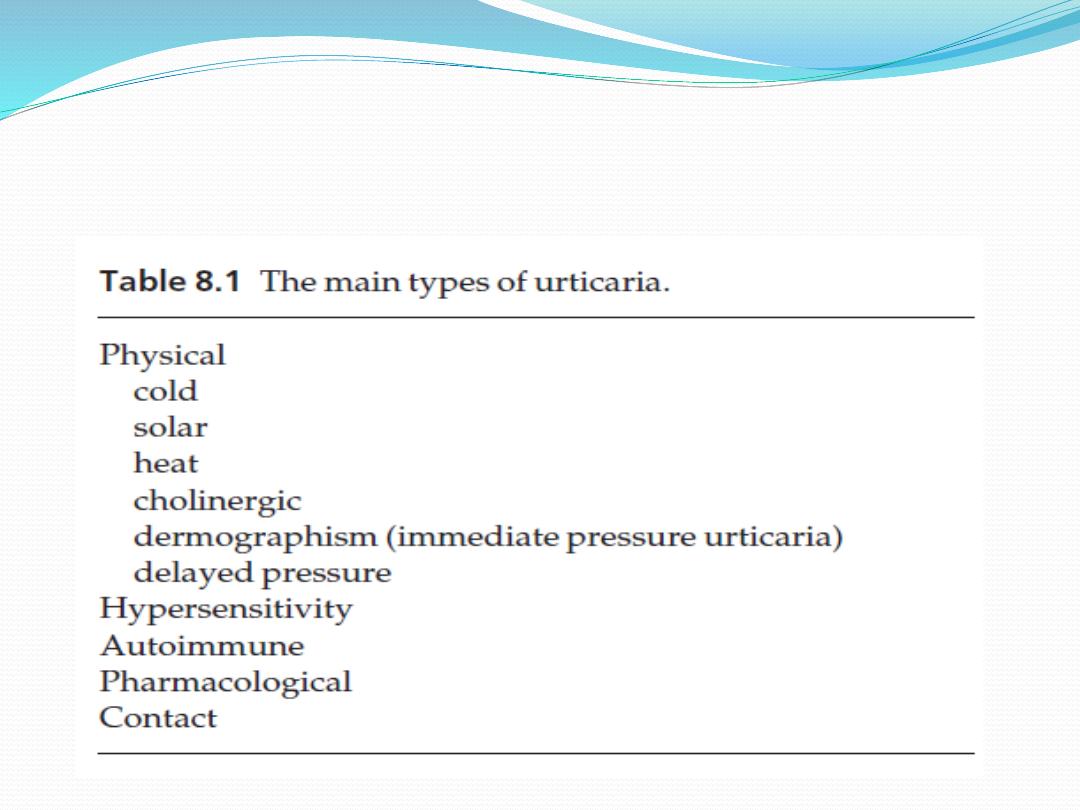
Classification

Physical urticarias
Cold urticaria
Patients develop wheals in areas exposed to cold (e.g. on
the face when cycling or freezing in a cold wind).
A useful test in the clinic is to reproduce the reaction by
holding an ice cube, in a thin plastic bag to avoid wetting,
against forearm skin.
A few cases are associated with the presence of
cryoglobulins, cold agglutinins or cryofibrinogens.
Solar urticaria
Wheals occur within minutes of sun exposure.
most have an IgE-mediated urticarial reaction to sunlight.
Some patients with solar urticaria have erythropoietic
protoporphyria

Heat urticaria
In this condition wheals arise in areas after contact with
hot objects or solutions.
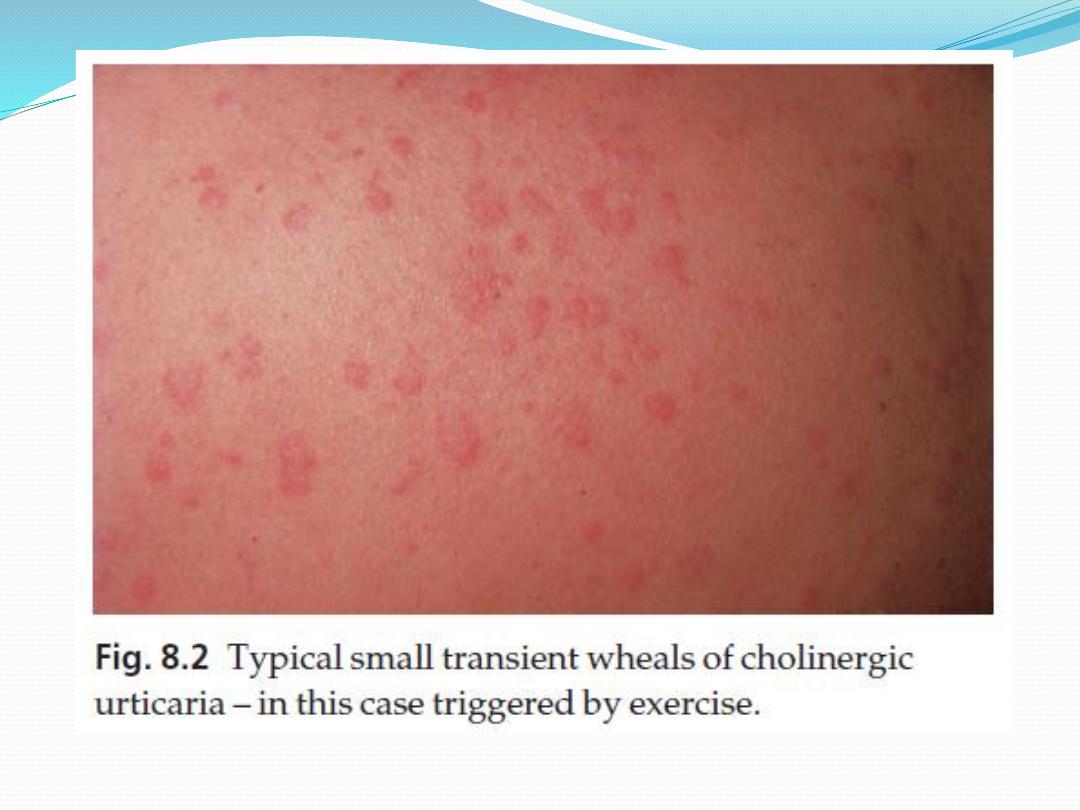
Cholinergic urticaria
Elicited by axiety, heat, sexual excitement or strenuous
exercise
The vessels over-react to acetylcholine liberated from
sympathetic nerves in the skin.
Transient 2–5 mm follicular macules or papules resemble a
blush or viral exanthem
Aquagenic urticaria
precipitated by contact with water, irrespective of its
temperature.

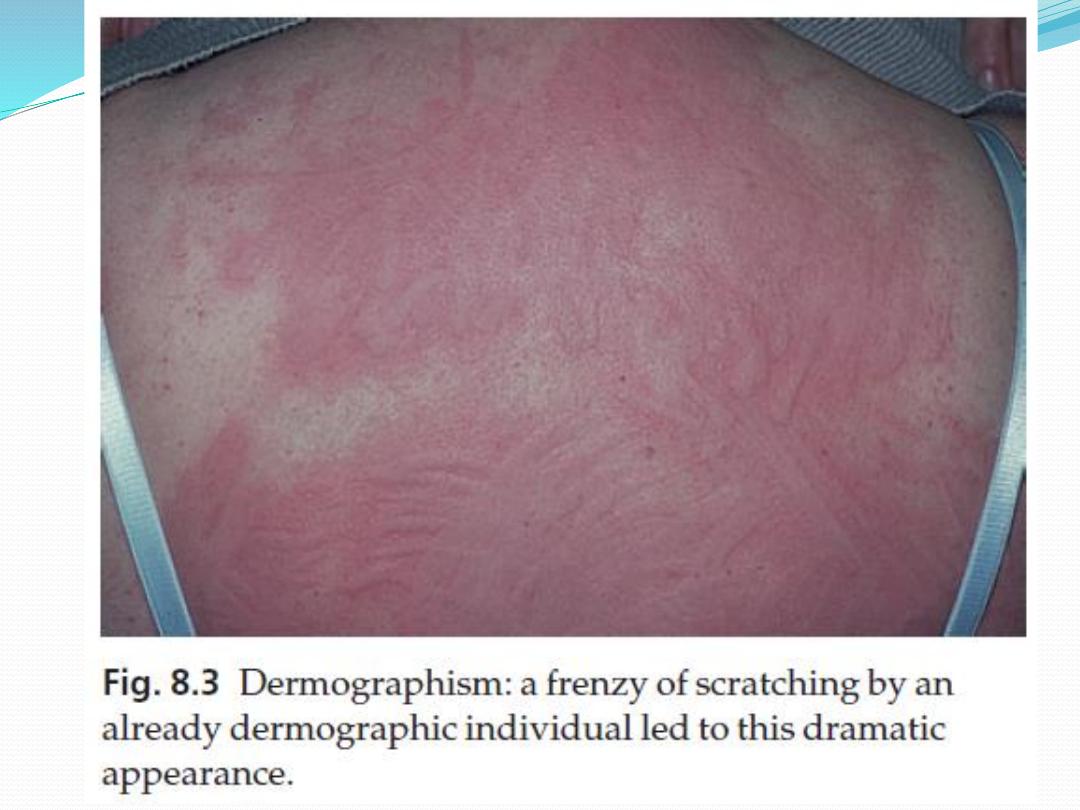
Dermographism
This is the most common type of physical urticaria
the skin mast cells releasing extra histamine after rubbing or
scratching, the linear wheals are therefore an exaggerated triple
response of Lewis.
They can be reproduced by scratching the back with a fingernail or
blunt object.
Delayed pressure urticaria
Sustained pressure causes oedema of the underlying skin and
subcutaneous tissue 3–6 h later.
last up to 48 h
kinins or prostaglandins, rather than histamine, probably mediate it.
It occurs particularly on the feet after walking, on the hands after
clapping and on the buttocks after sitting.

Other types of urticaria
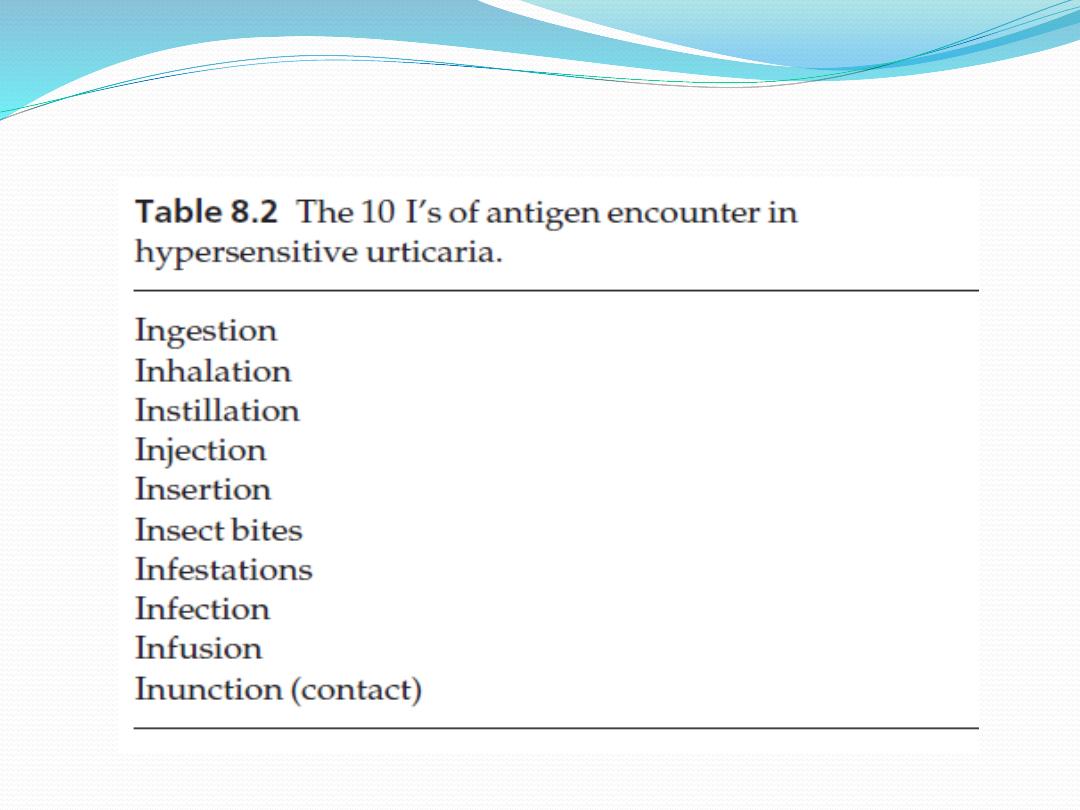
Hypersensitivity urticaria
common form of urticaria is caused by hypersensitivity, often
an IgE-mediated (type I) allergic reaction
Allergens may be encountered in 10 different ways (the 10 I’s)
Autoimmune urticaria
Some patients with chronic urticaria have an autoimmune
disease with IgG antibodies to IgE or to FcIgE receptors on
mast cells, here the autoantibody acts as antigen to trigger
mast cell degranulation.
Pharmacological urticaria
This occurs when drugs cause mast cells to release histamine
in a non-allergic manner (e.g. aspirin, non-steroidal anti-
inflammatory drugs [NSAIDs], angiotensin-converting
enzyme [ACE] inhibitors and morphine).

Contact urticaria
The allergen is delivered to the mast cell from the skin
surface rather than from the blood.
Wheals occur most often around the mouth as foods
and food additives are the most common culprits but
drugs, animal saliva, caterpillars, insect repellents and
plants may cause the reaction.
Recently, latex allergy has become a significant public
health concern.

Latex allergy
Possible reactions to the natural rubber latex include:
1.
contact irritant dermatitis
2.
contact allergic dermatitis
3.
type I allergy, include hypersensitivity urticaria (both by contact and
by inhalation), hay fever, asthma, anaphylaxis and, rarely, death.
Cornstarch powder in medical gloves bound to the latex proteins so that
the allergen became airborne when the gloves were put on.
Individuals at increased risk of latex allergy include health care workers,
those undergoing multiple surgical procedures (e.g. spina bifida patients)
Around 1–6% of the general population is believed to be sensitized to
latex.
Prevention of latex allergy by using non-latex (e.g. vinyl) gloves
should be worn by those not handling infectious material (e.g. caterers)
and, if latex gloves are chosen for those handling infectious material, then
powder-free low allergen ones should be used.

Presentation
Wheals
sudden appearance of pink itchy wheals, which can come up anywhere
on the skin surface
Each lasts for less than a day, and most disappear within a few hours.
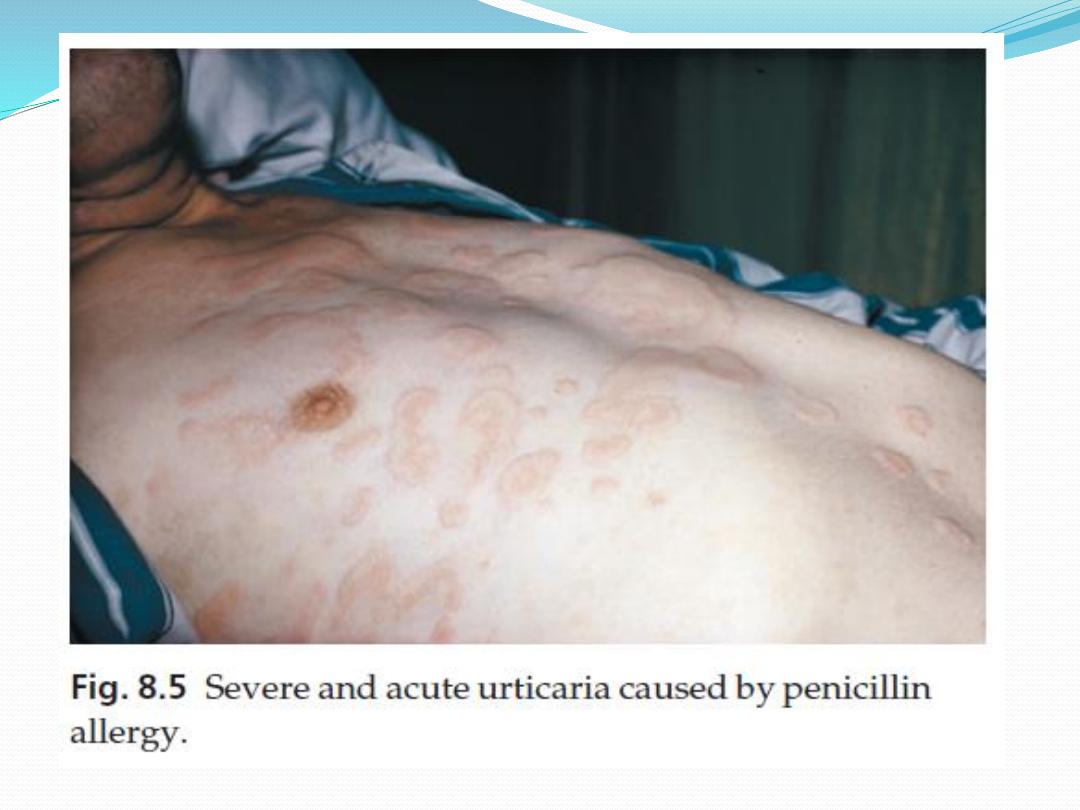
Lesions may enlarge rapidly and some resolve centrally to take up an
annular shape.
In an acute anaphylactic reaction, wheals may cover most of the skin
surface.
in chronic urticaria only a few wheals may develop each day.
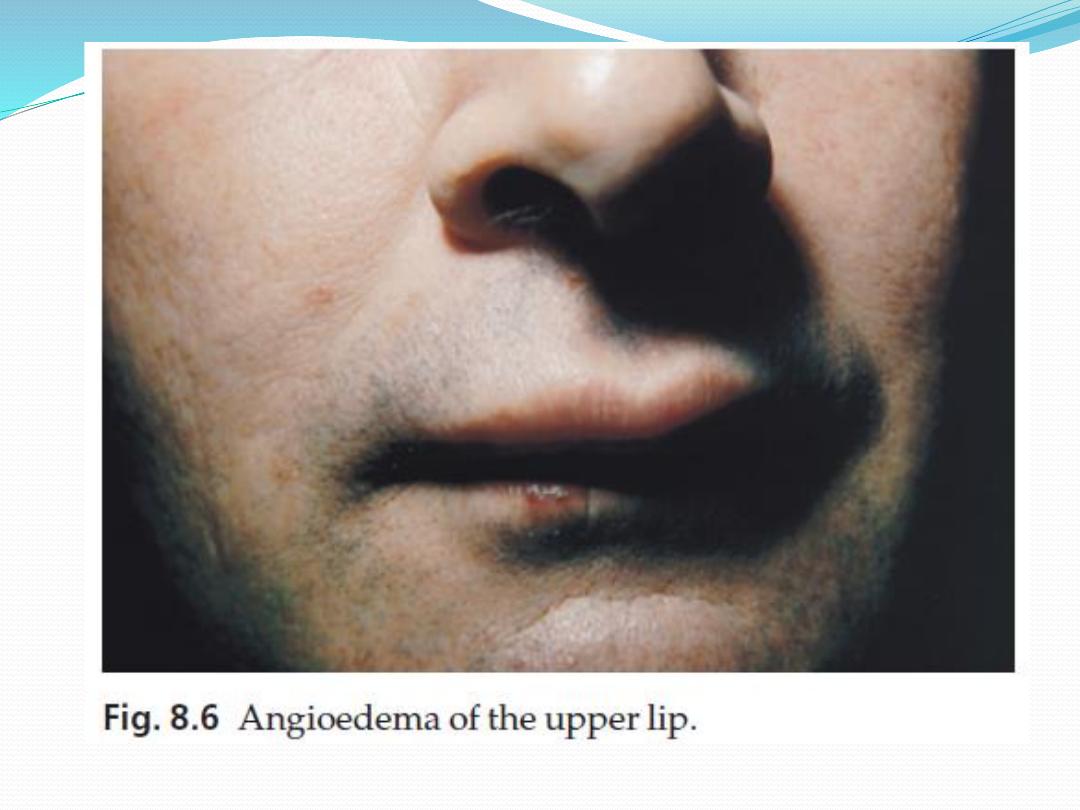
Angioedema
is a variant of urticaria that primarily affects the subcutaneous tissues,
so that the swelling is less demarcated and less red than an urticarial
wheal.
Angioedema most commonly occurs at junctions between skin and
mucous membranes (e.g. peri-orbital, peri-oral and genital).
It may be associated with swelling of the tongue and laryngeal mucosa


Course
depends on its cause
If the urticaria is allergic, it will continue until the
allergen is removed, tolerated or metabolized.
Most such patients clear up within a day or two, even if
the allergen is not identified but may recur if the
allergen is met again.
only half of patients attending hospital clinics with
chronic urticaria and angioedema will be clear 5 years
later.
Those with urticarial lesions alone do better, half
being clear after 6 months.

Complications
itch may be enough to interfere with sleep or daily
activities and to lead to depression.
In acute anaphylactic reactions, oedema of the larynx
may lead to asphyxiation, and oedema of the tracheo-
bronchial tree to asthma.

Differential diagnosis
There are two aspects to the differential diagnosis of urticaria.
The first is to tell urticaria from other eruptions that are not urticaria at all.
The second is to define the type of urticaria
DDX
1.
Insect bites or stings and infestations commonly elicit urticarial responses,
but these may have a central punctum and individual lesions may last longer
than 24 h.
2.
Erythema multiforme can mimic an annular urticaria.
3.
urticarial vasculitis may resemble urticaria, but individual lesions last for
longer than 24 h, blanch incompletely and may leave bruising in their wake.
4.
Some bullous diseases (e.g. dermatitis herpetiformis, bullous pemphigoid
and pemphigoid gestationis) begin as urticarial papules or plaques, but later
bullae make the diagnosis obvious. In these patients, individual lesions last
longer than 24 h
5.
On the face, erysipelas can be distinguished from angioedema by its sharp
margin, redder colour and accompanying pyrexia.
6.
Hereditary angioedema must be distinguished from the angioedema
accompanying urticaria as their treatments are completely different.

Investigations
The investigations will depend on the type of urticaria.
More is learned from the history than from the laboratory.
The history should include:
1.
details of the events surrounding the onset of the eruption
2.
review of systems may uncover evidence of an underlying
disease
3.
drugs, self-prescribed and over-the-counter medications (e.g.
aspirin and herbal remedies)
If a patient has ordinary urticaria and its cause is not obvious,
investigations are often deferred until it has persisted for a few
weeks or months, and are based on the history.
Many of the physical urticarias can be reproduced by appropriate
physical tests, but it is important to remember that
antihistamines should be stopped for at least 3 days before these
are undertaken.

If no clues are found in the history, investigations can be confined to a
complete blood count and erythrocyte sedimentation rate (ESR).
An eosinophilia should lead to the exclusion of bullous and parasitic
disease
a raised ESR might suggest urticarial vasculitis or a systemic cause.
If the urticaria continues for 2–3 months, the patient may be referred to
a dermatologist for further evaluation of internal disorders associated
with urticaria and on external allergens.
Patients frequently suspect a food allergy, but this is rarely found in
chronic urticaria.
Prick tests are Unhelpful
Even after extensive evaluation and environmental change, the cause
cannot always be found.

Treatment
The ideal is to eliminate the cause
In addition, aspirin – in any form – should be banned.

Antihistamines
are the mainstays of symptomatic treatment.
Cetirizine 10 mg/day and loratadine 10 mg/day, both with half-
lives of around 12 h, are useful. If necessary, these can be
supplemented with shorter acting antihistamines (e.g.
hydroxyzine 10–25 mg up to every 6 h acrivastine 8 mg three
times daily) or with a longer acting antihistamine (e.g.
chlorphenamine [chlorpheniramine] maleate 12 mg sustained-
release tablets every 12 h)
Chlorphenamine or diphenhydramine are often used during
pregnancy because of their long record of safety, but cetirizine,
loratadine and mizolastine should be avoided.
H2- blocking antihistamines (e.g. cimetidine) may add a slight
benefit if used in conjunction with an H1 histamine antagonist.

Sympathomimetic agents can help urticaria.
Pseudoephedrine (30 or 60 mg every 4 h) or
terbutaline (2.5 mg every 8 h) can sometimes be useful
adjuncts.
A tapering course of systemic corticosteroids may
be used, but only when the cause is known and there
are no contraindications
Low doses of ciclosporin may be used for particularly
severe cases.
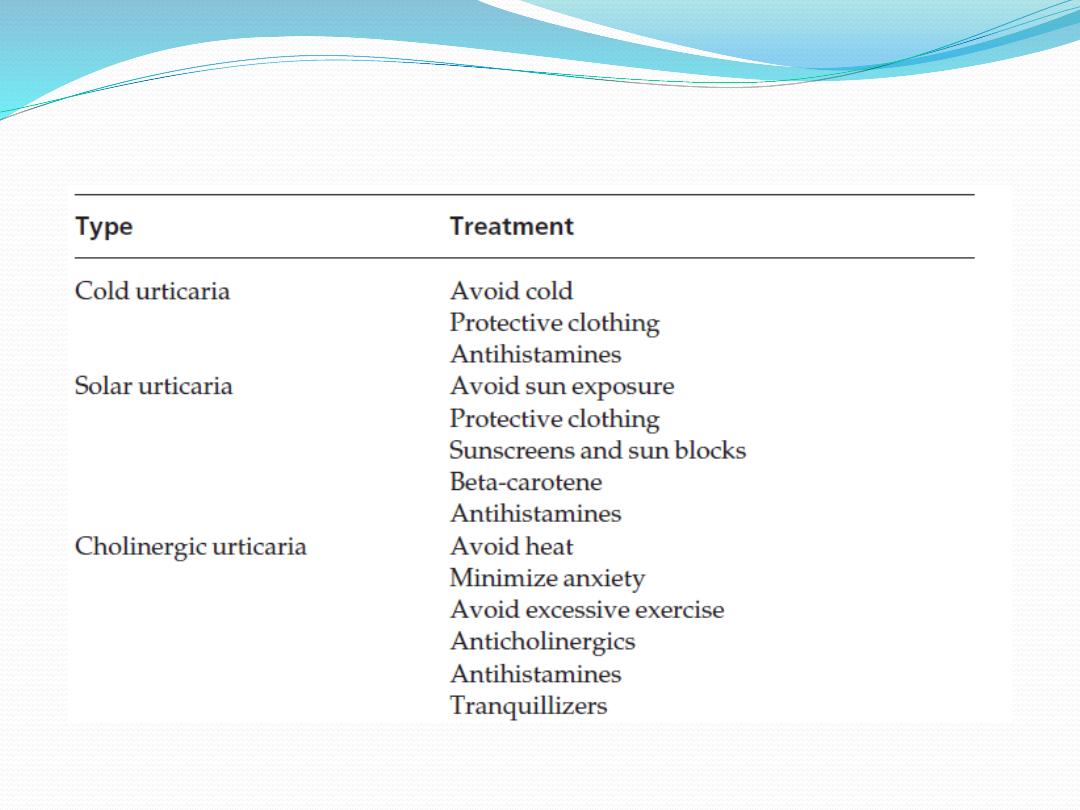
Types of urticaria and their
management
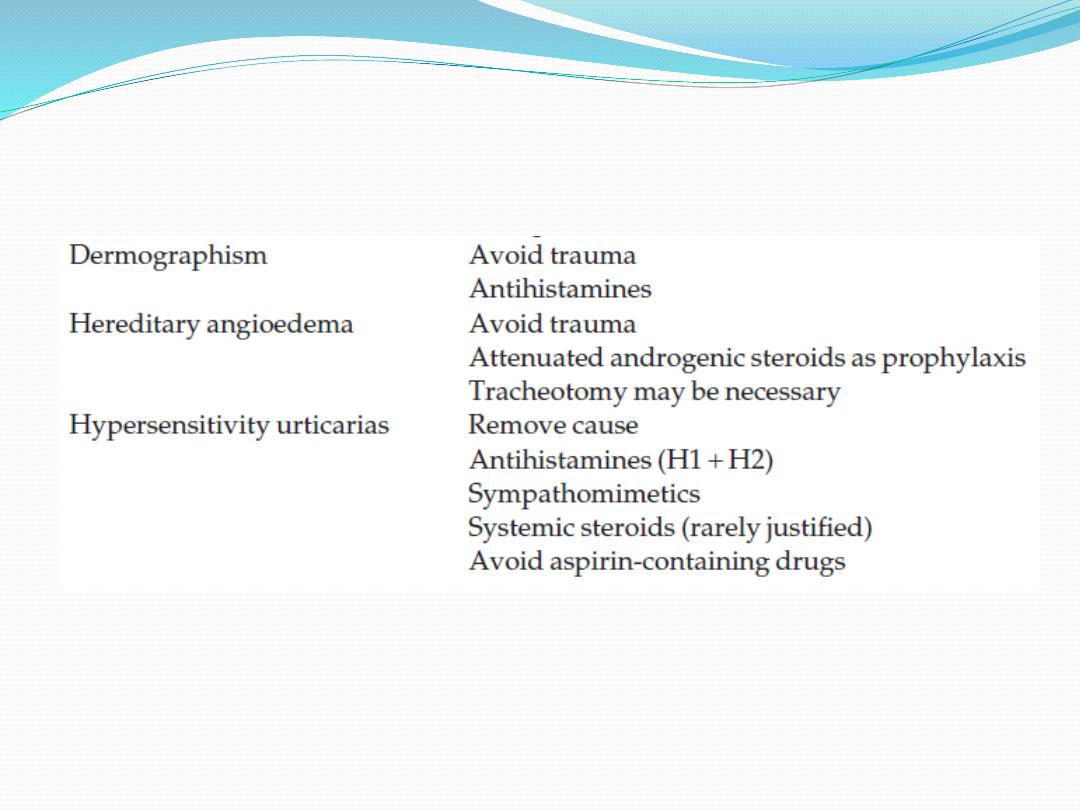
Types of urticaria and their management