Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Graves’ disease
Graves’ disease can occur at any age but is unusual before puberty and most
commonly affects women aged 30–50 years .The most common
manifestation is thyrotoxicosis with or without a diffuse goitre. Graves’
disease also causes ophthalmopathy and, rarely, pretibial myxoedema .
These extrathyroidal features usually occur in thyrotoxic patients but can
arise in the absence of thyroid dysfunction.
Graves’ thyrotoxicosis
Pathophysiology
The thyrotoxicosis results from the production of immunoglobulin G (IgG)
antibodies directed against the TSH receptor on the thyroid follicular cell,
which stimulate thyroid hormone production and proliferation of follicular
cells, leading to goitre in the majority of patients. These antibodies are
termed thyroid-stimulating immunoglobulins or TSH receptor antibodies
(TRAb) and can be detected in the serum of 80–95% of patients with
Graves’ disease.
The concentration of TRAb in the serum is presumed to fluctuate to account
for the natural history of Graves’ thyrotoxicosis . Thyroid failure seen in
some patients may result from the presence of blocking antibodies against
the TSH receptor, and from tissue destruction by cytotoxic antibodies and
cell-mediated immunity Graves’ disease has a strong genetic component.
A suggested trigger for the development of thyrotoxicosis in genetically
susceptible individuals may be infection with viruses or bacteria. Certain
strains of the gut organisms Escherichia coli and Yersinia enterocolitica
possess cell membrane TSH receptors and it has been suggested that
antibodies to these microbial antigens may cross-react with the TSH
receptors on the host thyroid follicular cell. Smoking is weakly associated
with Graves’ thyrotoxicosis but strongly linked with the development of
ophthalmopathy.
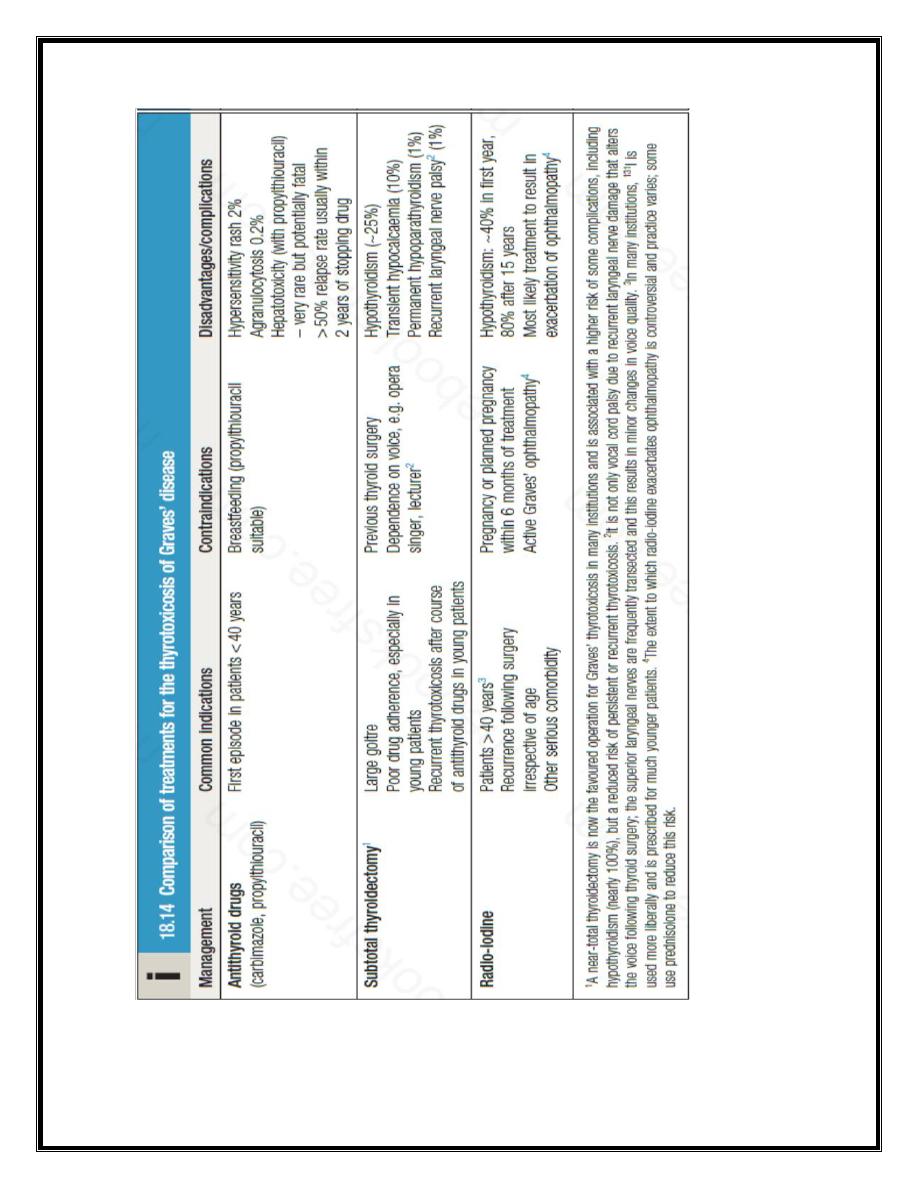
Management
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Symptoms of thyrotoxicosis respond to β-blockade but definitive treatment
requires control of thyroid hormone secretion.
Some clinicians adopt an empirical approach of prescribing a course of
antithyroid drug therapy and then recommending 131I or surgery if relapse
occurs.
Antithyroid drugs
:The most commonly used are
carbimazole
and its
active metabolite,
methimazole
,the
Propylthiouracil
is equally effective.
These drugs reduce the synthesis of new thyroid hormones by inhibiting the
iodination of tyrosine . Carbimazole also has an immunosuppressive action,
leading to a reduction in serum TRAb concentrations.
Antithyroid drugs should be introduced at high doses (carbimazole 40–60
mg daily or propylthiouracil 400–600 mg daily). Usually, this results in
subjective improvement within 10–14 days and renders the patient clinically
and biochemically euthyroid at 6–8 weeks. At this point, the dose can be
reduced and titrated to maintain T4 and TSH within their reference range.
In most patients, carbimazole is continued at 5–20 mg per day for 12–18
months in the hope that remission will occur.
Antithyroid drugs can have adverse effects. The most common is a rash.
Agranulocytosis is a rare but potentially serious complication that cannot be
predicted by routine measurement of white blood cell count but which is
reversible on stopping treatment. Patients should be warned to stop the drug
and seek medical advice immediately, should a severe sore throat or fever
develop while on treatment. Propylthiouracil is associated with a small but
definite risk of hepatotoxicity, which, in some instances, has resulted in liver
failure requiring liver transplantation, and even in death. It should therefore
be considered second-line therapy to carbimazole and be used only during
pregnancy or breastfeeding , or if an adverse reaction to carbimazole has
occurred.
Thyroid surgery: Patients should be rendered euthyroid with antithyroid
drugs before operation. Traditionally, a ‘subtotal’ thyroidectomy is
performed, in which a portion of one lobe of the thyroid is left in situ, with
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
the aim of rendering the patient euthyroid. While complications of surgery
are rare and 80% of patients are euthyroid, 15% are permanently
hypothyroid and 5% remain thyrotoxic. As a consequence, many endocrine
surgeons now opt to perform a ‘near-total’ thyroidectomy, leaving behind
only a small portion of gland adjacent to the recurrent laryngeal nerves. This
strategy invariably results in permanent hypothyroidism and is probably
associated with a higher risk of hypoparathyroidism, but maximises the
potential for cure of thyrotoxicosis.
Radioactive iodine 131I is administered orally as a single dose and is
trapped and organified in the thyroid . 131I emits both β and γ radiation and,
although it decays within a few weeks, it has long-lasting inhibitory effects
on survival and replication of follicular cells. The variable radio-iodine
uptake and radiosensitivity of the gland means that the choice of dose is
empirical.
The disadvantage of 131I treatment is that the majority of patients eventually
develop hypothyroidism.
131I is usually avoided in patients with Graves’ ophthalmopathy and
evidence of significant active orbital inflammation. In women of
reproductive age, pregnancy must be excluded before administration of 131I
and avoided for 6 months thereafter; men are also advised against fathering
children for 6 months after receiving 131I.
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
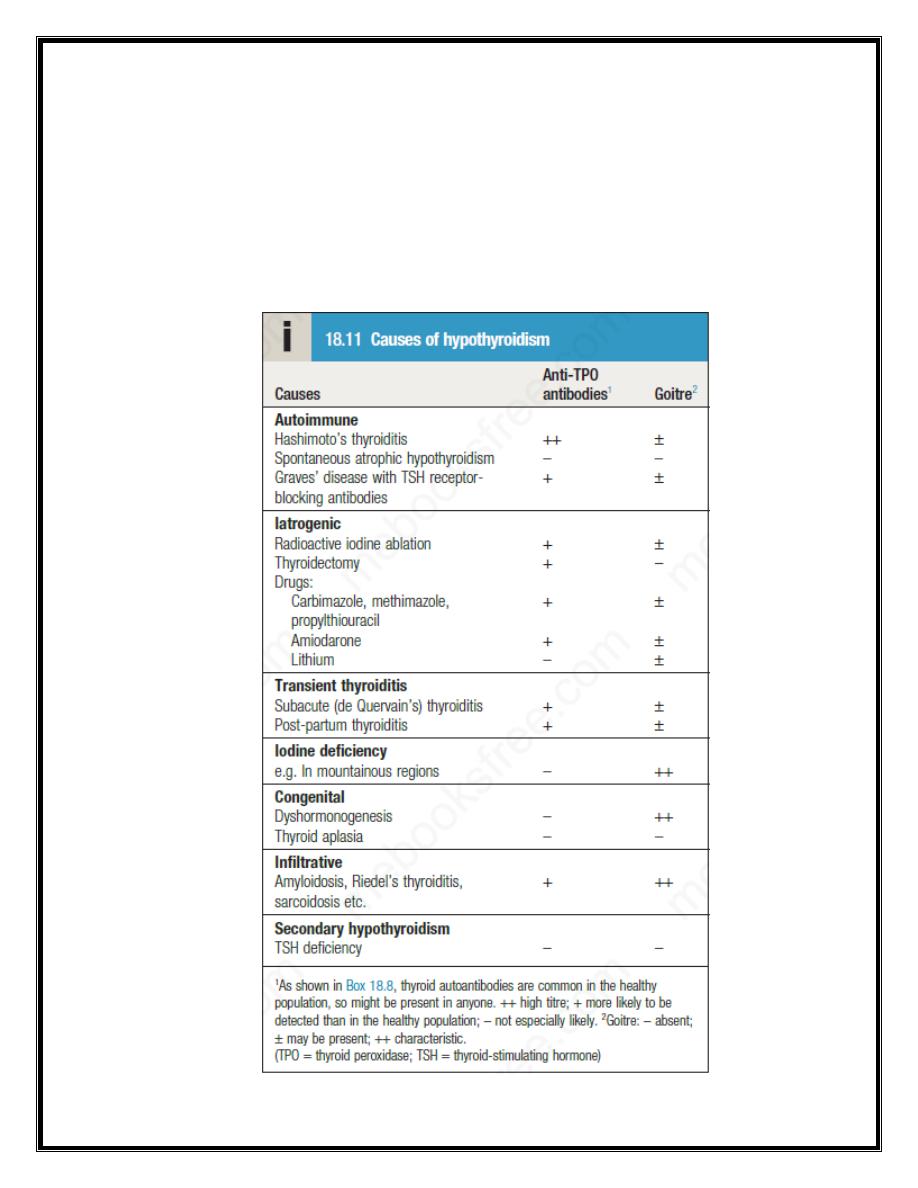
Hypothyroidism
Hypothyroidism is a common condition with various causes , but
autoimmune disease (Hashimoto’s thyroiditis) and thyroid failure following
131I or surgical treatment of thyrotoxicosis account for over 90% of cases,
except in areas where iodine deficiency is endemic. Women are affected
approximately six times more frequently than men.
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
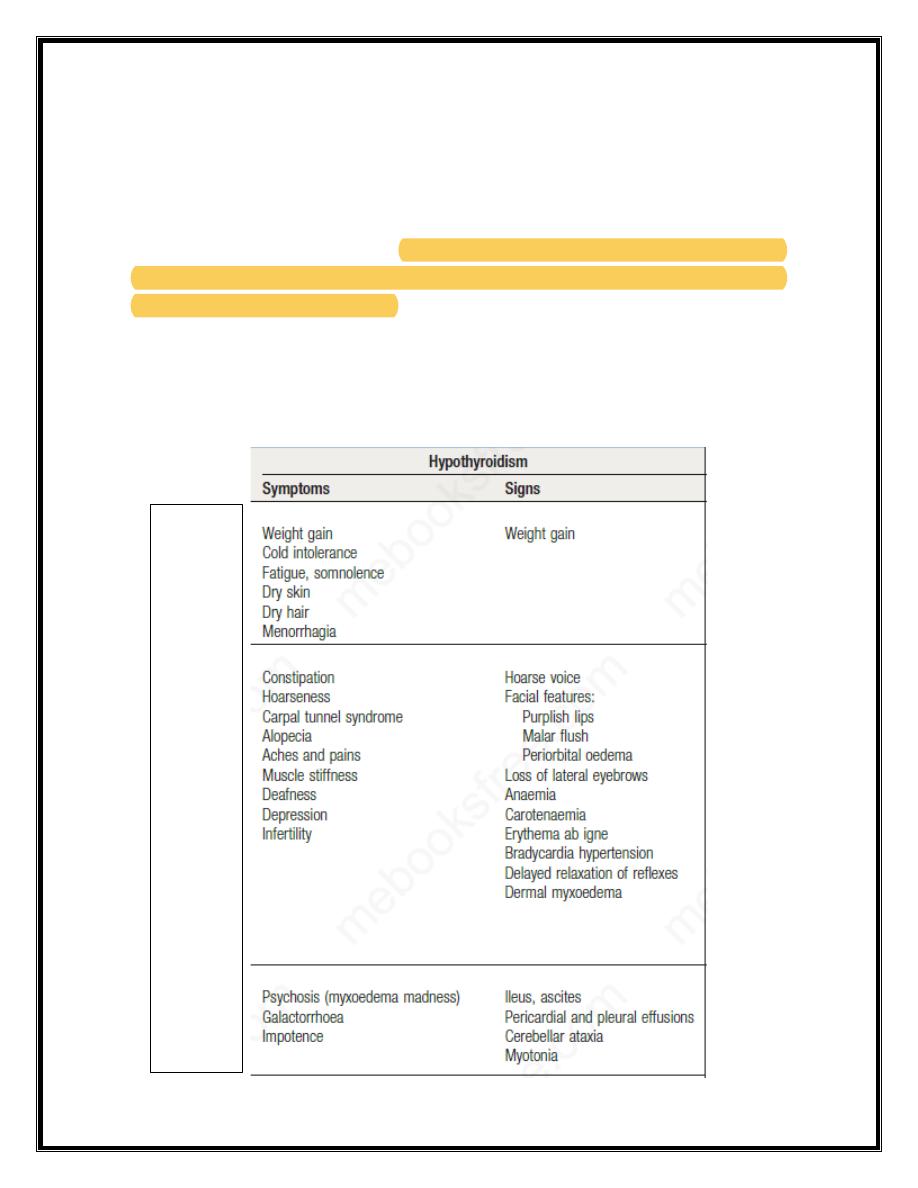
Clinical assessment
The clinical presentation depends on the duration and severity of the
hypothyroidism. Those in whom complete thyroid failure has developed
insidiously over months or years may present with many of the clinical
features listed below. A consequence of prolonged hypothyroidism is the
infiltration of many body tissues by the mucopolysaccharides hyaluronic
acid and chondroitin sulphate, resulting in a low-pitched voice, poor hearing,
slurred speech due to a large tongue, and compression of the median nerve at
the wrist (carpal tunnel syndrome). Infiltration of the dermis gives rise to
non-pitting oedema (myxoedema), which is most marked in the skin of the
hands, feet and eyelids.
Common
Less
common
Rare
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
The resultant periorbital puffiness is often striking and may be combined
with facial pallor due to vasoconstriction and anaemia, or a lemon-yellow
tint to the skin caused by carotenaemia, along with purplish lips and malar
flush. Most cases of hypothyroidism are not clinically obvious, however, and
a high index of suspicion needs to be maintained so that the diagnosis is not
overlooked in individuals complaining of non-specific symptoms such as
tiredness, weight gain, depression or carpal tunnel syndrome.
Investigations
In the vast majority of cases, hypothyroidism results from an intrinsic
disorder of the thyroid gland (primary hypothyroidism).
In this situation, serum T4 is low and TSH is elevated, usually in excess of
20 mIU/L. Measurements of serum T3 are unhelpful since they do not
discriminate reliably between euthyroidism and hypothyroidism. Secondary
hypothyroidism is rare and is caused by failure of TSH secretion in an
individual with hypothalamic or anterior pituitary disease. In severe,
prolonged hypothyroidism, the ECG classically demonstrates sinus
bradycardia with low voltage complexes and ST-segment and T-wave
abnormalities.
Measurement of thyroid peroxidase antibodies is helpful but further
investigations are rarely required.
Management
Treatment is with
levothyroxine
replacement. It is customary to start with a
low dose of 50 μg per day for 3 weeks, increasing thereafter to 100 μg per
day for a further 3 weeks and finally to a maintenance dose of 100–150 μg
per day. Patients feel better within 2–3 weeks. Reduction in weight and
periorbital puffiness occurs quickly but the restoration of skin and hair
texture and resolution of any effusions may take 3–6 months.
The dose of levothyroxine should be adjusted to maintain serum TSH within
the reference range. Some patients remain symptomatic despite
normalisation of TSH and may wish to take extra levothyroxine, which
Lec .2 Dr. Nihad Abdallah Al-jeboori /Subspeciality Endocrnology &Diabetes
suppresses TSH. However, suppressed TSH is a risk factor for osteoporosis
and atrial fibrillation , so this approach cannot be recommended.
Levothyroxine replacement in ischaemic heart disease:
Hypothyroidism and ischaemic heart disease are common conditions that
often occur together. Although angina may remain unchanged in severity or
paradoxically disappear with restoration of metabolic rate, exacerbation of
myocardial ischaemia, infarction and sudden death are recognised
complications of levothyroxine replacement, even using doses as low as 25
μg per day. In patients with known ischaemic heart disease, thyroid hormone
replacement should be introduced at low dose and increased very slowly
under specialist supervision.
Coronary intervention may be required if angina is exacerbated by
levothyroxine replacement therapy .