Diagnosis of skin diseases
By end of this lecture the student should be able to:• Identify the most common morphological presentations of skin lesions (primary & secondary lesions).
• Be able to fully describe any skin lesion based on:
Shape
Arrangement
Color
Distribution
Morphology
Be familiar with the most important tools for investigations in dermatology
The key to a successful Rx is a correct Dx
Dermatological diseases are usually visible, so inspection is all that is needed for DxKeen eyes
Magnifying lens
Correct diagnosis
How to bring order to confusion:
What component is mainly affected? (dermis, epidermis, subcutaneous fat, blood vessels)What is the primary change and what is secondary?
Next assess the lesions by type, shape, arrangement, and distribution.
Finally, how did the changes evolve over time?
Types of lesions
Primary lesionsSecondary lesions
Special phenomena
Primary skin lesions
They are the basic lesions with which the skin disease starts1-Macule: flat circumscribed skin discoloration less than 1 cm in diameter
A larger MACULE more than 1 cm in diameter is called A PATCHThey can be red, blue, white, brown


2---




3-



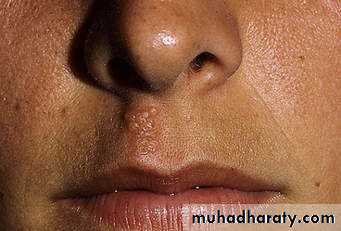
4- Nodule : A larger & deeper lesion than a papule, e.g., erythema nodosum, neurofibromatosis.



5- Blisters
A circumscribed elevation of the skin containing fluid, of 2 types:A) vesicle: less than 0.5 cm. in diameter e.g. acute dermatitis.
B) Bulla: larger than 0.5 cm, e.g. pemphigoid .
Eg of vesicles





6- pustule: A visible accumulation of pus, as in folliculitis.
7-8- Purpura
Visible, blood filled lesions in the skin, they are either:a) petechiae: pinhead sized macules of blood in the skin.
b) ecchymosis : larger extravasations of blood into the skin, as in many bleeding disorders.
E.g. of petechiae & ecchymosis



9-
10-
11- Telangectasia : Permanent visible dilation of superficial blood vessels in the skin as in rosacea


12- Comedo: A plug of keratin & sebum wedged in a dilated pilo-sebaceous follicle, there are 2 types; open (black heads) & closed (white heads), as in acne vulgaris.


Secondary skin lesions
These evolve from primary lesions during the natural progress of the disease, or may be created by events such as scratching or infection.They include:
1-Scale: Excess flakes of dead epidermal cells from the horny layer, could be mild as in chapping or severe as in psoriasis.


2) Crust: A collection of dried serum & cellular debris as in impetigo.


3-Erosion:
A focal loss of the epidermis, which does
not penetrate deeper than the
dermo-epidermal junction, & so heals
Without scarring as in impetigo,
& pemphigus.
4-Ulcer
A focal loss of epidermis &dermis & so heals with
scarring as in primary
syphilis.

5-fissure:
.A linear slit in the skin
with nearly vertical wallsas in finger tip eczema
6-Sinus :

A cavity or channel that
permits the escapeof pus or fluid
as in pilo-nidal sinus.
7-Excoriation

An ulcer or erosion, often
linear caused by scratching,
as in neurotic excoriations
8-Atrophy:

A depression in the skin
resulting from thinningof the epidermis or dermis
e.g. as a side effect of
topical or intra-lesional
steroids.
9-Scar:

A result of healing
where normal structuresare permanently replaced
by fibrous tissue, e.g. burn.
10-Lichenification
An area of thickened epidermis induced by scratching, the skin looks hyper pigmented ,thickened, with accentuation of skin markings, e.g. lichen simplex chronicus.
lichenified palques
Old trees

SPECIAL PHENOMENA
IN DERMATOLOGYKoebner’s phenomenon
The tendency of the rash to appear at sites of trauma, as in:Psoriasis
lichen planus
plane warts
acute eczema
vitiligo

Nikolsky's sign
Sheet-like separation of the epidermis by gentle tractionas in pemphigus

Auspitz's sign:
Appearance of
pin-point
dots of blood when
scales are forcibly removed in a psoriatic plaque


Configuration of lesions
Annular: T. corporis, granuloma annulareRound/ Discoid: nummular eczema, discoid lupus
Polycyclic: urticaria, SCLE
Arcuate: urticaria
Linear: scabies burrow, Koebner’s phenomenon
Reticular: livedo reticularis
Serpiginous: cutaneous larva migrans
Targetoid lesions: erythema multiformiGrouped/herpitiform: HSV
Zosteriform: herpes zoster
Scattered: chicken pox
OTHER AIDS TO DIAGNOSIS
1- DIASCOPY:
To differentiate erythema from telangectasia;press a slide firmly on the skin lesion,
if a red lesion blanches then it is
due to vasodilation(blood inside the
blood vessels), if not; it is purpura
(blood outside the vessels).
In TB of the skin diascopy reveals an appearance called apple- jelly nodules.
2- DermoscopyThe lesion is covered by mineral oil or water,
& observed by a hand held dermoscope, the fluid
eliminates surface reflection & make the
epidermis translucent , used especially for
pigmented lesions as malignant melanoma,
also to identify scabies mites in their burrows.

Wood's lamp

A long-wave ultra violet light (360nm),
obtained by a high pressure mercury lamp with a nickel-oxide & silica filter,the patient should be put in a darkened room, & a special fluorescence occurs in certain conditions which aids in their diagnosis:
Uses of WOOD’S lamp
A) Ring worm of scalp : greenish fluorescence.B) Erythrasma: coral red fluorescence in the flexures.
C) Porphyria : pinkish fluorescence of the teeth & urine of patients with porphyria cutanea tarda
D) Pityriasis versicolor: Yellowish fluorescence.
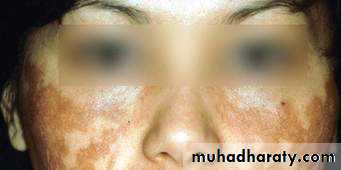
E) Pigmentary disorders: Both in hypo & hyperpigmentation there is increased contrast, as in vitiligo where areas of subtle depigmentation are more easily seen.
4)MYCOLOGY SAMPLES


For fungal infection of skin, hair & nail
5)LAB. INVESTIGATIONS :
As hematological,
biochemical, & serologicalTests, together with Gram’s stain
& culture for bacteria
6) CYTOLOGY (Tzanck's smear):


Useful in blistering diseases, viral infections as
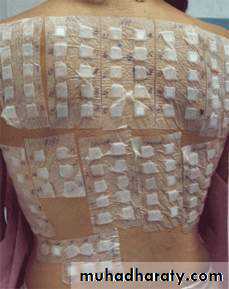
herpes simplex & zoster, & in pemphigus vulgaris7) PATCH TESTS:
To document the presence of allergic contact sensitization& to identify the causative agents. A battery of 20 antigens are
Applied to the back of patients
& examined in 24-48 hours,
any eczematous reaction
would suggest a delayed
hypersensitivity reaction
to this substance

8) PRICK TESTS:
Used to detect type I (immediate) hypersensitivityReaction to various antigens as pollen,
house dust mite, or dander, the
Skin is pricked with the antigen
& examined in 10 minutes
a wheal & flare would suggest
a positive reaction

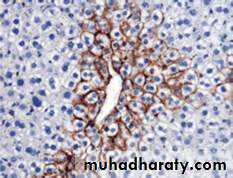
9) HISTOLOGY & IMMUNOFLUORESCNCE:
Ordinary H & E stainingIn tumor cases, immunohistochemistry
Direct & indirect immunofluorescence in auto immune diseases