
Infectious oesophagitis
Objectives
1. What are the common causes of infective esophagitis?
2. Where does it occurs ?
Most commonly occur in immune compromised pt as AIDS, solid organ
transplant, leukemia, lymphoma, and pt on chemotherapy, all are susceptible
to opportunistic infections.
Pathogens/;-
1. Candida albicans----may be in DM, steroid, pt on antibiotic therapy.
2. herpes simplex -----may be present in normal pts
3. Cytomegalovirus.
Clinical picture:
Odynophagia
Dysphagia.
Candida infection:-
Some times asymptomatic.
75% accompanied by oral thrush.
May be associated with other viruses in 25- 50 %, so it is unreliable indicator
for the causes of oesophagitis.
Cytomegalovirus
May occur in colon and retina.
Investigations:-
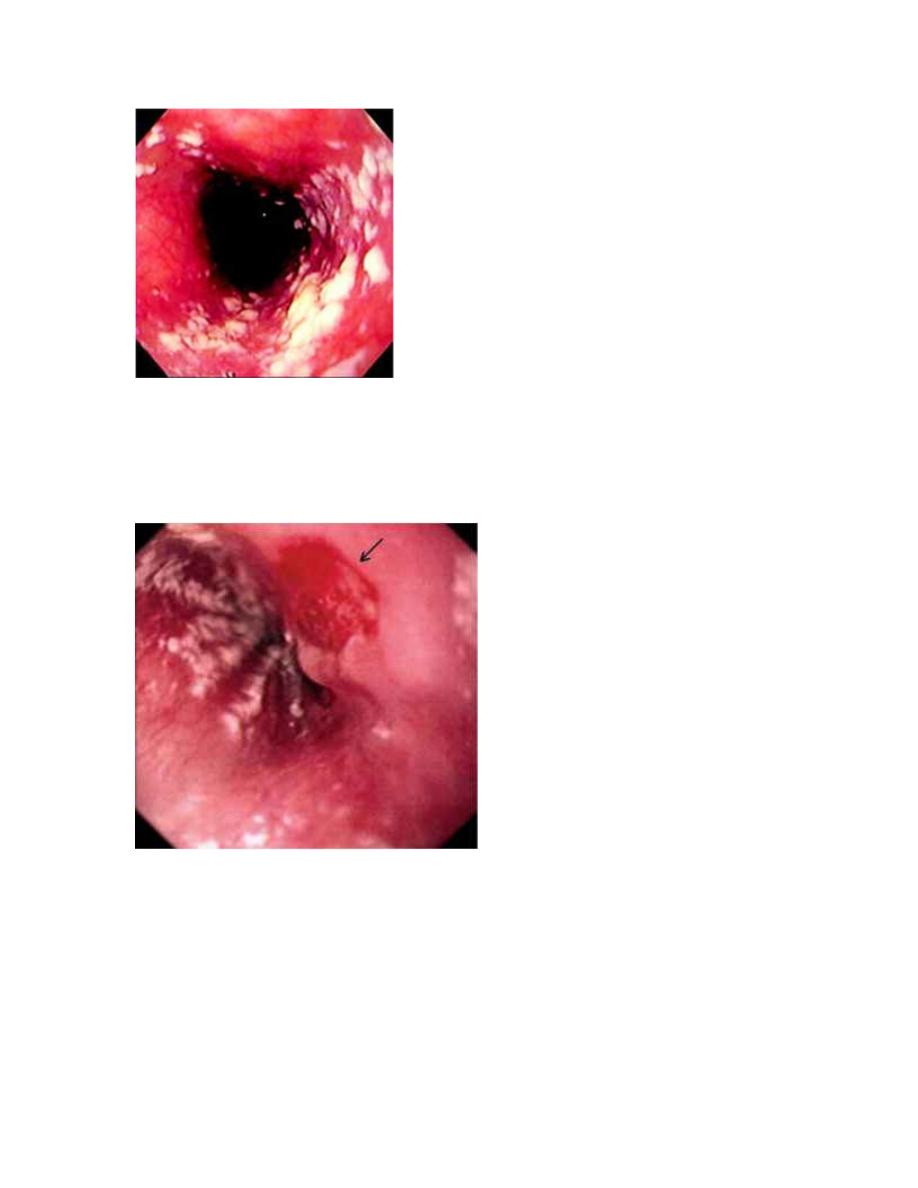
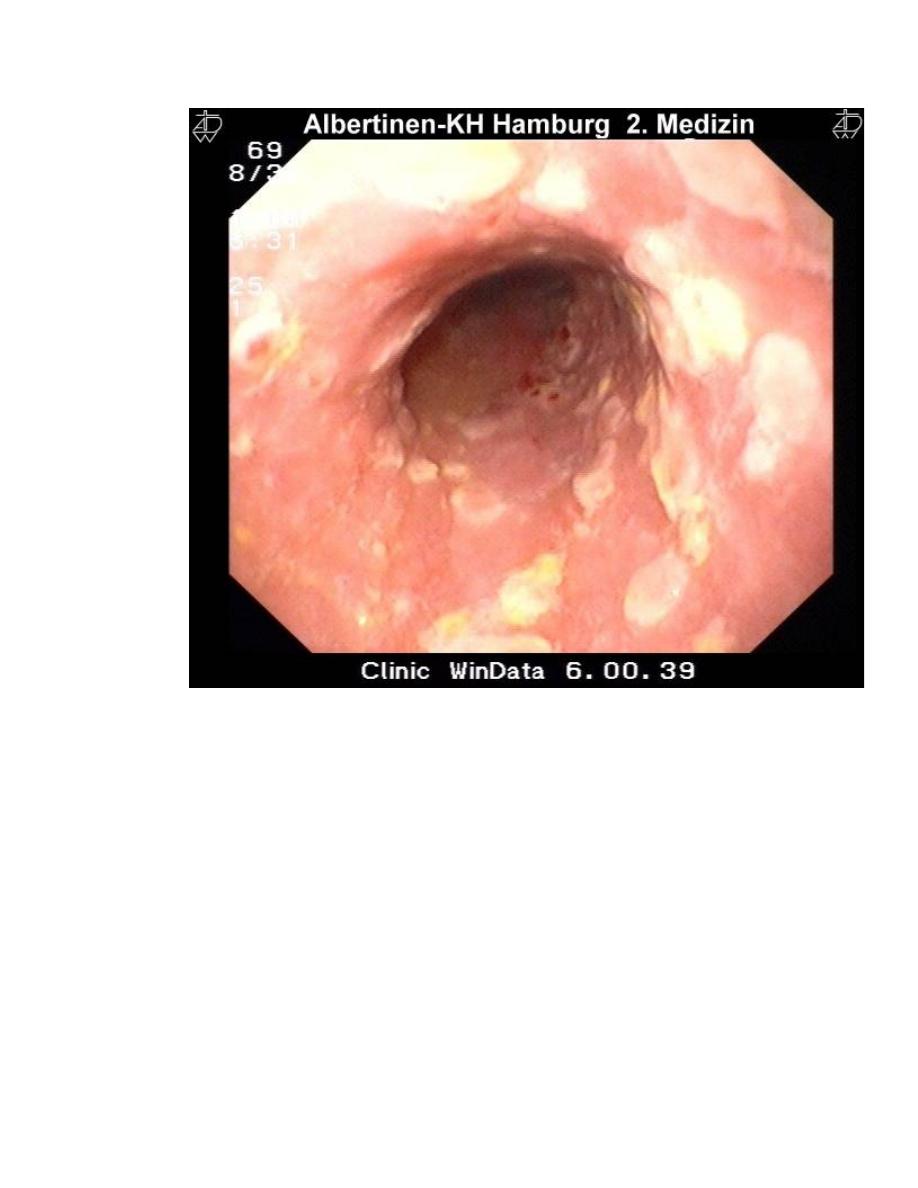
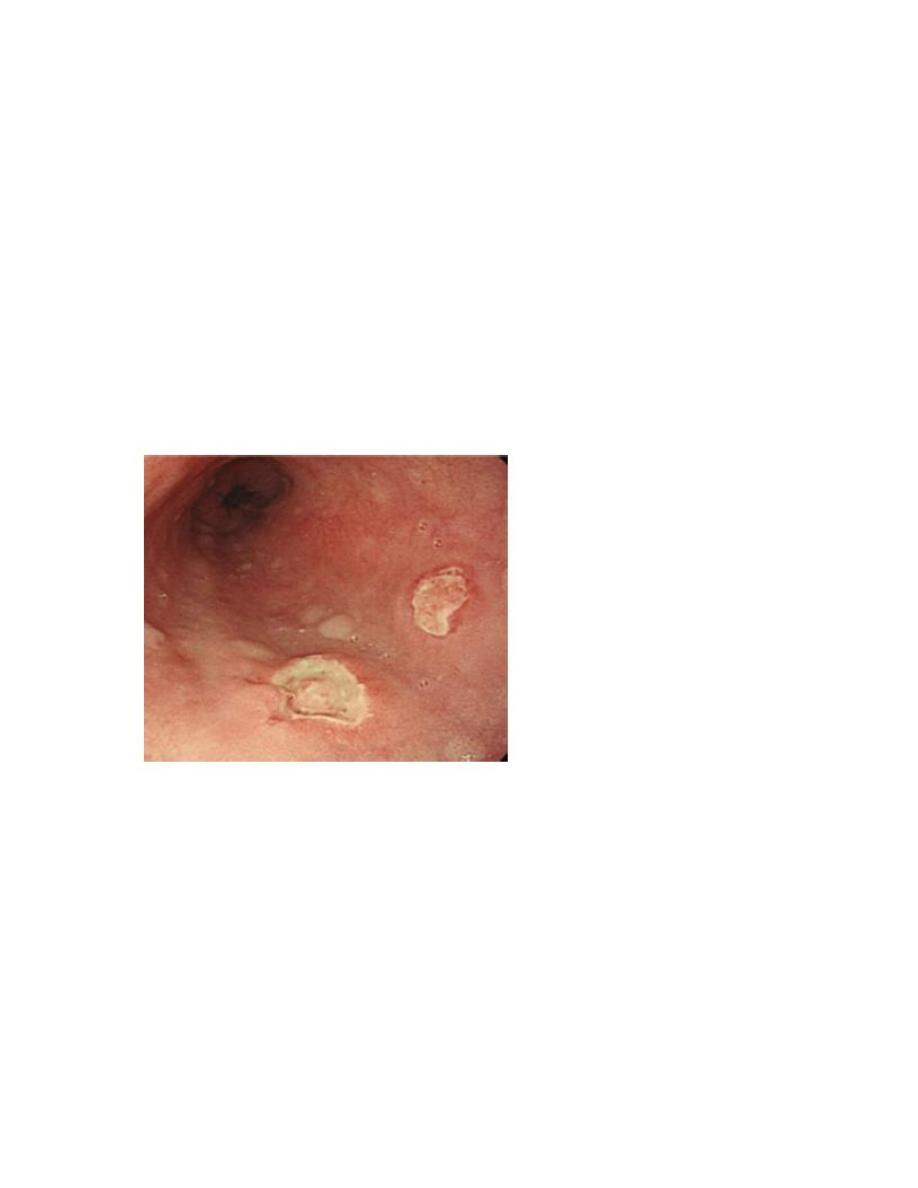
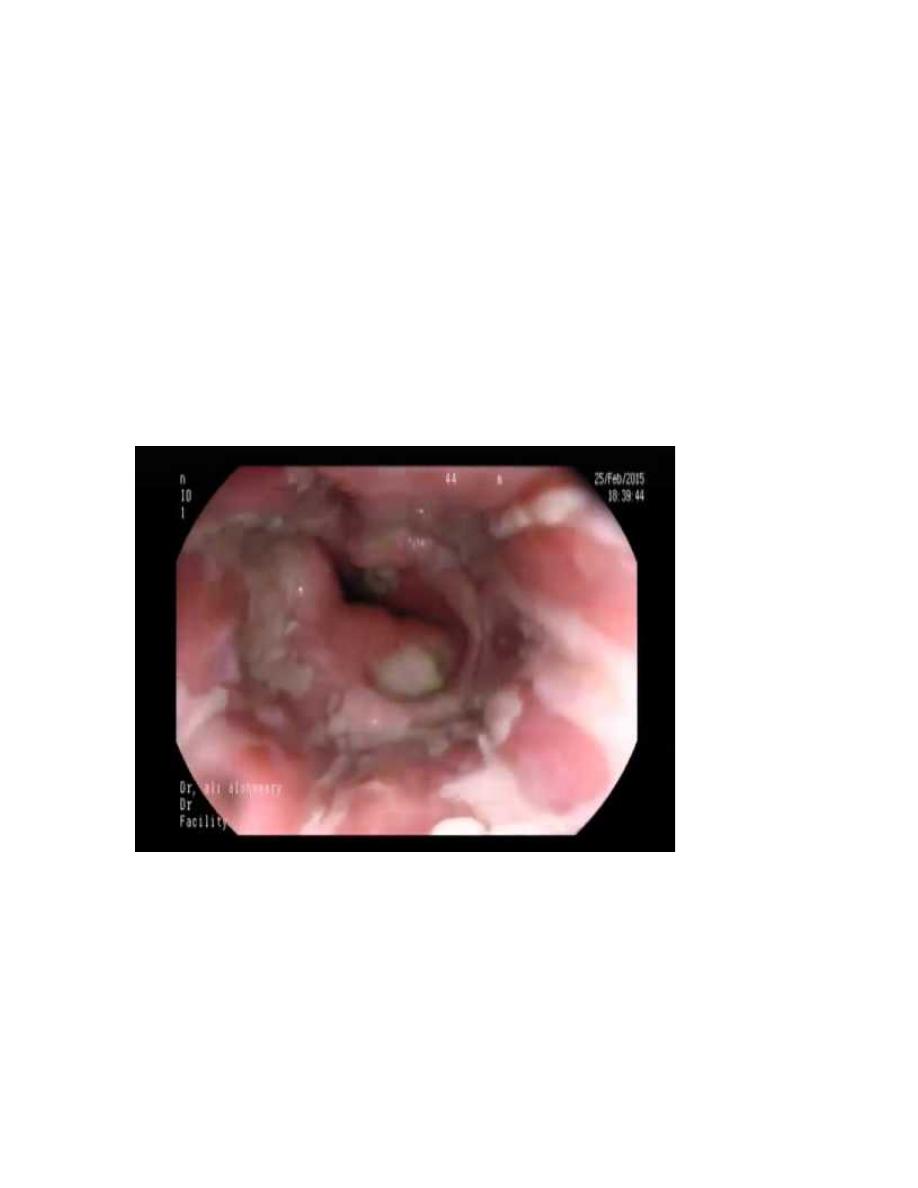
1. endoscope:-
a. Candida infection: - linear, white plaque, adherent to the mucosa.
b. CMV infection:-one or several large shallow, superficial ulceration.
c. Herpetic infection: - multiple small deep ulceration.
Treatment:-
Candida infection
1. normal immune system Candida infection ----
--topical agents:- nystatin 500000 units swish and swallow five times
daily
--Clotrimazole troches 10 mg dissolved in mouth five
times per day for 7- 14 days.
2. immune compromised
--oral :- fluconazole 100-200 mg \day
--systemic:- amphotericin B 0.5 mg \kg\d
Cytomegalovirus:-
Initial therapy:- gancyclovir 5 mg\kg iv 12 hourly for 3-4 weeks
Or discontinue the drugs in resolution.
In suppressive therapy:- gancyclovir continuous infusion 5 mg\kg iv.
Resistant cases: - foscarnet 90 mg \kg iv \12 hourly for 3-4 weeks, side
effects: renal failure
- may be symptomatic therapy only .
- oral acyclovir 200 mg five times daily.
- Famciclovir or valacyclovir may be used.
Pill induced oesophagitis:-
Caustic agents:-
NSAID, KCl, quinidine, ziduvudine, alendronate, iron, vit c, tetracycline,
doxycycline, clindomycin, methoprim.
Complications:-
- Acutely: - dysphagia odynophagia.
- Chronically – stricture ,hemorrhage, perforation
Prevention:-
- Drink pills with 4 oz water.
- Drink in supine position and prevent sleep till half an hour.
Corrosive oesophagitis:-
It is usually suicidal attempts, but it may be accidental, it can be caused
either
1. Alkaline substances like house hold bleaching agents, it is usually
severe, along extensive, it penetrate deeply to the tissue.
2. Acidic substances:- battery acids, it is usually severe also but less
penetration than alkaline medium.
Clinically:-
Usually pt has painful burns on the mouth and pharynx and extensive
erosive gastritis.
Dysphagia, drooling, gagging and others.
Extra GIT manifestations that results from aspiration as drooling and
wheezing.
Management and complications:-
It is usually complicated by perforation or strictures, mediastinitis,if the
lesion was severe initial management should be directed to circulatory
status and to attempt air way patency including laryngoscope, chest x- ray
is important to delineate pneumanitis or free perforation.
Endoscope is contraindicated because it may induce perforation. Barium
swallow may be of benefit.

-intravenous fluid and good analgesia.
- Nutritional support.
- no role for corticosteroid or antibiotics in prevention of stricture.
- Admission for 72 hours under observation
- Surgery is indicated for
1. Sepsis.
2. Shock
3. Perforation or strictures
4. Progressive deteriorations
Barrett’s esophagus (columnar lined esophagus)
It is a premalignant glandular metaplasia of lower esophagus which is
normally squamous epith. Replaced by columnar mucosa compose of a
cellular mosaic containing area of intestinal metaplasia.
It is found in 10 %of pt. investigating for GERD, but the true incidence may
be 20 times greater size is often asymptomatic; it is a major risk factor for
adenocarcinoma of lower esophagus.
It is more common in men , often older than 50 years, and in white
pt. ,alcoholic, while smoking is poorly associated with it .it converted to
malignant if it is continued for long time and more severe other factors that
play a role in that conversion.
E- Cadherin polymorphism, P53 mutations, transforming growth factor B
(TGF_B)., epidermal growth factor (EGF) receptors, COX2 and tumor
necrosis factor alpha(TNF).
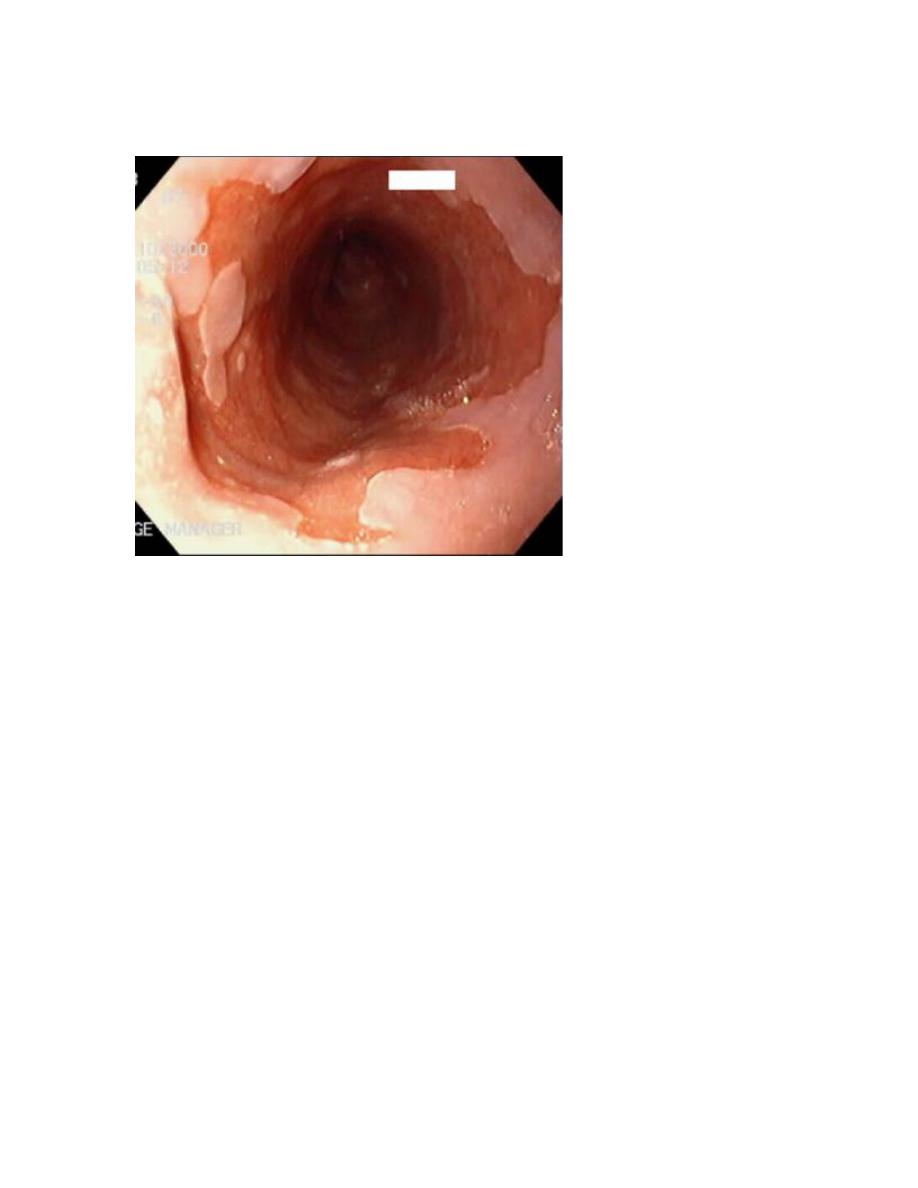
Diagnosis:-
Endoscope and multiple biopsies.
Management:-
Potent acid suppression or antireflux surgery with help for symptomatic
control only but it doesn’t affect the progression of dis. Or metaplasia or
malignant transformation.
Treatment of choice is ablation therapy or photodynamic therapy which
helps for progression of dis. But still many buried islands of glandular tissue
may persist underneath the squamous epithelium and cancer risk is not
eliminated.
Regular endoscope is important to decrease two year survival.
Surveillance is recommended every two years for those with
out metaplasia. And 6-12 months for those with low grade
dysplasia
Pt. with high grade dysplasia (HGD) may be treated with
ablation or photodynamic therapy;
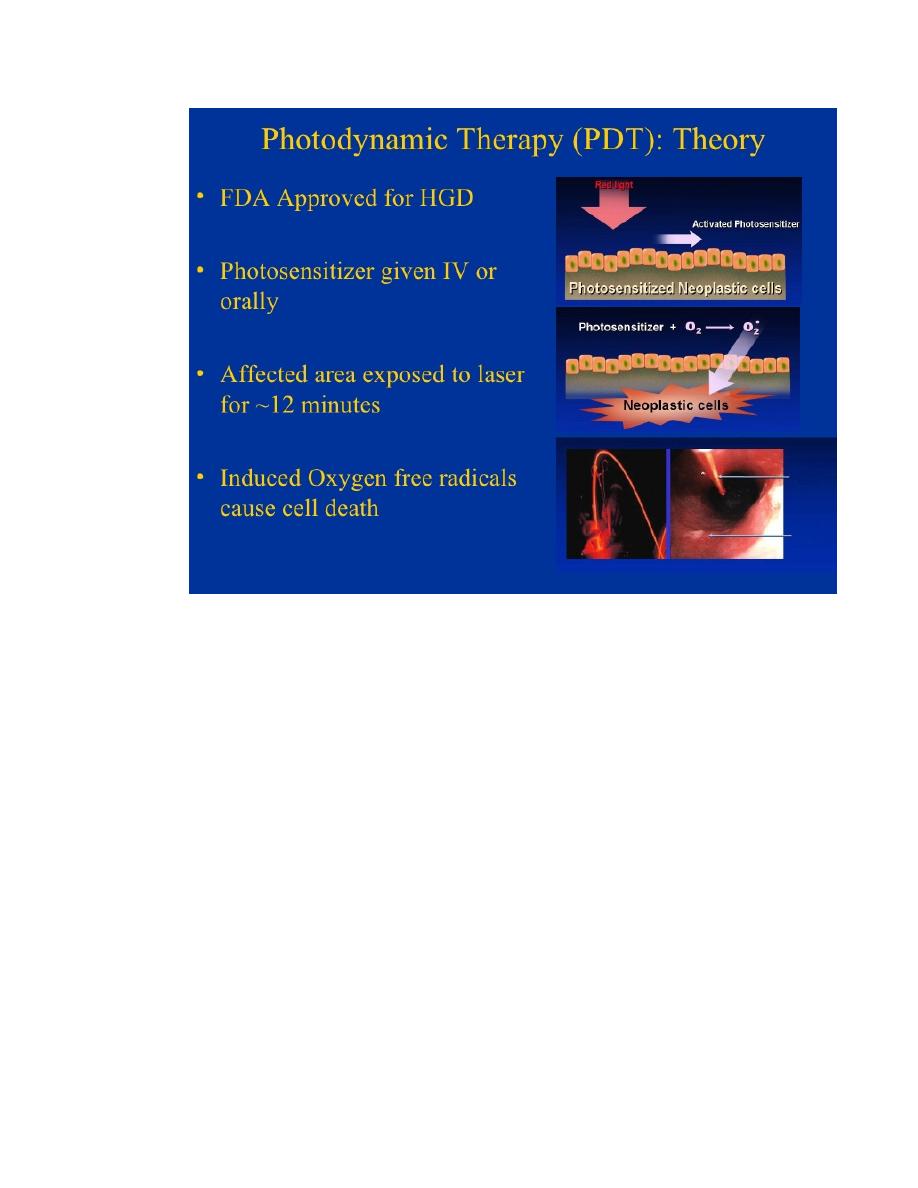
the resected area may contain malignancy up to 40% in high
grade dysplasia. Alternative therapy for (HGD) is close follow
up every 3 months.
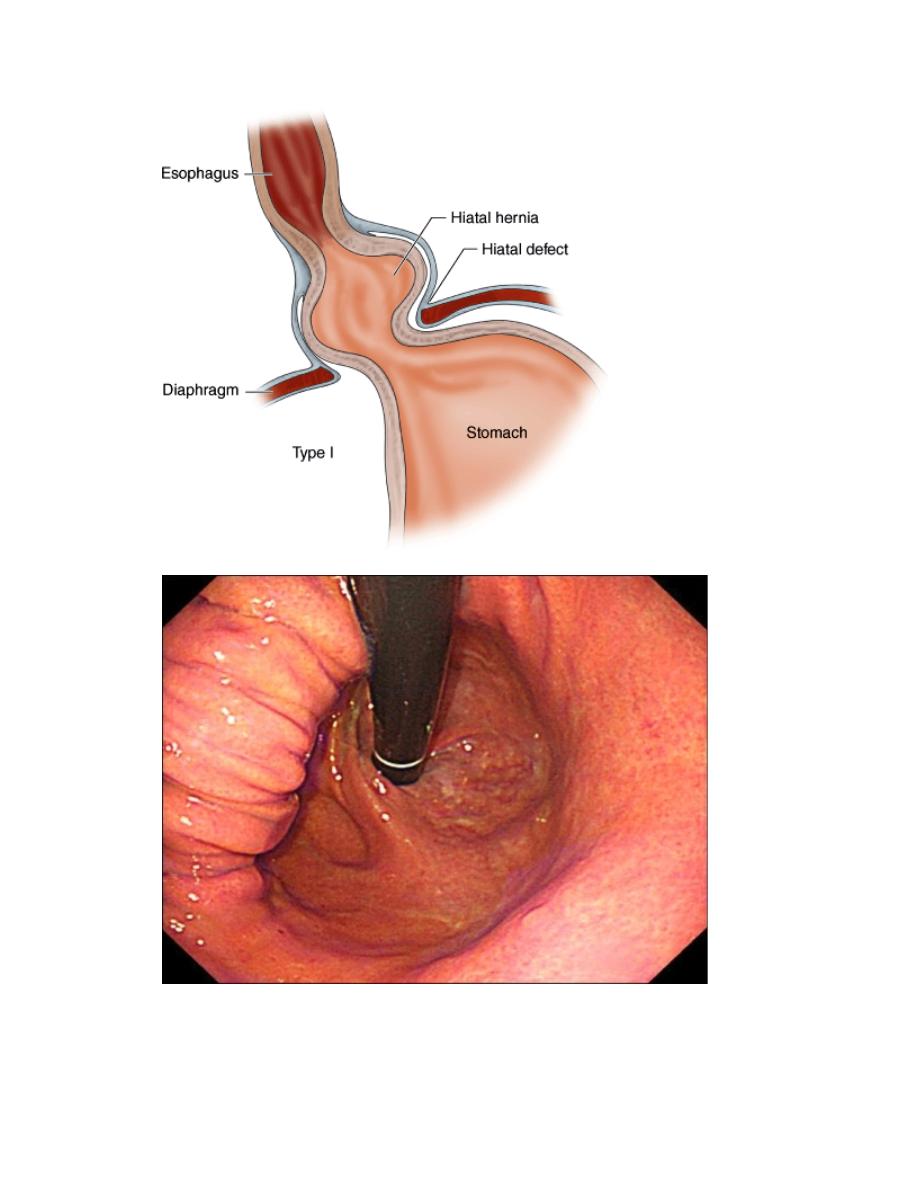
Hiatus hernia
Herniation of the stomach though the diaphragm into the chest, it occurs in
30 % of the general population. Often asymptomatic.
Types:-
Congenital:-treated during childhood,
.
Sliding type:-may be asymptomatic or symptomatic of GERD.
Complications—stricture.
2. Rolling type or Para esophageal:-when portion of the stomach lies
anterior to the esophagus, give vague symptoms of upper abd. Pain
nausea vomiting, fullness after eating.—complications gastritis,

bleeding, from gastric ulcer, iron deficiency anemia, gastric volvulus
and hernias strangulation.
Hiatus hernia is very common in patient with no symptoms and some
symptomatic patients have only a very small or no hernia
Almost all pt. who develop oesophagitis, Barrette’s oesophagitis peptic
stricture have hernia.
Investigations:-
If HH is large, it may be seen on chest x- ray as retro cardiac shadow
with a fluid level.
Endoscope is diagnostic procedure of choice.
Allowing direct assessment of hernia size, oesophagitis and stricture
formation and for biopsy and the passage of dilating boogies to treat a
stricture.
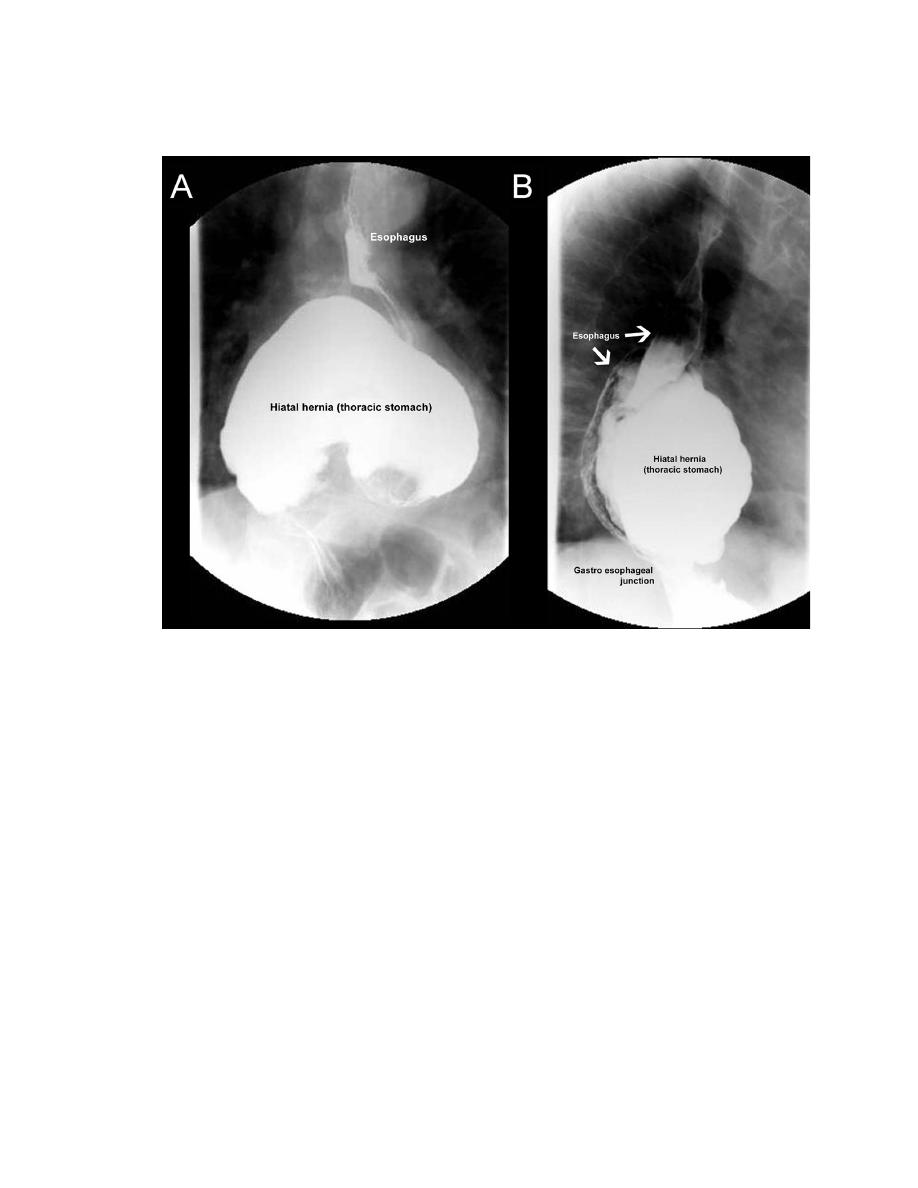
Barium swallow can be used to assess hernia size and the development of
complication.
Management:-
1. Sliding HH need no treatment a part from treatment of complications.
2. Complicated sliding HH and rolling hernia, surgery is indicated.
Peptic esophageal stricture:-
Fibrous stricture which occur at the end of the esophagus as a result of
persistent GERD,most pt are elderly and have poor esophageal peristalsis,
they present with dysphagia for sold first and then for liquid, pt .
Becomes frightened to eat regurgitation meals, develop increase pain and
aspiration then anorexia and weight loss.
Diagnosis:-
Endoscope and dilatation bogging and repeated on need, surgery is
indicated in:-
1. Young.
2. Pt. need frequent dilatation.
3. Severe symptoms.
Motility disorders
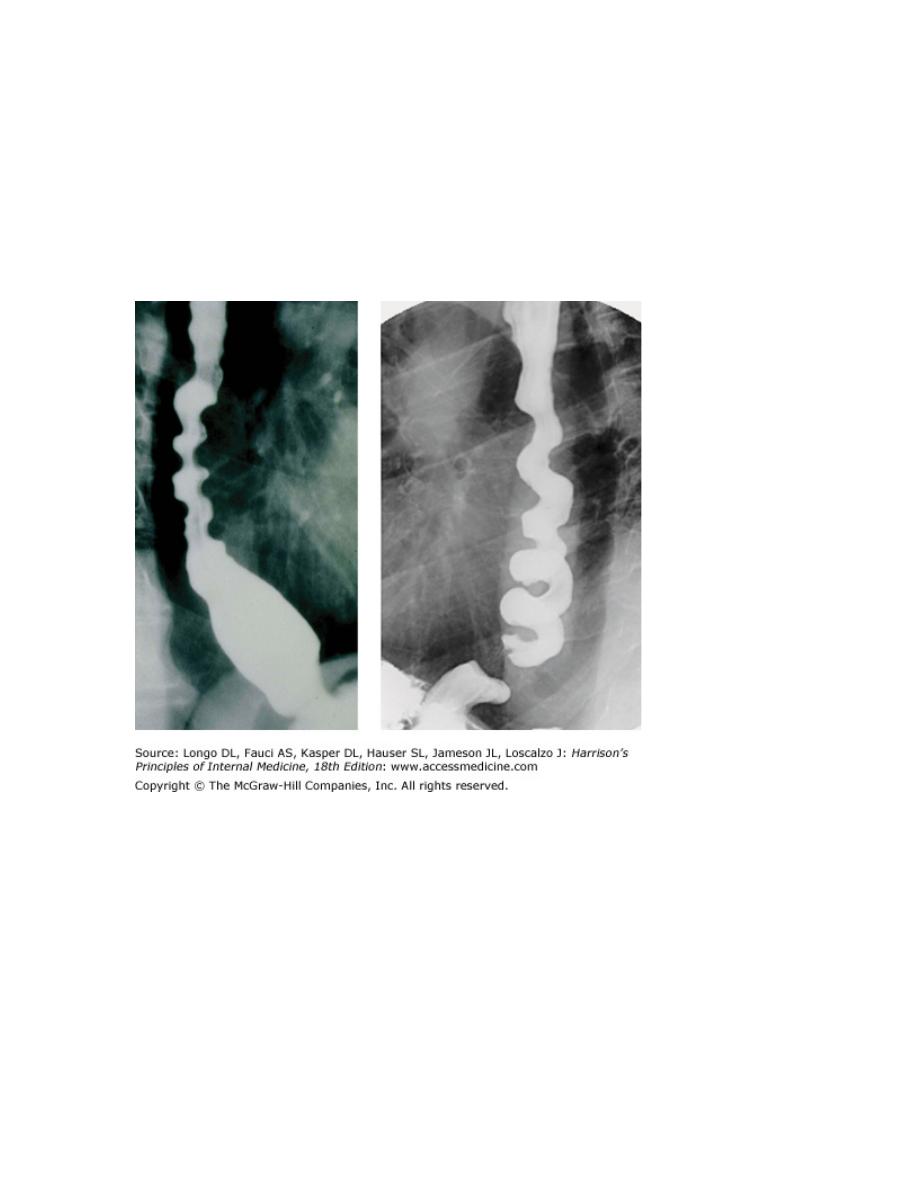
Diffuse Esophageal spasm: - is usually seen in elderly and present with
retrosternal chest pain and \ or dysphagia. Barium swallow shows a normal
esophagus but may undergo diffuse spasm to produce cork screw
configuration
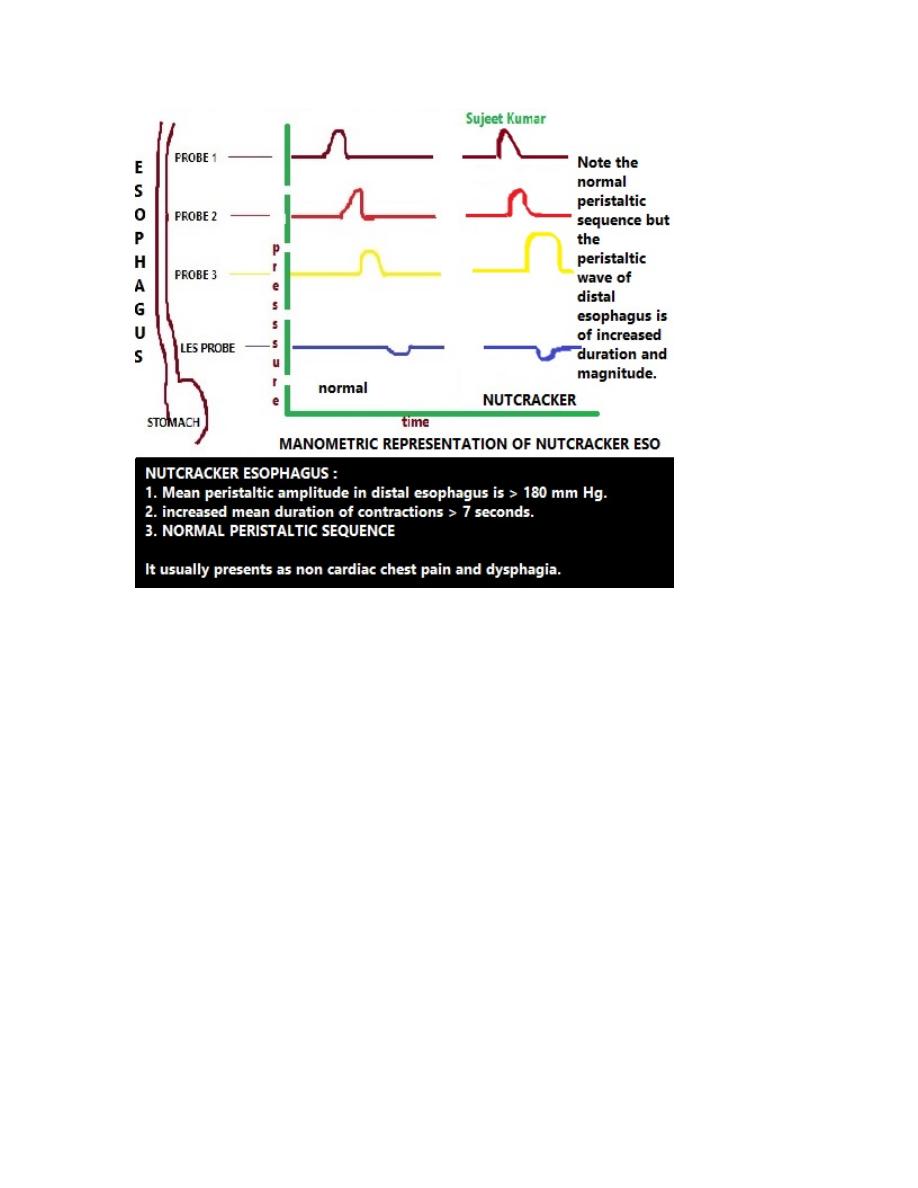
Manomerty shows diffuse burst of increase amplitude unrelated to
swallowing.
Angina is the main differential diagnosis, but esophageal spasm doesn’t
proceeded by exercise.
Treatment:-
Is also similar to angina
- Glycerin dinitrate regularly.
- Nifedipine
- In resistant cases, balloon dilatation or myotomy can be considered
but the result less than that with achalasia.