Cervical cancer
Prof. Dr. Alaa AL.NaserObjectives:
1.revise the anatomy of the cervix, blood supply, lymphatic's.
2. understand epidemiology and pathology of disease.
3. know optimum pre-treatment assessment, how to manage surgically and non-surgically.
4. recognize suspicious cervical lesions, and take appropriate biopsies.
5. Be able to counsel patients with regard to Dx., Mx., Prognosis.
Cervix (2.5 cm long, internal os connects to uterus, external os connect to vagina.
Cervix have 2 parts: supra vaginal part(anteriorly is bladder, post. Is the rectouterine pouch). Other part is vaginal part.
Blood supply(uterine arteries branches of internal iliac arteries, vaginal arteries which is branches of uterine arteries anastomosis with pudendal arteries)
Venous( via uterine venous plexus to internal iliac veins)
Lymphatic's(external iliac node, internal iliac, sacral node &superficial inguinal node)
Epidemiology
cervical cancer is one of the most common cancers in women worldwide. It is the third most common cancer in women, nearly all invasive squamous cell carcinoma are preceded by persistent HPV infection & CIN and vast improvement in screening dramatically lowered the incidence of invasive disease in developed countries, yet in developing countries remain the most lethal malignancy in women.It tends to occur in middle life. Most cases in woman younger than 50. It rarely in women younger than 20. 15% of cases of cervical cancer are fond in women over 65.
Risk
1. Demographic risk, high in Hispanic followed by African-American group, Asians and Pacific Islanders.
2. HPV infection is the primary etiologic infectious agent 99%. High risk type cancer of cervix, vulva, vulva and vagina. 2/3 cause by HPV 16,18.
3. Lower socioeconomic predictor's low education, women do not have easy access to adequate health services including pap smear.
4. Being younger than 17 at first full term pregnancy 2 times more than who wait for 25.
5. Cigarette smoking, chemicals and harmful substance are absorbed through blood stream, smoker twice risk than nonsmoker. Tobacco by-products found in the cervical mucus of women who smoke damage the DNA of cervix cells and also makes the immune system less effective in frightening HPV infections(genotoxicity secondary to the presence of tobacco-derived carcinogen in cervical mucus).
5. Reproductive behavior parity women who had 3 or more full term pregnancies have increased risk = unprotected coitus, low immunity, secondary to trauma.
6. COC long term use of birth control pills increased risk for cervical cancer and risk return back after stopping and to normal risk after 10 year sopping.
7. Being overweight more likely to develop adenocarcinoma.
8. Diet low in fruits and vegetables increased risk.
9. Chlamydial infection increases risk persistent HPV infection& invasive disease.
10. Having a weakened immune system either diseases HIV that weakened the immunity correlate with level of CD4 lymphocyte. And immune suppressive drugs.
11. DES (hormonal medication used in the past to prevent miscarriage, women of the mothers receive DES develop clear cell adenocarcinoma of cervix and vagina. And squamous cell carcinoma of cervix.
12. Having family history of cervical cancer if mother or sister have cervical cancer chance 2-3 times higher than if no one in family, may be familial tendency (but not genetically inheritance)
13. Sexual activity increase no. of sexual partner, early age of sexual intercourse.
Pathophysiology
The malignant transformation of cervical cells is intimately related to HPV infection, which infects basal keratinocytes and replicates during keratinocytes differentiation.(DNA virus), have regulatory early E and late L genomic regions. E protein required for replication and or cellular transformation, these include E6,E7.E6 bind to E6-AP which associate with tumor suppressor protein P53 cause rapid degradation. Loss of P53 result in failure of growth arrest and loss of apoptotic signal in response to cell damage.
E7 interacts with retinoblastoma tumor suppressor gene pRb, E7-pRb initiate cell growth. Both E6, E7 result in aggressive cervical cancer.
Tumor spread
1.The most common method for spread is via direct extension to adjacent tissue include parametria ,vagina ,pelvic side wall and bladder and rectum. Less common metastasize to ovaries.
2. Lymph node spread Para cervical, parametrial, ureteric, obturator, internal, external, common iliac L.N.
2. Lymph vascular space involvement as ca. invade deeper into stromal, it enters blood capillaries and lymphatic channels, so less commonly by hematogenous spread lung, bone, liver, mediastinum, spleen, adrenal and brain.
3. Blood borne spread is unusual.
Histological types
Squamous cell carcinoma: majority of cervical cancer, it develop after an interval of preinvasive disease, it k.k by increased N/C ratio, prominent mitotic figure CIN progress to CIS with subsequent invasive disease after penetration to basement membrane.
Grossly: range from small nodular lesion to large friable easily to bled. It spread by direct extension.
Adenocarcinoma (most other cervical cancer which develop from mucous secreting gland of endocervix)
Grossly the ectocervix appear normal, but cervix expand (barrel-shaped cervix).
Mixed cervical carcinomas (adenosquamous carcinoma
Diagnosis
SymptomsA large portion of women dx. With cervical ca. may be asymptomatic. Diagnosed after evaluation of abnormal pap smear.
For those with symptom early stage ca.create watery vaginal discharge, may contain blood ,between period and after menopause. with tumor growth and necrosis malodorous vaginal discharge.
intermittent vaginal bleeding that follow coitus or douching, as tumor enlarge patient may present with uncontrolled bleeding.
Pain during sex.
Extension to pelvic side wall, compress adjacent organs to produce symptom like lower extremities edema, low backache radiating to posterior leg, often radiating sciatic nerve root, lymphatic's, veins or ureter, ureteral obstruction , hydronephrosis and uremia, occasionally ca. invade bladder and rectum presented with vesico vaginal or rectovaginal fistula. Hematuria , bleeding per rectum.
Physical examination
Most women with cervical cancer finding is cervical lesion which should be biopsied.
Cervical cancer clinically staged and examination is critical for treatment planning. For this reason exam include detailed description of size (depth, width), rectovaginal exam to detect paramerium and pelvic side wall extension.
With advance disease enlarge supraclavicular L.N or inguinal L.N, lower extremities edema, ascites, decrease breath sound indicate lung metastases.
External genital and vaginal examination looking for concomitant lesions, HPV is risk for vulvar, vaginal, cervical cancer. Superficial groin and femoral L.N examination.
Cervix may appear grossly normal if micro invasive disease, or visible lesion entophytic, exophtic, polyploidy lesion or barrel-shaped cervix, cervical ulceration or granular mass.
Watery, purulent or bloody discharge.
Bimanual exam. Enlarge uterus, advance may have vaginal involvement.
Rectovaginal examination find rectovaginal septum thick irregular.
Per-rectum exam also required.
Test for women with symptoms of cervical cancer or abnormal pap smear results.
Diagnostic testing
Diagnostic test may be included in clinical staging of cervical cancer these are limited to standard CXR, IVP and barium enema.
1. Medical history and physical exam this include information related to risk factors and symptoms of cervical cancer.
PAP SMEAR screen test not diagnostic but may be done an abnormal pap test may mean more testing need.
2. Colposcopy symptoms suggestive cervical cancer or if abnormal pap test an instrument that stay outside the body with magnifying lenses. It help the doctors see the surface of the cervix closely and clearly, it can done safely even in pregnancy like pap test , not do during menstrual cycle, use acetic acid solution on cervix if abnormal area seen so biopsy taken.
3.Biobsy
colposcopy biopsy=abnormal area biopsy forceps small 1/8 inch section result mild cramping brief pain slight bleeding under local anaesthetic agent.
Endocervical curettage (TZ when cannot be seen by colposcopy by narrow instrument into cervical canal to scrape the inside tissue and send for lab exam.
Cone biopsy, removed a cone shaped piece of tissue from cervix including TZ. Cone biopsy not only diagnostic also treatment it completely remove precancerous lesion. It can done LEEP, LLETZ (local anaesthesia in doctor's office)
Cold knife cone biopsy in hospital surgical scalpel or laser is used, general anaesthesia or spinal or epidural.
4. Imaging has a vital role in determining correct management at initial staging, recurrent disease and complication.
Chest X-ray
Pelvic MRI(soft tissue parts of the body)= most sensitive for detecting locally advance disease.
imaging determined (tumor volume, parametrical extension, confirming that tumor is confined to the cervix, nodal status.
CT scans are usually done if the tumor larger or if there is concern about cancer spread.
Intra venous urography (rarely used if any abnormal area from cervical cancer obstructing ureters)
PET this test helpful if cancer spread to L.N using special glucose contain radioactive atom, cancer cells in the body absorbed this sugar and used special camera can detect radioactivity.
5.Cystoscopy, proctoscopy and EUA most often done in women who have large tumors.
STAGING
Tests used during cervical cancer staging
A-Lab test (CBC, urine analysis, LFT, RFT)B-Radiological (CXR, IVP, CT scan, MRI)
C-Procedural (cystoscopy, proctoscopy, EUA
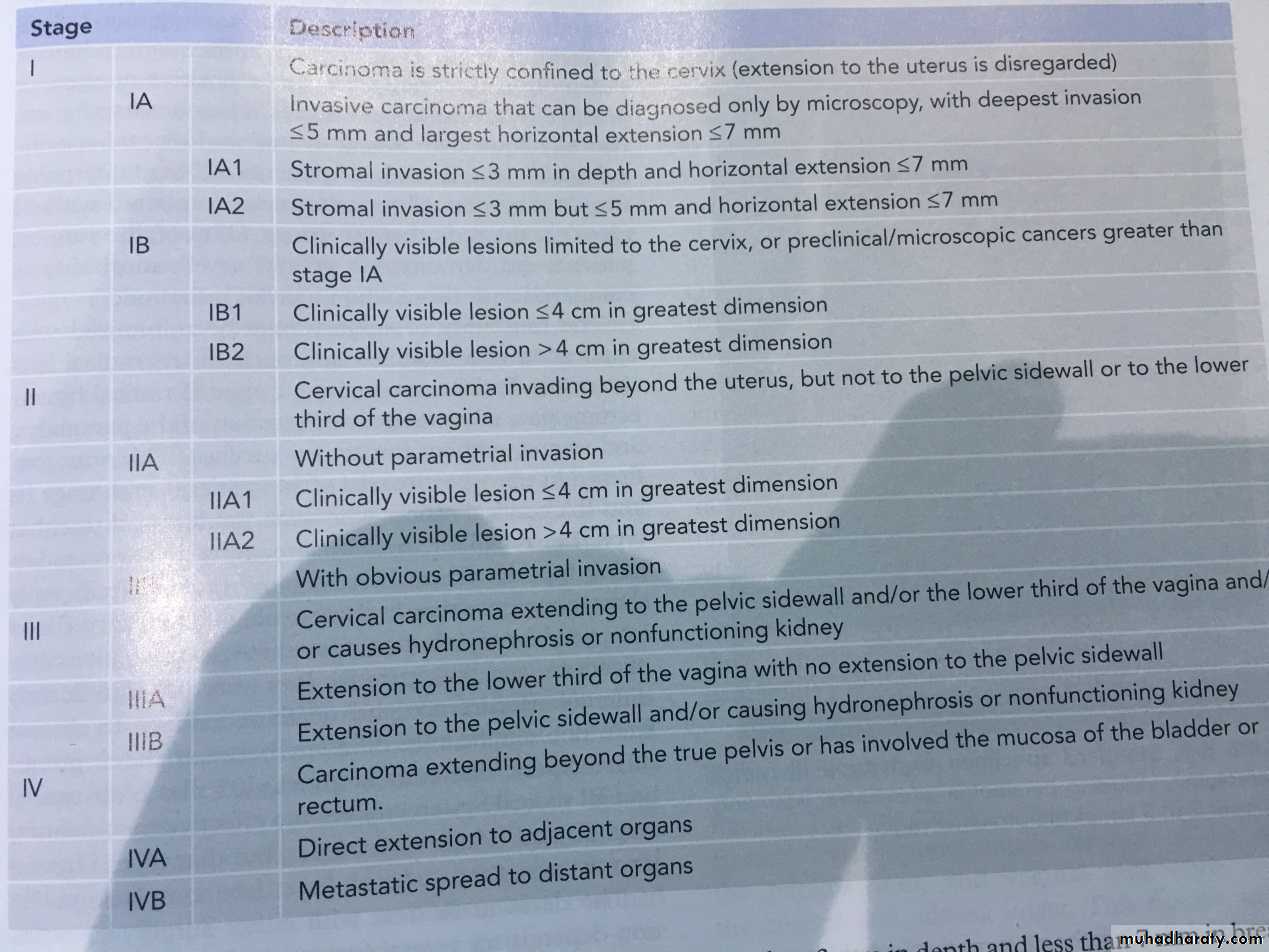
Cervical cancer staging
FICO staging based on physical exam with or without anesthesia and limited imaging study CXR, IVP and barium enema. C-T , MRI, PET may be used to assist in case of clinical suspsion of parametrial and pelvic side wall metastasis. few other tests in some cases, cystoscopy and proctoscopy. It is not based on what find during surgery.Surgical staging Lymph node dissection of pelvic and Para-aortic lymph node.
Prognosis
FIGO stage, size, surgical staging.Cervical cancer survival
Stage 5-years survival
1A 100%
1B 88%
11A 68%
11B 44%
111 18-39%
1VA 18-34%
Treatment
Early stage disease (stage I-IIA)
Advance stage IIB and higher.
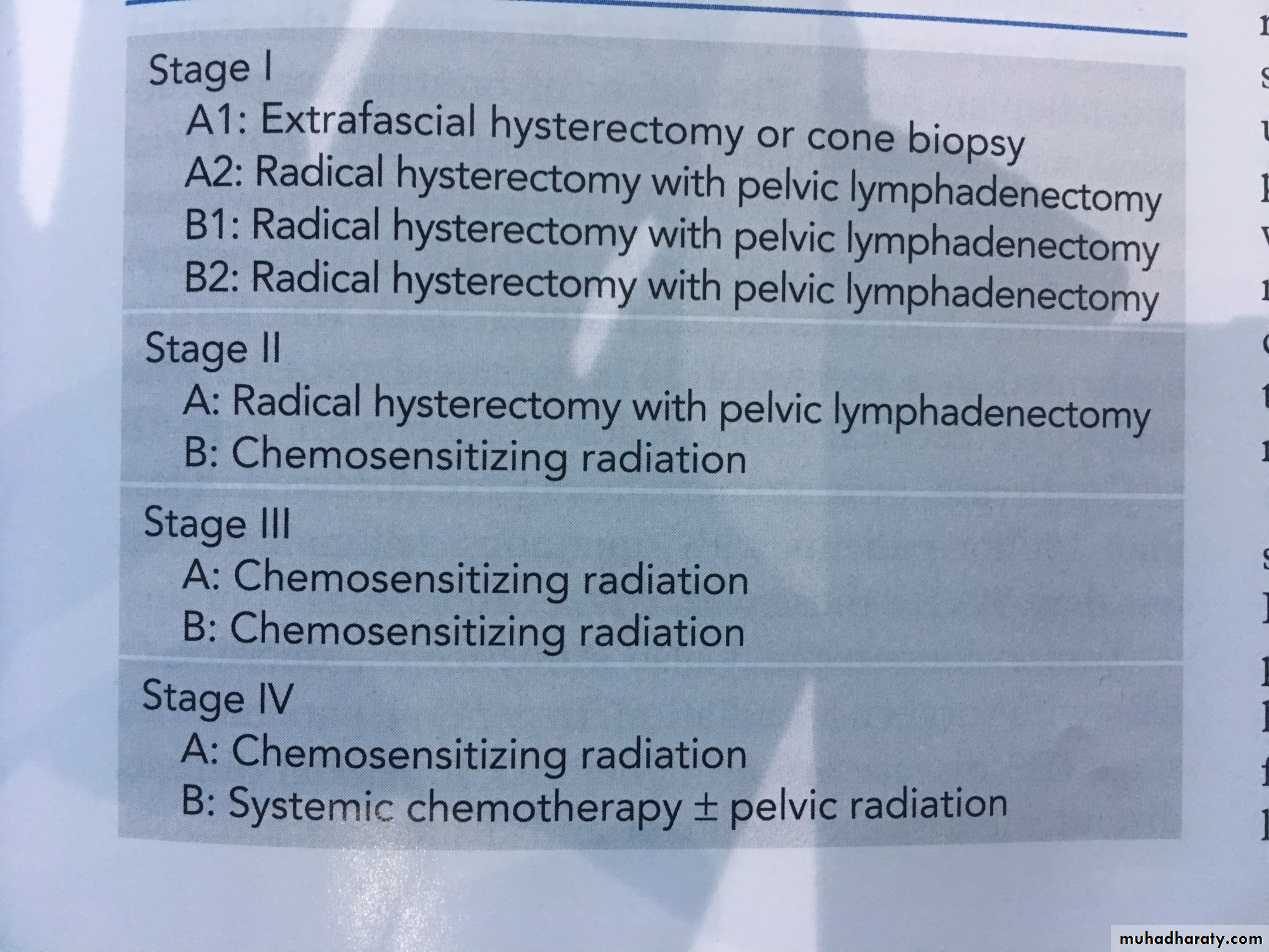
Primary disease stage 1A type one hysterectomy
1A2 radical hysterectomyTrachelectomy (uterine preservation treatment) in women wish to conserve fertility. MRI is performed preop. To assess tumour size and location. Exclude tumour greater than 2cm and involvement of uterine isthmus.
Stage 1B-11A either surgery or radiotherapy
Radical hysterectomy selected for young patient with low BMI, wish to preserve ovarian function, and have concern about sexual function.Stages 11B through 1VA
Advanced stage cervical cancers, treatment for these tumors must be individualized to maximize patient outcome, it have poor prognosis, radiation therapy by external beam pelvic radiation, brachytherapy(intracavity radiation), currently chemo radiation use for advance cancer, pelvic exenteration by removal of bladder,rectum,uterus (if present) and surrounding tissues.Stage 1VB
Poor prognosis treated with goal of palliation.