


ZYGOMATICO-ORBITAL FRACTURES
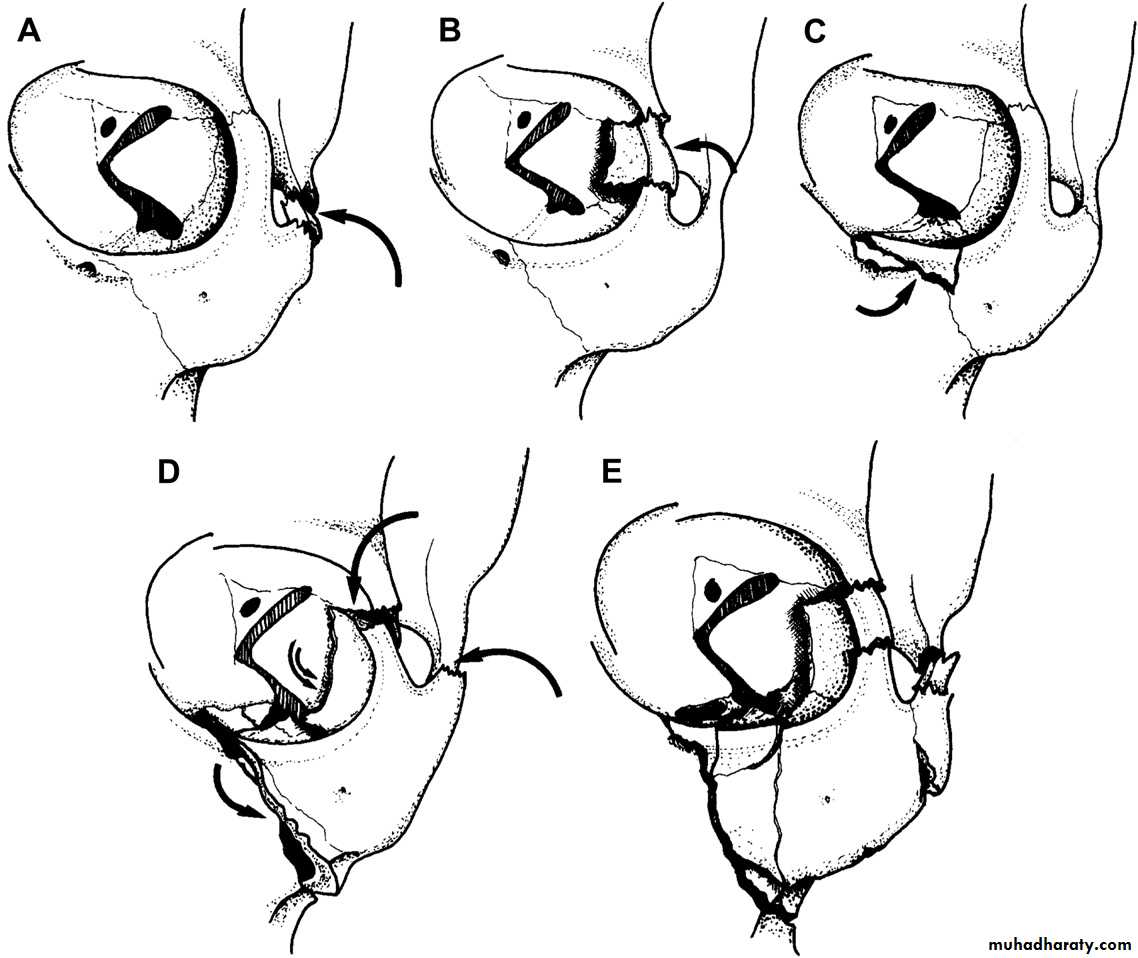
Zygomaticomaxillary complex fracture types: (A) type A1, isolated zygomatic arch fracture; (B) type A2, isolated lateral orbital wall fracture; (C) type A3, isolated infraorbital rim fracture; (D) type B, tetrapod fracture; (E) type C, multifragment zygoma lateral orbit complex fracture.
CLINICAL PRESENTATION
* Patients with nondisplaced ZMC fractures may exhibit only soft tissue signs such as ecchymosis and edema overlying the fracture sites and conjunctival hemorrhage. * Displaced fractures will generally cause ipsilateral facial flattening .The zygomatic arch may be intact, fractured and depressed, or bowed out.* Displaced ZMC and isolated zygomatic arch factures may also cause trismus as a result of spasm of the masseter muscle or mechanical impingement of the coronoid process against the displaced fragments.
* Others: Enophthalmos, Diplopia or squint, Limitation of ocular movements, Anesthesia or paraesthesia of the cheek, Buccal ecchymosis, Gagging of the posterior teeth on the injured side, Step deformity at fronto-zygomatic and zygomatico-maxillary sutures, and epistaxis.
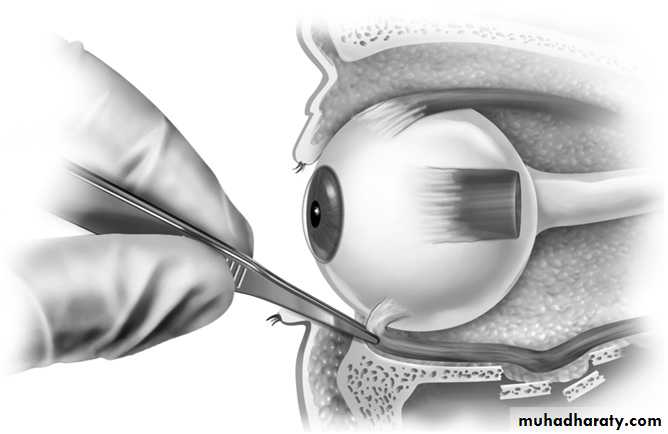
Evaluation of the extraocular muscles is performed by finger tracking. A forced duction test will generally differentiate between mechanical entrapment and restriction secondary to edema or contusion.
If restricted range of motion is detected, topical anesthesia is applied to the sclera and the forced duction test is performed by grasping the insertion of the rectus muscles at two simultaneous points with two pairs of Adson forceps.
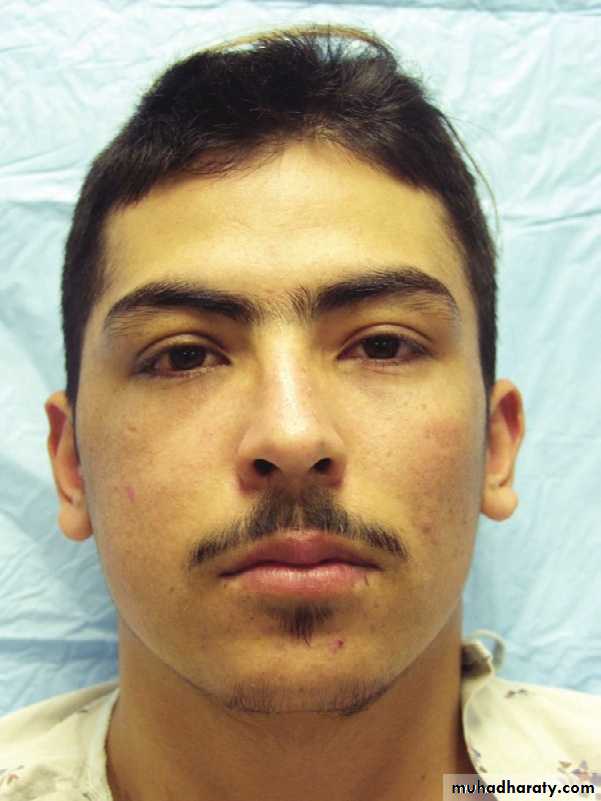
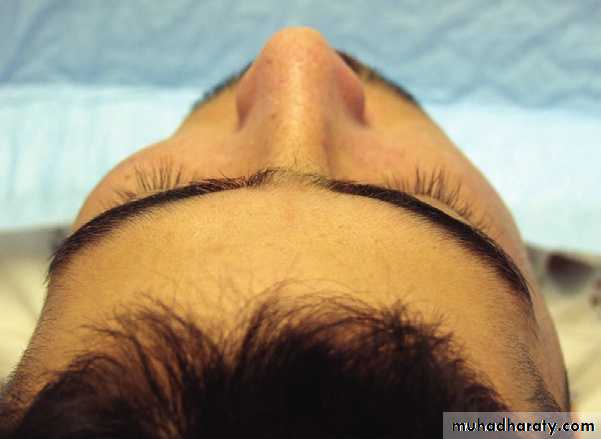
Typical appearance of a patient with a displaced fracture of the right zygomaticomaxillary complex. There is flattening in the area of the right malar eminence. Superior view of the same patient showing an obvious decreased projection of the fractured zygoma on the right.

Enophthalmos in a patient with a displaced zygomatico-maxillary complex fracture complicated by a fracture and inferior dislocation of the orbital floor
RADIOGRAPHIC EXAMINATION
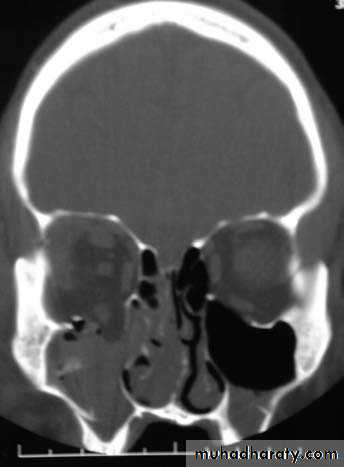
Computed TomographyCT is the gold standard for radiographic evaluation of zygomatic fractures. Axial and coronal images are obtained to define fracture patterns, degree of displacement, and comminution and to evaluate the orbital soft tissues.
Plain Radiographs
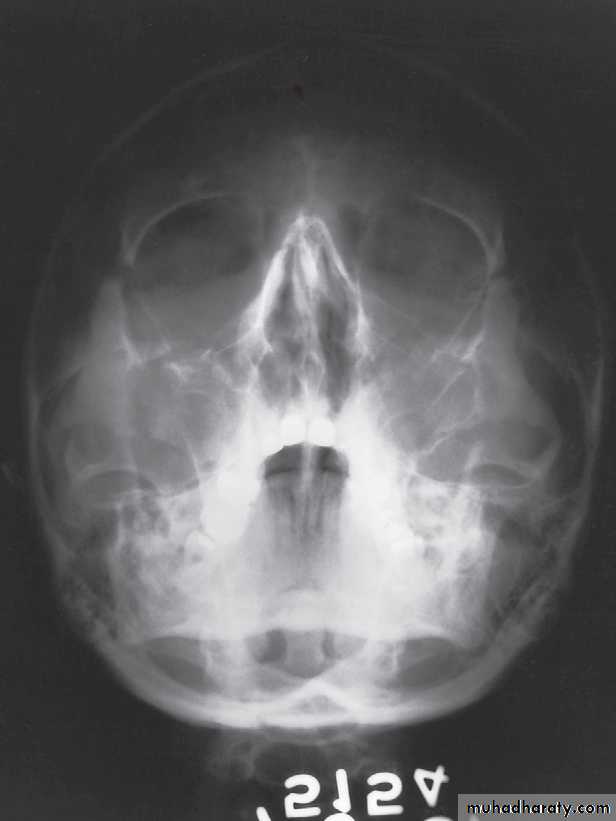
Waters’ View
Caldwell’s View
Submentovertex View

SURGICAL APPROACHES
Coronal approachA coronal flap is a useful approach when extensive exposure of the zygomatic arch, zygoma, and orbit is indicated.
Supraorbital eyebrow approach
A 2-cm incision placed over the lateral portion of the eyebrow allows rapid access to the lateral orbital rim and the zygomaticofacial suture.
Maxillary vestibular approach
Rapid and esthetic access to the anterior portions of the midface and zygomaticomaxillary buttress can be obtained through this approach.
Lower eyelid approaches
3 surgical options are available: The subciliary, lower eyelid crease, and transconjunctival approaches are the most commonly used methods.
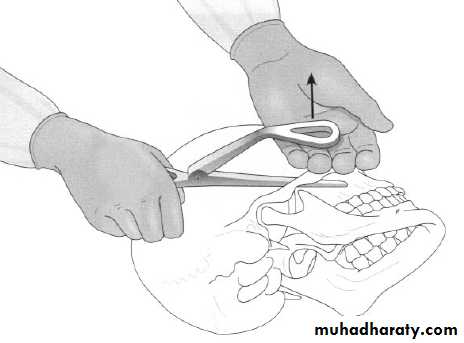
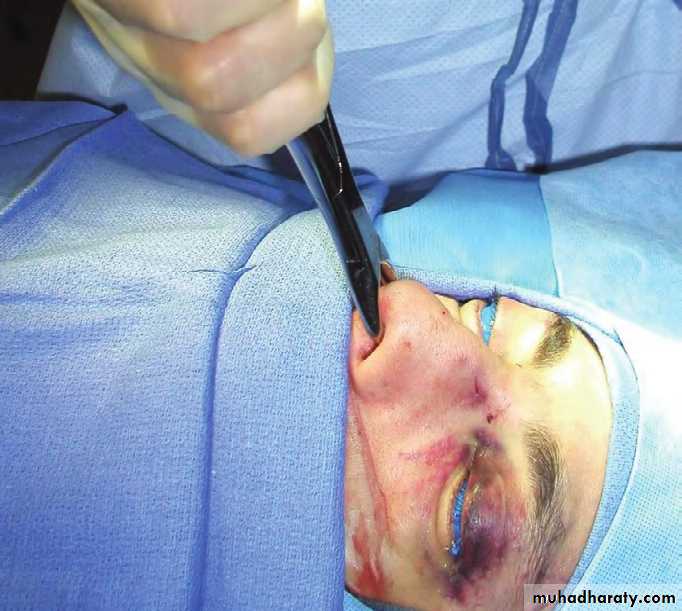
Gillies' temporal approach for the elevation of a depressed fracture's zygomatic complex
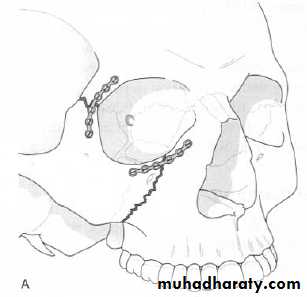
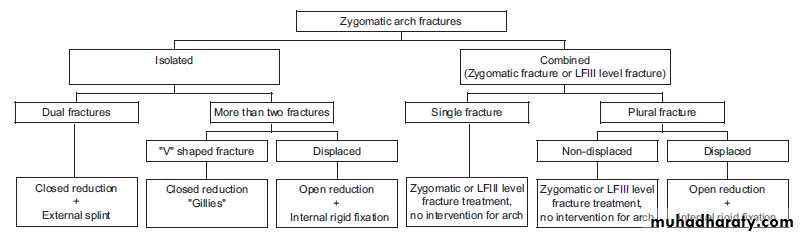
Displaced fractures are best managed by open reduction and fixation at two to three points. In the absence of comminution or instability at the zygomatic arch, reduction under direct visualization plus fixation at the frontozygomatic suture, zygomaticomaxillary buttress, and inferior orbital rim remains the best treatment option.
Intraoral exposure and fixation
of zygomaticomaxillary buttress fracture.BLOW-OUT FRACTURES
Orbital fractures are generally the result of blunt force trauma to the eye, causing a fracture of the thin bony wall or floor of the orbit. Increased pressure from sneezing, nose blowing, or coughing may precipitate air passage through a previously injured inferior or medial orbital wall. The inferior rectus muscle may become entrapped, resulting in diplopia on upward gaze. Injury to the inferior orbital nerve may result in decreased sensation of the cheek and upper lip.A 22-year-old otherwise healthy woman was struck in the right eye with an open hand at evening. The next morning, she blew her nose and experienced an abrupt onset of right periorbital swelling. She later complained of numbness of the right cheek and diplopia on upward gaze. The examination result was unremarkable, except for a swollen right lower eyelid with palpable crepitus.

THEORIES
Two mechanisms: hydraulic and buckling are generally believed to cause blowout fractures.The theory of the hydraulic mechanism suggests that the pressure increase of the orbital contents fractures thin and fragile parts of the orbital walls
The buckling mechanism explains that the orbital walls bend in response to impacts, then fracture.
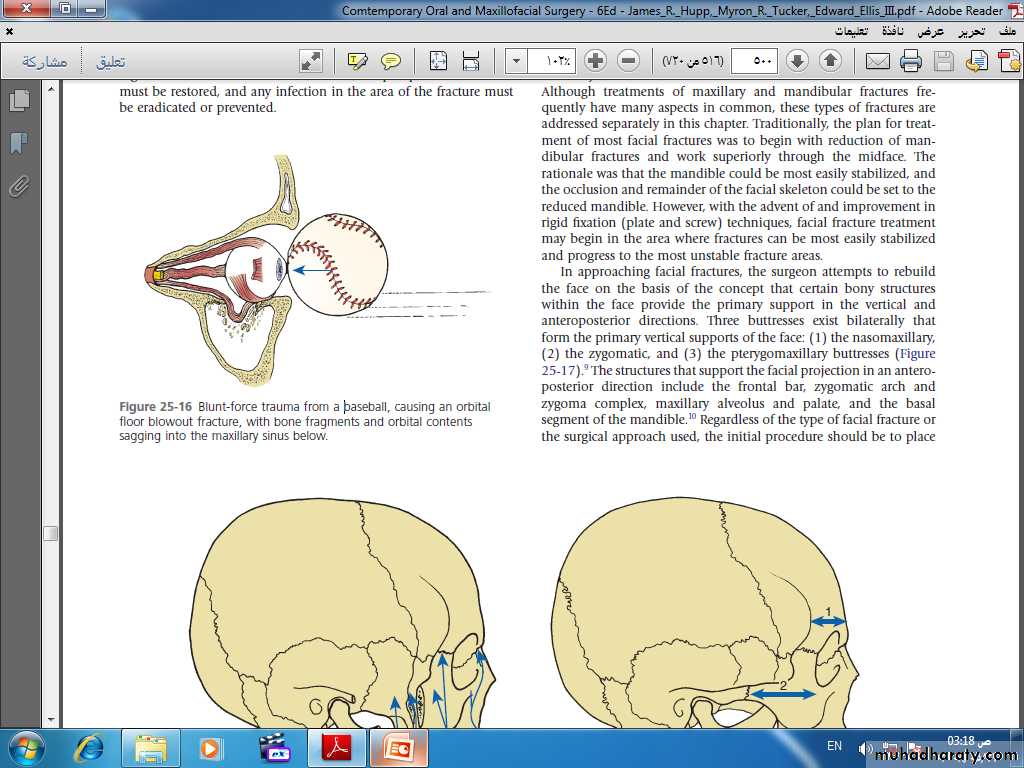
Blunt-force trauma from a baseball, causing an orbital
floor blowout fracture, with bone fragments and orbital contents sagging into the maxillary sinus below.Restricted eye movement
Subconjuctival approach and reconstruction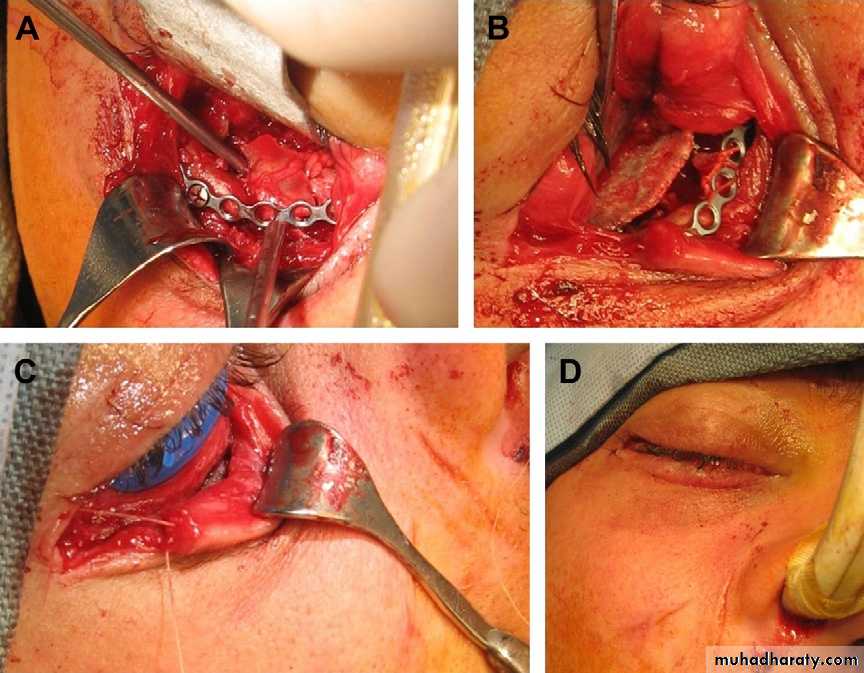
Intraoperative photographs of orbital floor reconstruction for patient with orbital floor blow-out fracture. (A) Fixation of orbital rim fractures with 1.3-mm plate through transconjunctival approach with lateral canthotomy and inferior cantholysis. (B) Reconstruction of orbital floor with Medpor Titan porous polyethylene.
NASAL AND NASO-ETHMOID FRACTURES
Nasal fractures are classified according to extent of injury into 3 planes
Plane I: ....................
Plane II: ....................
Plane III: ....................
The nasal complex is the most frequently fractured bone in the face in the adult patient. Due to its location on the face, less force is required to fracture the nasal complex than any other facial bone. Because of the frequency of injury, as well as complex topography and different components (bone, cartilage, mucosa, skin) of the nasal complex, appropriate management of the acutely injured nose is imperative in order to prevent adverse sequelae.

Bilateral comminuted nasal bone fractures and septal deviation following motor vehicle collision.

Using appropriate nasal reduction forceps, the nasal bones and the septum must be reduced in the appropriate vector. The reduction must be maintained by intranasal packings and/or splints.
Walsham forceps, Boies elevator, Asch forceps
NOE injuries: PATTERNS
Isolated NE injury: Usually this is due to severe impact confined to the nasal area. Maxilla’s frontal process(es) are fractured and depressed with nasal saddle deformity and elevation of nasal tip. Nasal bones may remain intact. Medial canthal ligament is
mostly still attached to a large bony fragment which facilitates its repositioning.
High –level NE injury (Craniofacial): In which, there is frontal bone fracture. This type may carry a risk of associated injury to the anterior cranial fossa. CSF –leakage is frequently present.
Low –level NE injury: Characterized by crushing of NE complex. Concomitant Le Fort III or severe Le Fort II fractures are often present. This type is frequently associated with orbital floor fractures and severe ocular injuries.
In severe impacts, especially those sustained by road traffic accidents, the last two patterns may be found concomitantly.
FINDINGS OF MY WORK (MASTER)
* Incidence of NE fractures in midface trauma was estimated and found to be (11.8 %).* Road traffic accidents were the cause of injury in more than half of the cases.
* Clinical signs associated with these injuries were examined and recorded as follows: Telecanthus in 15 cases (100 %), Saddle deformity in 13 cases (86.7 %), Lacerations in 11 cases (66.7 %), Mongoloid slant in 9 cases (60%), Enophthalmos in
6 cases (40 %), CSF –leak in 5 cases (33.3 %), infraorbital paresthesia in 4 cases (26.7 %), diplopia 3 cases (20 %) septal deviation in 2 cases (13.3 %), and epiphora in 2 cases (13.3 %).
CONCLUSIONS (MSc thesis)
* The majority of nasoethmoid (NE) injuries are combined with other facial fractures.* Nasoethmoid fractures should be considered in the diagnosis of all severe nasal, LeFort II, and LeFort III fractures.
* Extended NE injuries can occur either as “ highlevel” or “low-level” patterns. In severe cases, the two forms may be present.
* CSF–rhinorrhoea is a frequent finding in high –level NE injuries.
* Enophthalmos should be suspected in every naso-ethmoid injury, especially when a concomitant zygomatic fracture exists.
FRONTAL BONE FRACTURES
A frontal bone fracture is a unique facial fracture that often requires complex management. The location of the frontal bone, which contains the frontal sinus, is adjacent to vital structures, including the brain and eyes. A frontal bone fracture often occurs concomitantly with fractures of the skull, orbital roof, and nose, and many times it is associated with Le Fort and naso-orbito-ethmoid (NOE) fractures.
MANAGEMENTOF THE FRONTAL BONE FRACTURES
The three components involved in frontal sinus management include the anterior table, posterior table, and nasofrontal ducts.Minimally displaced anterior table fracture may require no treatment. If the anterior table fracture is severely comminuted or open, direct access to the bone is required. Once generous access is established, evaluation of the nasofrontal duct can be performed. If the nasofrontal ducts are patent, the surgeon may proceed with the appropriate reduction and fixation of the anterior table fracture.
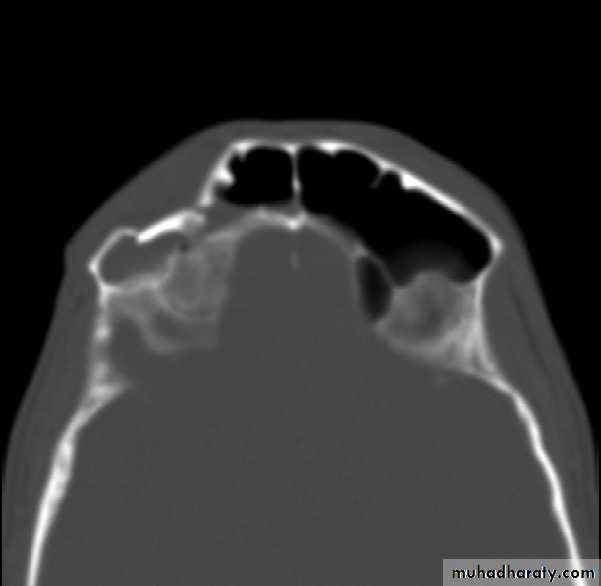
Displaced anterior table of a frontal sinus fracture.

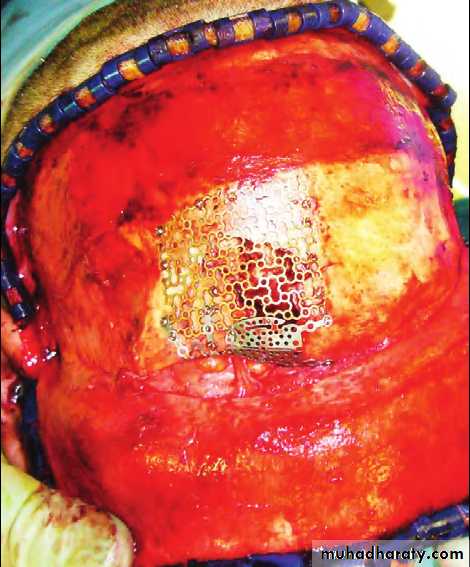
Reconstruction of the anterior table via coronal access with miniplates and mesh.
Dural repair and reconstruction of the frontal bar after craniotomy.PANFACIAL FRACTURES
* Panfacial fractures are those involving the mandible, maxilla, and zygomatic complex at the same time and usually accompanying naso-orbito-ethmoid (NOE) and frontal bone fractures.
* They are often associated with soft tissue injuries and loss of bony structures that can lead to severe posttraumatic deformities and disabilities like malocclusion, “dish” face deformity, and enophthalmos