Local Anesthetics
Dr. Hussain Adday Aljabery
M.B.Ch.B . M.Sc. FICMS ( RAD. )
Pharmacology

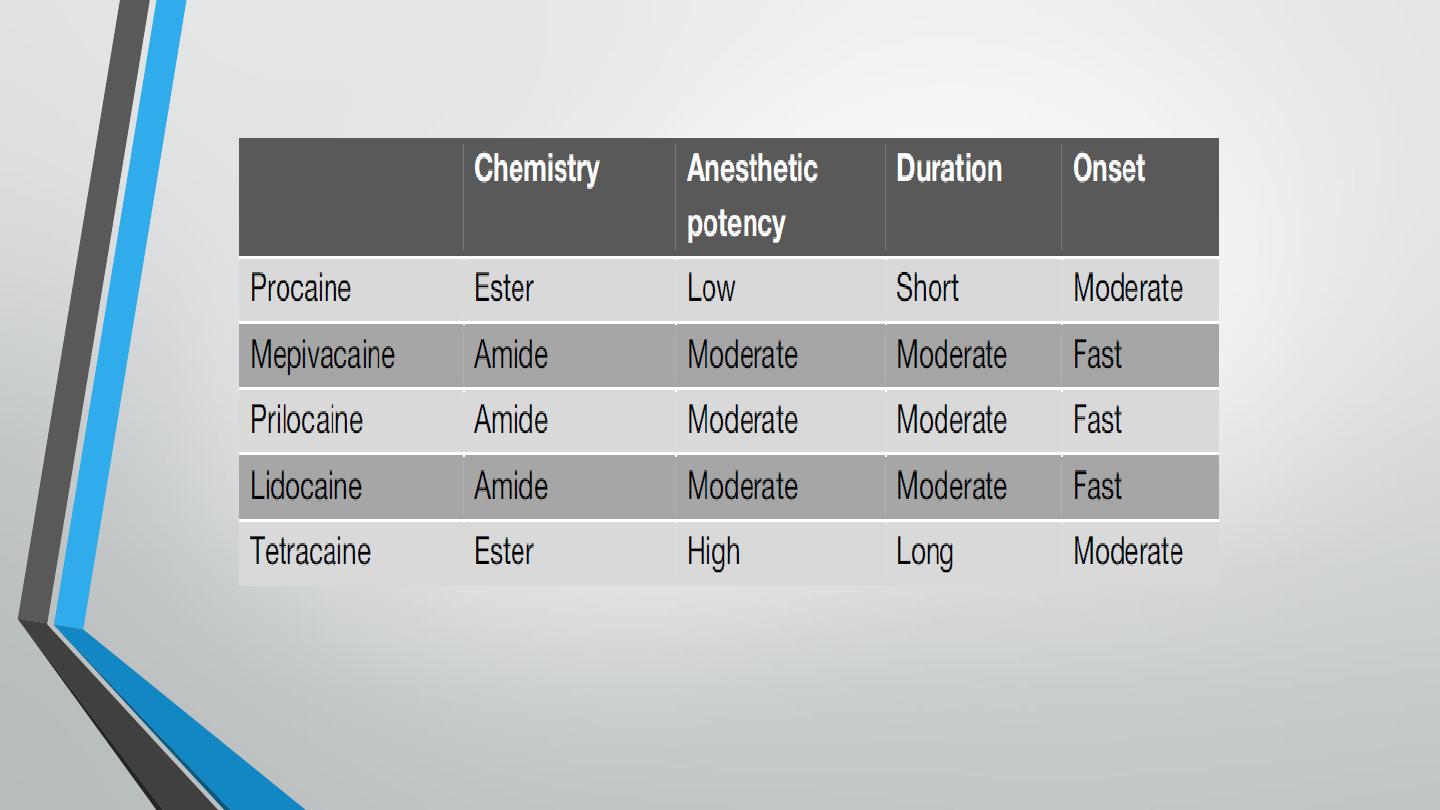
Classification
•
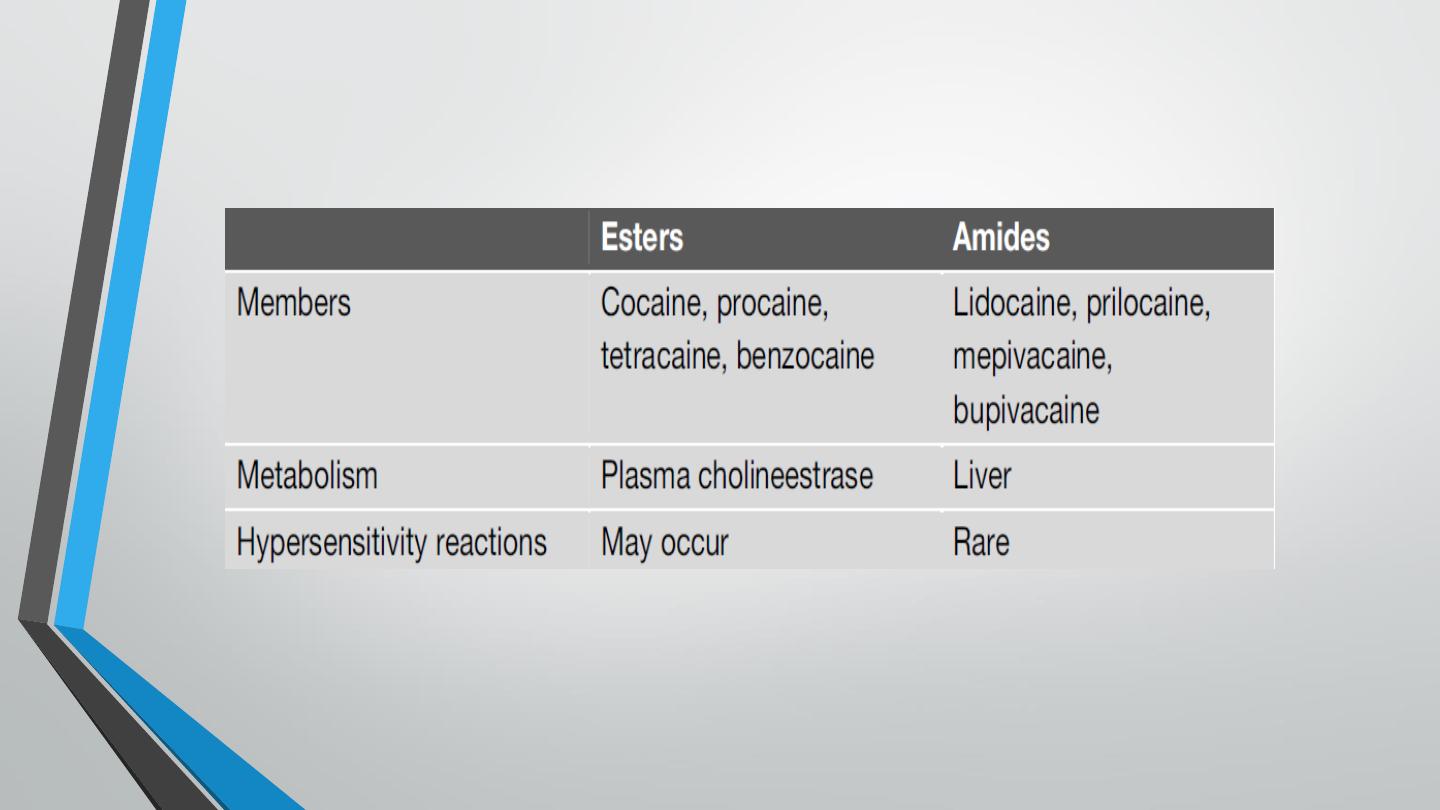
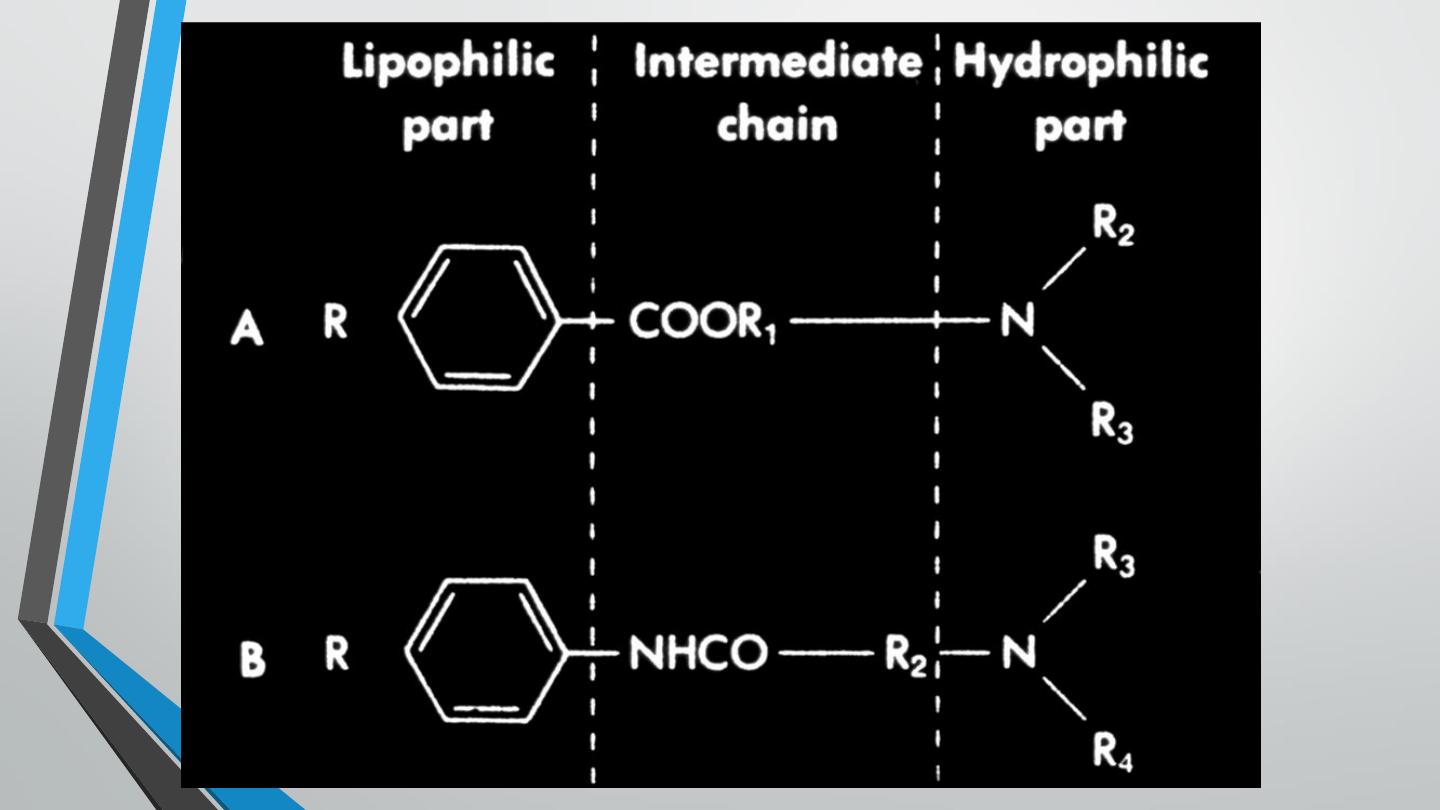
There are two classes of local anesthetics: amides and esters. The primary
differences between the two classes are in their relative metabolism
(amides have primarily a hepatic metabolism, whereas esters are
metabolized by plasma cholinesterases) and their potential for allergic
reactions (esters more than amides).

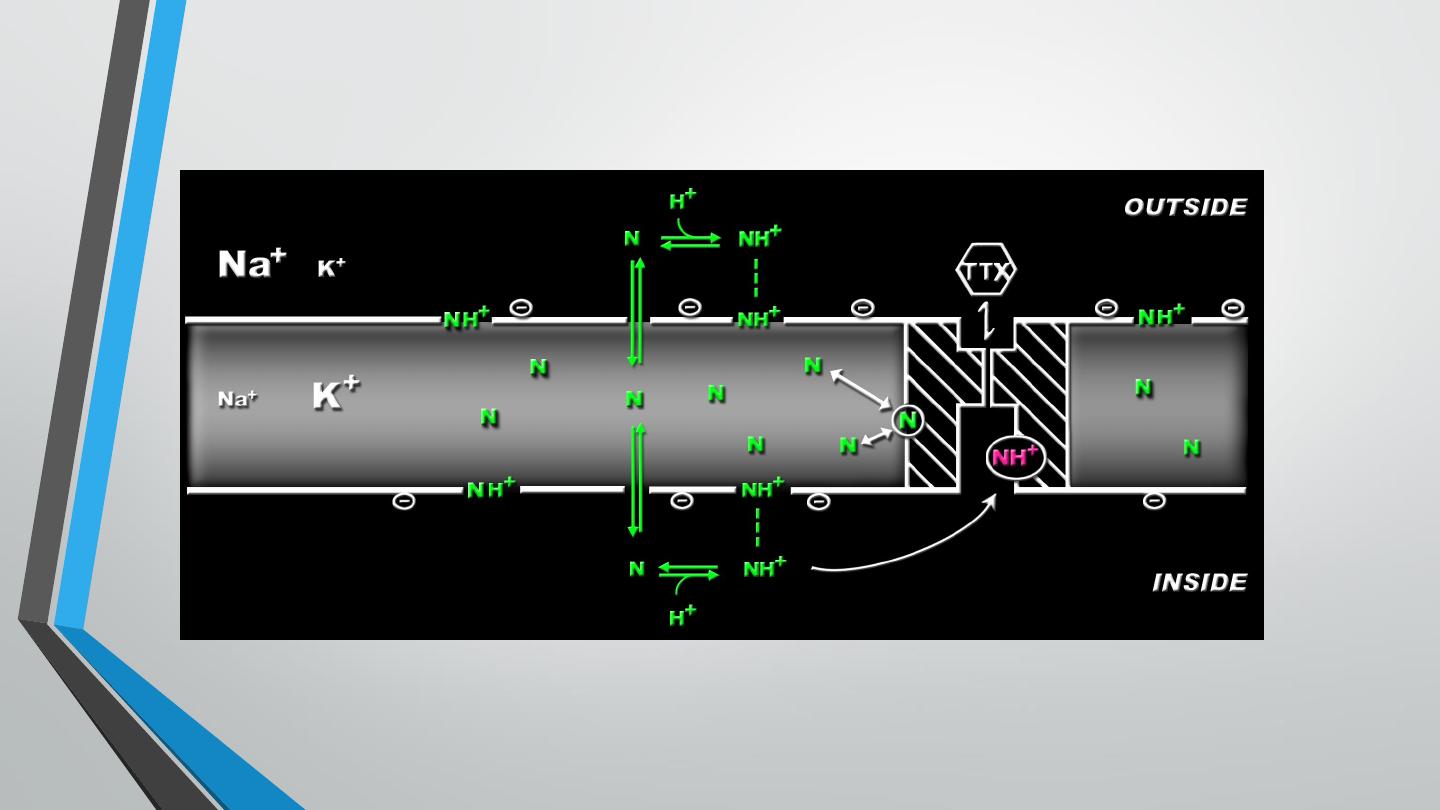
Mechanism of action
•
Local anesthetics block voltage dependent Na+ channels within the nerve
fibers →↓ nerve conduction.
•
In general, small nerve fibers (that carry pain sensation) are more sensitive
to local anesthetics than large fibers (motor and other sensations).
•
Myelinated fibers are blocked before non-myelinated fibers of the same
diameter.

Metabolism of Amide Local Anesthetics
•
Biotransformation by hepatic microsomal enzyme system
•
Drugs may increase metabolism via enzyme induction
•
Liver disease may decrease metabolism via decreased
functional tissue
•
Decreased metabolism secondary to decreased hepatic
blood flow

Metabolism of Ester Local Anesthetics
•
Hydrolyzed by plasma cholinesterase
•
Factors which may lead to decreased plasma esterase activity
•
Liver dz—decreased protein synthesis
•
Pregnancy—decreased pseudocholinesterase activity
•
Atypical pseudocholinesterase
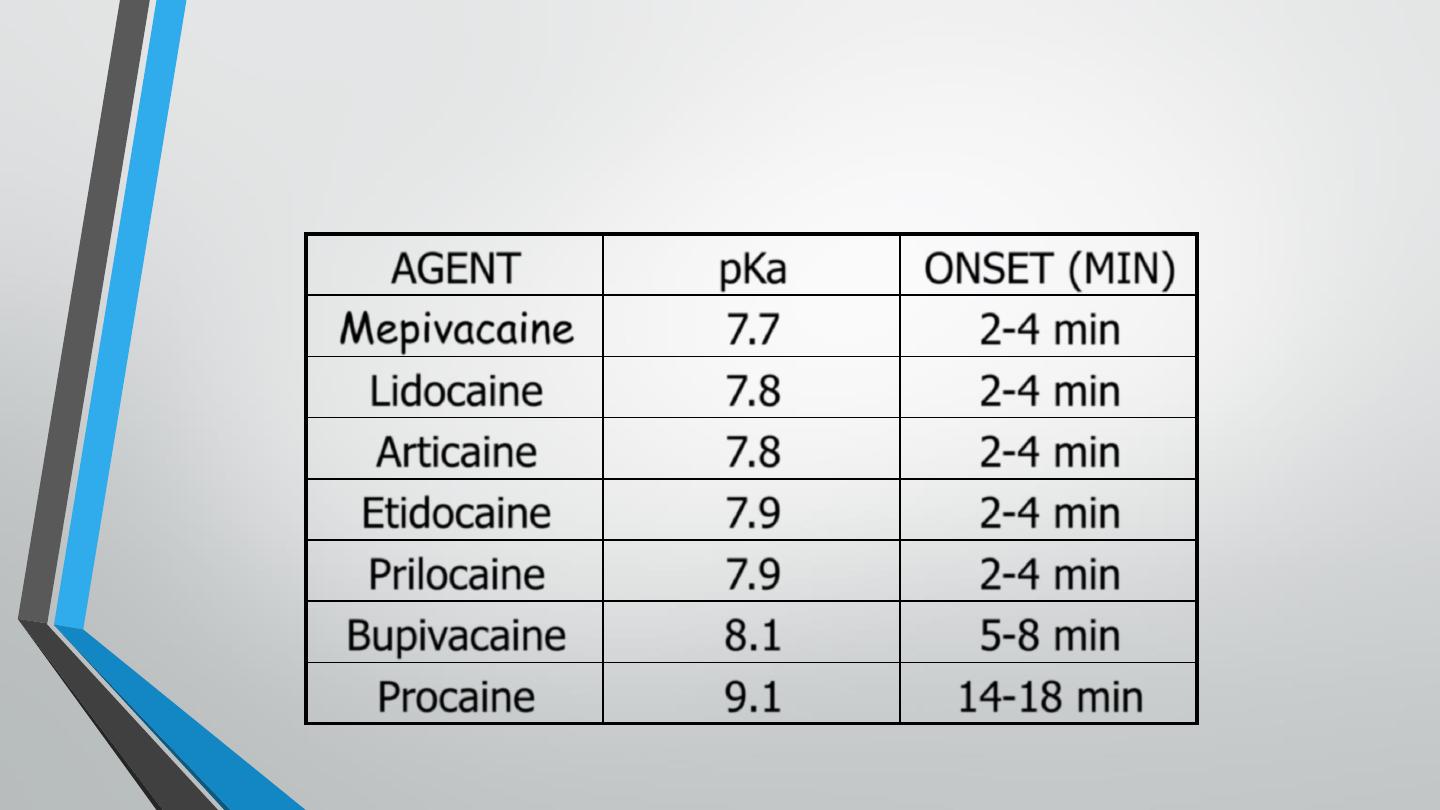
Local Anesthetics: pK
a
vs. Onset of
Action
AGENT
pKa
ONSET (MIN)
Mepivacaine
7.7
2-4 min
Lidocaine
7.8
2-4 min
Articaine
7.8
2-4 min
Etidocaine
7.9
2-4 min
Prilocaine
7.9
2-4 min
Bupivacaine
8.1
5-8 min
Procaine
9.1
14-18 min

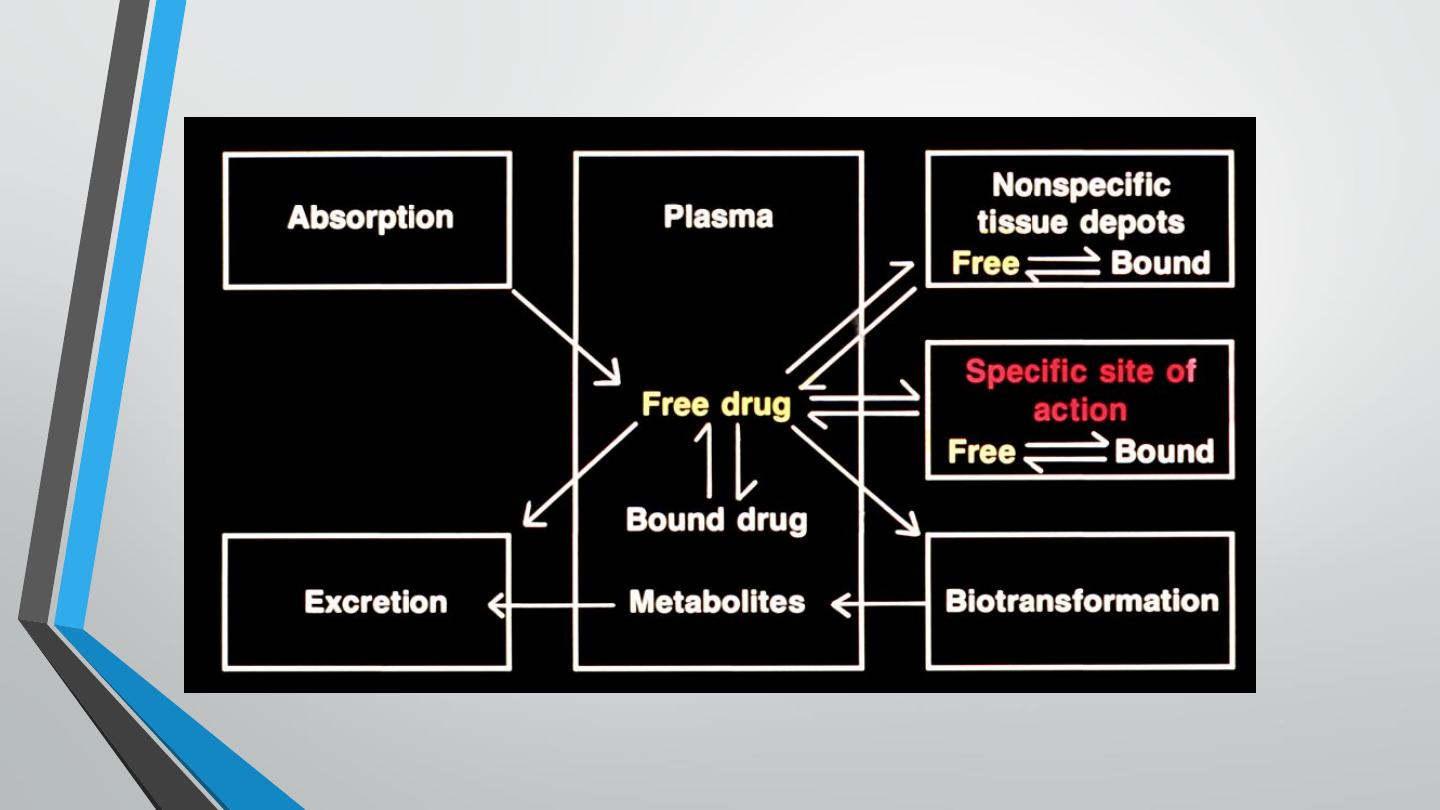
Excretion of Local Anesthetics
•
Active metabolites excreted by kidney
•
Severe renal disease may result in accumulation of active
metabolites and produce toxicity

Adjuvants of local anesthetics
❑
Vasoconstricotors e.g. adrenaline:
– They are added to produce local VC; this will reduce wash of the anesthetic
by the local blood flow and thus prolongs the duration of the anesthetic.
Vasoconstrictors should not be added for ring block of hands, feet, fingers,
toes, and ear pinna to avoid tissue damage.
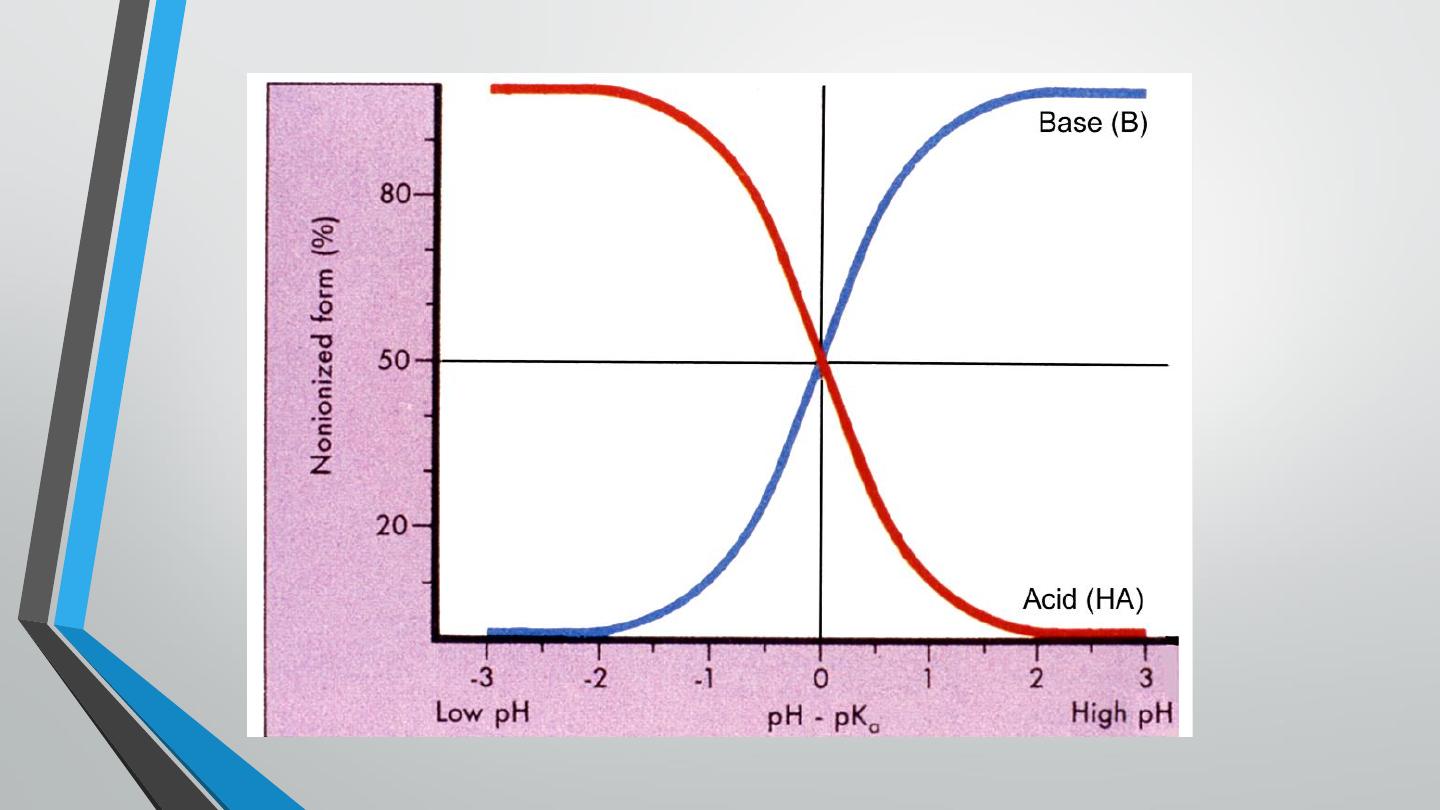
❑ Sodium bicarbonate:
– All local anesthetics are weak bases. Addition of bicarbonate to the
anesthetic solution maintains the anesthetic in the non-ionized state and this
increases lipid solubility and enhances penetration of the anesthetic into the
nerve sheath.

Techniques and clinical uses
◼
Surface (topical) anesthesia: is used for anesthetization of the skin, mucous
membranes, or cornea.
▪
Treatment of itching caused by insect bites or irritant condition.
▪
To relieve pain caused by oral, laryngeal, or rectal disorders e.g. piles.
▪
Corneal anesthesia in ophthalmic surgery.
◼
Infiltration anesthesia: injecting an anesthetic directly into the subcutaneous
tissue for minor surgical procedures e.g. dental procedures. Epinephrine may be
added to prolong the duration of action.
◼
Nerve block: injecting the local anesthetic close to the appropriate nerve trunk
proximal to the intended area of anesthesia e.g. radial nerve block or retro-orbital
block for ocular surgery.


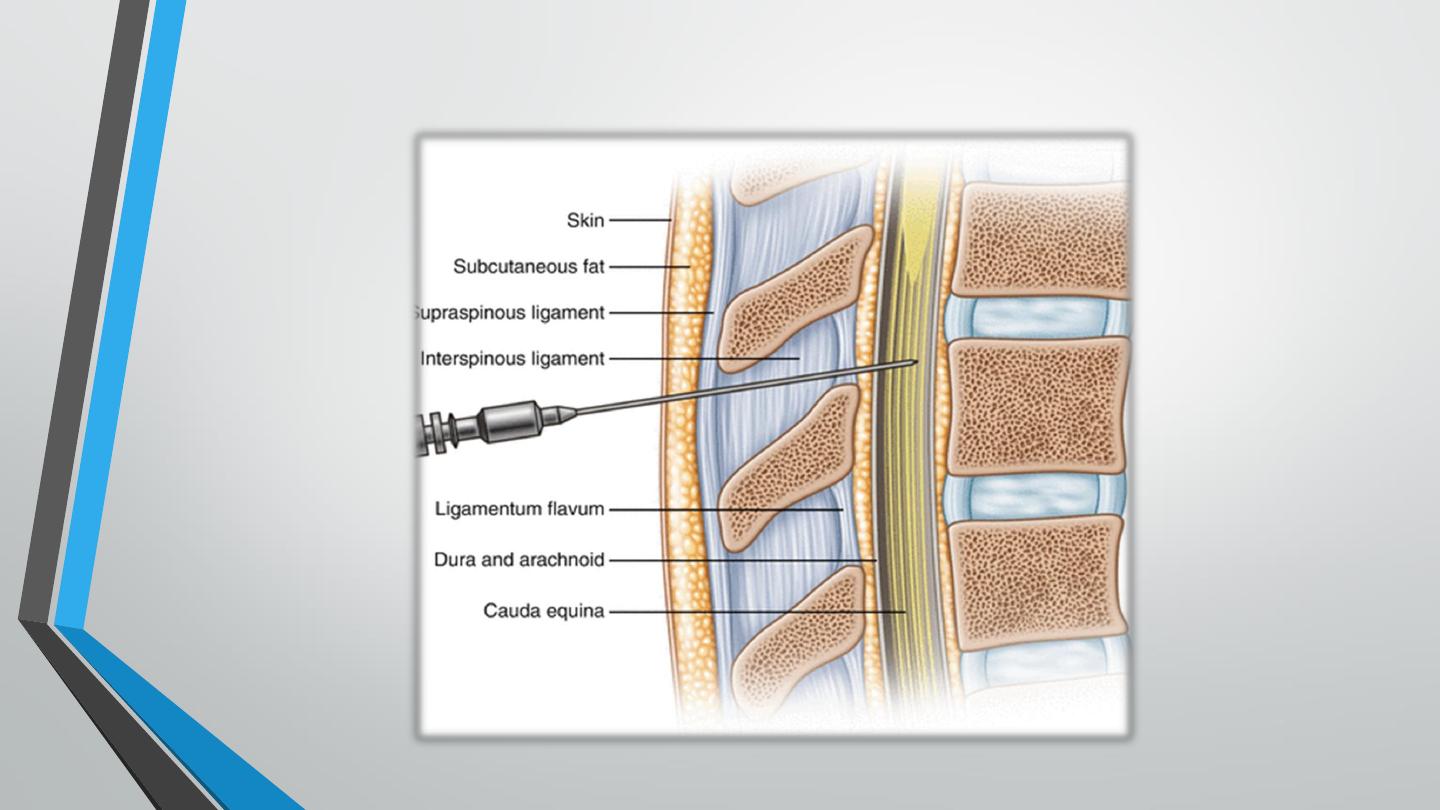
▪ Spinal anesthesia: is used for surgeries of the lower limb or pelvic structures. A
local anesthetic is injected into the subarachnoid space below the terminal end
of the spinal cord (usually between 3
rd
and 4
th
lumber vertebra).
◼
Epidural anesthesia: the anesthetic is infused into the space between the dura
mater and the connective tissue lining the vertebral canal as alternative to
subarachnoid anesthesia.

Adverse effects
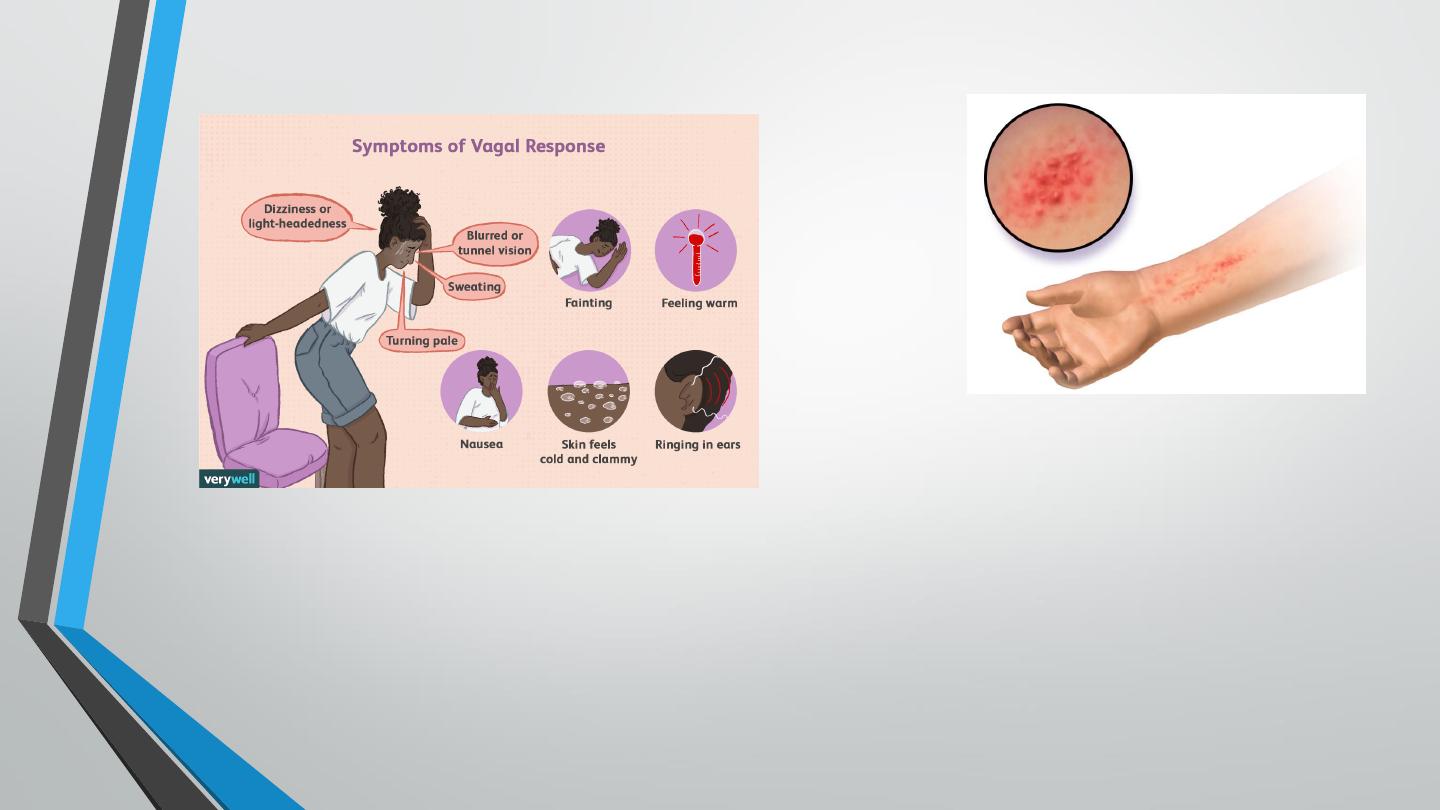
– Surface anesthesia: allergic dermatitis.
– Infiltration anesthesia: faulty intravascular injection can lead to:
CNS excitation: irritability and convulsions
CVS depression: bradycardia, hypotension, myocardial depression or cardiac arrest.
– Vasovagal syncope: vasovagal (also called neurocardiogenic) syncope is usually associated with
bradycardia (rather than tachycardia) and pallor (rather than flushing). These differences can be
helpful in distinguishing it from anaphylaxis.
– Spinal anesthesia:
Spinal shock due to sympathetic outflow paralysis.
Headache due to CSF leakage.
Respiratory paralysis.
Septic meningitis.

Recommendations
▪
The choice of local anesthetic for infiltration depends on several factors, including duration of
the procedure, need for hemostasis, patient sensitivity to catecholamines, and patient allergy to
local anesthetics.
▪
Prior to infiltration, the clinician should determine if the patient has any history of allergy.
Patients with a true allergic reaction to a local anesthetic need evaluation by an allergy specialist.
▪
Local anesthetic infiltration is contraindicated in the following conditions:
– If the area needed to be anesthetized is so large because the amount of anesthetic needed
exceeds the maximal safe dose.
– If the patient has history of allergy to local anesthesia.
Spinal shock
•
–phenomena surrounding physiologic or anatomic transaction of the spinal
cord that results in temporary loss or depression of all or most spinal reflex
activity below the level of the lesion. Demonstrated only in settings of
severe spinal cord injury occurring during relative brief period.

CHARACTERISTIC OF SPINAL SHOCK
•
Motor Effects
– Paraplegia ,Quadriplegia
•
Loss of tone -Muscles become flaccid
•
Areflexia - All superficial and deep reflexes are lost
•
Sensory Effects -All Sensations are lost below the level of transection
•
Complete lesions above T1 will eliminate all sympathetic outflow.
•
Lesions between T1 and T6 will preserve sympathetic tone in head and upper
extremities but deny it to the adrenals and lower extremities.
•
Lesions between T6 and the lumbar cord will preserve adrenal innervation but
denervate the lower extremities.

Treatment of spinal shock
▪
Place the patient in the supine position with the legs elevated.
▪
Airway support: oxygen and artificial respiration.
▪
If there are convulsions, give i.v. diazepam.
▪
If there is hypotension, give i.v. fluids plus vasoconstrictors.
▪
Cardiopulmonary resuscitation (CPR) is necessary when cardiac function is
interrupted.

Local Anesthetics:
Drug Interactions
•
Tricyclic antidepressants
•
Cocaine
•
Beta-adrenergic blocking agents
•
Phenothiazines
•
alpha blocking effect
Thanks