1
Hymenolepis nana
Hymenolepis nana (Von Siebold, 1852) Blanchard, 1891, the dwarf tapeworm, was
discovered by Bilharz, in 1851, in the small intestine of a native boy autopsied in
Cairo, Egypt. Dwarf tapeworm infection in human beings is primarily limited to
children in warm climates.
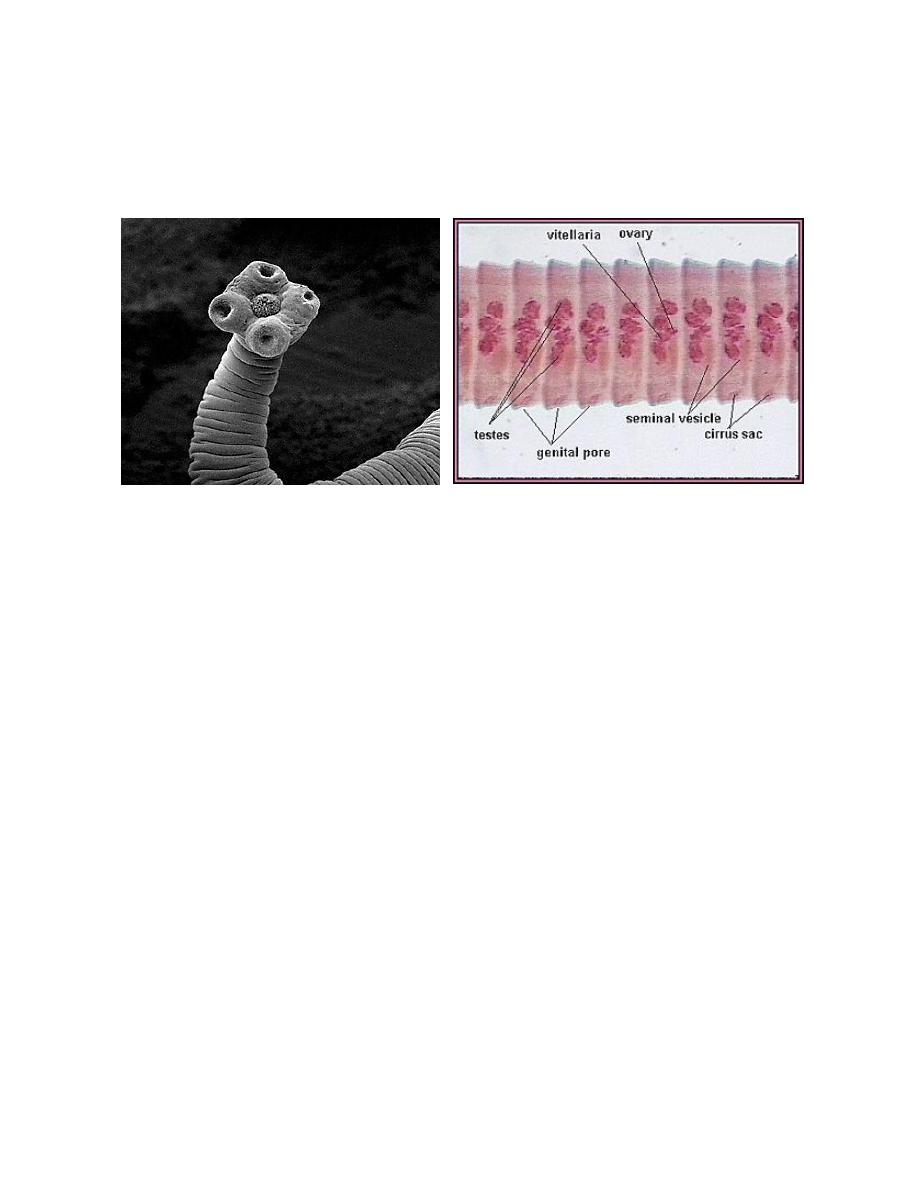
Morphology, Biology and Life Cycle
Hymenolepis nana is the smallest of the tapeworms which parasitize the human
intestine. The entire worm has a length of only 25 to 40 mm and a maximum
breadth not usually exceeding 1 mm. The terminal gravid proglottids usually
disintegrate before separation from the strobila, so that the eggs are thoroughly
mixed with the feces. The average infection consists of a few to several worms, but
thousands have reported from some patients. The eggs of H. nana are grayish
hyaline, nearly spherical, 30 to 47 microns in diameter.
When eggs are swallowed, they hatch in the duodenum where they rapidly
transform into cysticercoid larvae. These then migrate into the duodenal or jejunal
canal, become attached to the mucosa, and in about 2 weeks develop into complete
worms. Thus, both the larval and mature stages are developed in the same
individual. Moreover, in heavy infections it seems entirely probable that
reinfection may occur by internal autoinfection, due to hatching of eggs in the
upper levels of the small bowel.
Certain strains of the murine variety of H. nana can utilize fleas and beetles for
development of the cysticercoid larval stage.
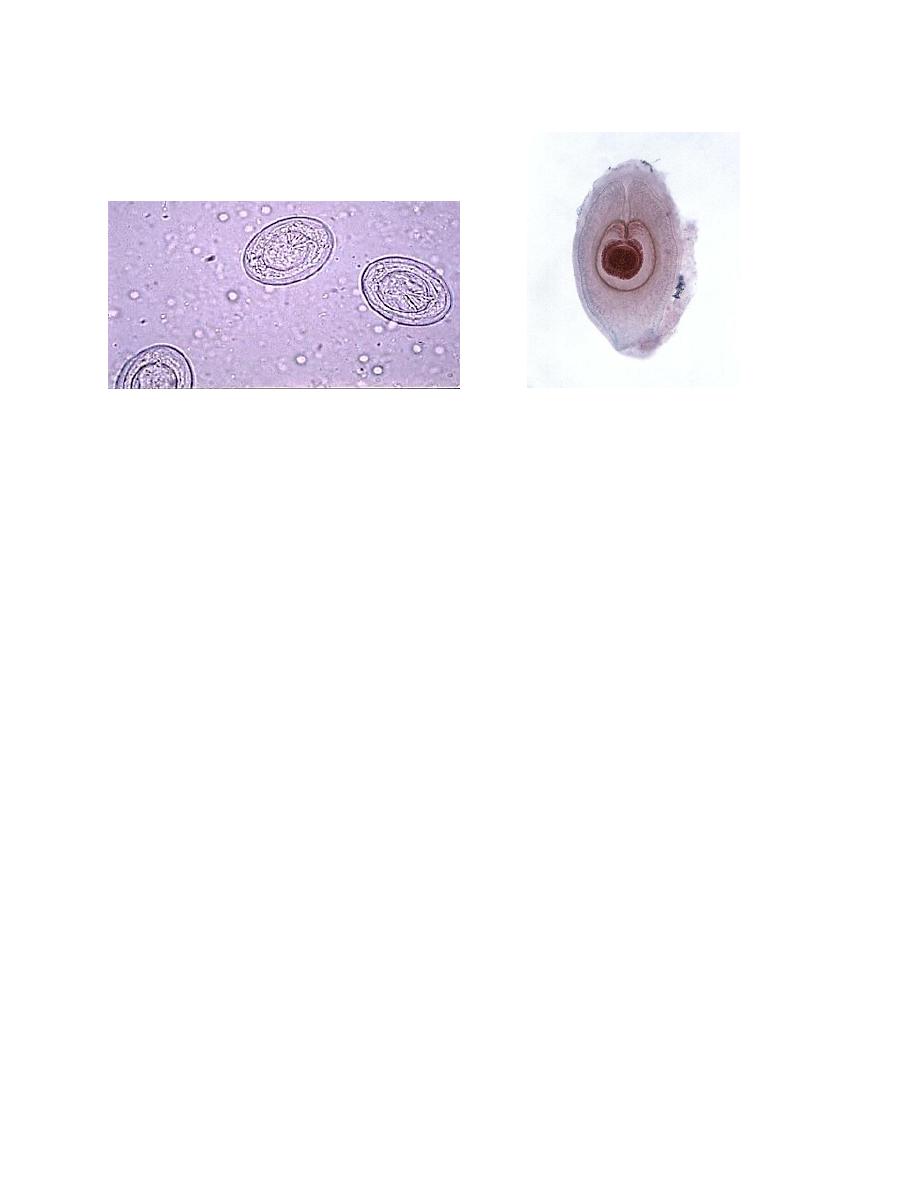
2
Eggs Cycticercoid
Pathogenicity and Symptomatology
Infection with a few Hymenolepis nana may produce no detectable symptoms or it
may be responsible for diarrhea, anorexia, vomiting, insomnia, loss of appetite and
weight, irritability and urticaria. Heavy infection invariably is pathogenic, causing
moderate to profuse diarrheic stools, abdominal pain, anorexia and exaggerated
nervous disorders, or extreme apathy.
Diagnosis and Treatment
Diagnosis is based on recovery of the species characteristic eggs in the stools.
Treatment is available. A prescription drug called praziquantel is given.
Praziquantel, adults and children, 25mg/kg in a single-dose therapy. Sometimes
more than one treatment is necessary.
Epidemiology
H. nana (human strain) requires no extrinsic development and has only a single
host; infection is essentially one of anus-to-mouth transmission. For this reasons
younger children are particularly susceptible subjects. Moreover, although young
children can be infected with H. nana eggs from rodent sources, this type of
infection is probably uncommon. Lack of personal cleanliness and particularly the
soiling of clothing with egg-laden feces provide opportunity for repeated exposure
of the small child and his playmates.
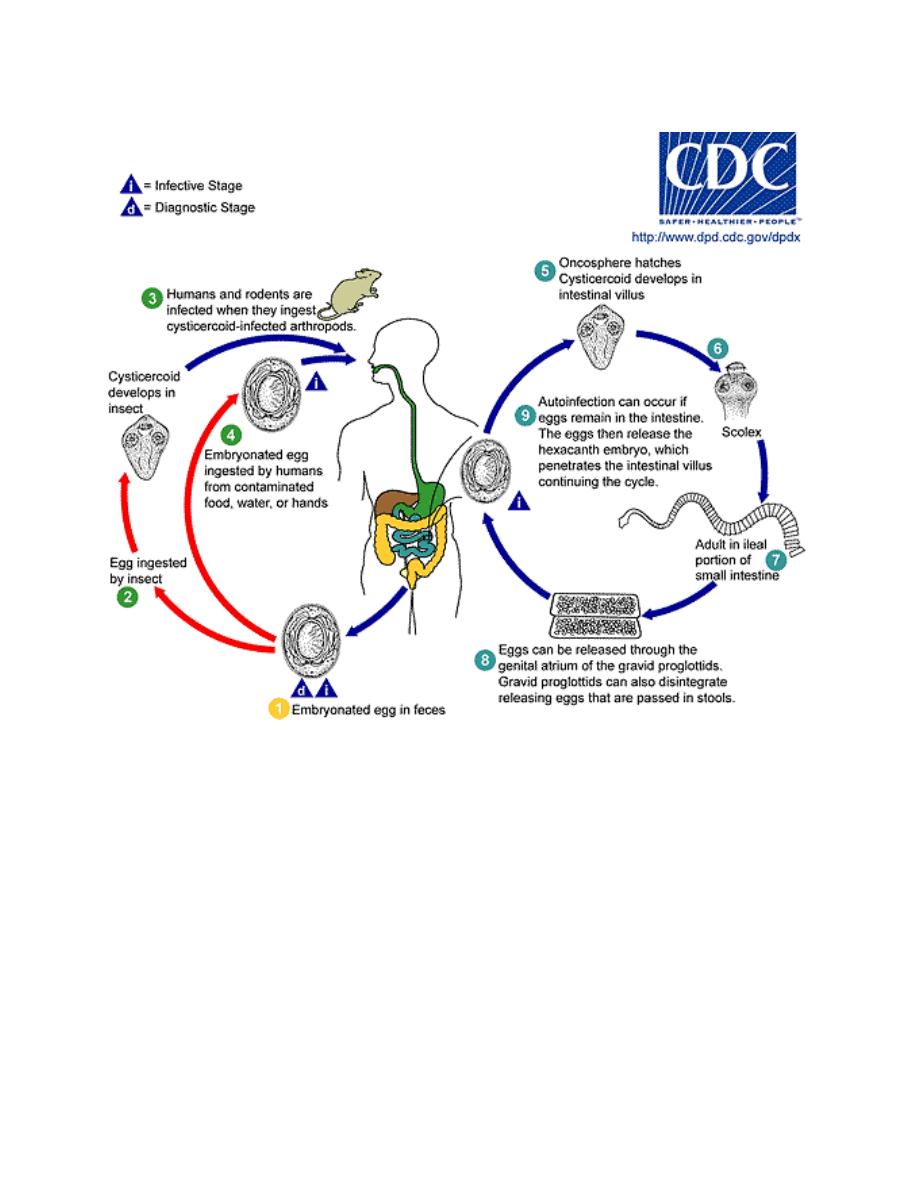
3
Life Cycle of Hymenolepis nana