Pathology of GIT ESOPHAGUS
Sept. 30 2015Prof. Dr Faeza Aftan
Col of Med.
Aliraqia University

ESOPHAGUS
• Congenital Anomalies; atresia & fistula• Diverticula
• mucosal webs (Plummer-Vinson syndrome, Paterson-Brown-Kelly )
• Achalasia
• Laceration (Mallory-Weiss tears,)
• Esophagitis,
• Reflux (GERD)
• Barretts
• Neoplasm
Obstruction
Mechanical;
- atresia, Fistula, duplication.
- Inflammation & scarring.
- tumor
Functional;
- Achalasia, (primary & secondary)
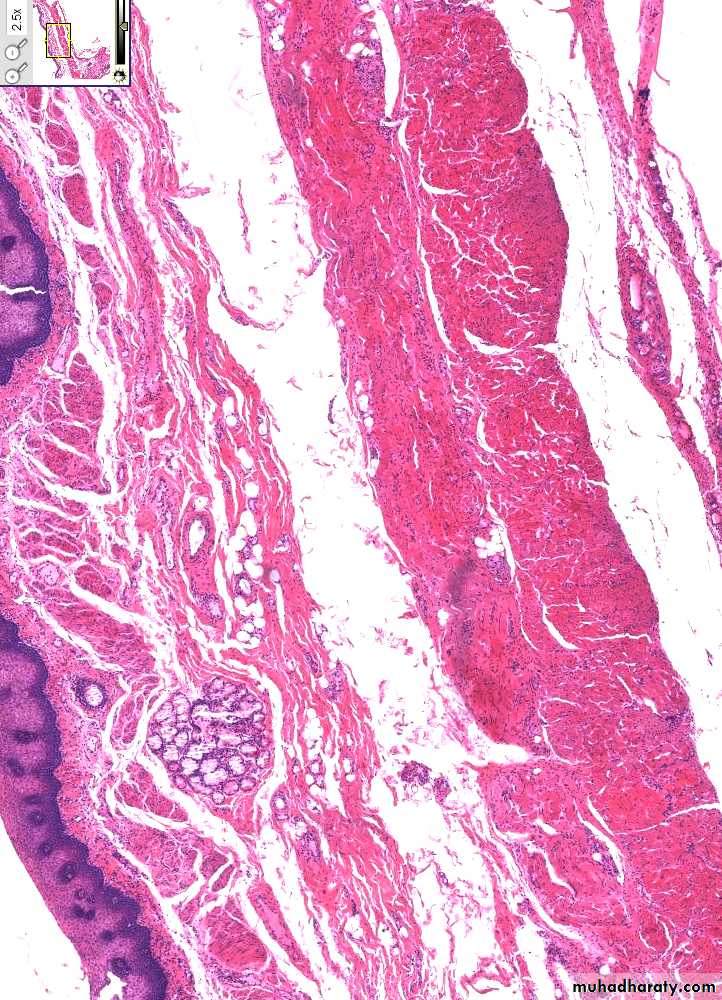
Normal esophageal-gastric junction
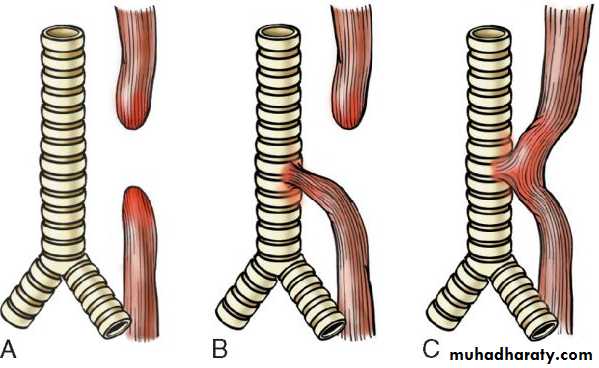
Esophageal atresia and Tracheoesophageal fistula.
A, Blind upper and lower esophageal segments.B, Blind upper segment with fistula between lower segment and trachea.
C, Fistula between patent esophagus and trachea. Type B is the most common.
most common
Mechanical Obstruction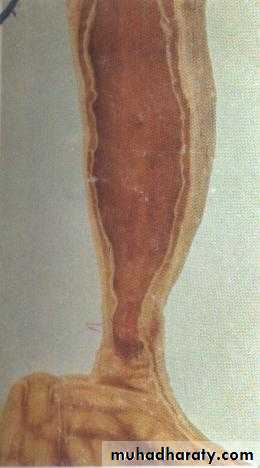
Functional obstruction

• Achalasia
• incomplete LES relaxation,• increased LES tone,
• aperistalsis of the esophagus.
• failure of distal inhibitory neurons.
• 1ry; idiopathic, most common.
• 2ry; cancer, Chagas dis. or fibrosis, amyloidosis, DM
Achalasia
LES are regulated by excitatory (ACH, substance P) & inhibitory (NO, VIP) neurotransmitters.achalasia lack inhibitory subst. The result is a nonrelaxed esophageal sphincter.
Autopsy specimens, on L/M, shown an inflammatory response ( lymphocytes, eosinophils and mast cells), loss of ganglion cells, and neurofibrosis.
Unknown cause.
an autoimmune, hereditary, neurodegenerative, genetic and infections.

DIVERTICULA
• ZENKER (HIGH)• TRACTION (MID)
• EPIPHRENIC (LOW)
• TRUE vs. FALSE?

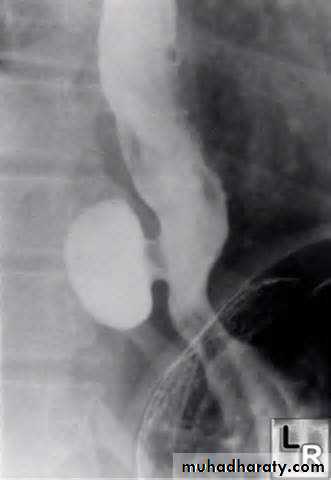
Esophageal diverticulum
Zenker diverticulumTraction
Epiphrenic diverticulum

Dilated portion of stomach protrudes above diaphragm
Common! Usually asymptomatic.
Heartburn, reflux esophagitis
Danger: ulceration, bleeding
Hiatal Hernia
Sliding (L) & rolling (R) hiatal hernias
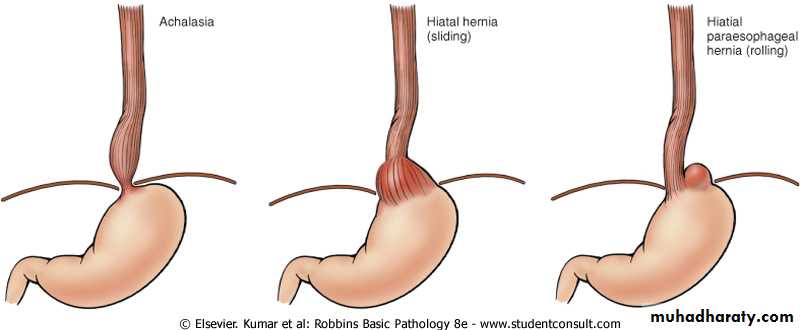
Hiatal hernias
VARICES• THREE common areas of portal/caval anastomoses
• Esophageal
• Umbilical
• Hemorrhoidal
• 100% related to portal hypertension
• Found in 90% of cirrhotics
• MASSIVE, SUDDEN, FATAL hemorrhage is the most feared consequence

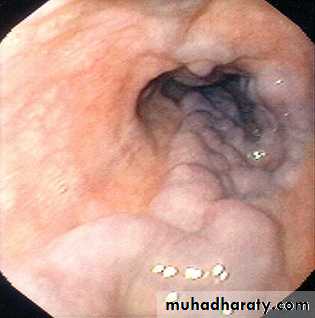
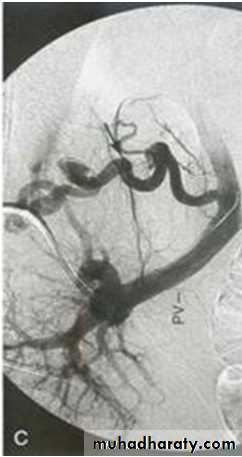
Esophagial Varices
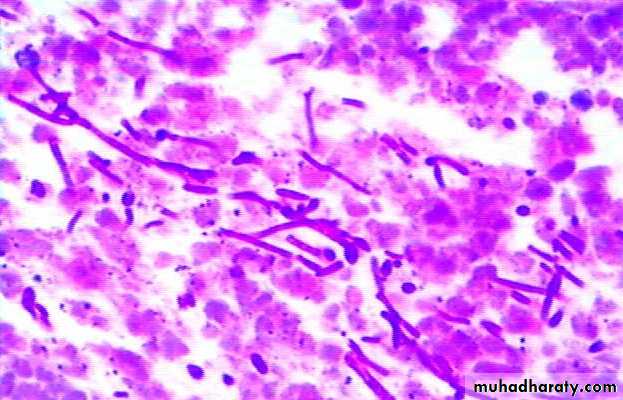
EsophagitisInfective esophagitis
viral, Bacterial, Fungal
Non infective eophagitis
Alcohol, Pills, Acid & alkali, chemotherapy & radiotherapy.
Reflux esophagitis
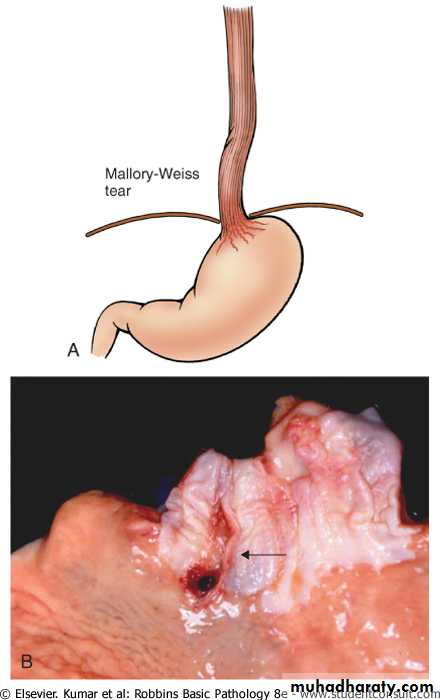
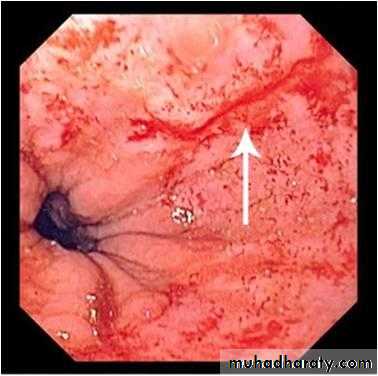
Laceration (Mallory-Weiss tears)
Candida esophagitis

ESOPHAGITIS - Herpes


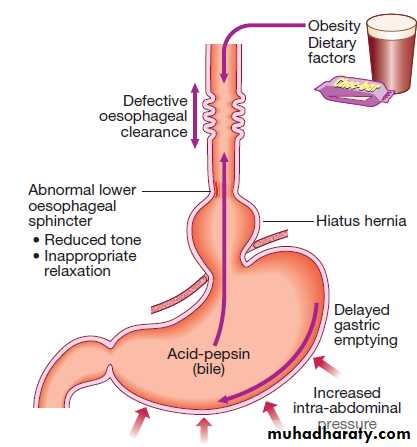

Factors associated with the development of
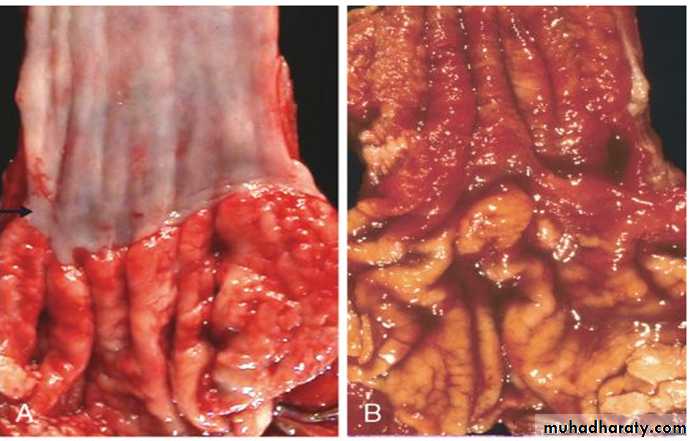
gastro-oesophageal reflux disease.Severe reflux oesophagitis
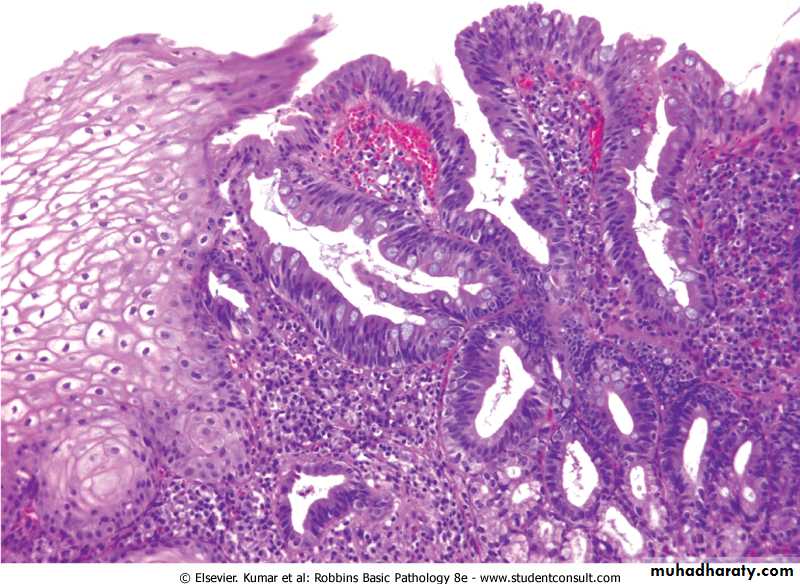
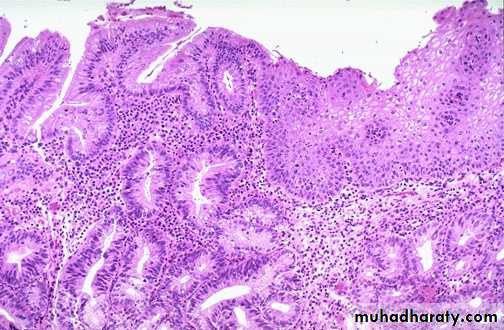
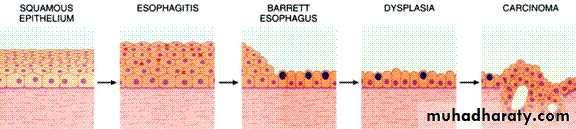
Barrett’s oesophagus
REFLUX/GERD
Barrett esophagus; long segment= >3 cm Vs. short segment< 3 cm is involved
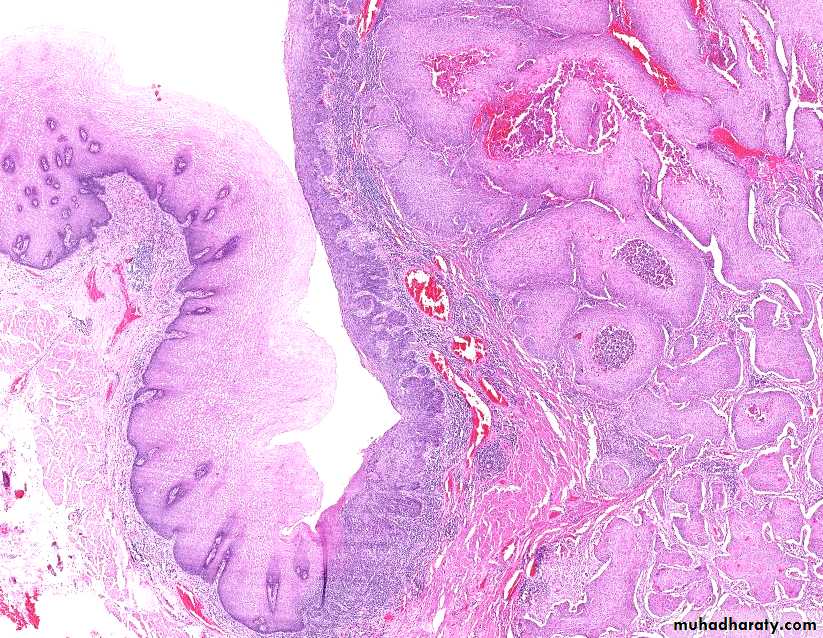
Barrett esophagusReplacement of squamous epithelium by columnar epithelium with goblet cells
Complication of long-standing reflux esophagitisDanger: risk of adenocarcinoma
screen for high-grade dysplasia
Barrett Esophagus
Barrett esophagus
Molecular studies suggest that Barrett epithelium may be more similar to adenocarcinoma than to normal esophageal epithelium, consistent with the view that Barrett esophagus is ???? a pre-malignant condition
LACERATION
• Tears are LONGITUDINAL• Usually secondary to severe VOMITING
• Usually in ALCOHOLICS
• Usually MUCOSAL tears
• By convention, they are all called:
• MALLORY-WEISS
Mallory-Weiss tears
TUMORS
• BENIGN• MALIGNANT
• Squamous cell carcinoma
• Adenocarcinoma

SQUAMOUS CELL CARCINOMA
>45 Yearsmales 4X > females.
underdeveloped areas.
50% occur in the middle 1/3 of esophagus

Tobacco, > 3/4
Alcoholpolycyclic hydrocarbons,
nitrosamines,
fungus-contaminated foods,
HPV
radiation therapy
Very hot beverages
loss of tumor suppressor genes, including p53 and p16.
Other: poverty, caustic esophageal injury, Achalasia,
Plummer-Vinson syndrome, Nutritional deficiencies,



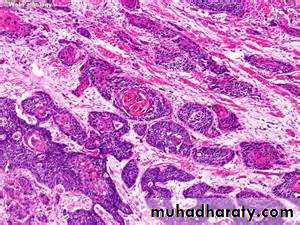
Esophageal Sq cell ca.
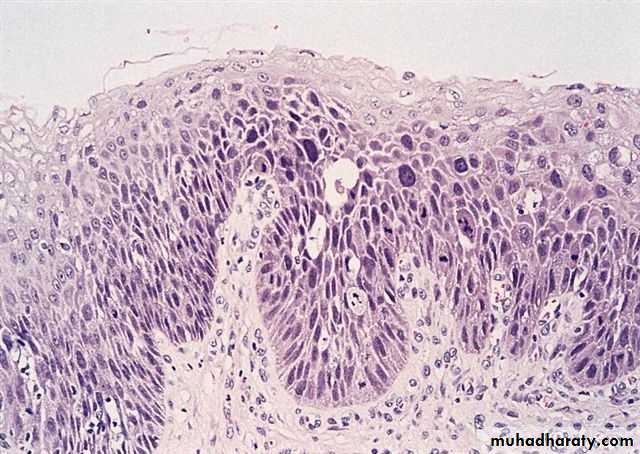
Squamous dysplasia
SQUAMOUS CARCINOMA• DYSPLASIAIN-SITUINFILTRATION
Squamous Cell Carcinoma
Squamous cell carcinomas
The rich submucosal lymphatic network promotes spread, even away from the principal mass.
ca of up 1/3 of esophagus __ cervical LN.
middle 1/3 __ mediastinal, paratracheal, & tracheobronchial LN;
lower 1/3 spread to gastric and celiac LN.
ADENOCARCINOMA
• BARRETT’s• BARRETT’s
• BARRETT’s
• BARRETT’s
• BARRETT’s
• BARRETT’s
• BARRETT’s
• Obesity
• Tobacco & alcohol
• H. pylori
• Female hormones
ADENOCARCINOMA
Progression of Barrett esophagus to adenocarcinoma occurs through genetic and epigenetic changes. accumulate mutations.
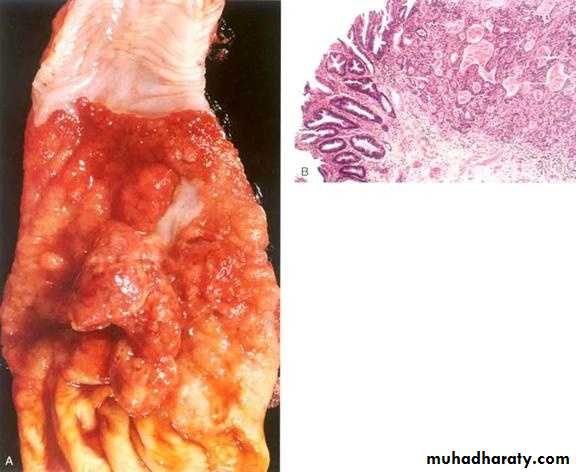
ADENOCARCINOMA

Esophageal adenoca. Sq cell ca.
AdenocarcinomaCommonest type in US
Risk factor: Barrett esophagus
Distal 1/3 of esophagus
Symptoms: late obstruction
• Squamous cell carcinoma
• Commonest type worldwide
• Risk factors: smoking, alcohol, genetics, esophagitis.
• Middle 1/3 of esophagus
• Symptoms: insidious onset; late obstruction
Esophageal Carcinoma
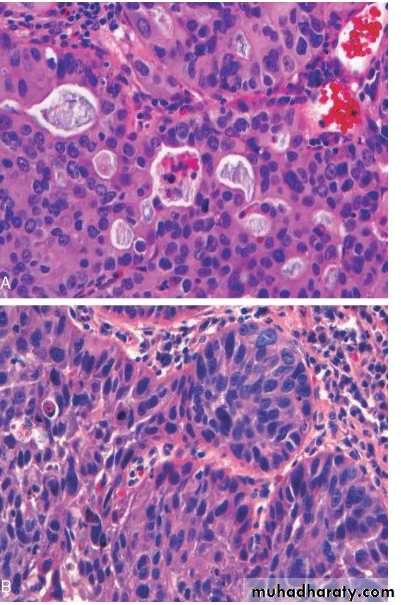
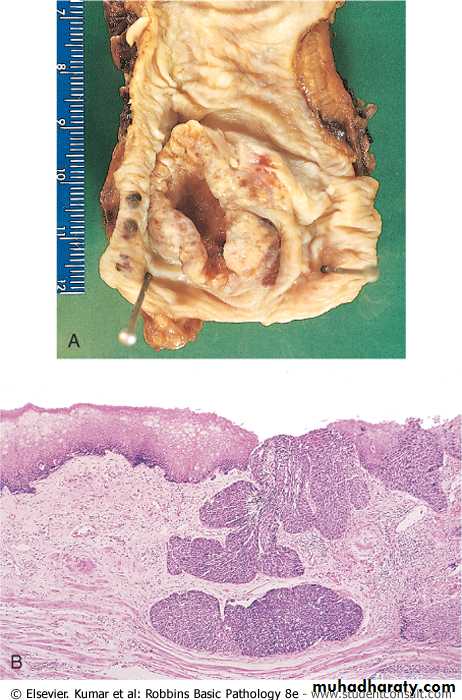
Esophageal cancer.
A, adenocaB, Sq cell ca.
BENIGN TUMORS• LEIOMYOMAS
• POLYPS
• CONDYLOMAS (HPV)
• LIPOMAS