
Malignant Lymphomas ( NHLs) pathology
Malignant lymphomas (Non-Hodgkin's lymphomas-NHLs)
Malignancies of the lymphoid system which primarily manifest themselves outside the
bone marrow, at the sites of normal lymphoid homing
• Lymph nodes
• Spleen
• M.A.L.T .
• Anywhere
(Lymphomas outside lymph nodes and spleen are referred to as extranodal
lymphomas)
Clinical presentation
• Enlarging mass(es), typically painless, at sites of nodal tissue
• Compression ,infiltration of hollow organs
• Pain ,obstruction, perforation
• Interference with normal organ function -
• Solid organ infiltration- kidneys, liver, bone marrow
• Systemic symptoms
• Fever
• Night sweats
• Weight loss
• If marrow infiltrated, can have leukemic component
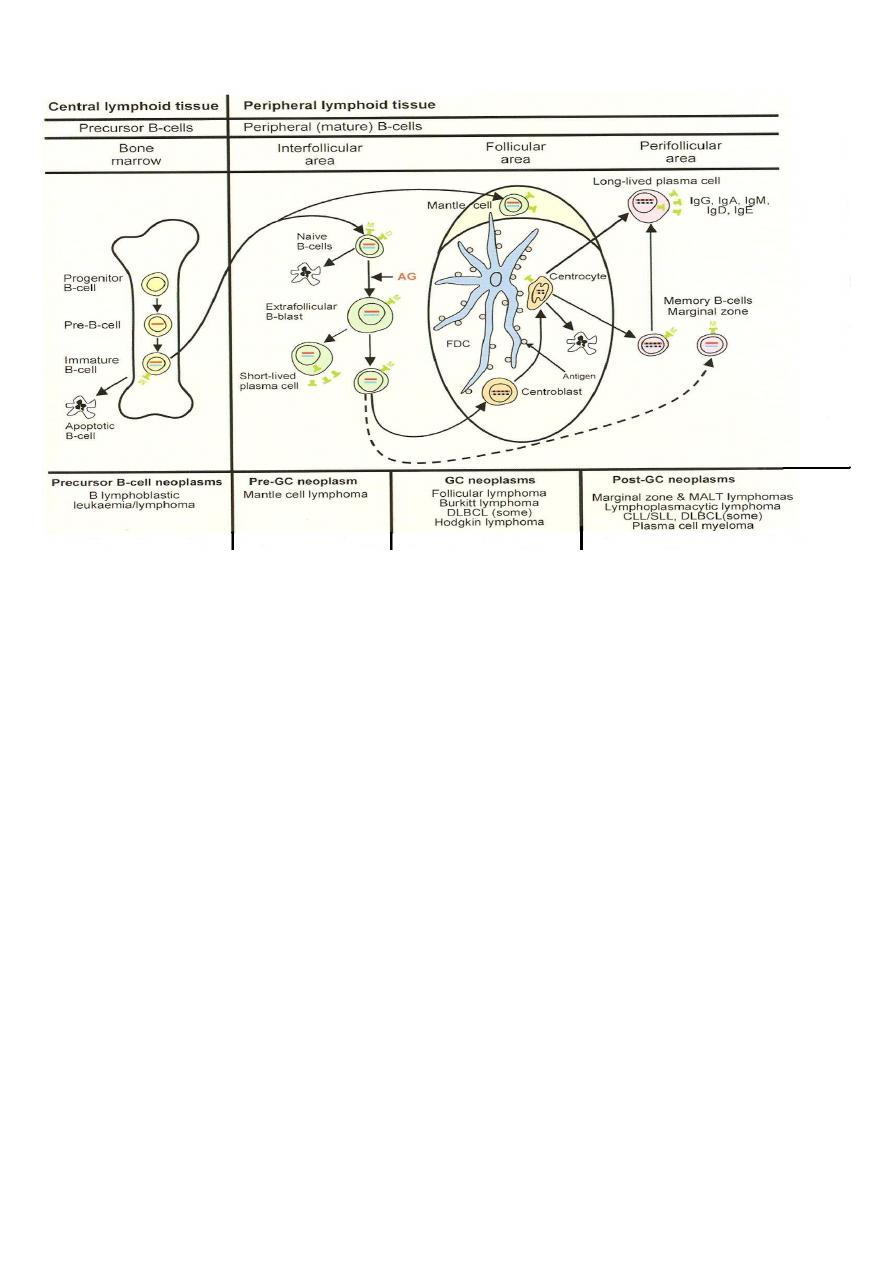
REAL/WHO classification- backbone
• B cell neoplasms
• Precursor B cells-related to acute leukemia
• Peripheral B cell lymphomas- the majority of B cell lymphomas
• T cell and Natural Killer cell neoplasms
• Precursor T cells
• Peripheral T cell and NK neoplasms
• Hodgkin’s lymphoma
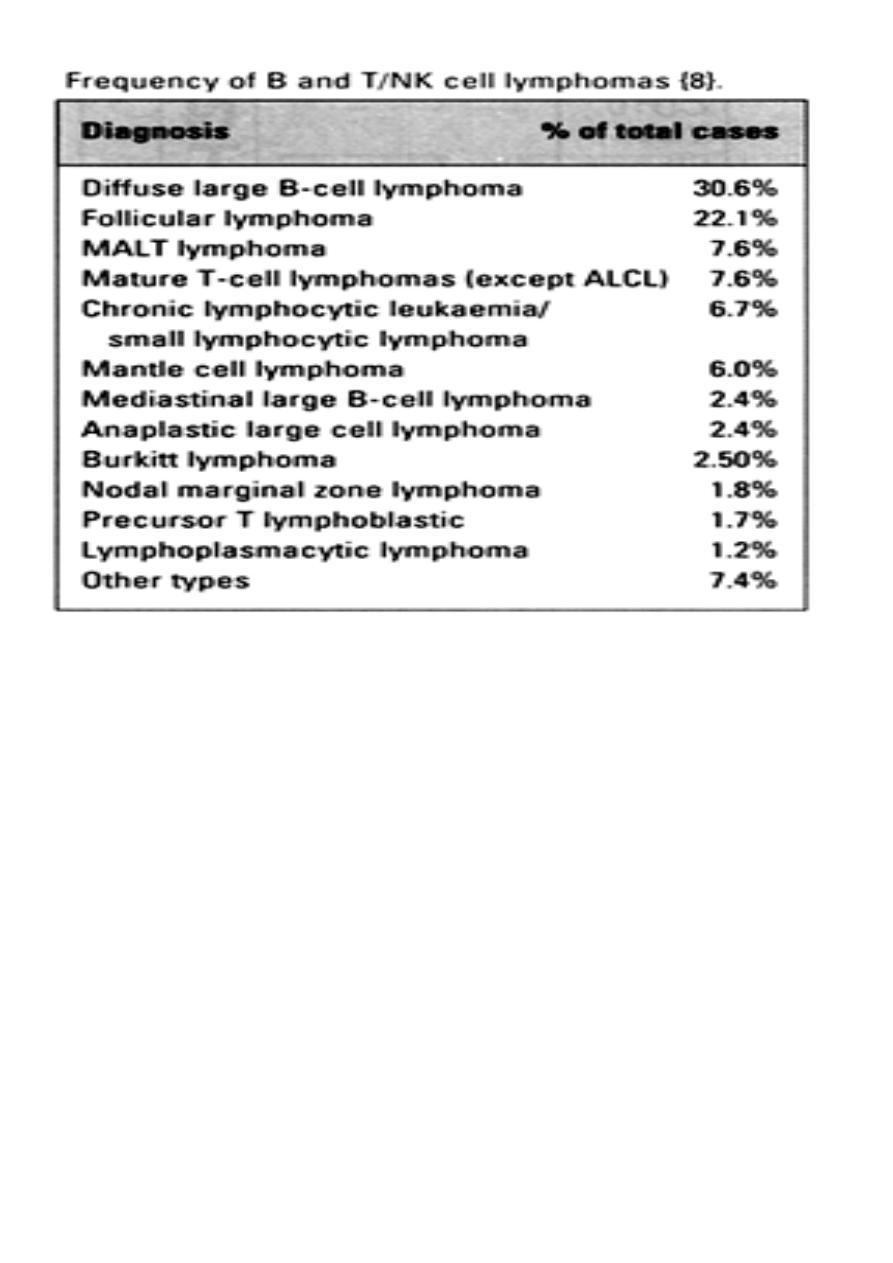
Frequency of lymphomas
Example Indolent Lymphoma :
Follicular lymphoma .
Clinical
• Most common type of indolent lymphoma in US; second most common type lymphoma
overall
• Disease of adults >40 (median age 59)
• Usually widely disseminated at diagnosis, incl. bone marrow
• Will respond to “gentle chemotherapy” but will relapse
• Overall 5 yr survival 72%
• Over time, additional mutations --> progression (“transformation”) to large cell
lymphoma --> aggressive clinical course
• Although Gr.1 is most common presentation, some patients present with predominance
of large cells within follicles -->more aggressive clinical course
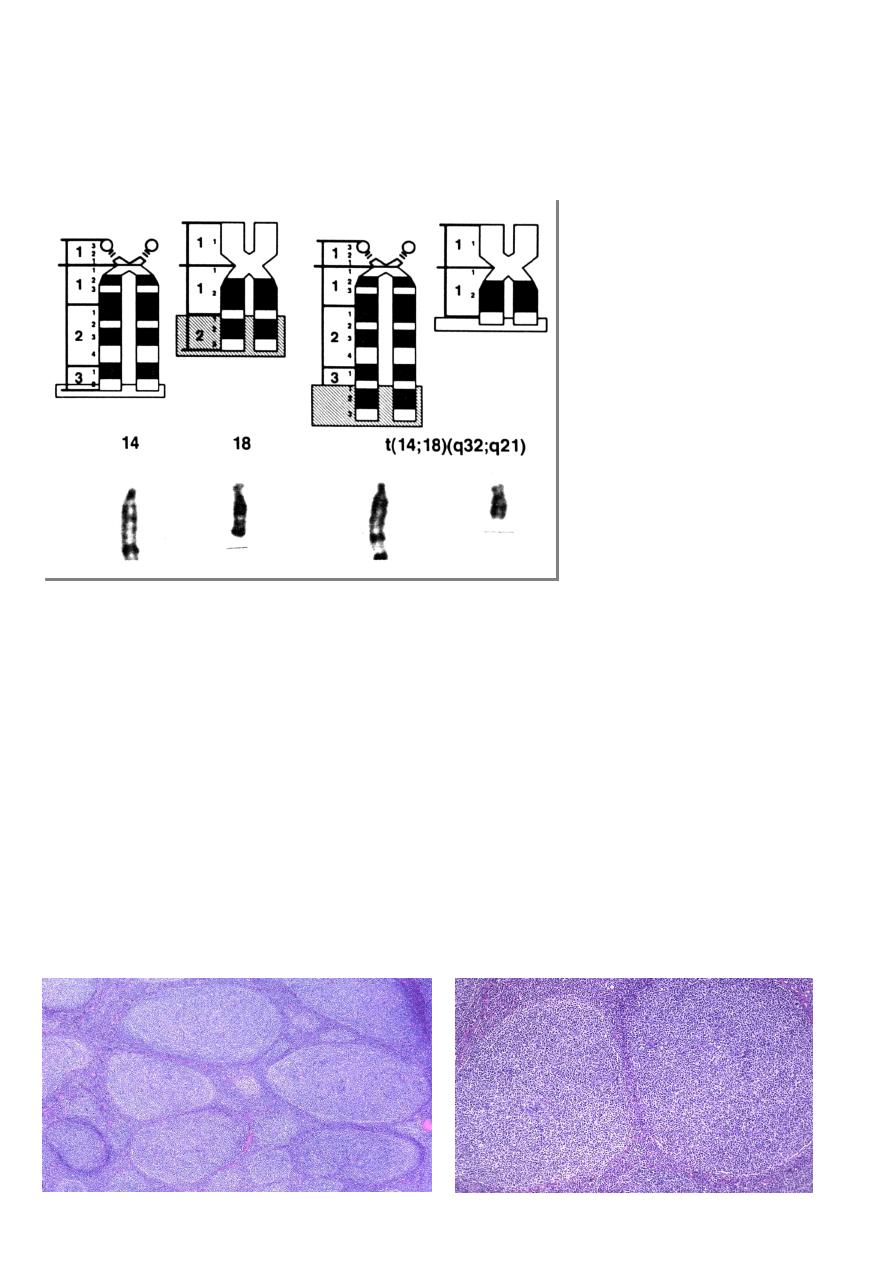
Pathogenesis :
• Due to t(14;18)(q32, q21)
• Upregulates expression of an anti-apoptotic protein Bcl2
Follicular lymphoma
Epidemiology :
• FL accounts for about 20% of all lymphomas
• Highest incidence in USA and Western Europe
• Median age 6th decade .
• rarely occurs < 20
• M/F = 1/1.7
• Paediatric cases predominantly males
Sites of involvement:
• Predominantly LN, but also BM, Spleen, Peripheral blood, GIT, soft tissue, Skin
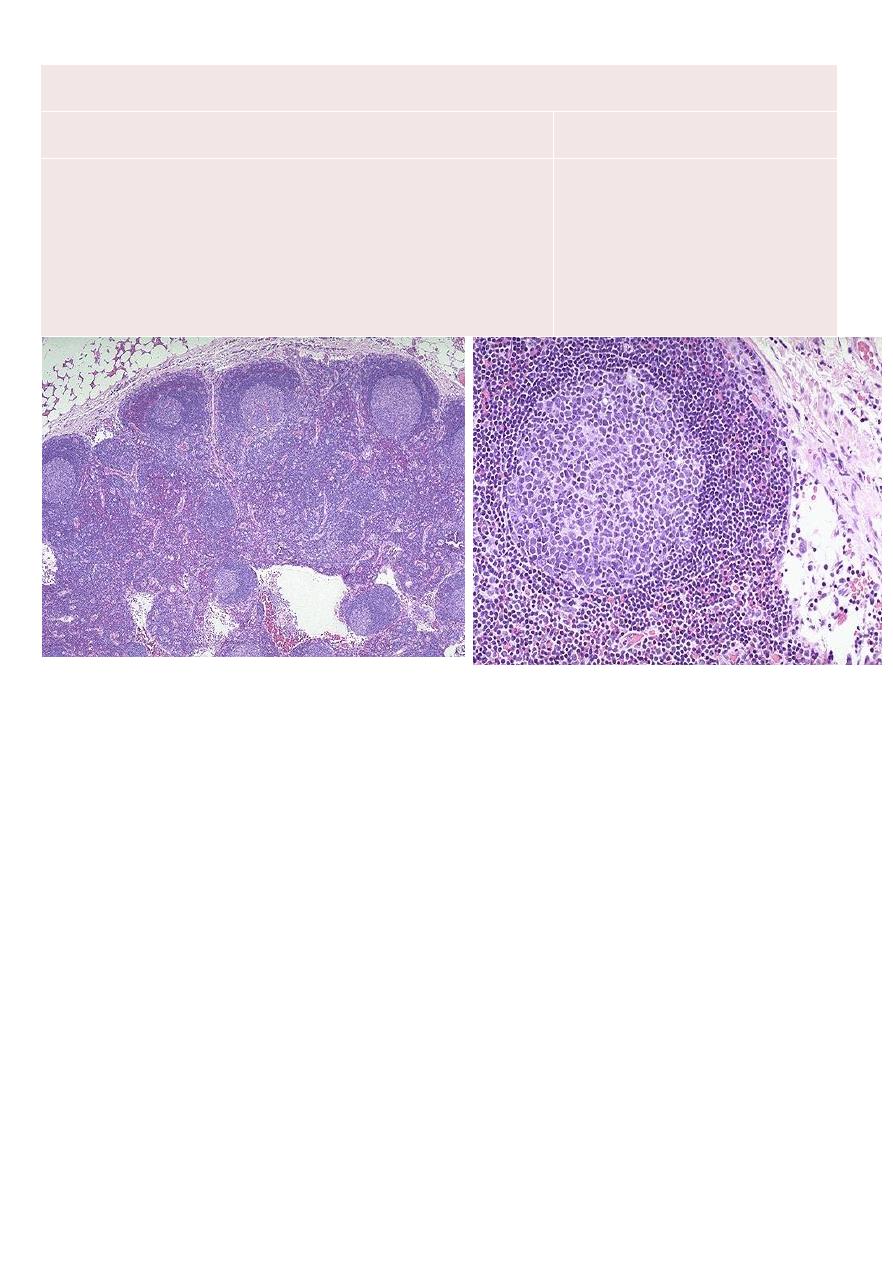
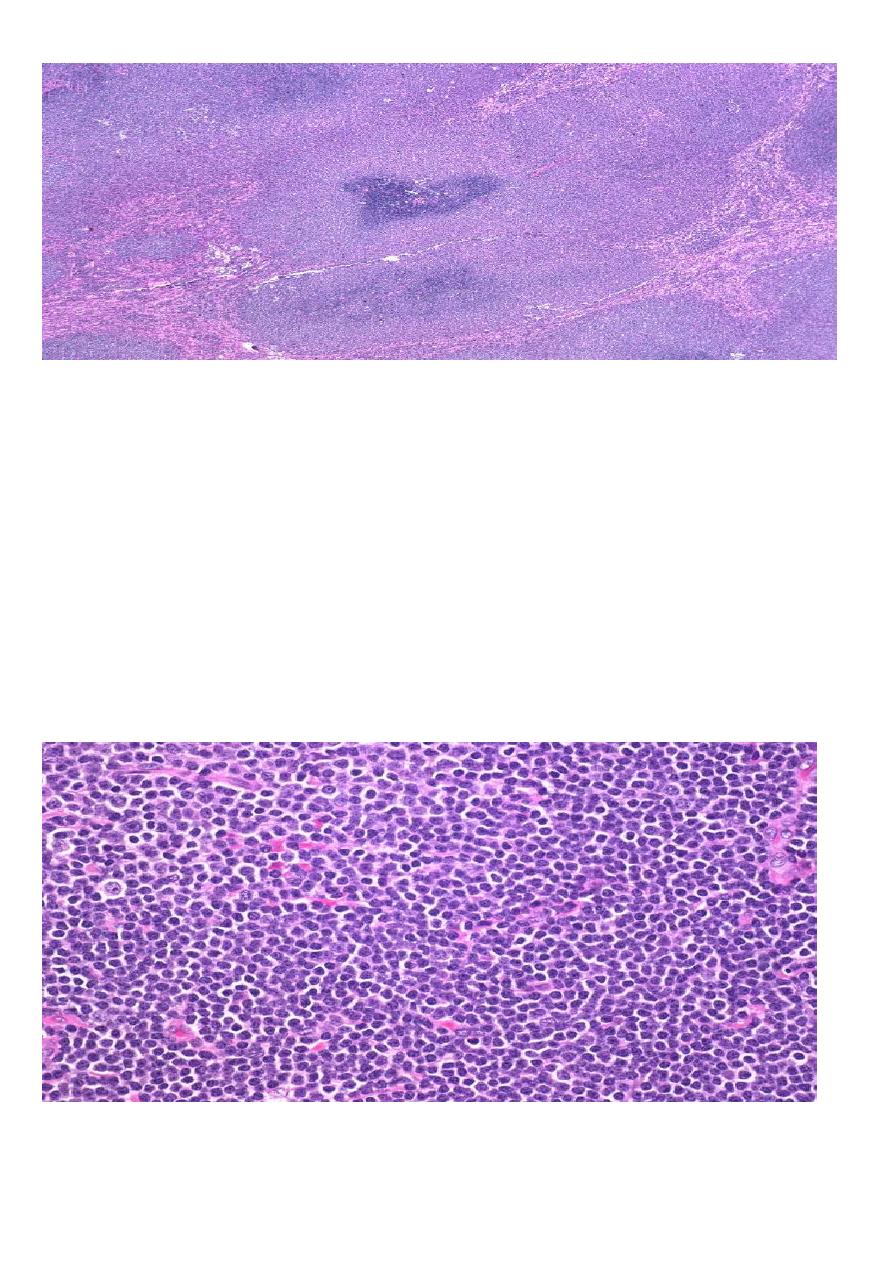
Follicular lymphoma .
Follicular lymphoma or Reactive hyperplasia
Low Power (Architectural)
Benign
Malignant
1. Loosely packed follicles
2. Polymorphic follicles
3. Prominent mantle zones
4. Polarized follicles
5. Preserved open sinuses
6. No capsular invasion or transgression
7. Polyclonal light chain expression
8. Non-reactive for BCL-2
1. Tightly packed follicles
2. Monomorphic follicles
3. Absent or obscured mantle
zones
4. Unpolarized follicles
5. Destroyed and constricted
sinuses
6. Extension into perinodal soft
tissue
7. Monoclonal light chain
expression
8. Reactive for BCL-2
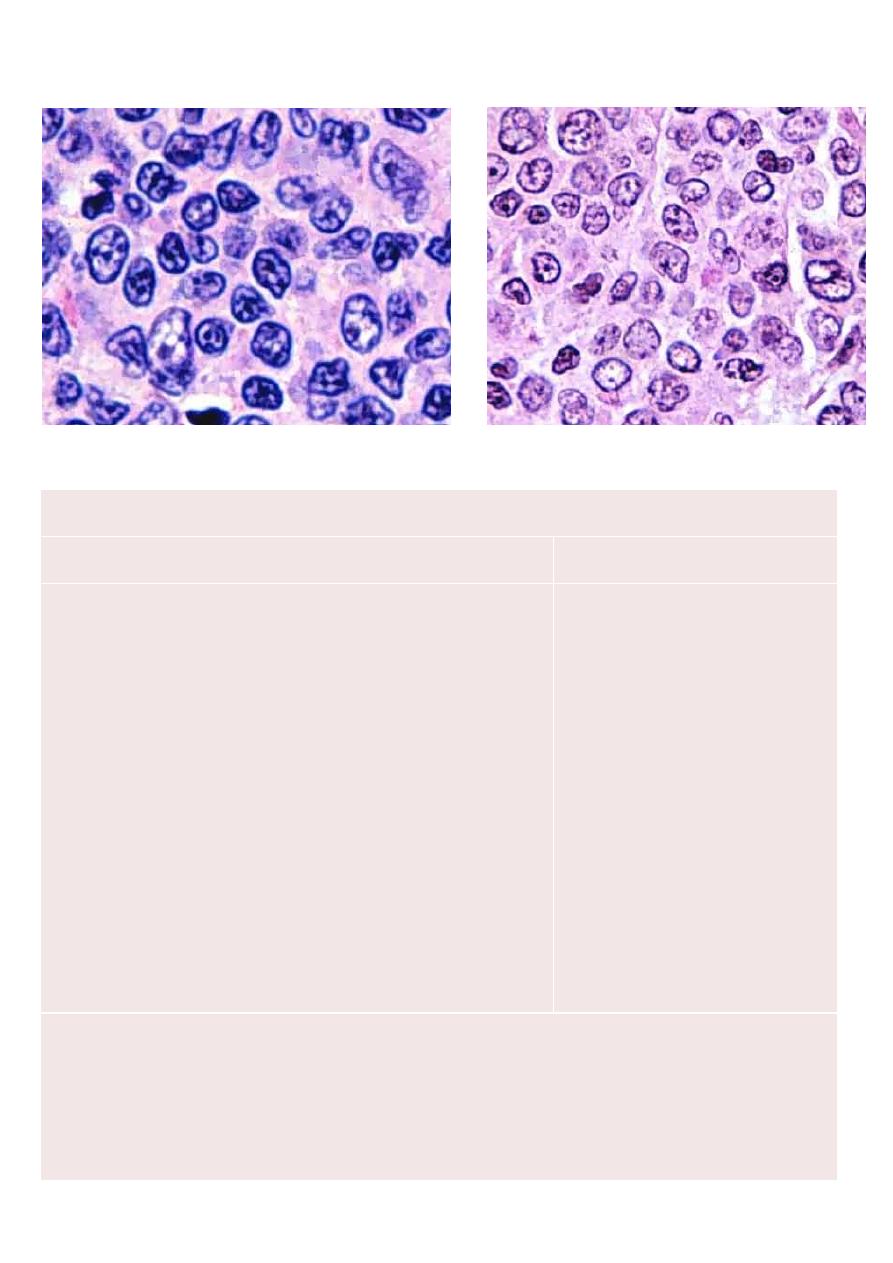
High Power (Cytological)
Benign
Malignant
1. A very high mitotic rate
2. Tingible-body macrophages
3. Between follicles are the usual paracortical lymphoid cells
1. A lower mitotic rate
2. No Tingible-body
macrophages
3. Between follicles atypical
cleaved cells may be found
Examples: aggressive B cell lymphoma-Diffuse large B cell lymphoma
• Clinical
• Most common lymphoma- 30% NHL
• Disease of adults and children, but median age 64
• Limited versus widespread disease
~ 1:1
• Presents with rapidly enlarging masses
• Approximately 40% curable with aggressive chemotherapy/ stem cell transplant
• Pathogenesis
• Not as clearly defined as previous examples- several cytogenetic abnormalities
associated with large cell lymphoma, but no defining one
Diffuse Large B cell lymphoma
• Pathology
• Benign equivalent- large replicating B cells of germinal center and paracortex
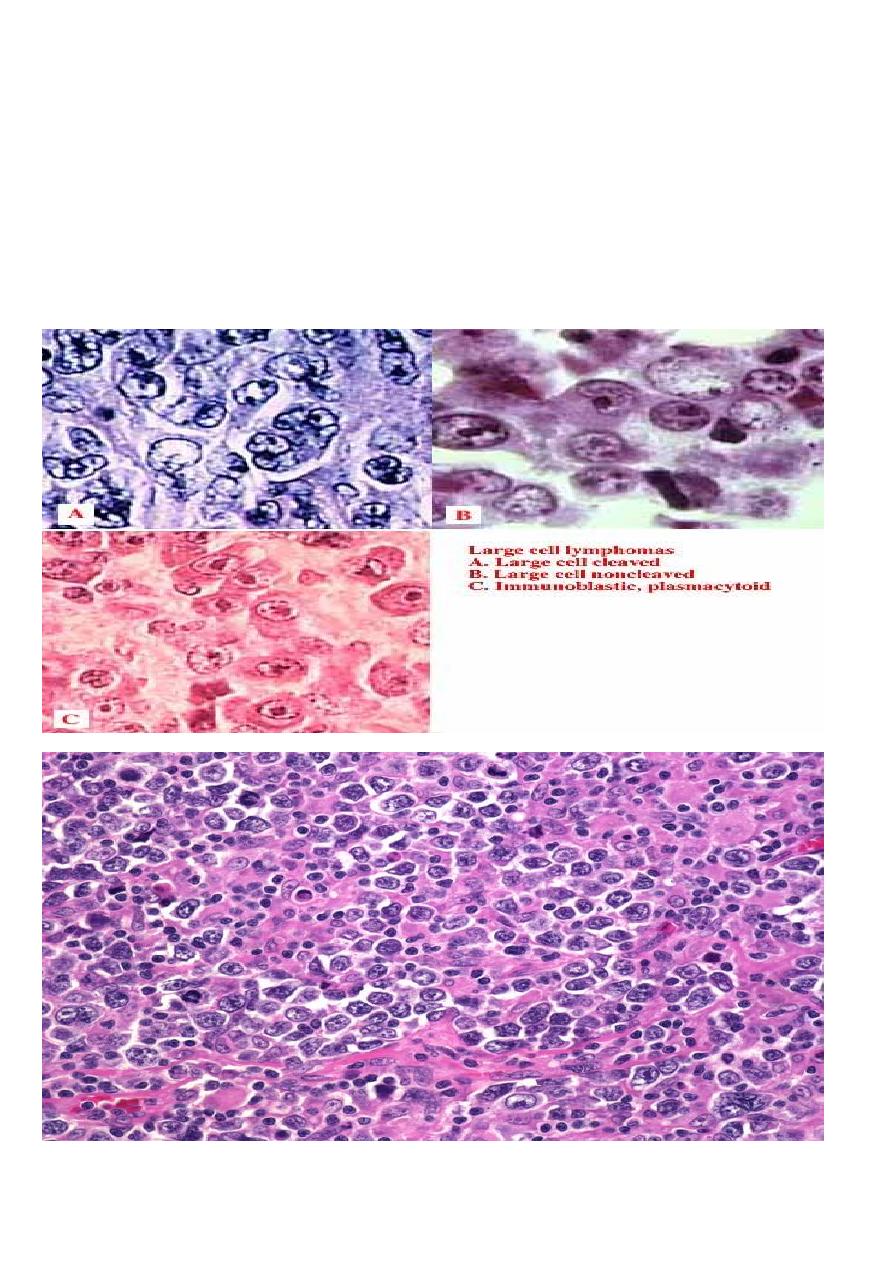
• Diffuse infiltration of lymph node
• Often necrosis; increased mitotic rate
• Cytology: Oval or cleaved nucleus with vesicular chromatin and 1-3 nucleolus
• Nucleus larger than that of reactive macrophage
• Several cytologic subtypes initially felt to have differing clinical behavior .
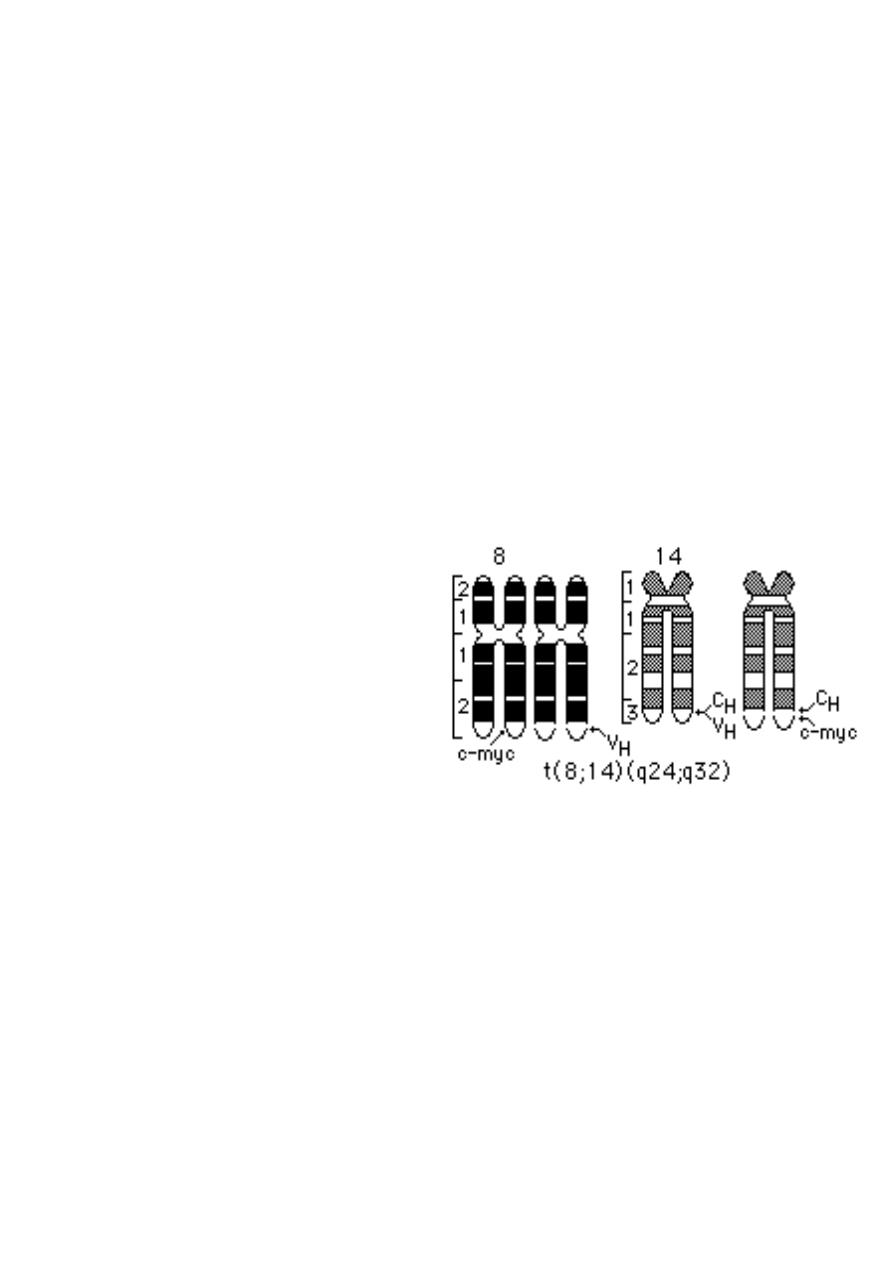
Burkitt's lymphoma
• Clinical
• 3% lymphomas
• Disease of adults and children -
median age 31
• Initially recognized in Africa by Thomas Burkitt
• Association with Epstein Barr virus infection
• Localization in jaw
• In US, usually presents in ileocecal region of children
• 1/3 of all childhood lymphomas
• Earlier, very aggressive and rapidly fatal
• Now, ~70-80% children
curable
• 40%of adults
• Pathogenesis :
• t(8;14), producing upregulation
of myc oncogene, a cell cycle
regulation gene
Burkitt's lymphoma
• Pathology
• Benign equivalent is replicating small noncleaved cell of germinal center:
• Diffuse infiltration of lymph node
• Very high mitotic rate,
• Attracts macrophages to phagocytize> starry sky pattern at low power
• Cytology: round nucleus, smaller than that of reactive macrophage
• Vesicular chromatin and 2-5 nucleoli
• Immunophenotype:
• Positive: Monoclonal light chain, CD19, CD10
• Negative: CD5
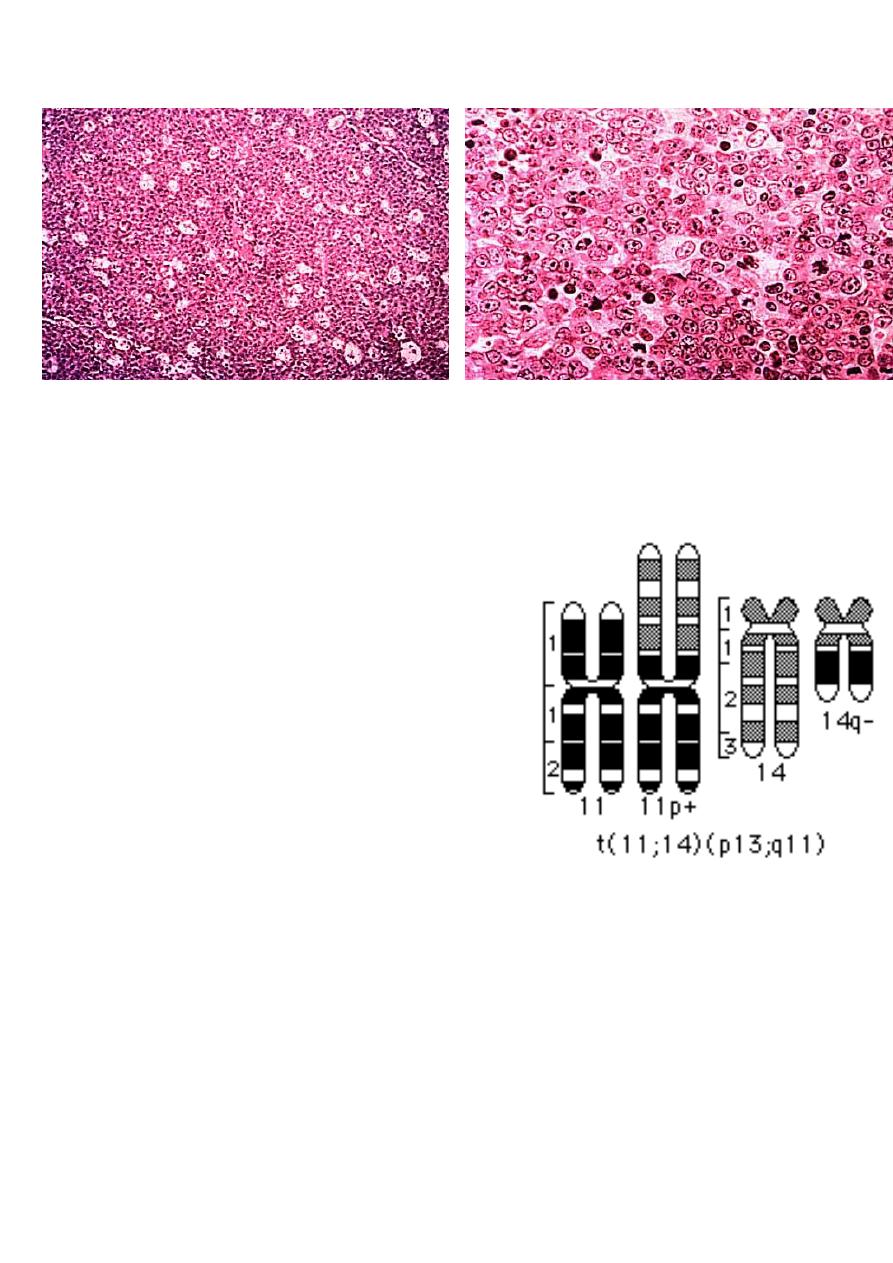
Mantle cell lymphoma
Clinical
• 6% lymphomas
• Disease of adults (median age 63)
• Usually widely disseminated
• Poor response to all attempted therapies ,
• ?curable with transplant
• 5yr survival 27%
Pathogenesis
• Due to t(11:14)
• Upregulates Bcl1 (cyclin D1), a cell cycle
regulator
•
Mantle Cell Lymphoma
• MCL accounts for 3-10% of NHL
• Middle age – older patients
• Male > Female
• LN +/- Spleen, BM, Peripheral blood
• Extranodal sites : GIT and Waldeyer’s ring
• Prognosis poor, median survival 3-4 years
• Genetic hallmark: t(11;14)(q13:q32) CCND1/1GH translocation -> Cyclin D1 over-
expression
• CD20,CD19, CD79a, PAX5 , CD5 & Cyclin D1 positive
• CD23 negative
CLL/SLL
• Most common leukaemia in adults in the western world
• 6.7% of all NHL biopsies
• Indolent Clinical course
• Generalised lymhadenopathy + leukaemic phase
• Diffuse growth of small lymphocytes with prolymphocytes and paraimminoblasts in
Proliferation Centres
• Trisomy 12 (33%), 13q (25%)
• Transformation to large cell lymphoma in 5% of cases
• Positive for PAX5, CD22, CD19, CD20, CD5, CD23 and CD79a
• Cyclin D1 negative
Peripheral T cell lymphomas
• Predominantly leukemic/disseminated

• T-cell prolymphocytic leukemia
• T-cell large granular lymphocytic (LGL) leukemia
• NK cell leukemia
• Adult T-cell leukemia/lymphoma
• Predominantly nodal
• Angioimmunoblastic T-cell lymphoma
• Peripheral T-cell lymphoma unspecified
• Anaplastic large cell lymphoma ,T/null-cell
• Predominantly extranodal
• Mycosis fungoides
• Sezary syndrome
• Primary cutaneous CD30+ T-cell lymphoproliferative disorders
• Subcutaneous panniculitis-like T-cell lymphoma
• NK/T cell lymphoma, nasal and nasal-type
• Enteropathy-type intestinal T-cell lymphoma
• Hepatosplenic T-cell lymphoma
Key points regarding T cell lymphomas
• Clinical
• Represent 20% all lymphomas
• More often extranodal than B
• Can involve skin, midline facial area, liver
• Very characteristic clinical presentations
• Most diseases bad: high stage, and poorer response to therapy than B cell
lymphomas of all grades
• Pathogenesis :
• Characteristic cytogenetic findings associated with several types

• Anaplastic large cell lymphoma -
t(2:5):ALK1 gene
• Hepatosplenic T cell lymphoma -
Isochromosome 7
• Pathology
• Cytologic features not as predictive of behavior as B cell lymphomas
• Anaplastic large cell lymphoma
-- →better prognosis than most indolent B
cell lymphomas- 77% 5 year survival
• Mycosis fungoides, indolent cutaneous lymphoma, incurable, but with long
clinical course
• Immunophenotypic studies frequently demonstrate
• Loss of normal T cell associated antigens
• Antigens associated with Natural Killer cell function
• Immunology absolutely necessary to recognize
Clinical presentation
• Enlarging mass(es), typically painless, at sites of nodal tissue
• Obstruction ,ulceration of hollow organs- pain, perforation
• Interference with normal organ function -
• Solid organ infiltration- kidneys, liver, bone marrow
• Systemic symptoms
• Fever
• Night sweats
• Weight loss
• If marrow infiltrated, can have leukemic component
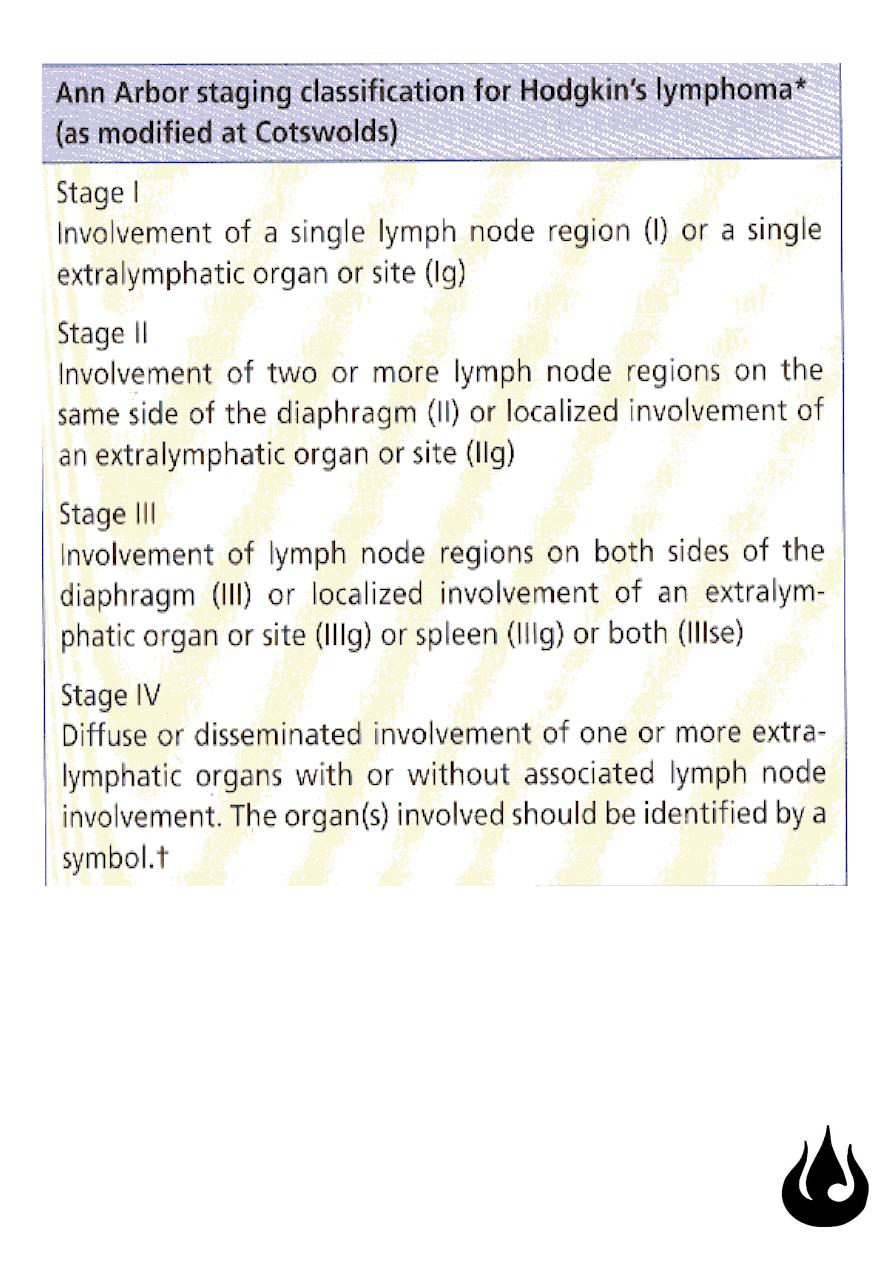
Clinical staging of lymphomas
• Defines extent of disease; determines therapy and prognosis
• Based on physical, radiologic examination, bone marrow biopsy and aspiration
• Ann Arbor Staging system
• B symptoms- fever, weight loss >10% body weight, night sweats
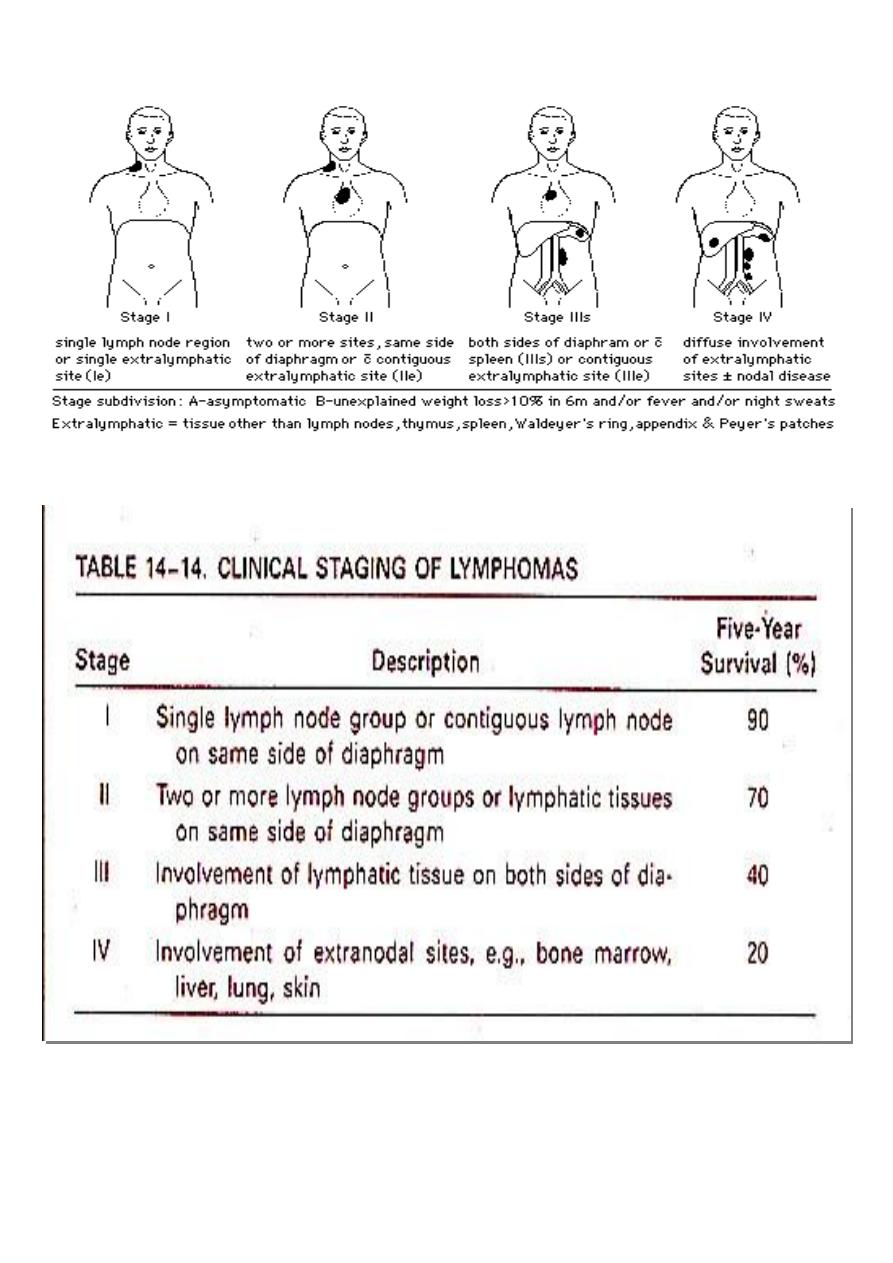
Staging table
"Fake it till you make it"