SYSTEMIC HYPERTENSION AND
ANTIHYPERTENSIVE DRUGS
Dr. Hussain Addai Aljabery
M.B.Ch.B. M.Sc. ( Pharma.)
D.M.R.D. F.I.B.M.C ( Radiology)

Hypertension:
■ Hypertension is a very common disorder, particularly past middle age. It is not a
disease in itself, but is an important risk factor for cardiovascular mortality and
morbidity.
■ INCIDENCE
• Elevated blood pressure is a common disorder, affecting approximately 30% of adults
in the United States.
• Although many patients have no symptoms, chronic hypertension can lead to heart
disease and stroke, the top two causes of death in the world.
• Hypertension is also an important risk factor in the development of chronic kidney
disease and heart failure.

Basic inform ation
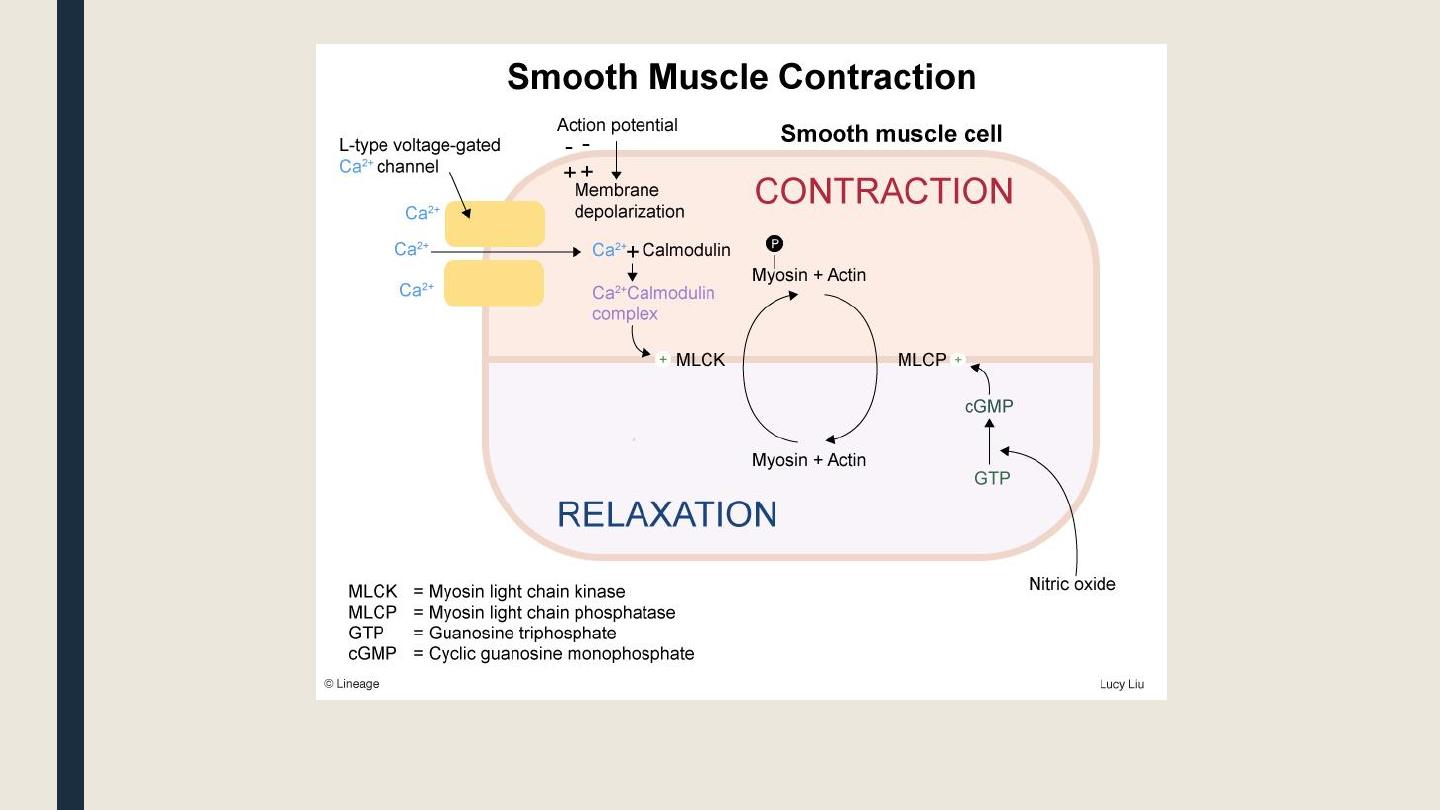
Vascular smooth muscle contraction and relaxation
Vasoconstriction
is initiated by opening of voltage gated L-type
Ca2+ channels in the membrane of vascular smooth muscle
cells. Increase d intracellular Ca2+ triggers the phosphorylation of
myosin light chain kinase
which initiates contraction.
Vasodilation
is initiated by either:
§ Activation of guanylyl cyclase → ↑cGMP → dephosphorylation of
myosin
light chain kinase
smooth m.s relaxation.
§ Opening of K+ channels in the vascular smooth muscle cell mem
sm
o
oth ms stabilization (hyperpolarization) → relaxation.
▌
The vascular endothelium and local vasomotor control
■ Beside the neural control of blood vessels through the sympathetic and
parasympathetic systems, the vascular endothelium produces various compounds
that help controlling the vascular tone:
Nitric oxide
(NO; or EDRF)
It is a diffusible gas with very short half-life. It causes VD by
increase in intracellular cGMP . It protects against
atherosclerosis, high blood pressure, heart failure and thrombosis.
PGI2
It is synergistic to NO. It causes VD via specific receptors
Endothelin
Is a 21- amino-acid peptide. By its action on ET
A
receptors, it
causes severe VC and vascular smooth muscle hypertrophy.
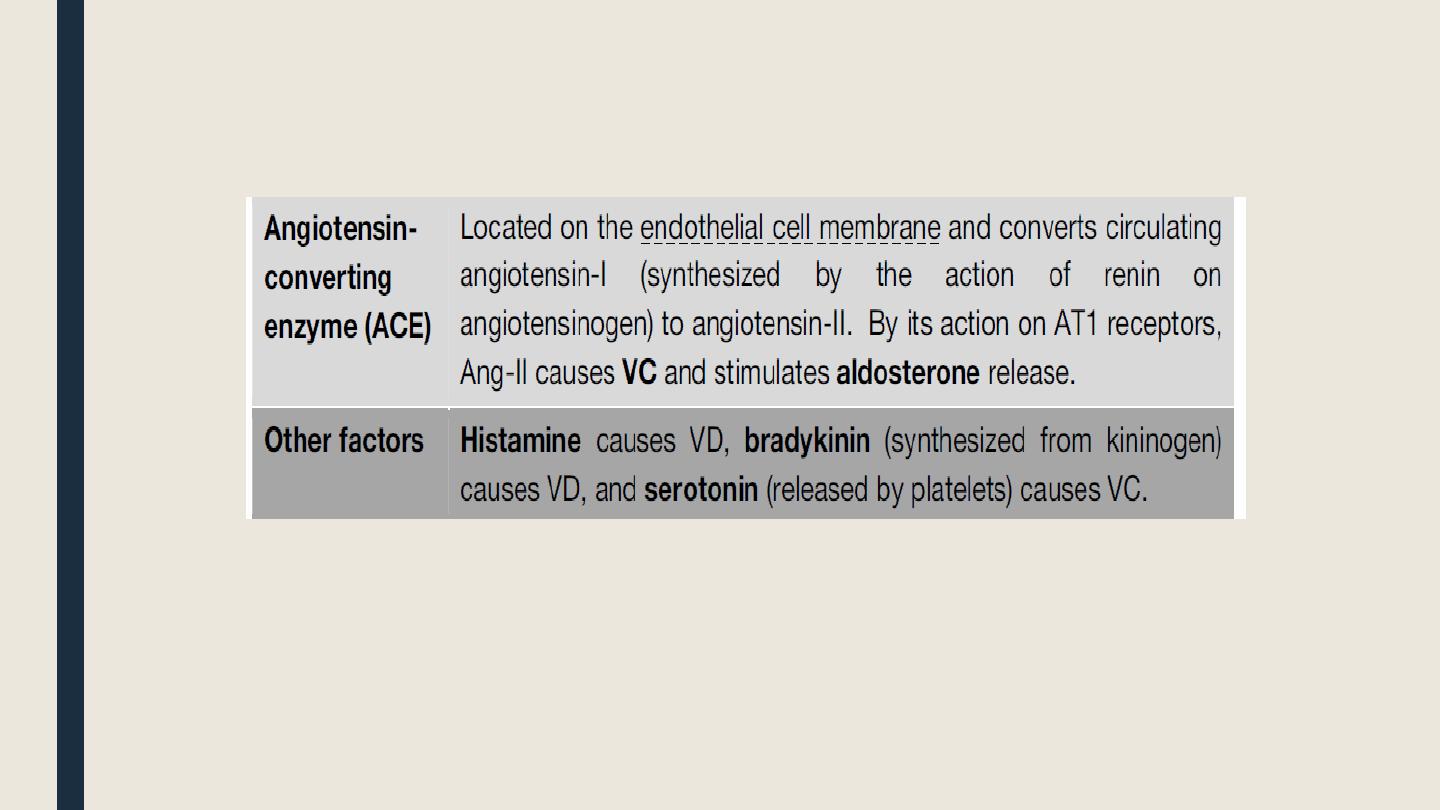
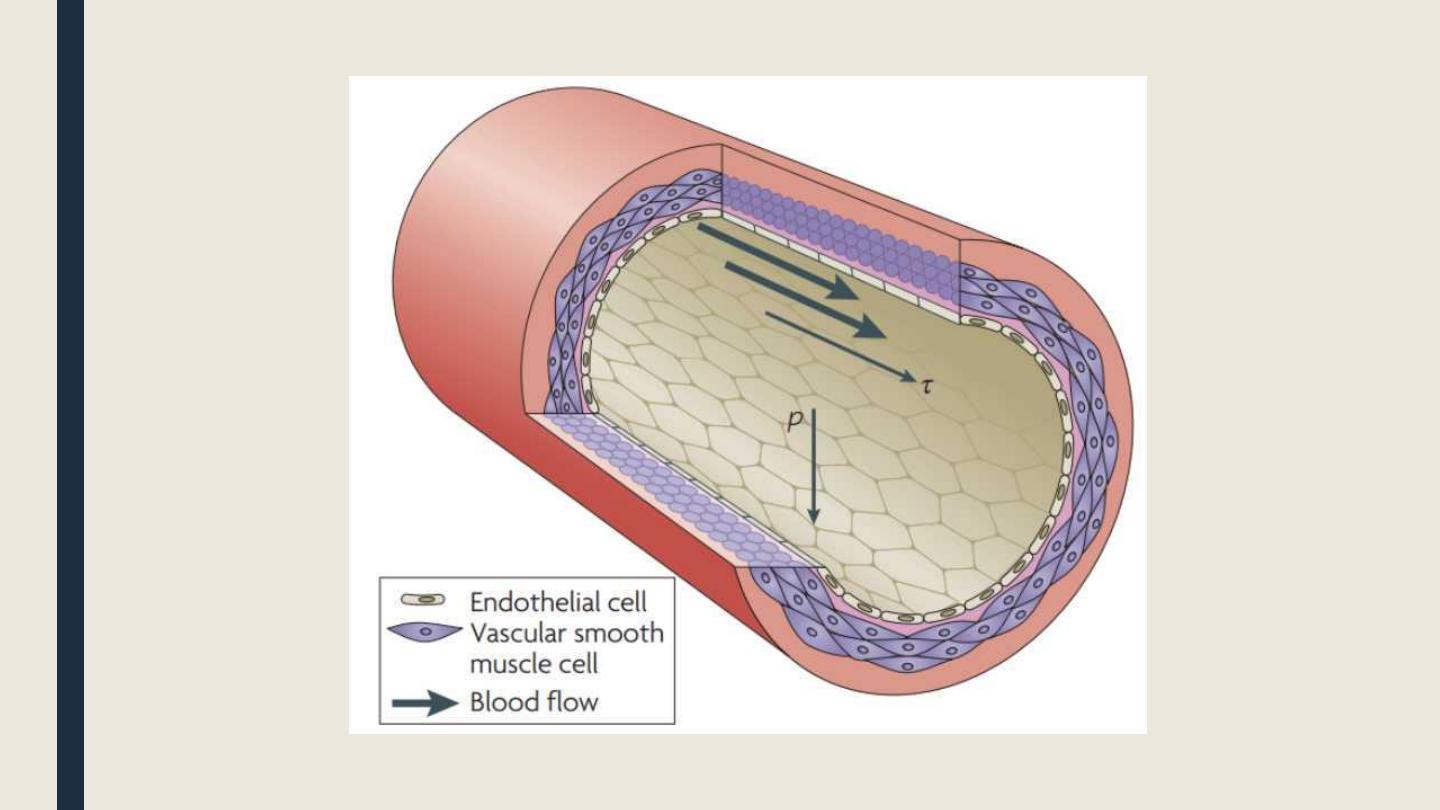
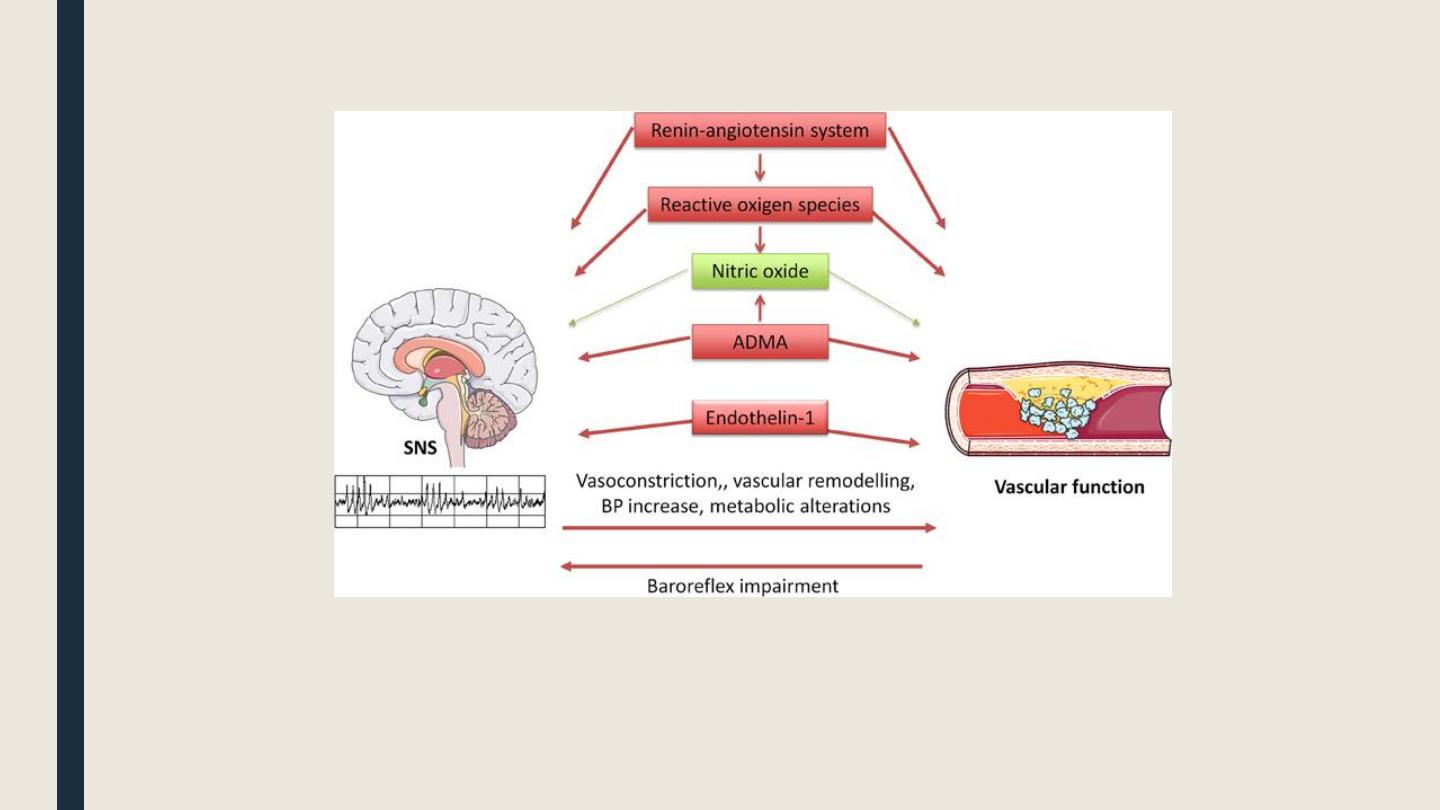
Diagram illustrating interrelationships between
the sympathetic nervous system (SNS) and
vascular function

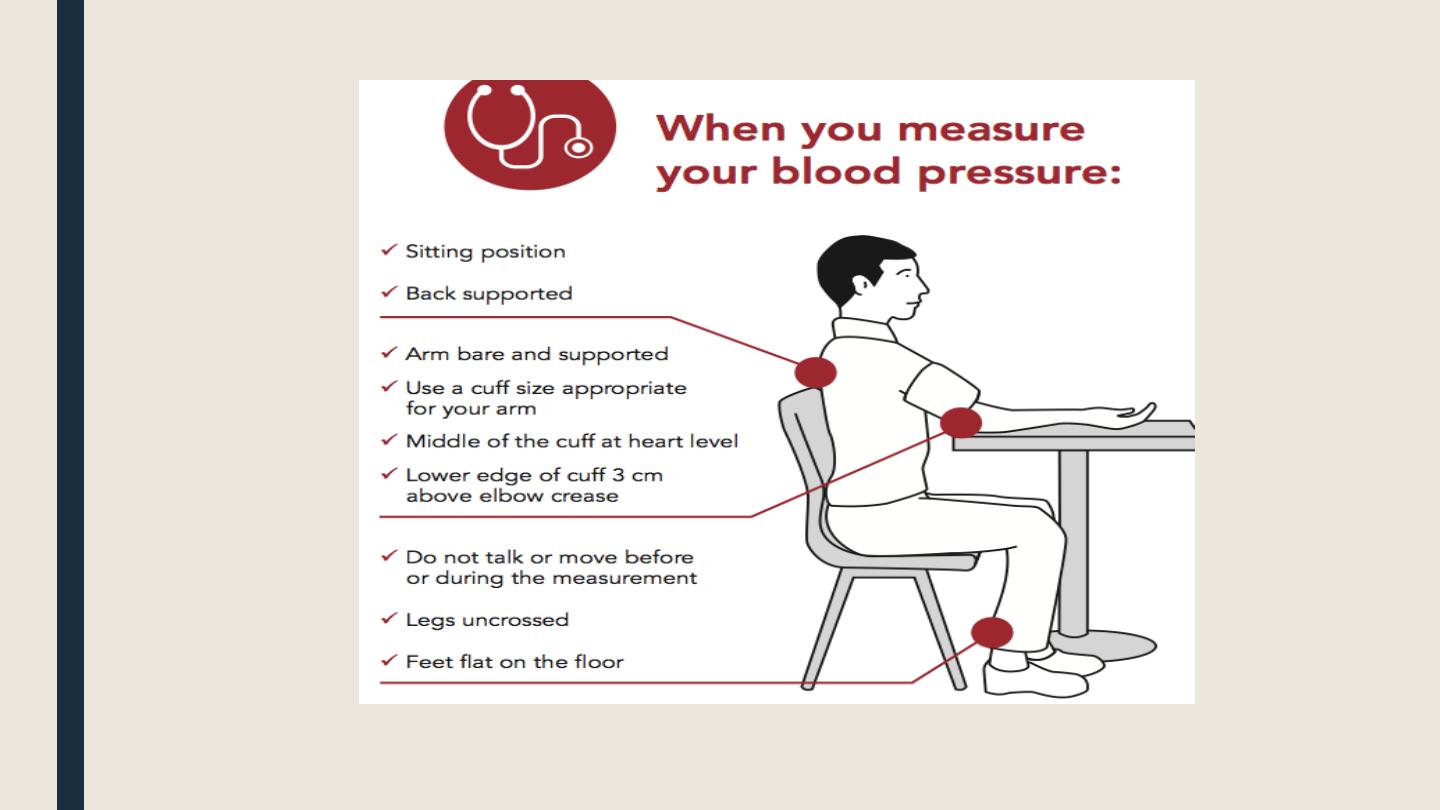
Checking Blood Pressure
•The first sounds that are heard indicate systolic pressure (top number).
•When the sounds stop, diastolic pressure has been reached (bottom number).
•Average blood pressure is: 120/80 mmHg
•The Mean pressure can be calculated by the next equation :
■ Mean pressure = Diastolic BP + 1/3 × Pulse pressure.
■ Pulse pressure can be calculated as following : Systolic BP -Diastolic BP
•Usually the Mean pressure = 93 mmHg , and this is the actual pressure that push the
blood to the circulation.
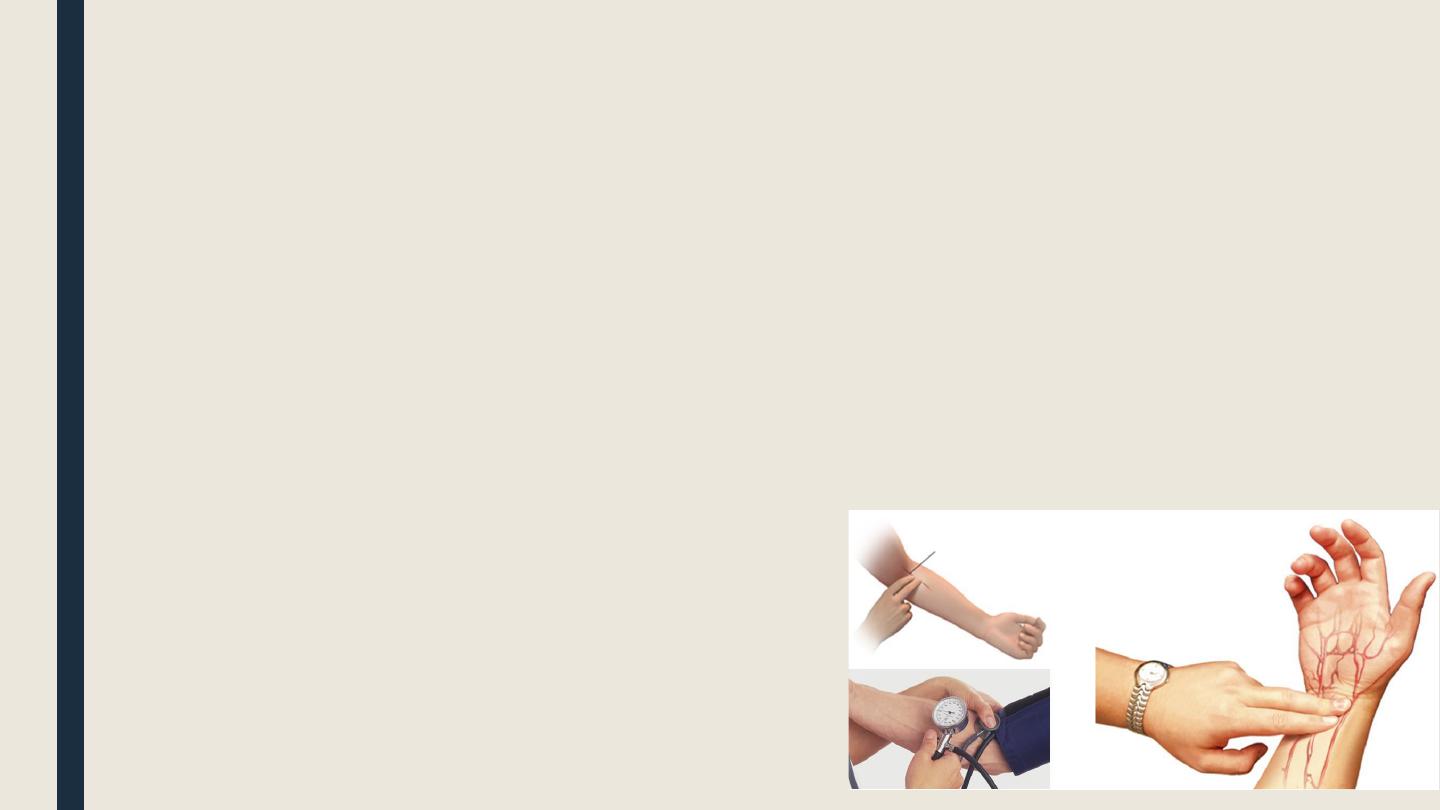
There are 2 method to measure the ABP :
1-Palpation:
Measure only the systolic blood pressure, without the stethoscope by palpating the
Radial pulse in the Radial Artery
2-Auscultation:
Measure the both.. systolic& diastolic blood pressure, with the stethoscope by
auscultating the Brachial pulse in the Brachial Artery

The Sphygmomanometer has 3
types :
1-Mercury Sphygmomanometer.
2-Aneroid Sphygmomanometer.
3-Digital Sphygmomanometer
█ Management of systemic
hypertension
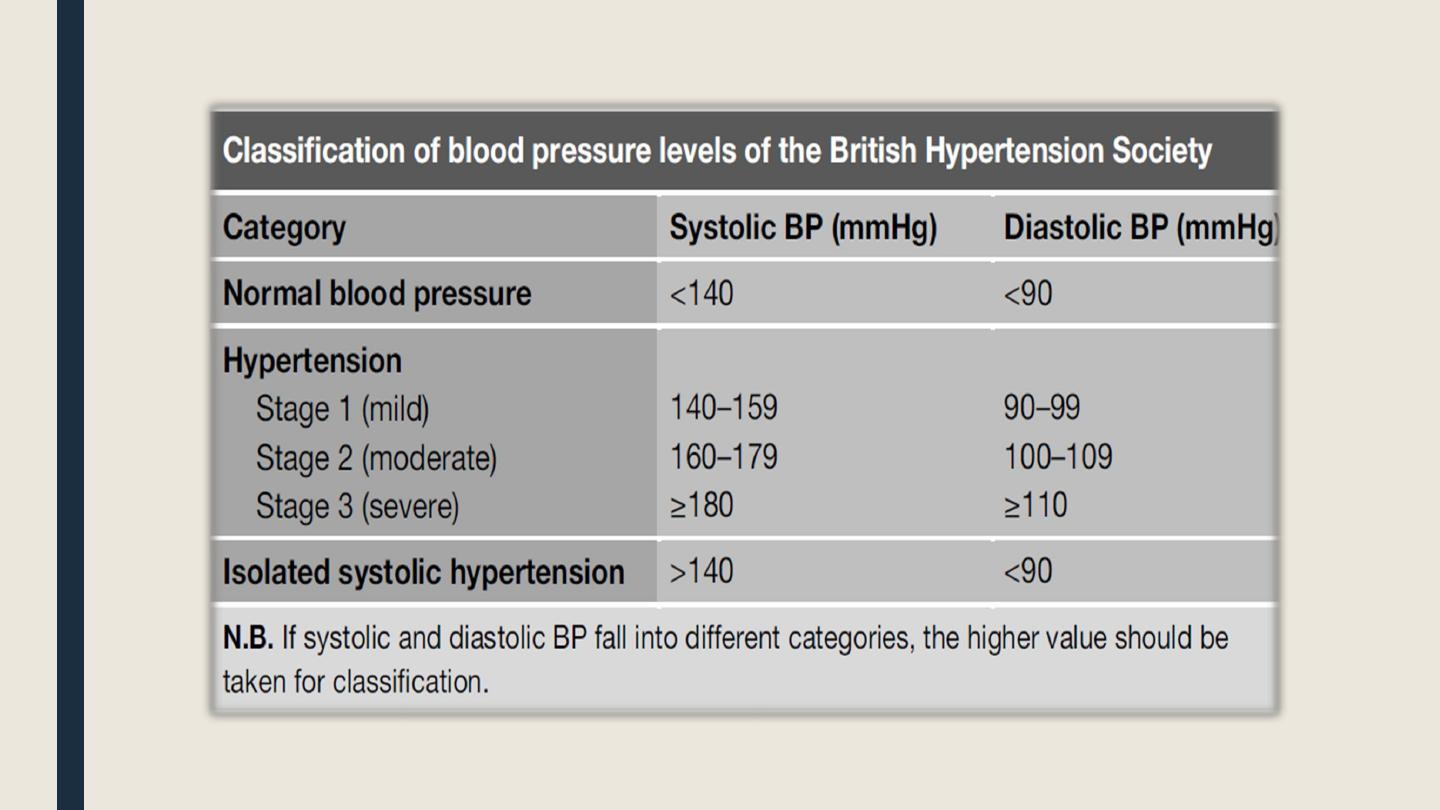
■ Systemic hypertension is persistent elevation of BP above 140/90.
■ Classification of hypertension:
According to etiology: primary (= essential, 90%) or secondary.
According to type: systolic, diastolic, or mixed.
According to degree: see table.
Target BP:
For most patients, the goal of therapy is to maintain BP < 140/90 mm Hg.
In patients with DM or chronic kidney disease, BP should be < 130/80 mm Hg.
Normal Regulation of Blood Pressure
■ According to the hydraulic equation, arterial blood pressure (BP) is directly
proportionate to the product of the blood flow (cardiac output, CO) and the
resistance to passage of blood through precapillary arterioles (peripheral vascular
resistance, PVR)
■ • BP = CO × PVR
Blood pressure is maintained by
• Moment-to-moment regulation of cardiac output and peripheral vascular resistance
exerted at three anatomic sites arterioles, postcapillary venules (capacitance vessels),
and heart.
• Kidney
• Baroreflexes mediated by autonomic nerves (combination with humoral mechanisms,
including the renin-angiotensin-aldosterone system)
• Local release of vasoactive substances

Non-drug therapy = life style modification:
Dietary sodium restriction and potassium and magnesium supplementation.
Stop smoking and avoid stress.
Weight reduction alone can correct hypertension in 75% of obese patients.
Daily physical exercise (~30 min/day): it lowers serum cholesterol, improves
endothelial functions, and enhances tissue oxygenation.
Control of risk factors: e.g. diabetes mellitus, hyperlipidemia, and obesity.
Avoid drugs that ↑ BP e.g. sympathomimetics, sodium-containing drugs, oral
contraceptive pills, corticosteroids
N.B. Patients failing to normalize BP after 2 weeks of non-pharmacological therapy
should be considered for drug therapy.
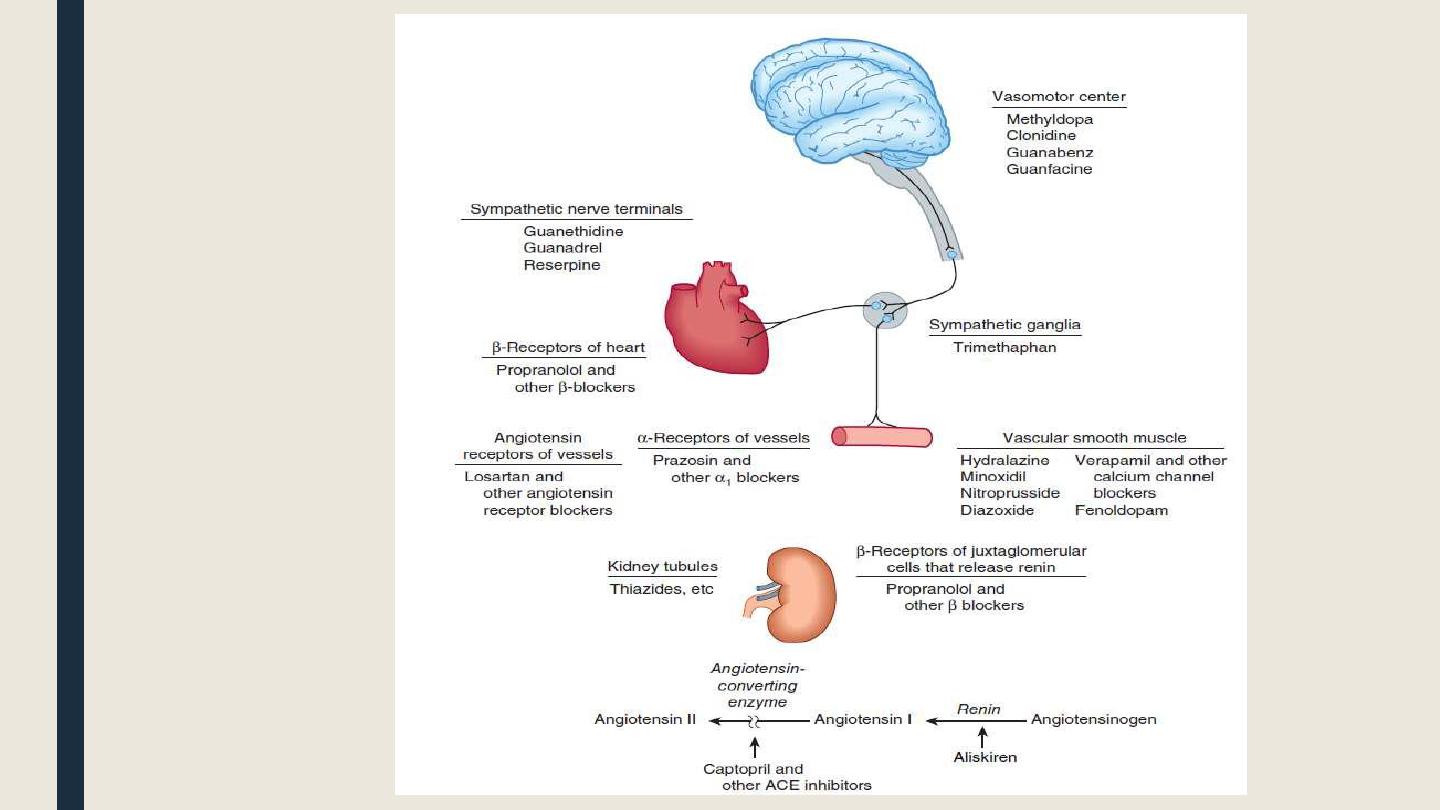
Sites of action of the major
classes of antihypertensive drugs
█ Beta-blockers
■ Indications of beta-blockers in hypertension:
Hypertension associated with cardiac problems e.g. IHD, cardiac arrhythmia,
aortic dissection, etc.
Hypertension associated with thyrotoxicosis.
Hypertension associated with increased sympathetic over activity.
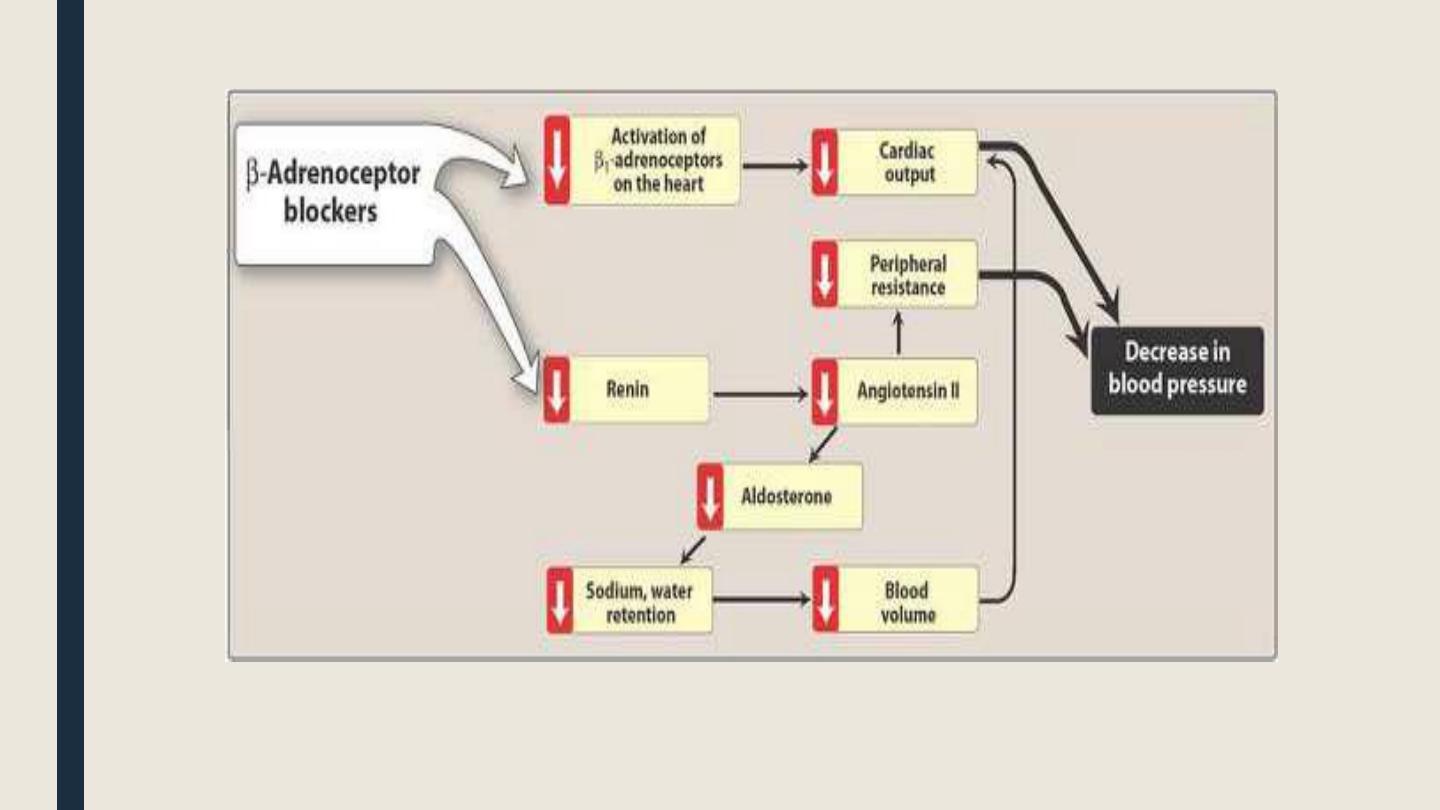
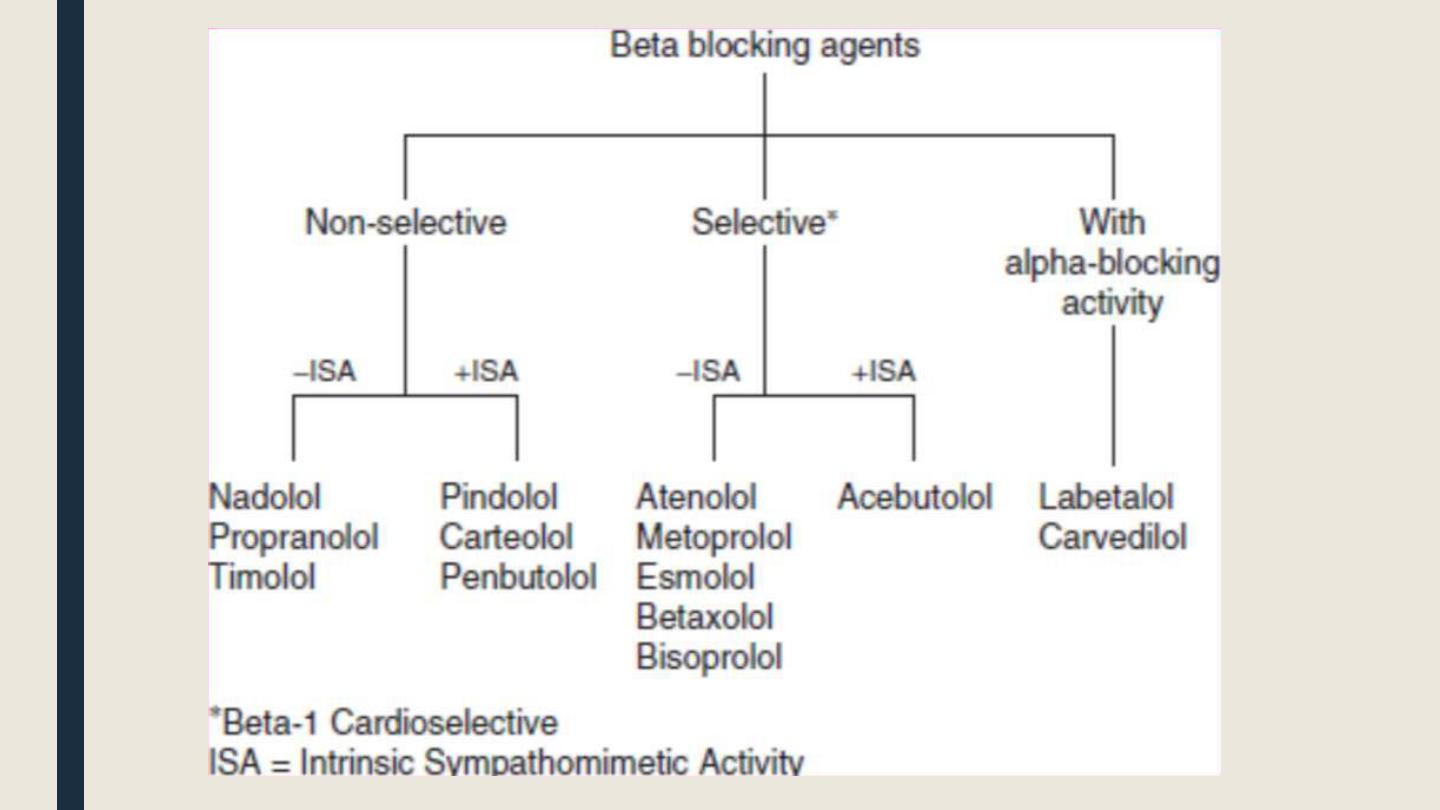
β-Adrenoceptor-blocking Agents
■ β-Blockers are currently recommended as first-line drug therapy for hypertension when
indicated-for example, with heart failure.
A. Actions
• The Beta-blockers reduce BP primarily by decreasing cardiac output. They may also
decrease sympathetic outflow from CNS and inhibit the release of renin from the kidneys,
thus decreasing the formation of angiotensin II and secretion of aldosterone.
• Prototype β-blocker is propranolol, which acts at both β1 and β2 receptors.
• Selective blockers of β1 receptors, such as metoprolol and atenolol, are among the most
commonly prescribed β-blockers.
• The selective β-blockers may be administered cautiously to hypertensive patients who also
have asthma, for which propranolol is contraindicated due to its blockade of β2-mediated
bronchodilation.
Adverse effects
■ Bradycardia, fatigue, lethargy, insomnia, and hallucinations, hypotension,
decrease libido, impotence. Drug-induced sexual dysfunction can severely
reduce patient compliance.
■ Decrease HDL and increase plasma triacylglycerol.
■ Drug withdrawal: Abrupt withdrawal may cause rebound hypertension,
probably as a result of upregulation of β-receptors.
■ Used cautiously in the treatment of patients with asthma, acute heart failure,
or peripheral vascular disease.
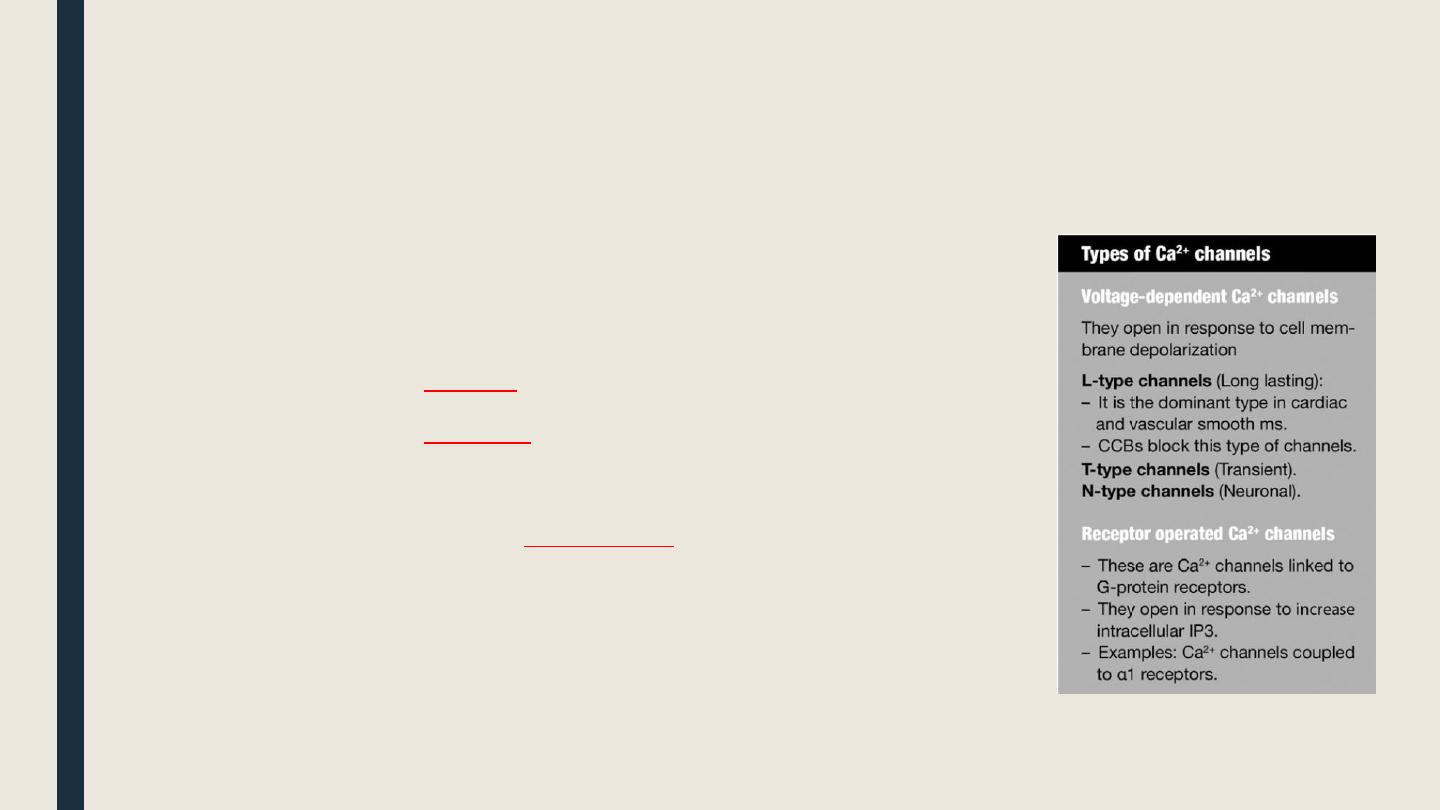
█ Calcium channel blockers (CCBs)
■ These are drugs that block voltage- gated Ca 2+ channels
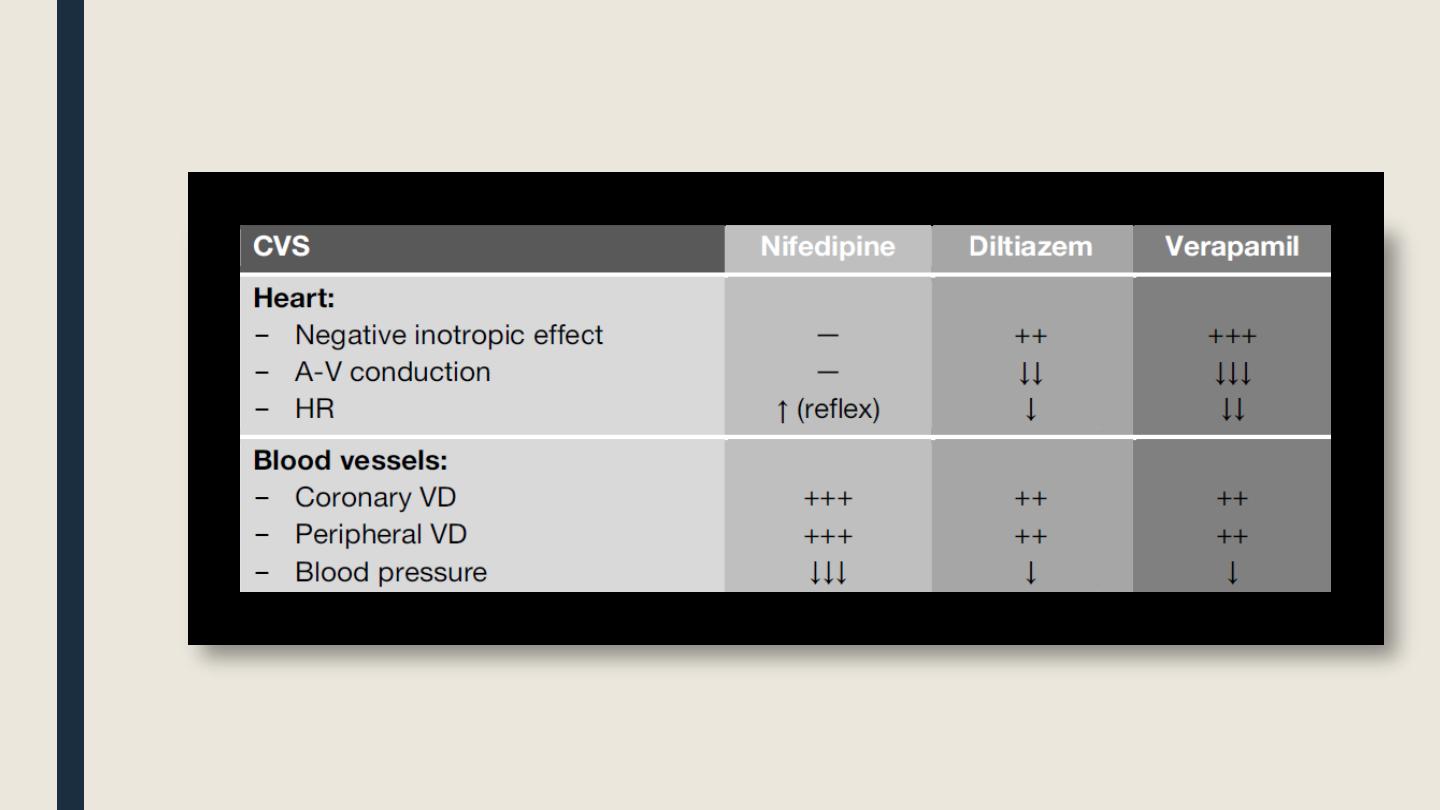
o CCBs according to tissue selectivity
■ CCB with mainly
cardiac
effects: verapamil, diltiazem.
■ CCB with mainly
vascular
effects:
(dihydropyridines): nifedipine, amlodipine, nimodipine, nicardipine
■ CCB with main effect on
other tissue
:
flunarizine, cinnarizine
Other effects
They relax all smooth muscles (vascular, bronchial, GIT, uterine, etc.). cell necrosis and apoptosis.
§ They ↓ Ca2+- mediated
§ Verapamil ↓ insulin release from pancreatic beta cells but of little clinical sign finance.
§ Therapeutic uses
▌Cardio- selective CCBs (verapamil & diltiazm):
Ischemic heart disease (IHD):
■ They ↓↓ myocardial contractility and myocardial O2 demand.
■ They produce coronary VD and ↑ coronary blood flow.
■ They ↓ Ca2+- mediated myocyte cell necrosis.
N.B. vasculoselective CCBs (dihydropyridines) e.g nifedipine are also beneficial in
IHD but they cause considerable peripheral VD so the dose should be adjusted to
avoid hypotension and reflex tachycardia.,
Cardiac arrhythmias: supraventricular
tachycardia (SVT):
■ SVT include atrial flutter, fibrillation, paraxysmal atrial tachycardia, etc.
■
Verapamil ↓ AV conduction, so it protects the ventricles from the rapid atrial rate
(also β-blocker have the same effect).
■ N.B. Nifedipine is contraindicated as it causes hypotension and reflex tachycardia.

Hypertrophic obstructive cardiomyopathy (HOCM):
■ In hypertrophic obstructive cardiomyopathy, the wall of the left ventricle and
interventricular septum is much thickened leading to narrowing of the aortic
outlet and obstruction of blood flow.
■ Increasing contractility worsens the obstruction while decreasing contractility
reduces resistance to blood flow through the aortic outlet and improve exercise
tolerance.
N.B. Nifedipin is contraindicated because produces reflex tachycardia → worsening of
the outflow obstruction .
Arterial hypertension:
■ They ↓ myocardial contractility and COP.
■ They cause peripheral VD due to ↓ vascular smooth ms.
Vasculo-selective CCBs ( Nifedipine and amlodipine):
§ Arterial hypertension.
§ Peripheral vascular disease (e.g. Raynaud’s disease and intermittent
claudication): to improve peripheral microcirculation.
§ Nifedipine is sometimes used to relax the uterus and delay preterm labor
§ Nimodipine as high affinity for cerebral BV. It is used for prevention of cerebral
vasospasm and ischemia complicating subarachnoid hemorrhage.
Adverse effects
■ Verapamil & diltiazem:
– Bradycardia and heart block.
– Worsening of CHF (due to their –ve inotropic effect).
– Constipation due to ↓ GIT motility.
■ Nifedipine:
– Hypotension and reflex tachycardia.
– Gingival (gum) hyperplasia.
– Salt & water retention (=ankle edema; more common than with verapamil due to
significant VD and hypotension).
Contraindications & precautions
■ Verapmil & diltiazem:
– Congestive heart failure.
– Bradycardia nd heart lock.

■ Wolff- Pakinson-White syndrome:
In WPW syndrome , there is accessory conducting pathway between atria and ventricles
other than the normal AV system causing a unique type of atrioventricular re-entry
tachycardia
■ As a rule, most drugs that ↓ AV nodal conduction (Adenosine; Beta-blockers; CCBs;
Dioxin) can paradoxically ↑ the conduction in the abnormal pathway leading to
worsening of the tachycardia.
WPW syndrome can be managed by amiodarone but definitive treatment includes laser
ablation of the accessory pathway .
■ Verapamil should not be combined with digitalis or β-blockers as aggravate
bradycardia caused by these drugs (nifedipine is the drug of be used with β-blocker
because it doesn't cause bradycardia).

Nifedipne:
■ hypotension.
■ hypertrophic obstructive cardiomyopathy (HOCM) .
■ unstable angina (risk of reflex tachycardia).
■ supraventricular tachycardia (SVT ) .
Angiotensin-converting enzyme inhibitors (ACEIs
▌Background
■
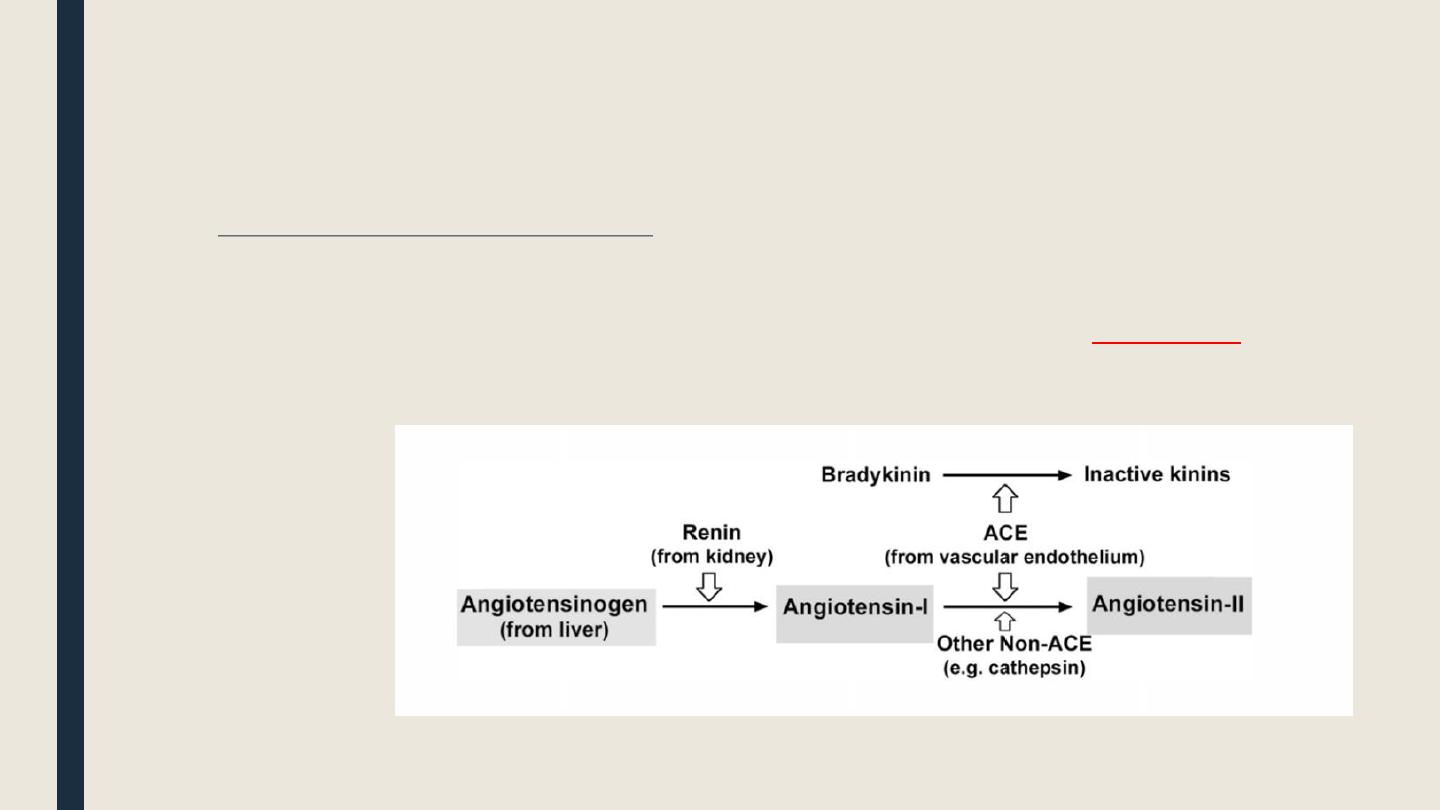
The renin-angiotensin-aldosterone (RAAS) system
§ When renal ischemia occurs, there is ↓ RBF and ↓ GFR. This lead to acute oliguria that may develop to acute tubular
necrosis.
■
As a compensatory mechanism, renin is released from the juxtaglomerular cells of the kidney as a
rescue message
to
initiate stimulation of RAAS as follows:
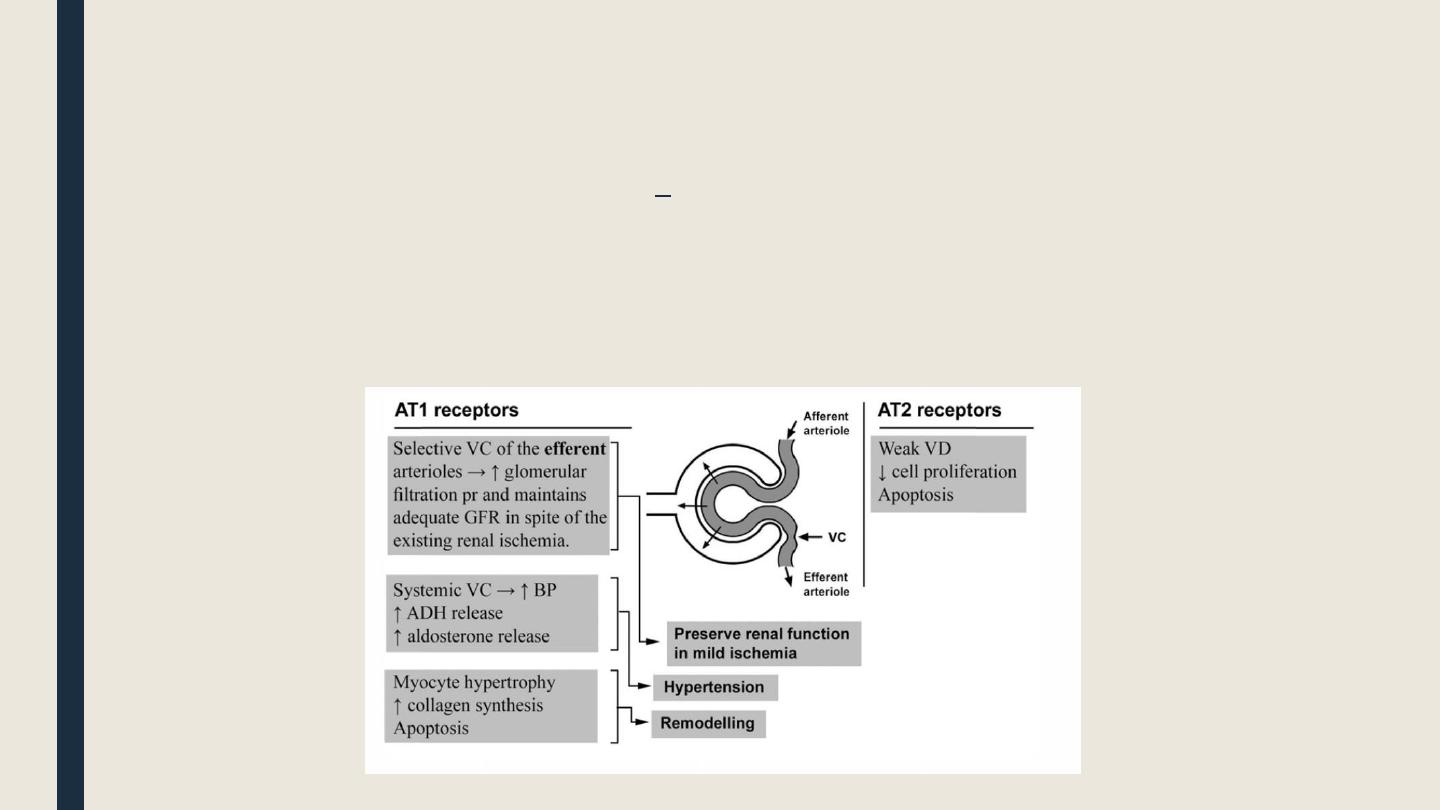
■ Ang-II acts on AT1 receptors in the efferent arteriole of the kidney causing their VC
and thus maintains adequate GFR in spite of the ↓RBF.
§ Unfortunately, Ang-II acts on AT1 receptor in other vascular beds and tissues causing
systemic VC, cell hypertrophy, and apoptosis (i.e. degenerative changes).

Should we inhibit the RAAS?!
Inhibition of the RAAS will correct the hypertension but also will ↓ GFR and aggravate
RF if renal ischemia was grave.
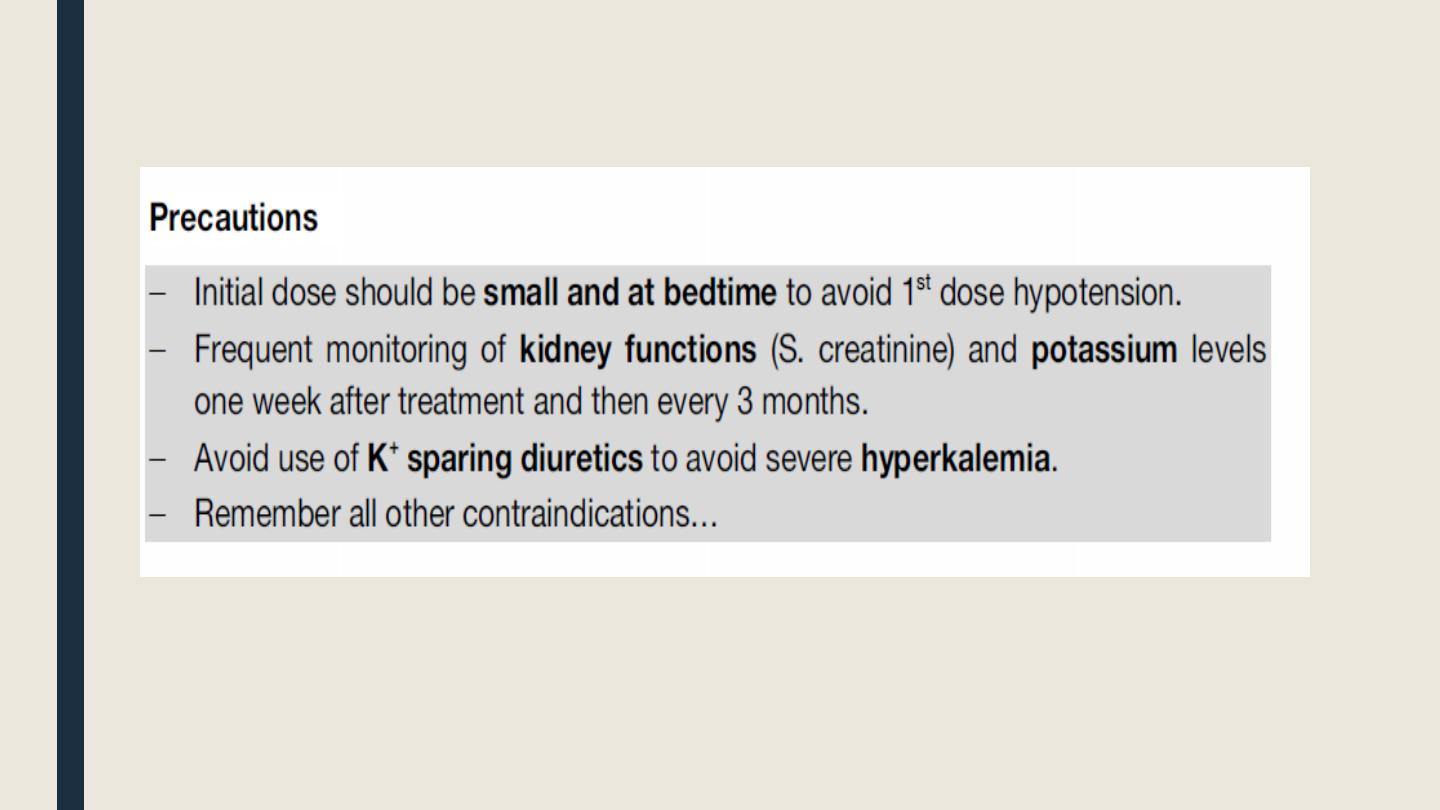
Normal S. creatinine is 0.3-1.2 mg/dl. If S. creatinine is up to 3 mg/dl (i.e. mild renal
impairment) → you can block RAAS.
If S. creatinine >3 mg/dl (i.e. severe renal impairment) → blocking the RAAS is
dangerous and will aggravate RF.
█ Angiotensin converting enzyme inhibitors
■ Classification
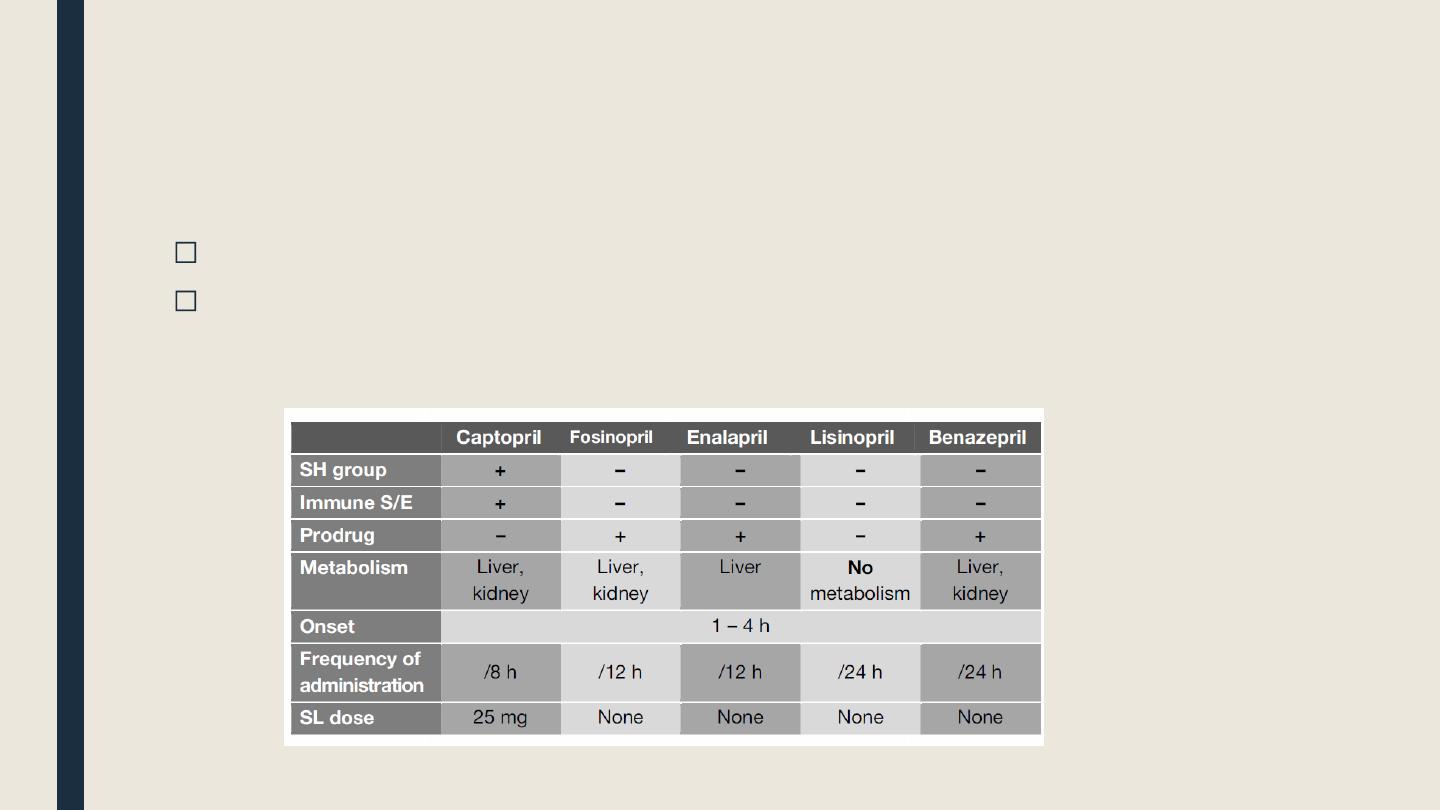
SH-containing drugs: Captopril, zofenopril, alacepril
Non SH-containing drugs: Enalarpril, fosinopril, lisinopril, benazepril, ramipril
Pharmacological properties of some ACEIs

Mechanism of action
■ They inhibit Ang-converting enzyme (ACE) in the vascular endothelium leading to:
– Inhibition of both Ang-II formation and aldosterone release (→ ↓ both VC and salt & water
retention).
– Prevent degradation of bradykinin which is a potent VD.
– Most ACEIs have direct VD action to both arteries (i.e. ↓ afterload) and
veins (i.e. ↓ preload).
Pharmacological effects
■ They ↓ BP mainly by decreasing peripheral resistance but no reflex tachycardia or
changes in the COP c n occur. This may be due to either (1) resetting of
baroreceptors; and/or (2) enhanced parasympthetic activity.
■ They ↑ COP (only in presence of CHF ) due to reduction venous return (preload), and
systemic BP(afterload).
■ They ↓myocardial changes complicating acute myocardial infarction
(ventricular hypertrophy, and dens collagen scar) because they prevent
myocyte cell hypertrophy and collagen synthesis (i.e. prevent cardiac remodeling).
■ Other tissue : they ↓ apoptosis, ↓ cell hypertrophy, & ↓ collagen synthesis
(i.e. They reduce degenerative changes caused by the action f Ang-II on AT1
receptors).
Therapeutic uses
■ Systemic hypertension :
-
Hyperreninemic hypertension.
-
Normoreninemic hypertension:
because they are direct VDs.
■ Congestive heart failure (CHF):
- To ↓
after load and preload through reduction of both systemic vascular
resistance, and aldosterone release (↓Na and H2O retention ).
- To ↓ myocardial hypertrophy and dilatation i.e. ↓ remodeling).
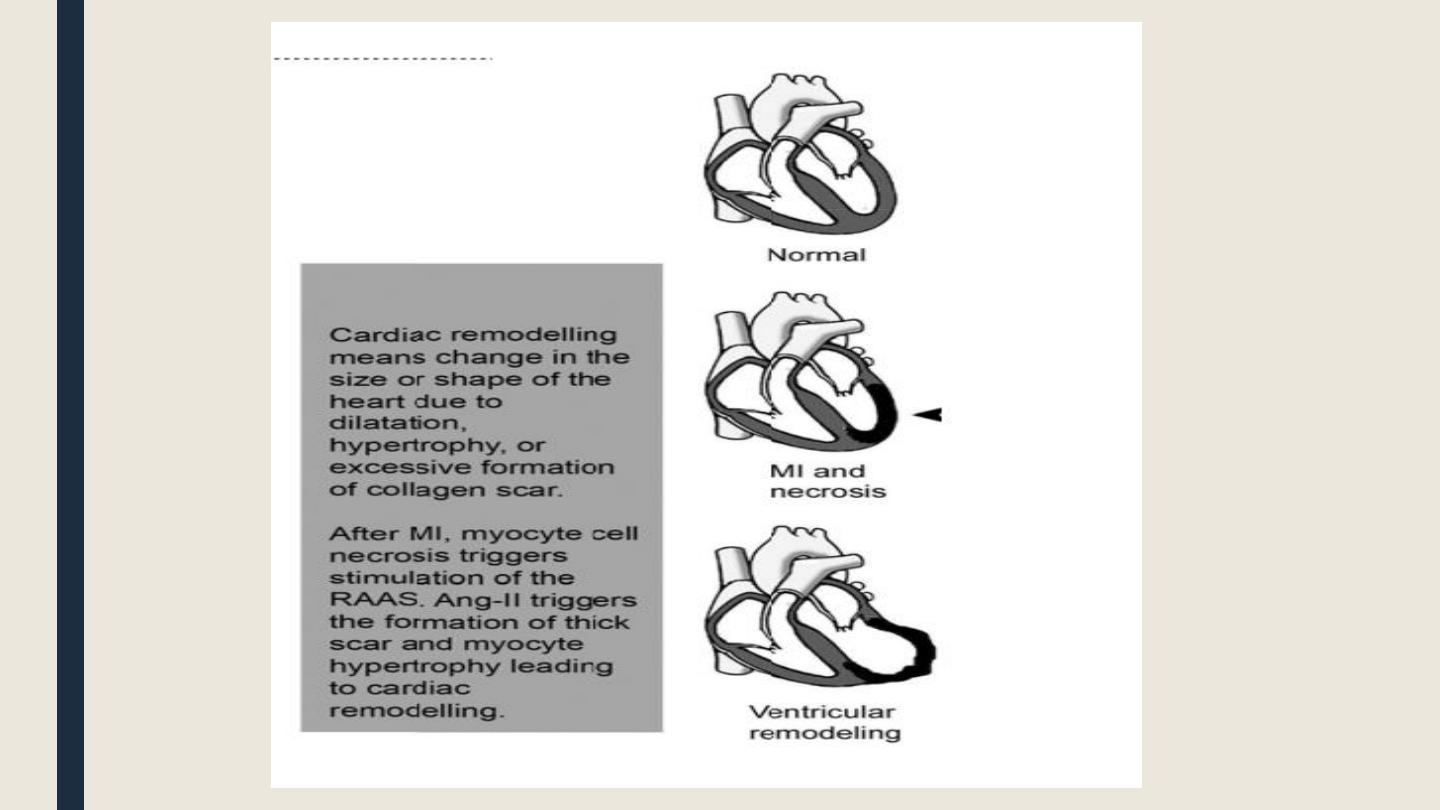
■ To prevent
L
V hypertrophy
(rem
odeling) after acute MI through:
-
↓
arterial BP (
↓
myocardial strain)
- ↓
myocyte cell hype trophy, apoptosis, and collagen synthesis.
■ Diabetic nephropathy & microalbuminuria:
–
They
↓
renal changes complicating diabetic nephropathy (mesangial cell
apoptosis
,
prolifeation, and coll
a
gen sy
n
thesis),
thus reducing microalbuminuria
(provided that renal impairment is not grave).
Adverse effects:
C: Dry Cough (the most common): inhibition of ACE leads to accumulation of and PGs,
which cause bronchial irritation and spasm.
Treatment: stop ACEIs. Cough will resolve after a few days.
A: Angioedema (edema of the face, tongue and throat): due to accumulation of
bradykinin or due to immune reaction. It may be life threatening.
P: Aggravation of Proteinuria in patients with significant renal failure.
T: Taste changes: temporary loss of taste (ageusia and dysgeusia).
O: Orthostatic (First dose) hypotension: especially in sodium depleted (hypovolemic)
patients. Prevention: start by small at bedtime then increase gradually
P: Pregnancy: teratogenesis (fetal pulmonary hypoplasia and renal dysfunction)
R: skin Rash
I: Increase K+ (hyperkalemia) due to ↓ aldosterone release.
L: Leukopenia (neutropenia): especially in patients with impaired renal function.
■ Contraindications
■ Hypotension: when systolic BP is less than 95 mm Hg.
■ Severe renal failure or bilateral renal artery stenosis (SCr > 3 mg/dl). Why?
-In these conditions, the use of ACEIs is dangerous because they ↓ Ang-II → ↓ VC of the efferent
arterioles → ↓ glomerular filtration pressure and↓ GFR → aggravation of renal failure in both
kidneys.
- Dangerous hyperkalemia may occur.
- Dangerous neutropenia may occur.
■ Pregnancy and lactation :
thee may cause fetal pulmonary hypoplasia and growth retardation.
■ Hyperkalemia:
■ Neutropenia, thrombocytopenia or severe anemia (ACEIs
may cause bone Marrow depression).
■ Immune problems whether due to autoimmune diseases or due to immunosuppressive
drugs )
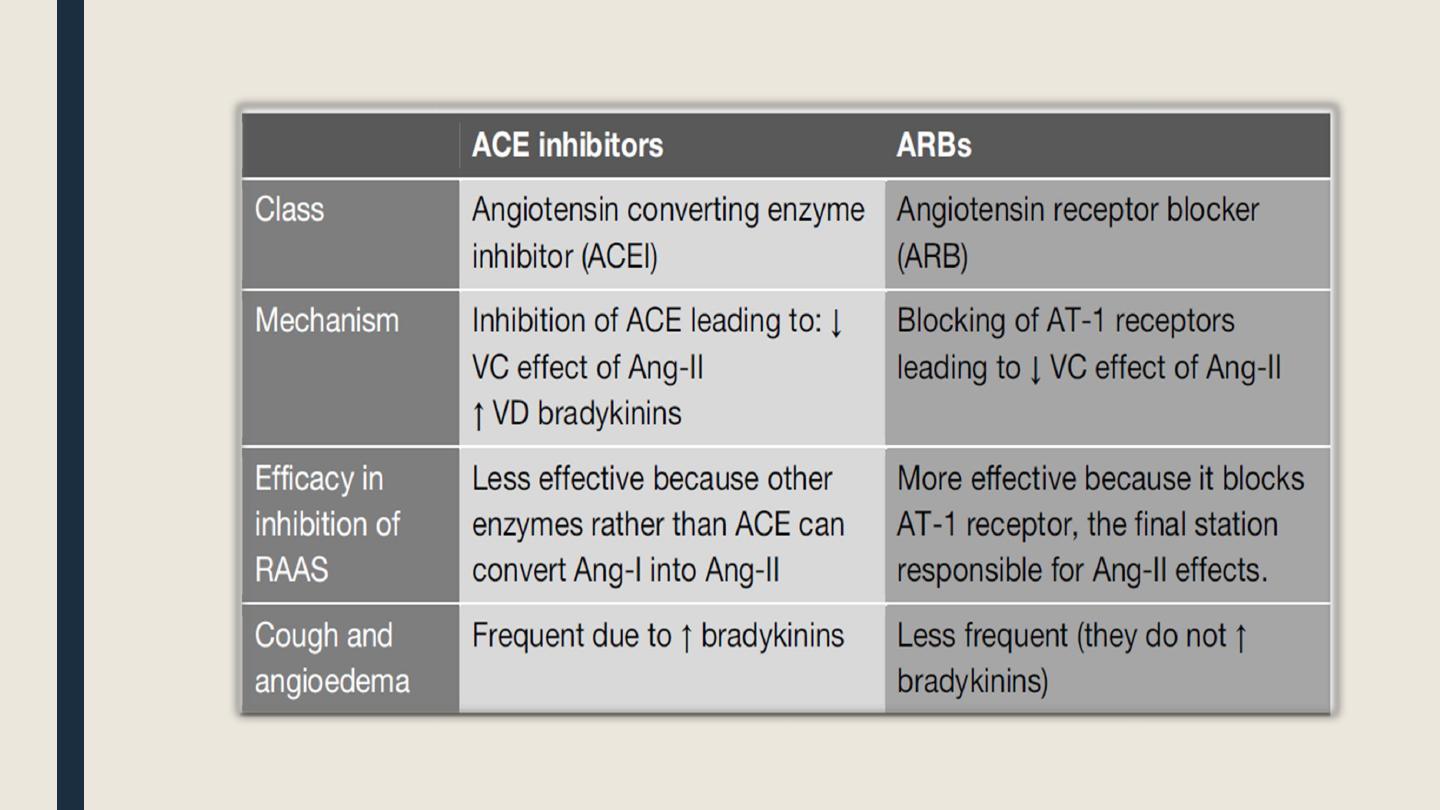
█ Angiotensin II receptor blockers (ARBs)
(Losartan- Valsartan- Candesartan- Telmisartan)
They selectively block AT1 receptors and they exert most of the pharmacological
effects seen with ACEIs.
They have no effect on bradykinin metabolism.
They have the potential for more complete inhibition of Ang-II action compared with
ACE inhibitors because there are non-ACE enzymes (cathepsin and chymase) that can
convert Ang-I into Ang-II.
The adverse effects and contraindications are similar to those of ACE inhibitors but
cough and angioedema are less common than with ACE inhibitors.
█ Direct renin inhibitors: aliskiren
Activation of angiotensinogen into Ang-I by renin is the rate limiting step in formation
of RAAS.
Aliskiren is a recently approved drug for treatment of hyperreninemic hypertension. It
inhibits renin activity and consequently the RAAS.
The efficacy and side effects of aliskiren are comparable to ACEIs and ARBs.