Fluids used in surgery
IntroductionTotal body fluid accounts for approximately 60% of total body weight(this can be 70% or higher in newborn down to 50-55% in mature women).
Total body fluid can be divided into intracellular and extracellular.
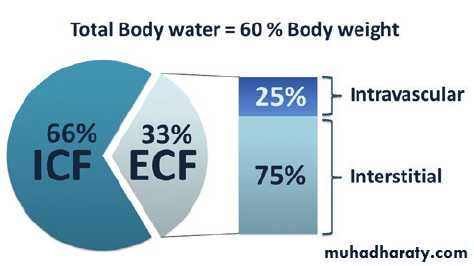
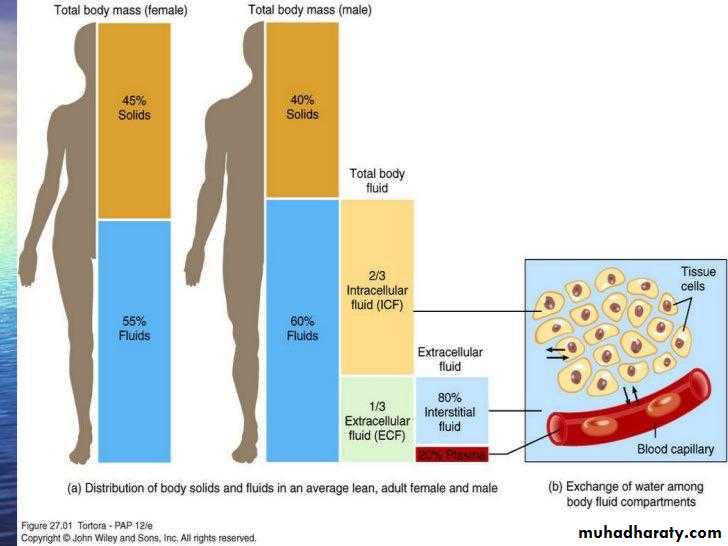
Extracellular fluid
Accounts for 1/3 of the total body weightSolutions that contain small molecules that flow easily through cell membranes.
This will increase fluid volume in both the interstitial and intravascular spaceSolutions that contain large molecules that do not pass the cell membranes.
They remain in the intravascular compartment and expand the intravascular volume by drawing fluids from extravascular space.
o.9 sodium chloride(normal saline)
Indication:
1- to treat volume deficit from hemorrhage, sever vomiting or diarrhea, heavy drainage from GIT suction, fistulas or wounds.
2- shock.
3- mild hyponatremia.
4- metabolic acidosis(DKA).
5- resuscitation.
6- it’s the only fluid used with administration of blood products.

caution
Because normal saline replaces extracellular fluid, it should be used cautiously in certain patients(those with cardiac or renal disease ) for fear of fluid volume overload.Dextrose 5%
It’s considered an isotonic solution, but when dextrose is metabolized, the solution actually become hypotonic and causes fluid shift into cells.
caution.
D5W is not good for patients with renal failure or cardiac problems since it could cause fluid overload.Patients at risk for intracranial pressure should not received D5W since it could increase cerebral edema.
It should not be used in isolation to treat volume deficit because it dilutes plasma electrolyte concentrations.
Never mix dextrose with blood as it causes blood to hemolyze.
Not used for resuscitation, because the solution will not remain in the intravascular space.
Not used in early post operative period, because the body's reaction to the surgical stress may cause an increase in antidiuretic hormone secretion.
Ringer lactate(Hartmann solution)
Is the most physiologically adaptable fluid because its electrolyte content is most closely related to the composition of the body's blood serum and plasma.
Another choice for first –line fluid resuscitation for certain patients, such as those with burn injury.

indication
To replace GIT fluid losses.Fistula drainage.
Fluid losses due to burns and trauma.
Patient experiencing acute blood loss or hypovolemia due to third- space fluid shift.
caution
Don’t give ringer lactate to patient with liver disease as they can’t metabolize lactate.Used cautiously in patients with severe renal impairment because it contains some potassium.
Should not be given to a patient whose pH is greater than 7.5.
Ringer solution
Used in a similar fashion as LR, but doesn’t have the contraindications related to lactate
Hypotonic fluids
Hypotonic fluids have a lower concentration of solutes, and osmolarity less than 250 mOsm/L.It lowers the serum osmolarity within the vascular space, causing fluid to shift from the intravascular space to both the intracellular and interstitial spaces.
These solutions will hydrate cells, although their use may deplete fluid within the circular system.
indications
Hypotonic fluids are used to treat patients with conditions causing intracellular dehydration, such as:1- hypernatremia.
2- DKA.
3- Hyperosmolar hyperglycemic state.
cautions
Never give hypotonic solution in patients who are t risk for increased ICP because it may exacerbate cerebral edema.Don’t used hypotonic solutions in patients with liver disease, trauma, or burns due to the potential for depletion of intravascular fluid volume.
Hypertonic solutions
Solutions that have higher tonicity or solutes concentration, they have osmolarity of 375 mOsm/L or higher.The osmotic pressure gradient draws water out the intracellular space, increasing extracellular fluid volume, so they are used as volume expanders.

indications
1- patients with severe hyponatremia.2- patients with cerebral edema.
Caution
Be alert when administrating hypertonic solutions because of their potential for causing intravascular fluid volume overload and pulmonary edema.Should not be given for indefinite period of time.
Colloid solutions
It expand the intravascular volume by drawing fluid from the interstitial space into the intravascular compartment through their higher oncotic pressure.The same effect as hypertonic crystalloids solutions but it requires administration of less total volume and have a longer duration of action because the molecules remain within the intravascular space longer.
Colloid
5% albumin(human albumin solution).The most commonly utilized colloid solutions.
It contains plasma protein fractions obtained from human plasma and works to rapidly expand the plasma volume.
Used for:
Volume expansion.
Moderate protein replacement.
Achievement of hemodynamic stability in shock states.
contraindications
1- severe anemia.
2- heart failure.
3-Known sensitivity to albumin.
4-ACEI should be withheld for at least 42 hours before administrating albumin because of the risk of atypical reactions, such as flushing and hypotension.
Transfusion reaction
Signs of transfusion reactions:Fever, flank pain, vital sign changes, nausea, headache, urticaria, dyspnea and bronchospasm.
Rx:
1- stop the transfusion.
2- keep the I.V line open with normal saline solution.
3- notify the physician and blood bank.
4-intervene for signs and symptoms as appropriate.
Monitor the vital signs.
Other colloids
HydroyethalstarchesAnother form of hypertonic synthetic colloids used for volume expansion.
Contain sodium and chloride used for hemodynamic volume replacement following major surgery and to treat major burns.
Less expensive than albumin and their effect can last 24 to 36 hours.

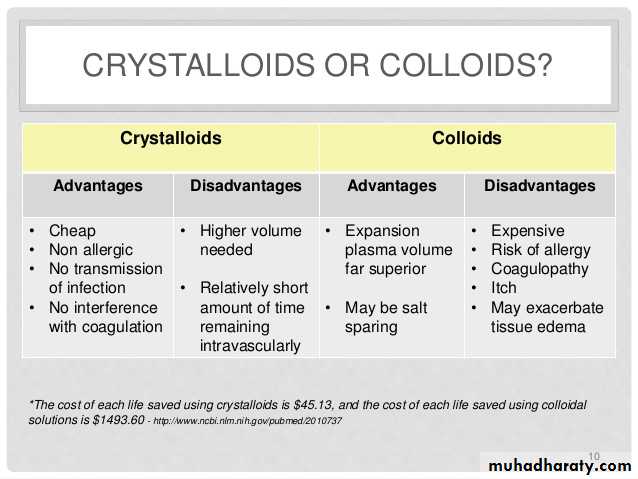
CRYSTALLOIDS VS. COLLOIDS
Fluid therapy in surgeries
fluid therapy is needed pre-operatively, intraoperatively and postoperatively.Pre-operative fluid therapy
The administration of maintenance fluids should be all that is required in an otherwise healthy individual who is under orders of receiving nothing by mouth for some time before the time of surgery. This does not, however, include replenishment of pre- existing deficit or ongoing losses.Maintenance therapy calculation
For the first 10kg give 100ml/kg per dayFor the second 10kg give an additional 50ml/kg per day
For weight above 20kg give an additional 20ml/kg per day
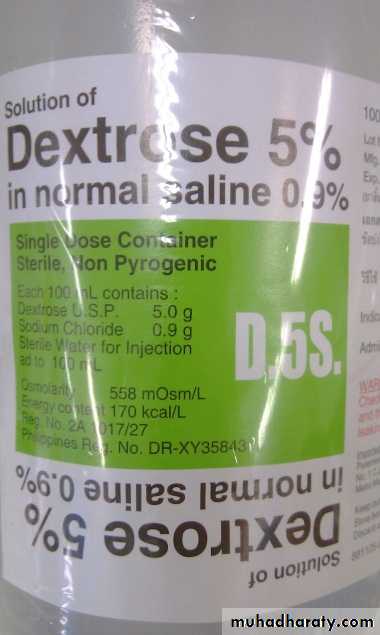
The appropriate choice of fluid would be 5% dextrose in 0.45% sodium chloride at 100ml/h as initial therapy, with potassium added for patients with normal renal function.
Fluid deficit in surgical patients
many surgical patients have volume and/or electrolyte abnormalities associated with their surgical disease so it must be evaluated as it is a vital step in the pre-operative assessment and care.Volume deficit should be considered in patients who have obvious GI losses, such as through emesis or diarrhoea, as well as patient with poor oral intake secondary to their disease.
Less obvious cases are those with third space or non functional ECF losses, that occur with GI obstruction, peritoneal or bowel inflammation, ascites, crush injuries, burns, and sever soft tissue infection such as necrotizing fasciitis.
So how do we assess hydration status?
the assessment acute volume loss is primarily clinical through the following:• Patients level of consciousness
• Thirst• Eye glistening
• Sunken eyes
• Floor of mouth and mucous membrane
• Tongue
• Skin turgor
• Pulse (rate, rhythm and volume)
• Blood pressure
• Urine output
Acute volume deficits should be corrected as much as possible before the time of operation, so once its diagnosed prompt fluid replacement should be started with usually isotonic crystalloid depending on the measured serum electrolyte values.
Intraoperative fluid therapy
with the induction of anaesthesia, hypotension will develop and this hemodynamic instability is best avoided by correcting known fluid losses, ongoing losses, and providing adequate maintenance fluid therapy preoperatively.Intra operative fluid losses beside measured blood loss especially in major abdominal surgeries are associated with continued extracellular losses in the form of bowel wall edema, peritoneal fluid and wound edema during surgery. And not to forget third space or parasitic losses such as in burns cases, so the intraoperative fluid therapy should aim at maintaining base line requirements correcting known fluid losses and replacing ongoing losses.
So saline administration is necessary to restore the obligate fluid losses mentioned earlier, although no accurate formula can predict intraoperative fluid needs, replacement of fluid during surgery often requires 500 to 1000ml/h balanced solution to support homeostasis.
Postoperatively fluid therapy
Postoperative fluid therapy should be based on the patient’s current estimated volume status and projected ongoing losses.Criteria of fluid given postoperatively:
1.Isotonic solution2.Contains energy
3.does not contain electrolyte
so according to this criteria the fluid of choice is Dextrose 5%
Postoperative fluids replacement
1- first day: 2L Dextrose 5% is given
2- second day: 2L of dextrose with 1Lof normal saline.3- third day :-fluid is given as 2???????? day with potassium 60 mmol/ 24 hr.
IV line common problems
1- infiltration.When the catheter is introduced into the tissue surrounding the blood vessels.
2- phlebitis.
3- hypothermia
When large amounts of cold fluids are infused rapidly.
4- local infection(abscess)
Cases
25 years old male with multiple GSW in chest and abdomen with GCS 12, was brought to the ED on your night shift, following the trauma protocol; team A was assigned to manage the patient's airway and breathing and you were assigned on managing his circulation and control of bleeding.1.What will you assess first?
2.What actions you will take upon your assessment?
3.What type of fluid you'll give this patient?

Assess the following:
1.Conciuosness level2.Pulse
3.Blood pressure
4.Skin colour
Perform the following actions:
1.Two large-bore cannulae for intravenous access.2. Withdrawal of blood for blood test and cross matching.
3. Initiation of intravenous fluid and send for blood type (O negative).
4.Measure patients blood pressure and monitor his urine output after insertion of Foley's catheter.
5.look for any site of bleeding and control it if possible.
This patient has acute blood loss so the best fluid to be given for resuscitation is colloid or 0.9% normal saline until the blood is available.
On Christmas eve, a 35 years old male was ambulated to the ED after catching on fire in his own house due to electrical dysfunction. The patient weighs 70kgs and upon examination he had second and third degree burns in about 20% BSA.
1.Regarding his fluid therapy management, what type of fluid should you use and what is the rate of infusion in the first 24hrs?
Parkland formula for fluid resuscitation
• Use lactated ringer’s solution
LR 4ml x weight (kg) x % BSA burned over the initial 24hours
Half over the first 8hrs from the time of burn, other half over the subsequent 16hrsPost operative patient with perforated DU was moved from the recovery room to his bed in the surgical ward, the patient has a Foley's catheter and a drain at the site of the surgery.
-What is the most important thing to never miss in such patient regarding his fluid therapy management?
-Is urine output considered deficit or not?
-upon examination, he was running fever of 39°c, action to be taken?

1.Never forget to chart and replace the added losses through the drains!
2. no, urine in Foley’s cath. Is included in the patients maintenance therapy unless it passes more than 1500ml/day.
3. for every 1°c above 37°c add 250ml to his fluid therapy.