


OBJECTIVES:to through a light on:1- congenital anomalies of the nose 2- nasal trauma
Congenital Anomalies of the Nose1-Choanal atresia
2-Congenital nasal masses
3-Agenesis of the nose
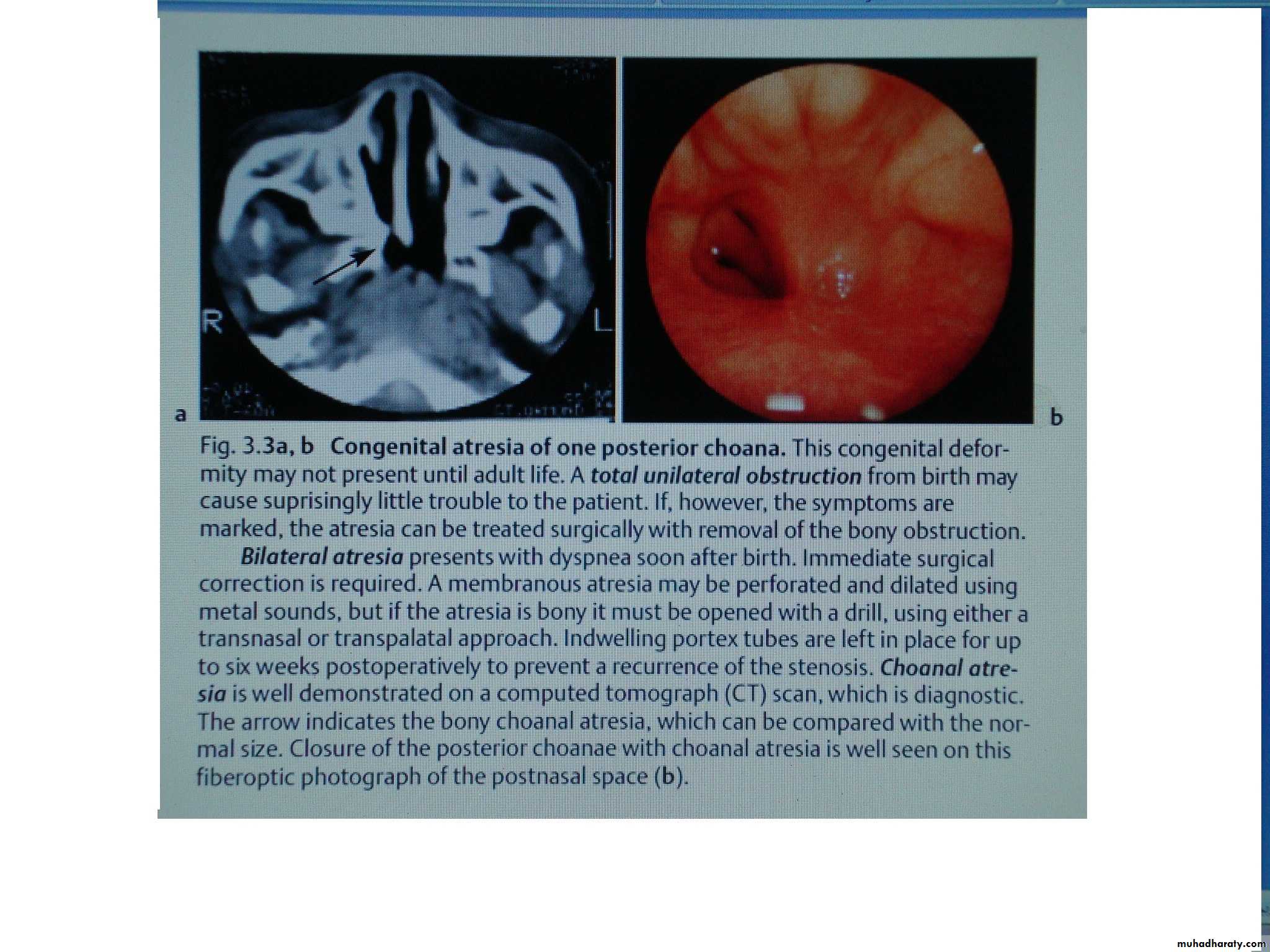
1- Choanal atresia:
Incidence: (1 per 8000 live births).Aetiology:
1-Due to persistence of the primitive bucco-nasal membrane.
2-Non-syndromal choanal atresia can be transmitted as an autosomal recessive trait,
Types:
1- Bony2- Membranous
3- Partly bony and partly membranous.
Degrees:
1- Complete unilateral (most common).
2- Complete bilateral atresia.3- Incomplete unilateral atresia.
4- Incomplete bilateral atresia.
Pathology:
Usually when the atretic plate is of the bony type, it is thin and easily perforated. Choanal atresia may be associated with:Bowing of lateral nasal wall.
Facial asymmetry.
High arched palate and deformed or absent teeth.
Clinical features:
It is more common in female than male in a ratio of 2:1.A- Unilateral choanal atresia
1- Presents usually in later childhood or even adulthood.
2- Nasal obstruction (unilateral).
3- Excessive tenacious and glue-like nasal discharge (unilateral).
B- Bilateral choanal atresia
1- Almost always presents as respiratory emergency at birth.
2- As a result of nasal obstruction and as the child at birth is obligate nasal breather; the child will demonstrate cyclical change in oxygenation, becoming cyanosed during quiet periods (because the mouth is closed) and normal pink color return when the child cries.
Choanal atresia may be associated with the so called CHARGE association:
C → colobomatous blindness.H → heart disease.
A → atresia of choana.
R → retardation of growth.
G → genital hypoplasia in males. E → ear deformities.
Diagnosis:
1- Mirror test (total absence of nasal airflow, no condensation occurs on a cold metal surface held close to the nostrils).2- Plastic catheter: cannot be passed through the nose to nasopharynx.
3- Cotton wool held close to nostrils → no movement of the cotton.
4- Air blown into the nostril through closely fitting tube is not heard to enter the pharynx.
5- CT scan: to see the thickness of bony atresia.
6- Contrast radiography: a radio opaque substance instilled into the nose does not reach the nasopharynx.
Treatment:
Emergency treatment: is needed in bilateral atresia to maintain airway by neonatal waters airway and then either by tracheostomy or endo-tracheal intubations.Definitive treatment: is by surgical removal of the atretic plate by:
1- Trans-nasal approach (used when atresia is membranous or thin bony plate)
2- Trans-palatal approach (used when atresia is thick bone).
3- Trans-septal approach.
4- Trans-antral approach
2- Congenital Nasal Masses:
Which include:
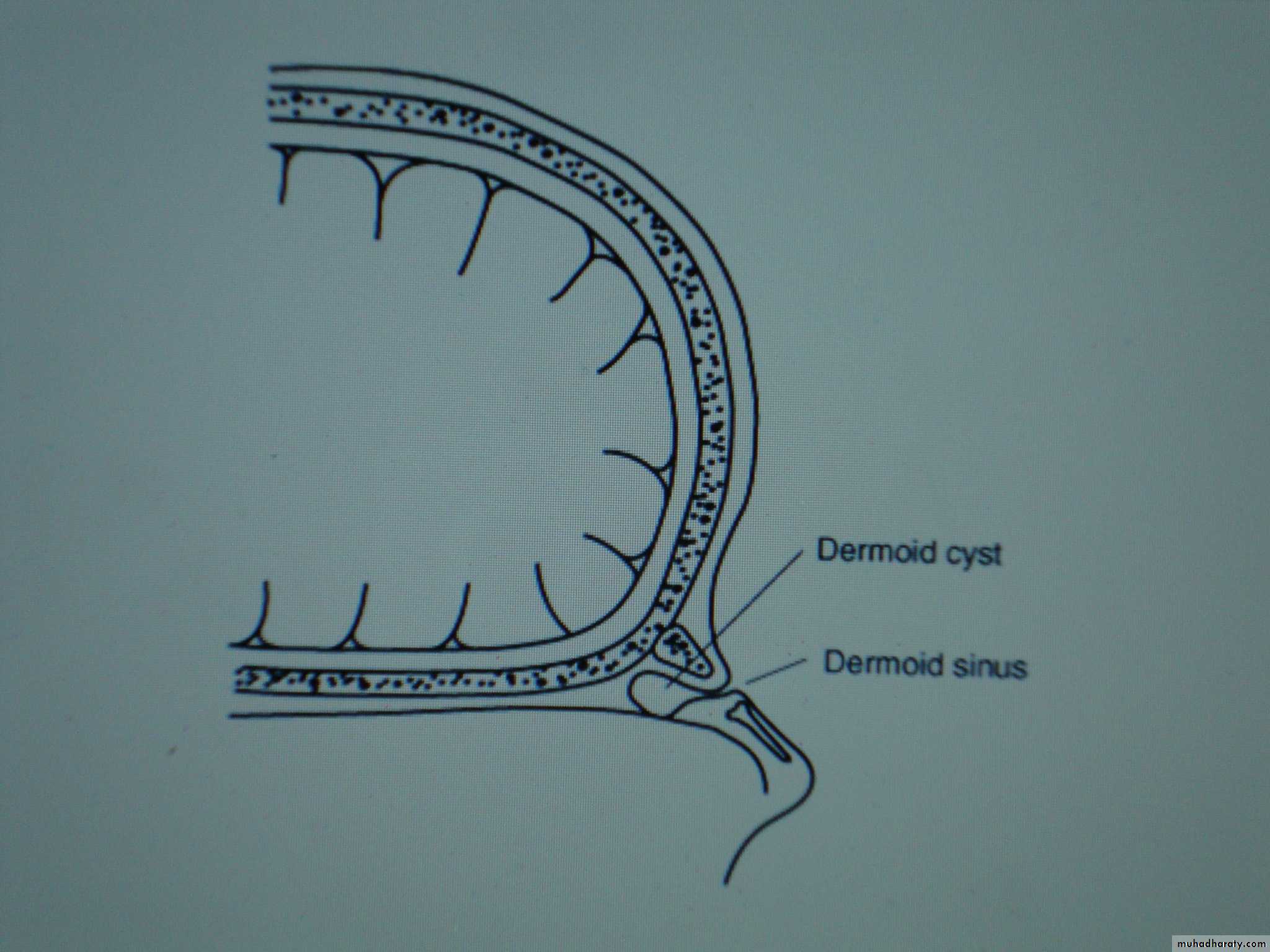
A- Nasal Dermoids: Dermoids are formed as a result of sequestration of epithelial elements during fusion of the median nasal process. They present as solid masses or cysts, occurring anywhere in the midline of the nose. They may also present as sinuses recognized by minute opening sometimes containing single hair.
Treatment is by surgical excision of both sinuses with hair.
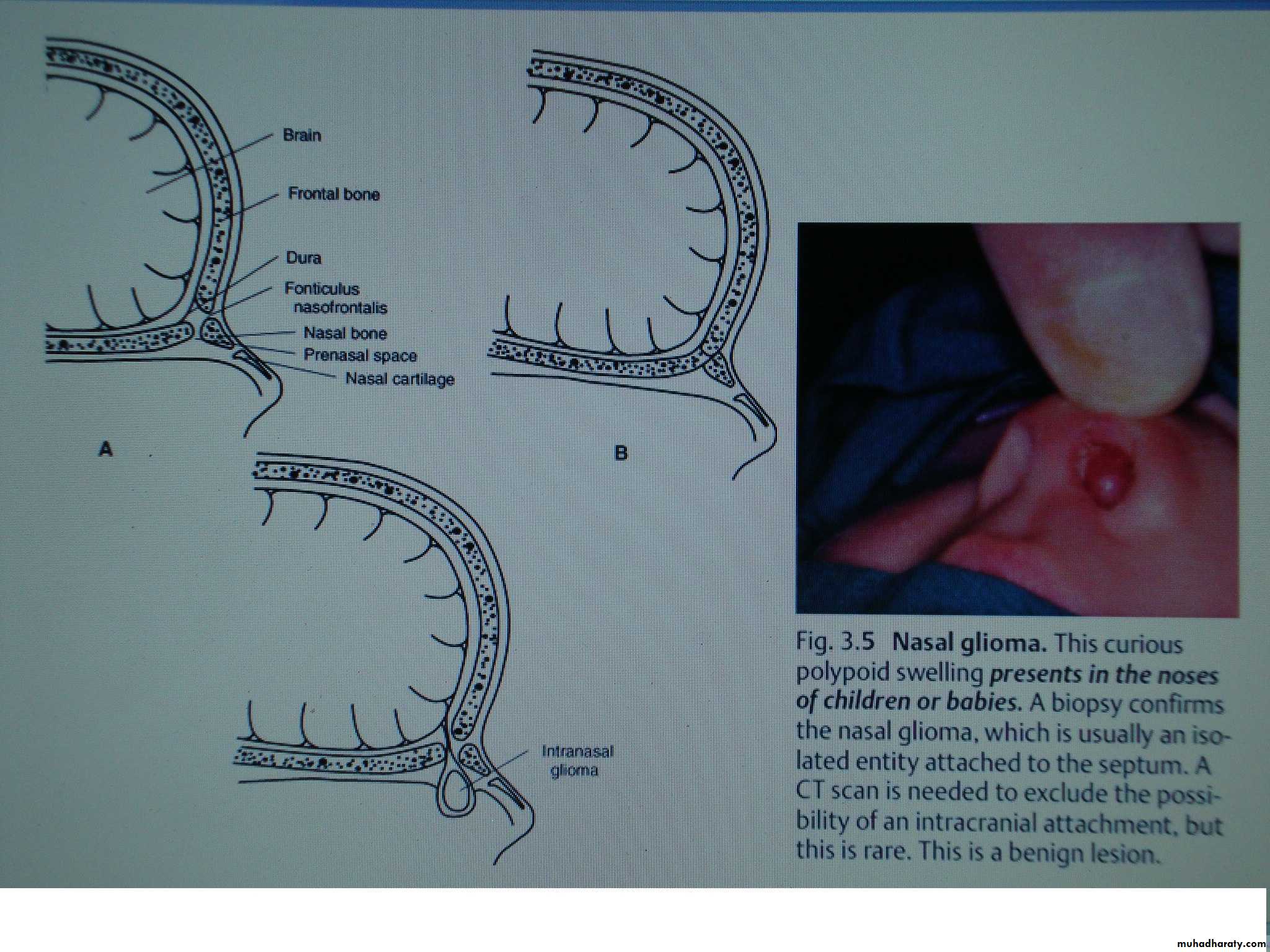
B-Nasal Glioma:
Usually diagnosed by or seen after birth. It could be extranasal (60%). Presented as subcutaneous mass to one side of nasal bridge. Or intranasal (30%) causing nasal obstruction or in combination (Both extra and intra-nasal (10%)).Treatment is by surgical excision.
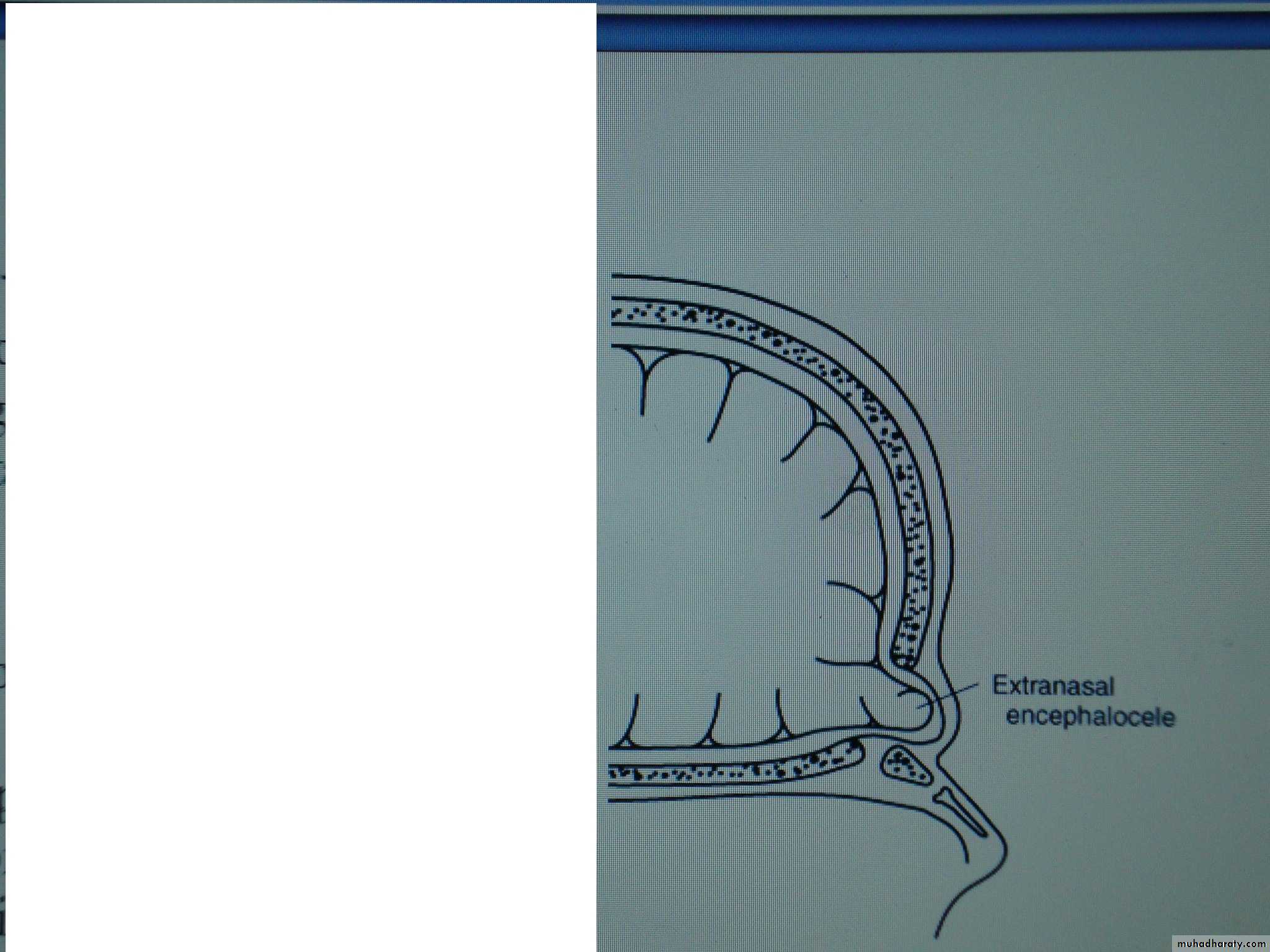
C- Nasal Meningo-encephaloceles.
There are local herniation of glial tissue & meninges through a defect in the skull. They contain CSF so injury to them may cause CSF rhinorrhoea & meningitis.They are connected to intracranial cavity, so they increase in size during crying. It may present as a cystic mass over the root of the nose or intranasal mass. CT scan is necessary to show the exact size of the bony defect.
Treatment is by surgical excision.
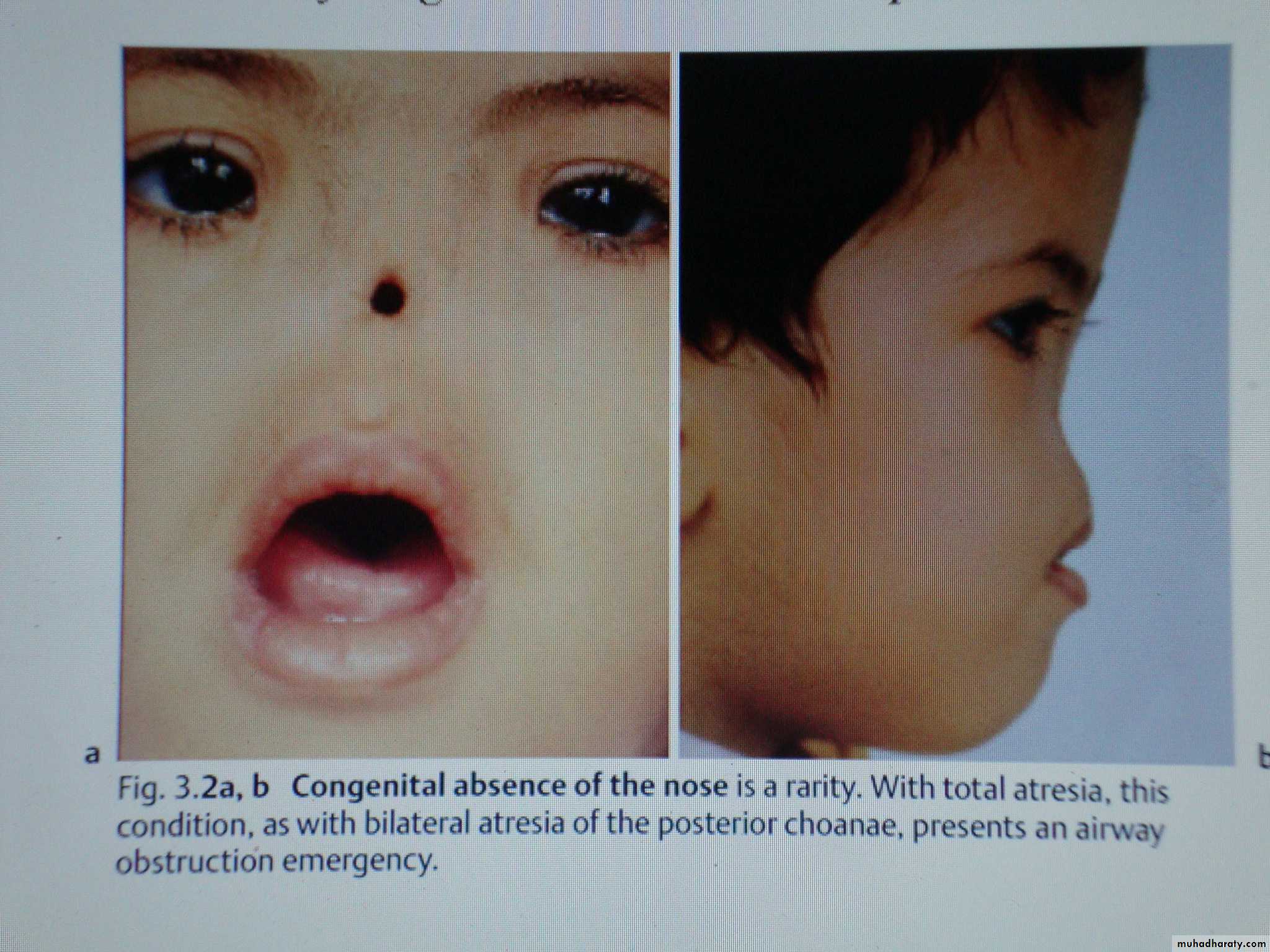
3- Agenesis of the Nose: includes:
Total agenesis → total absence of the nose.Partial agenesis → absence of one nasal cavity.
Treatment is by surgical reconstruction or prosthesis.
4-Cleft Nose:
Cleft nose ranges from minor notching of the nasal tip to total midline division of the nose into separated nasal cavities. It's associated with cleft lip or palate.Treatment is by surgical reconstruction.
Nasal trauma
Fractures of the noseSeptal Haematoma
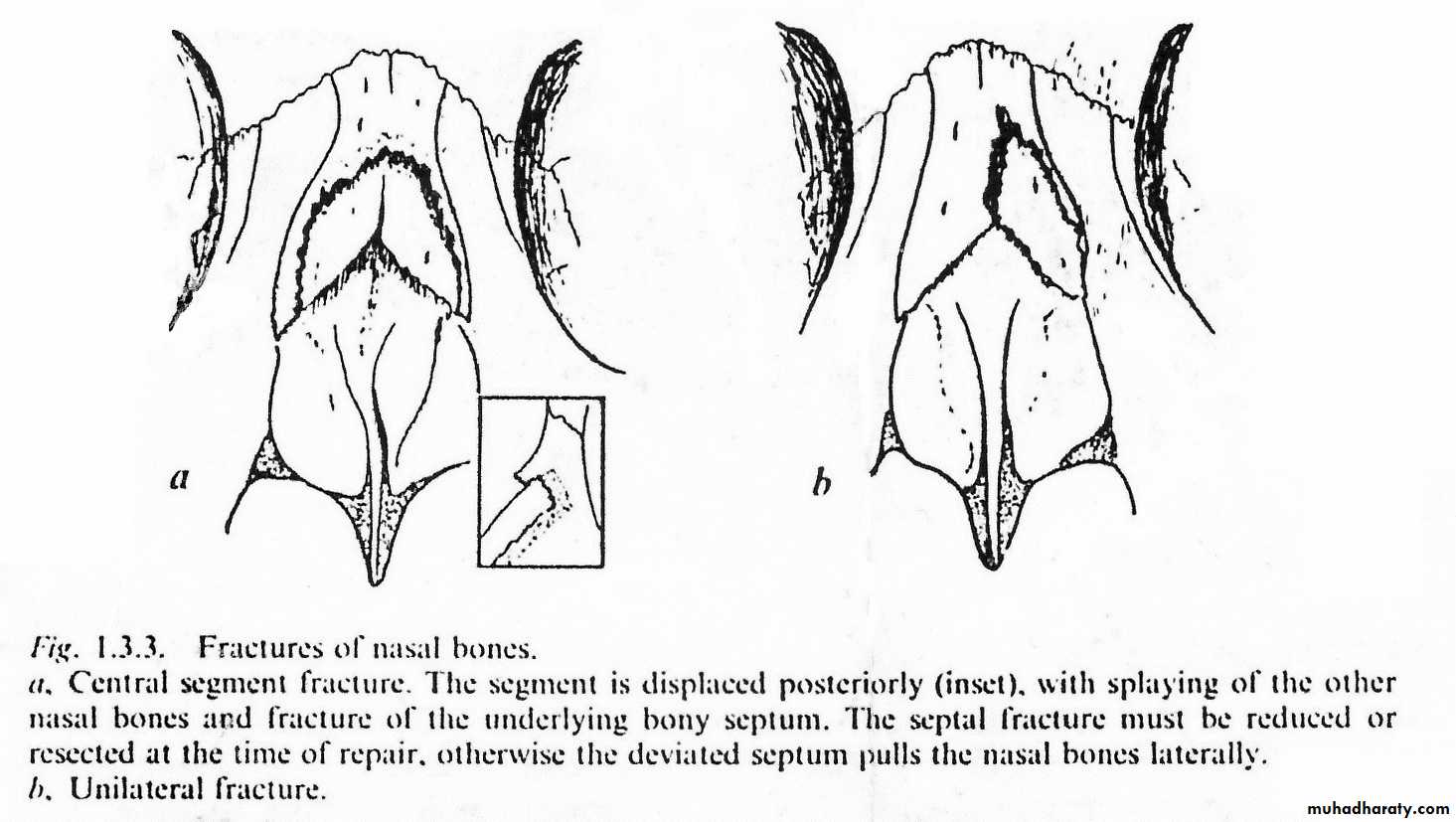
Fractures of the nose:
Classification:
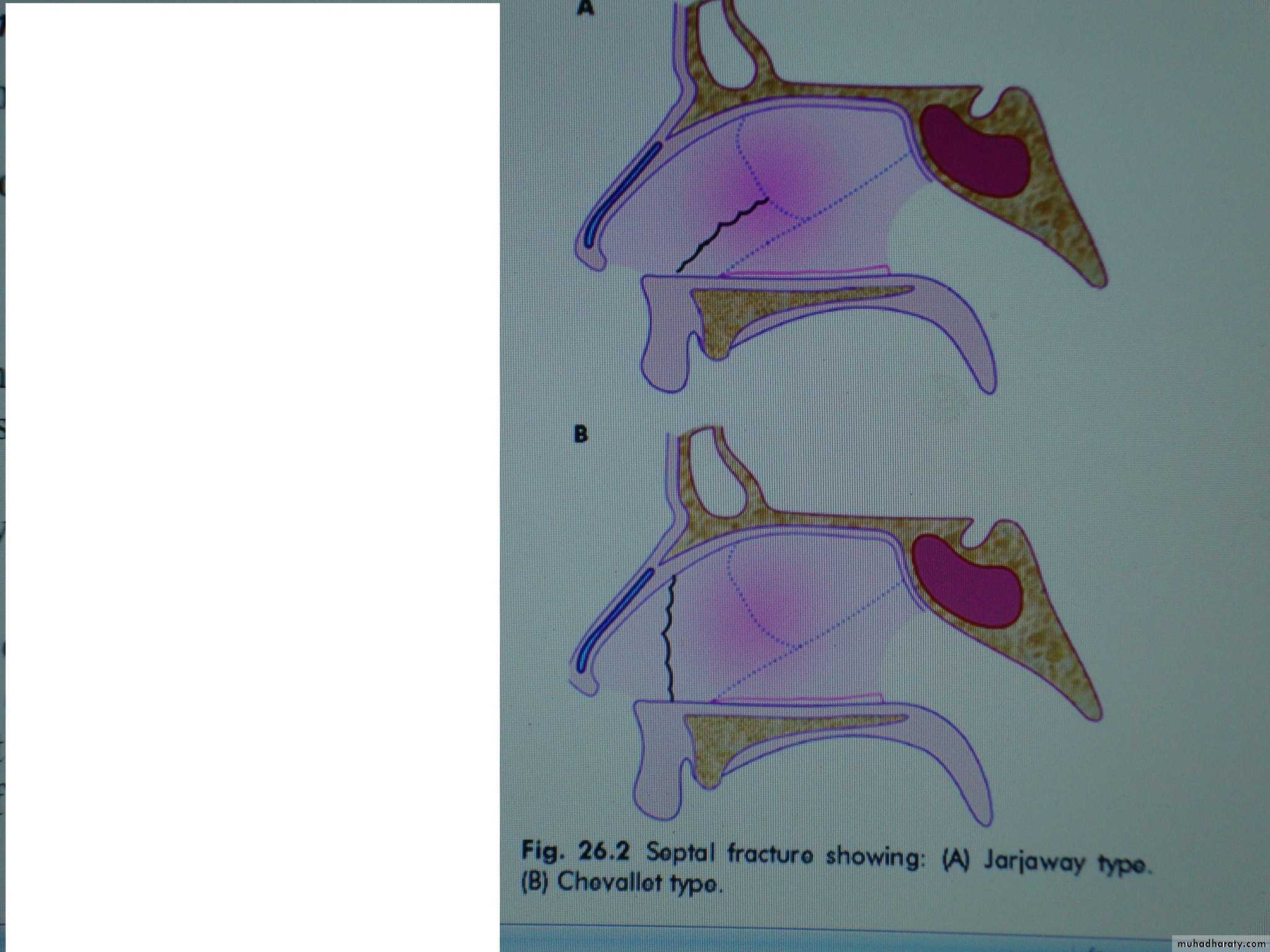
Type 1:
Due to frontal or fronto-lateral blow. There is vertical fracture of the nasal septum (Chevallet fracture which runs from the maxillary spine to the nasal bones).
The thin distal portion of the nasal bone is depressed or displaced. Chevallet fracture occurs in severe variant of type 1.
Type 2:
Due to lateral trauma, there is (Jarjaway fracture) which is C shaped fracture of the perpendicular plate of ethmoid and the quadrilateral cartilage. The nasal bones are displaced laterally but no gross depression. Also there is fracture of the frontal process of maxilla.Type 3:
Due to high velocity trauma, there is involvement of the orbito-ethmoidal complex. There is gross depression, the perpendicular plate of ethmoid rotate backward which result in forward directed nostrils (pig-like appearance).
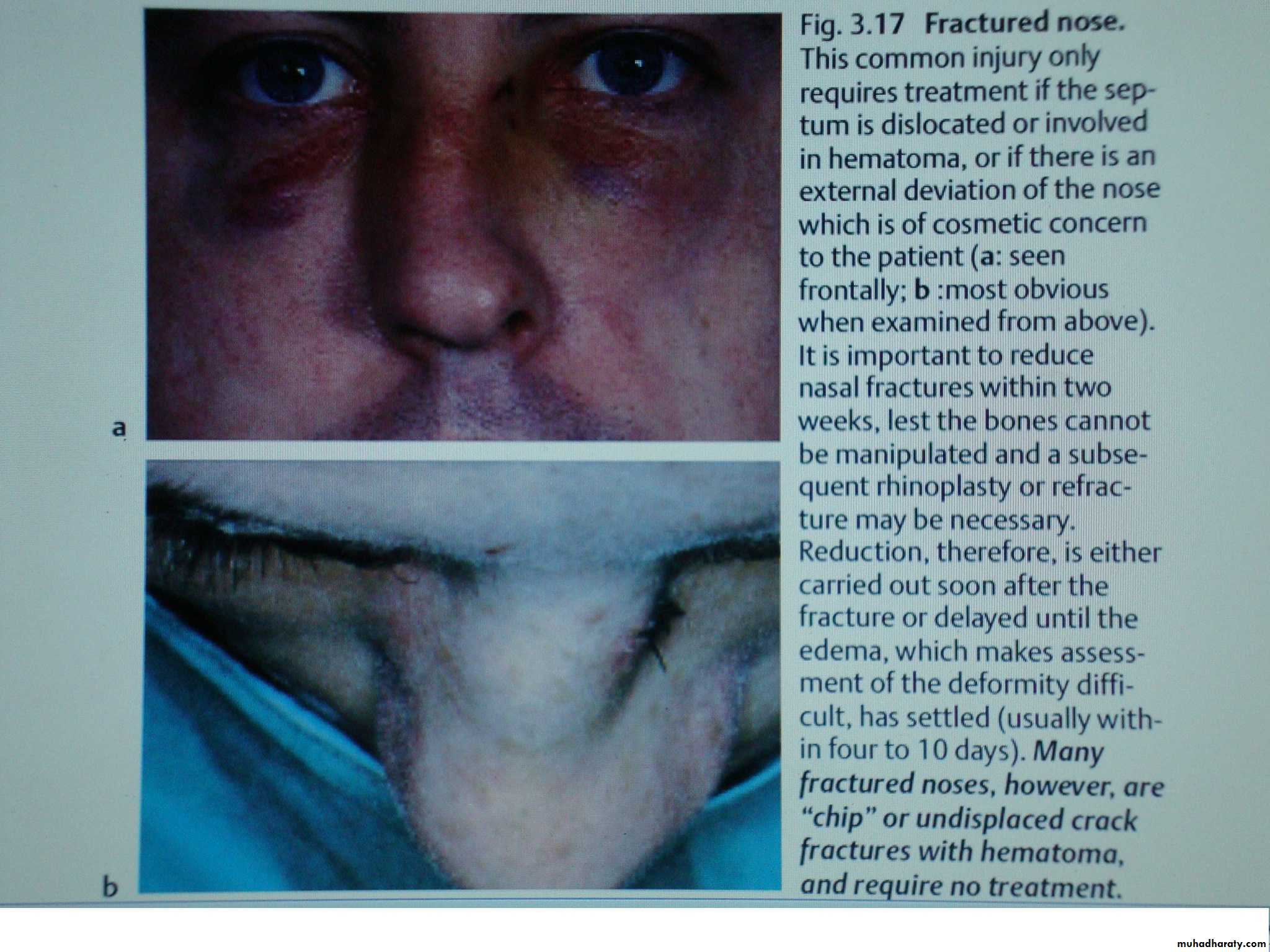
Clinical features:
Deformity →External swelling.
Black eye.
Pain.
Epistaxis.
Nasal obstruction
Diagnosis:
X-ray of nasal bone (lateral view). It is important medicolegally, but is of little value clinically.
Treatment:
If the patient presented early before swelling appears, we reduce the fracture immediately or reduce it after 5−7 days. If the patients presented with swelling over the nose, then we have to leave him as the facture is reduced after 5−7 days. If the patient is presented with new nasal bone fracture and has history of previous external nasal deformity, then the best treatment is septo-rhinoplasty at later phase of the patient's life. When the fracture is left to be reduced after 5−7 days we have to give topical vasoconstrictor to improve the nasal airways and analgesia.In type 1 fracture reduction by digital pressure or Walsham's forceps or an elevator is enough.
In type 2 fractures we need to reduce the nasal bone fracture by Walsham's forceps and reduce the septal fracture by open reduction through Killian incision.
In type 3 fracture we need open reduction and internal fixation.
Complication of nasal bone fracture:
Deformity and nasal obstruction.CSF leaks.
Orbital complication:
Telecanthus.
Epiphora due to damage to the lacrimal ducts.
Septal haematoma.
Septal deviation.
Anosmia.
Notes:
Walsham's forceps consists of one prong which is inserted into the nostril and the other prong which is rubber covered and placed on the external aspect of the skin overlying the nasal bone and the bone are then mobilized and reset.
After reduction we do nasal packing and external supporting by POP.
Asche's forceps (sometimes used to correct septal fracture) consists of 2 parallel prongs placed on either side of the septum and then the septum manipulated into normal position.
When the patient is presented with a history of nasal bone trauma and fracture for more than 2 weeks → the fracture needs osteotomies to be reduced (the fracture cannot be reduced by using Walsham's forceps).
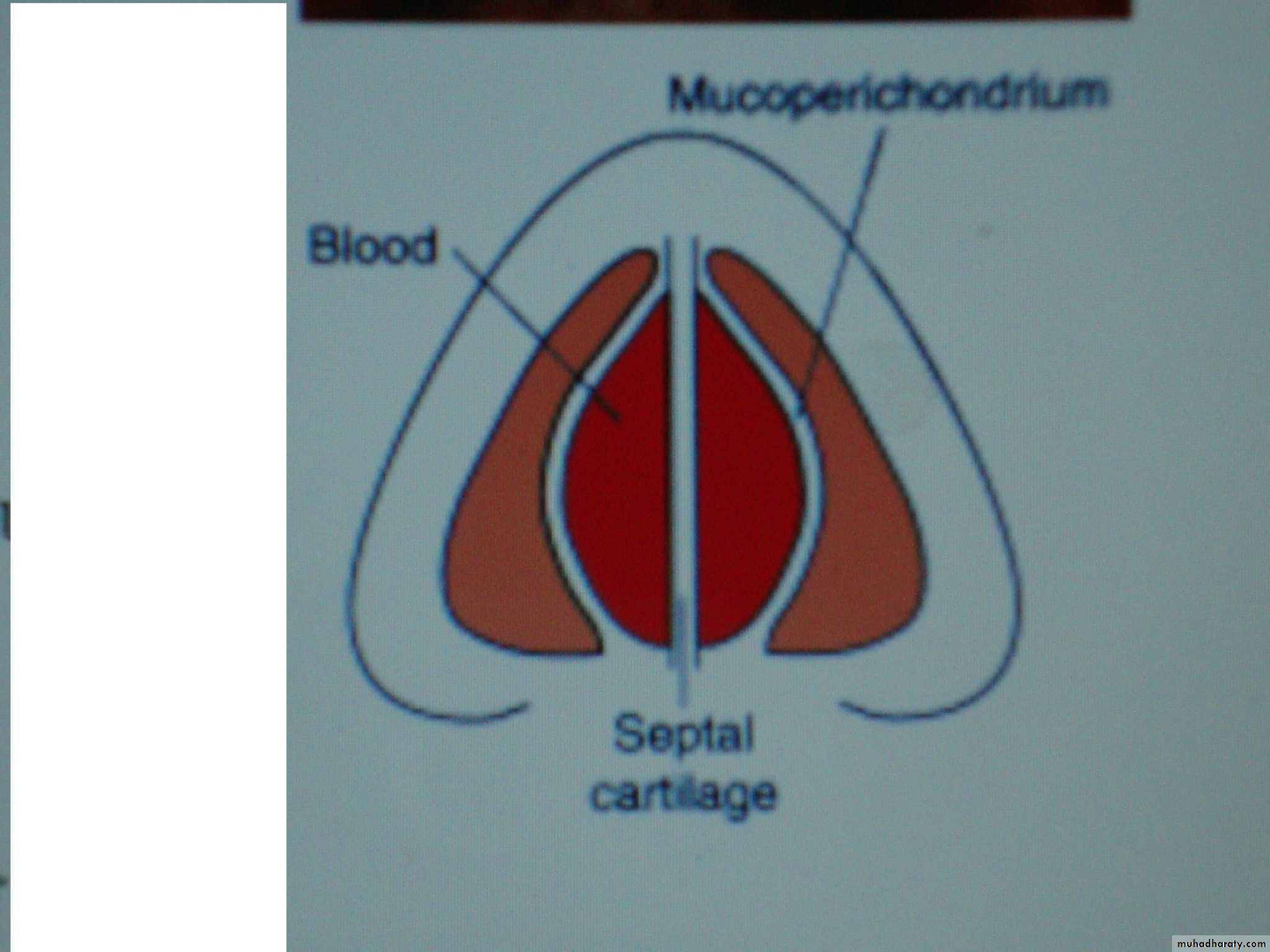
Septal Haematoma:
Definition:Collection of blood beneath muco-perichondrium &/or periosteum of nasal septum.
Aetiology:
Septal haematoma occurs due to trauma and may be associated with nasal bone fracture.
Pathology:
Submucasal blood vessels are torn and the mucosa remains intact resulting in haematoma formation.There may be septal fracture and the blood pass from one side to other side resulting in bilateral haematoma. The blood accumulates in the subperi-chondrial layers interfere with the vitality of the cartilage → cartilage necrosis → saddle nose, so that the haematoma should be treated immediately.
Also the collagenases enzymes increase the rapidity of cartilage necrosis.
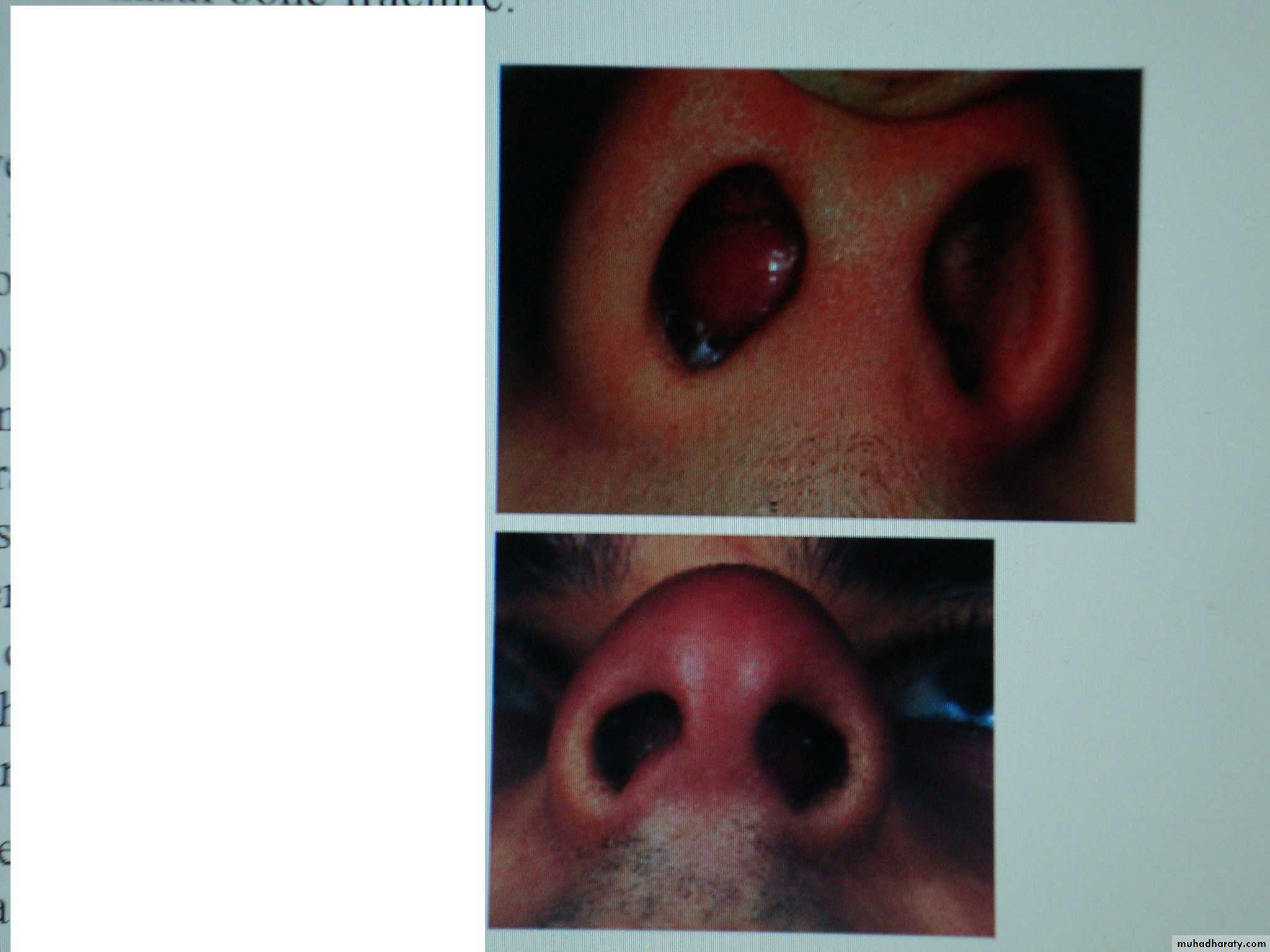
Symptoms and signs:
Nasal obstruction.
Discomfort.
On examination there is smooth rounded bilateral septal swelling.
Treatment:
Early surgical drainage of the haematoma to reduce the risk of cartilages necrosis by using hemitransfixation incision, suction of the blood, put drain and then packing of the nose.Aspiration in early small haematoma under aseptic technique by wide bore needle may be repeated.
Antibiotic to prevent infection.
Complications:
External nasal deformity.→ Saddle nose (because the septal cartilage support the nasal dorsum).
→ Affection of facial growth.
Septal thickening.
Septal abscess: due to infection of haematoma, clinically there is fever and increasing pain treated by surgical drainage.
Septal perforation due to necrosis of the cartilage.
Intracranial spread of infection:
Cavernous sinuses thrombosis.
Meningitis.
Brain abscess.