
Antidepressant Drugs
Dr. Hussain Adday Aljabery
M.B.Ch.B . M.Sc. FICMS ( RAD. )
Pharmacology
DEPRESSION
Types
Symptoms
Diagnosis
Causes
Treatment
TYPES OF DEPRESSION
Major depression
Chronic depression (Dysthymia)
Atypical depression
Bipolar disorder/Manic depression
Seasonal depression (SAD)

SYMPTOMS
persistently sad, anxious, or empty moods
loss of pleasure in usual activities (anhedonia)
feelings of helplessness, guilt, or worthlessness
crying, hopelessness, or persistent pessimism
fatigue or decreased energy
loss of memory, concentration, or decision-making capability
restlessness, irritability
sleep disturbances
change in appetite or weight
physical symptoms that defy diagnosis and do not respond to
treatment (especially pain and gastrointestinal complaints)
thoughts of suicide or death, or suicide attempts
poor self-image or self-esteem (as illustrated, for example, by
verbal self-reproach)
DIAGNOSIS
Extensive patient and family history
Blood test for hypothyroidism
Current medication
DSM-IV
One of the first two symptoms
Five other symptoms

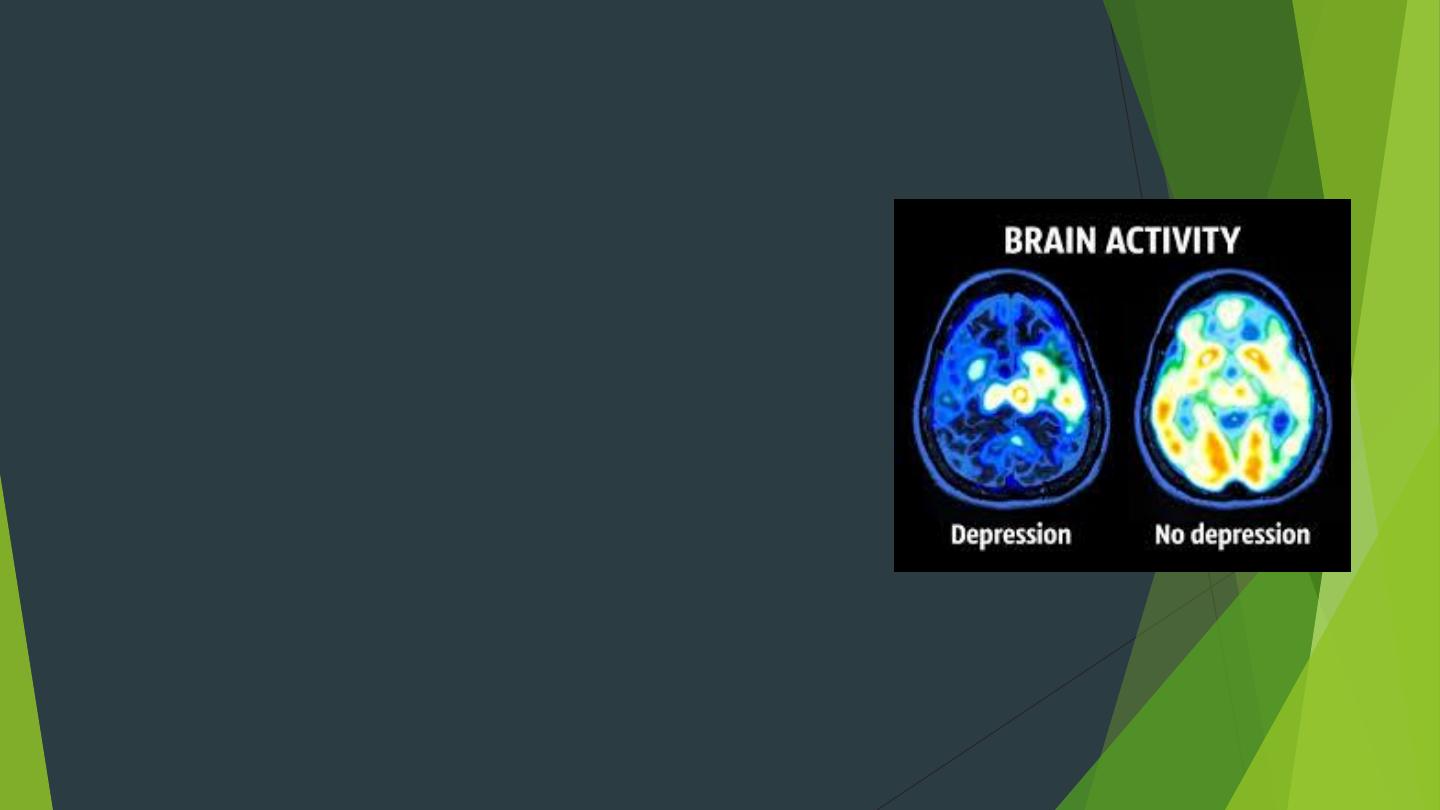
CAUSES OF DEPRESSION
Genetics
Death/Abuse
Medications
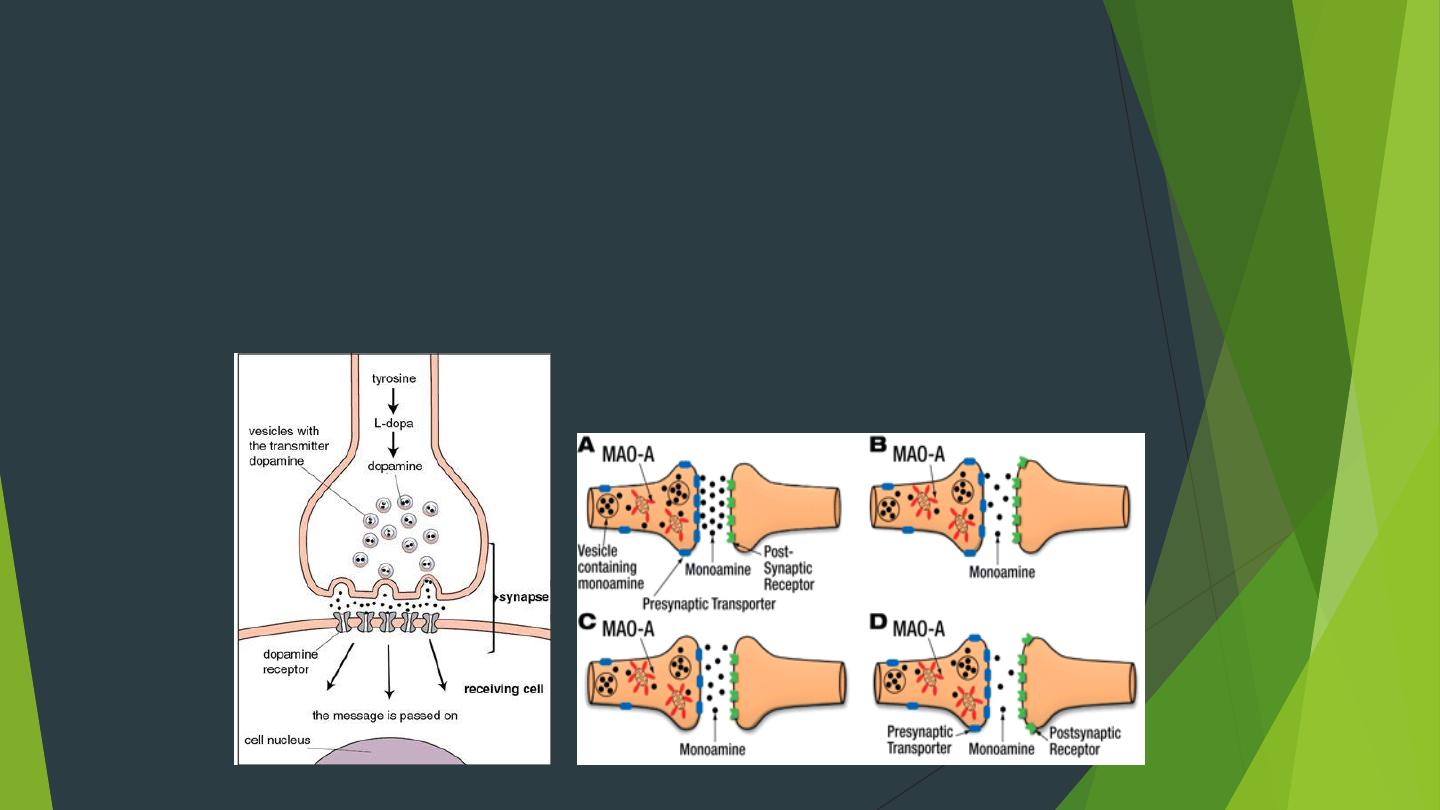
NEUROTRANSMITTERS AND THE
CATECHOLAMINE HYPOTHESIS
Neurotransmitters pass along signal
Smaller amount of neurotransmitters causes depression
TREATMENT FOR DEPRESSION
Psychotherapy
Electroconvulsive therapy
Natural alternatives
Medication
SSRIs
MAOIs
TCAs
SNRIs
NDRIs
TeCAs

Basic information
Depression is disorder of mood rather than disturbance of thought or cognition. It is
postulated that depression is due to deficiency of
NA
and/or
5-HT
in the CNS while mania
results from functional excess. Psychic depression is characterized by both emotional and
biological symptoms.
Recent studies suggest t that overactivity of post-synaptic c 5-HT2A receptors in some brain
areas is s involved in the pathogenesis of depression and psychosis
Unipolar depression
(major depressive disorder): more common, may bee reactive (70% ) or
endogenous (25%), characterized by low mood and loss of interest or pleasure in normally
enjoyable activities in normally enjoyable activities t.
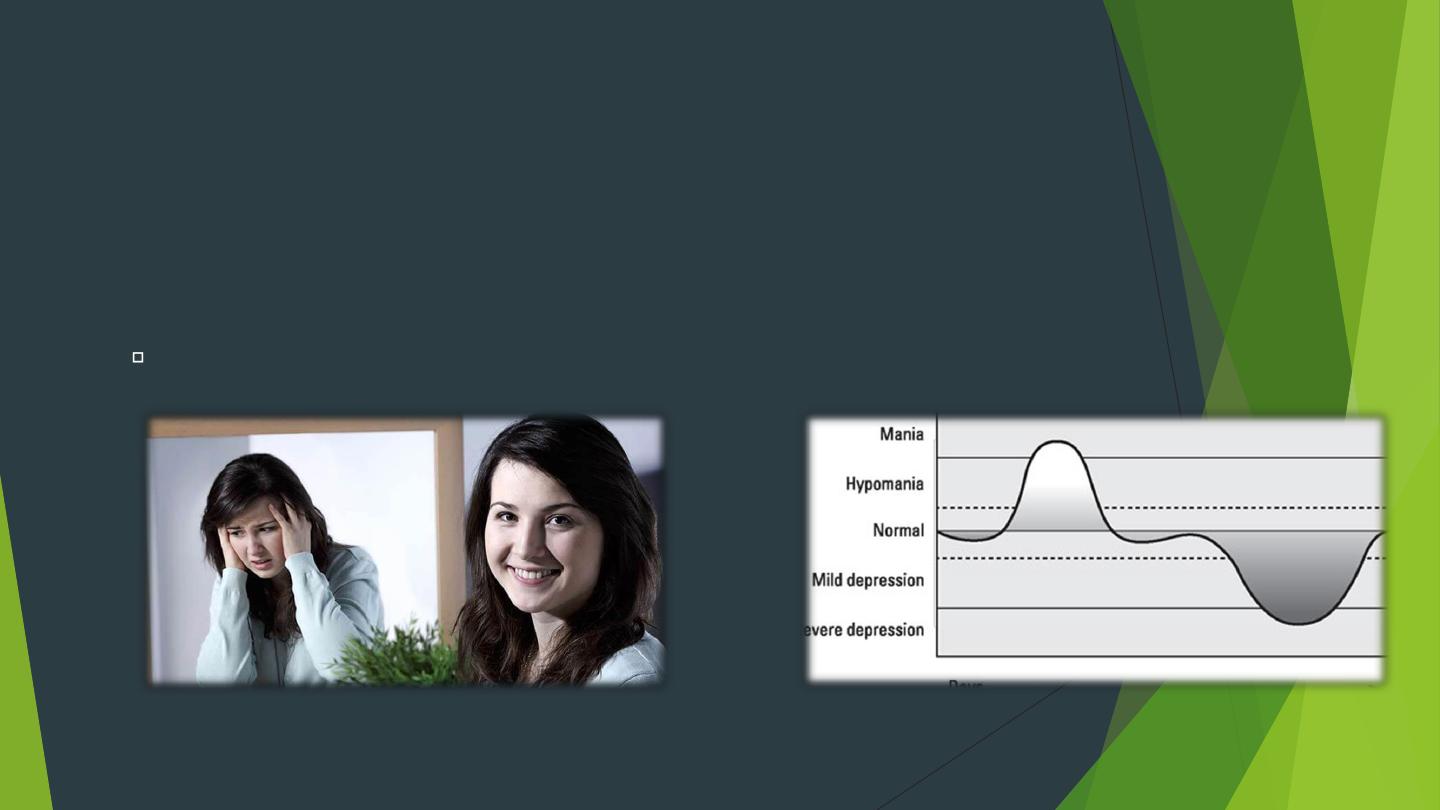
Bipolar depression
(manic-depressive disorder): less s common, characterized by
oscillating periods of depression and mania. There is strong hereditary origin. The
therapeutic effect occurs only y after 2-3 weeks of drug u administration s and is more
closely associated with adaptive changes in neuronal receptors and brain neurotropic
factors.

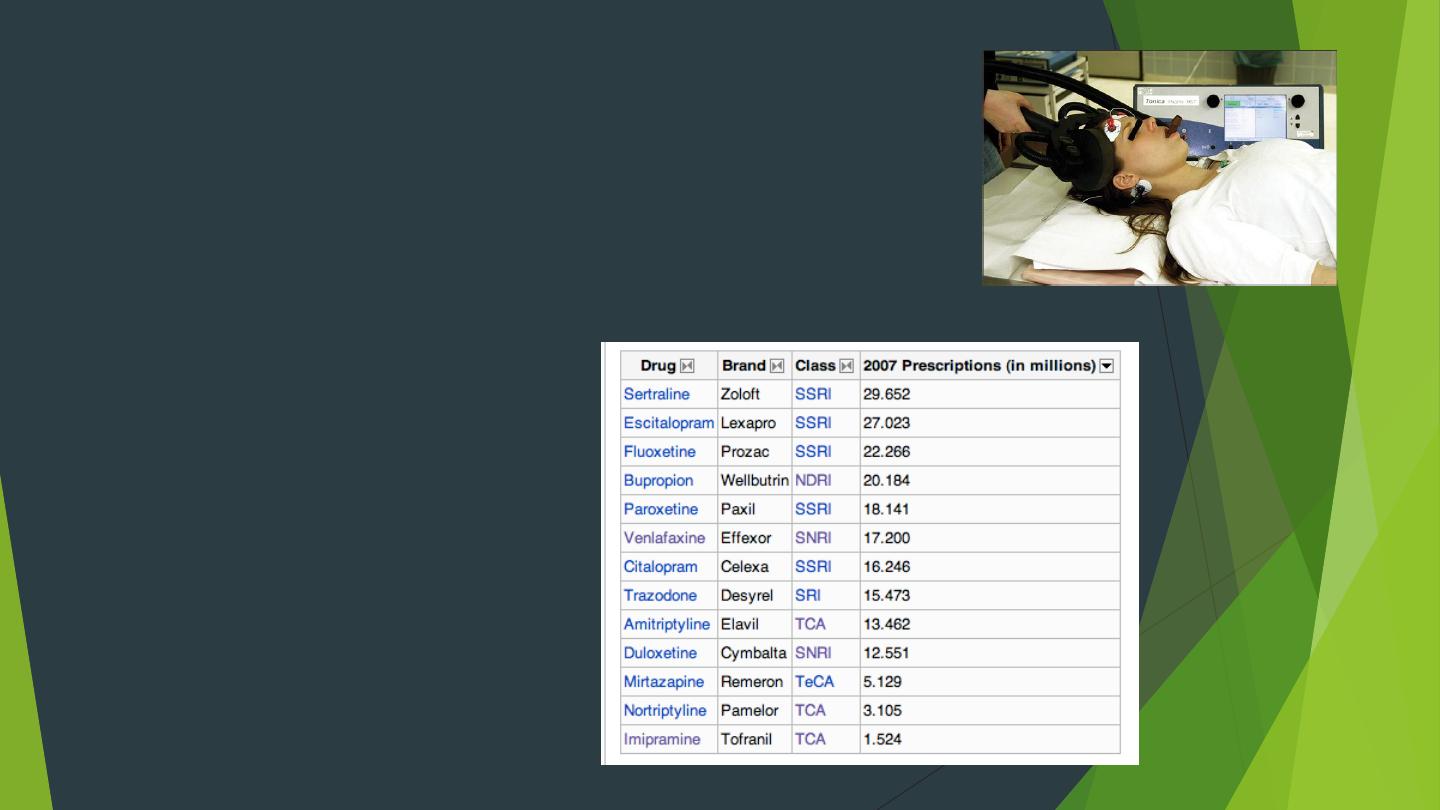
Classification of antidepressant drugs :
Tricyclic antidepressants (TCA )
e.g. imipramine, amitriptyline .
Selective serotonin reuptake inhibitors (SSRI
): e.g. fluoxetine , sertraline.
Atypical heterocyclic antidepressants
: e. g. maprotiline, trazoddone.
Monoamine oxidase inhibitors (MAOI)
e. g. clorgyline , selegiline
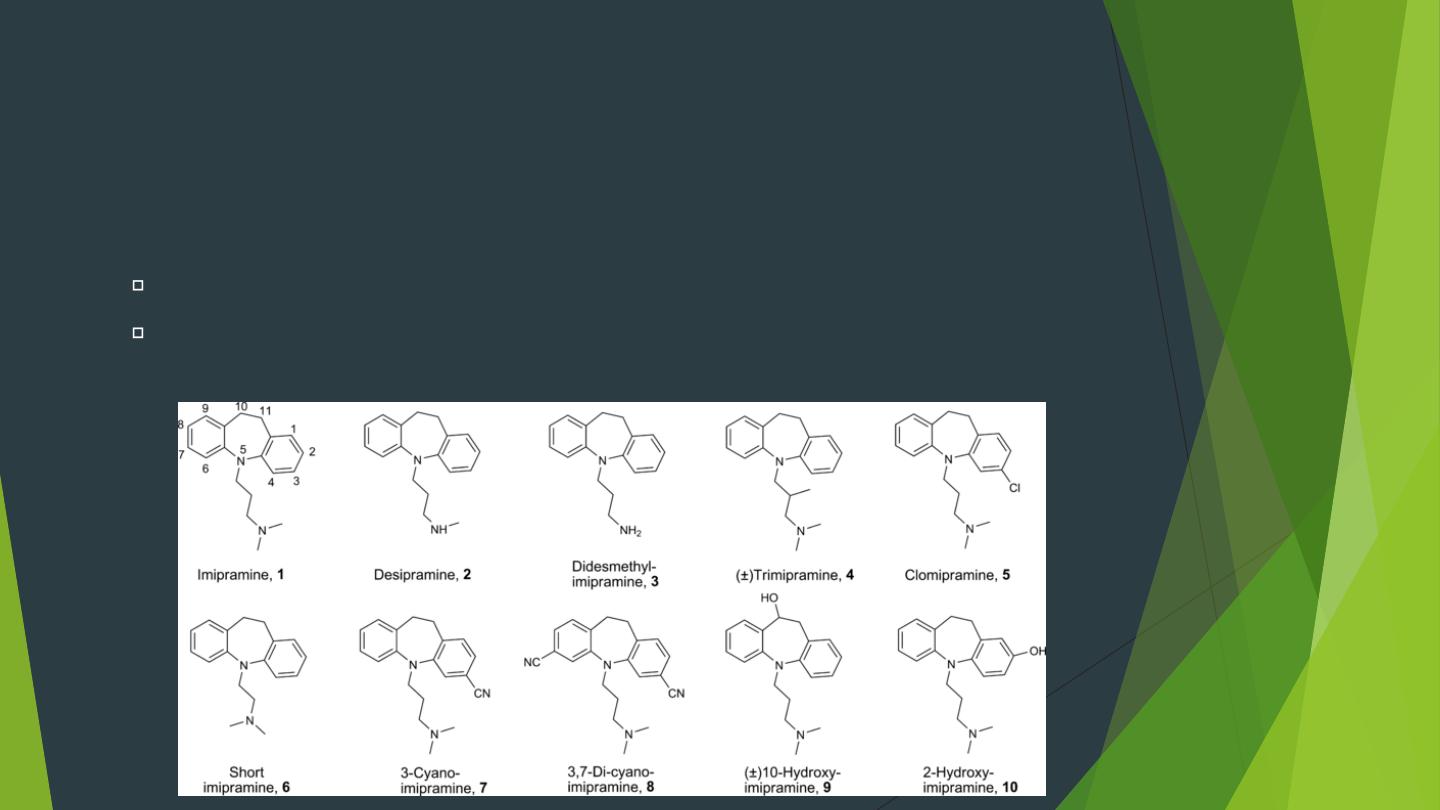
Tricyclic antidepressants (TCA)
Imipramine, Desipramine, Clomipramine, Amitriptyline,
Nortriptyline
Pharmacokinetics
They are well absorbed after oral administration. They have
large Vd
.
Most TCA have
long t1/2
because they are metabolized into active
metabolites and undergo enterohepatic cycling.
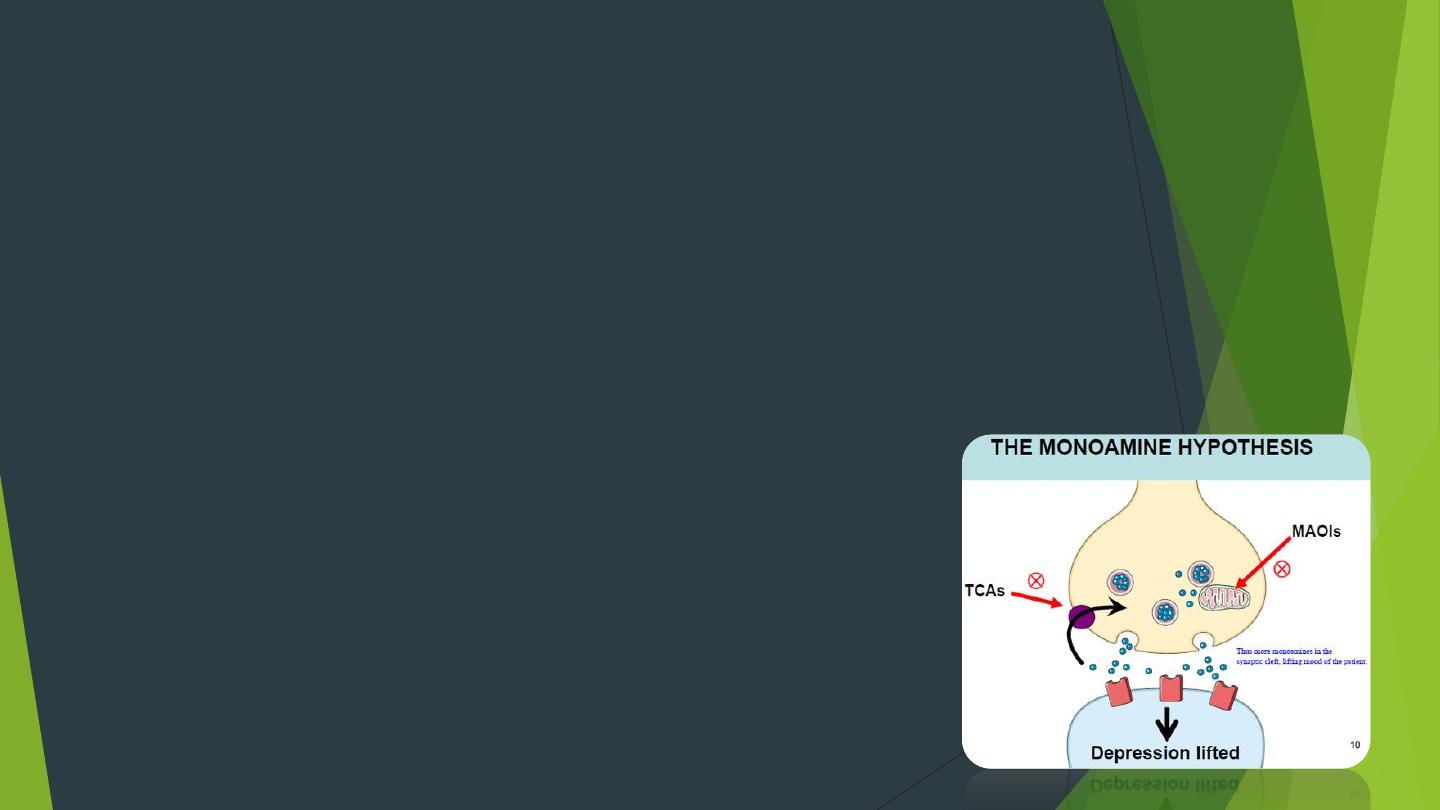
Mechanism of action: (inhibition of the
amine pump)
TCA inhibit neuronal reuptake of both 5-HT & NA leading to their
accumulation in synaptic spaces and the brain tissue.
It has been suggested that improvement of the
emotional
symptoms is
related to enhancement of
5-HT
transmission while improvement of
biological
symptoms is related to enhancement of
NA
transmission.
Elevation of mood in depressed patients occurs after 2-3 weeks
Therapeutic uses
Major depressive disorder.
Nocturnal enuresis in children (imipramine).
Chronic pain syndromes, neuropathic pain, and prophylaxis of migraine
(unclear mechanism).

Adverse effects
Sedation
is common at the start of therapy but tolerance develops later. It
may be due to antagonism with histamine H1 and/or muscarinic receptors.
CNS troubles
: memory dysfunction, agitation, seizures, and suicidal thoughts.
Atropine-like action
: very common - dry mouth, blurred vision, urine
retention, etc.
Orthostatic (postural) hypotension
: due to peripheral α1 receptor blockade.
Cardiac arrhythmias
: tachycardia, widening of QRS, and ↑ QT interval.
Hepatotoxicity
: cholestatic hepatitis.
Weight gain.

Drug interactions
Toxic synergism with
MAOIs
and
SSRIs
(irritability and convulsions).
TCA antagonize the antihypertensive effect of
clonidine
and
methyldopa
.
TCA have additive
anticholinergic effect
with other drugs having
anticholinergic activity
TCA overdose
Metabolic acidosis
Atropine-like effects
Cardiac arrhythmia
Management
IV NaHCO3 (1st step).
IV lidocaine
Dialysis is ineffective

Selective serotonin reuptake inhibitors (SSRIs)
Fluoxetine, Paroxetine, Sertraline, Citalopram, Escetalopram
They are the most commonly prescribed antidepressants due to their limited
toxicity. They are also used for some other psychiatric disorders.
Sertraline is the preferred antidepressant following myocardial infarction as
there is more evidence for its safe use in this situation than other
antidepressants.
When stopping an SSRI the dose should be gradually reduced over a 4 week
period, this reduces the risk of relapse.

Mechanism of action
They selectively block 5HT reuptake leading to accumulation of 5-HT in brain
tissue.
Their effect appears after 2-3 weeks like other antidepressants.
Therapeutic uses
Major depressive disorder.
Obsessive-compulsive disorder (OCD).
Anxiety disorders (generalized anxiety disorder, social phobia, panic
disorder).
Adverse effects
–
GIT irritation
is the most common side effect. A proton pump inhibitor
should be prescribed if a patient is also taking a NSAID to avoid GIT bleeding.
–
Sedation or insomnia
at the start of therapy but tolerance develops later.
–
Muscle cramps
and twitches.
–
Sexual dysfunction
in up to 40% of patients – the main cause of
noncompliance.
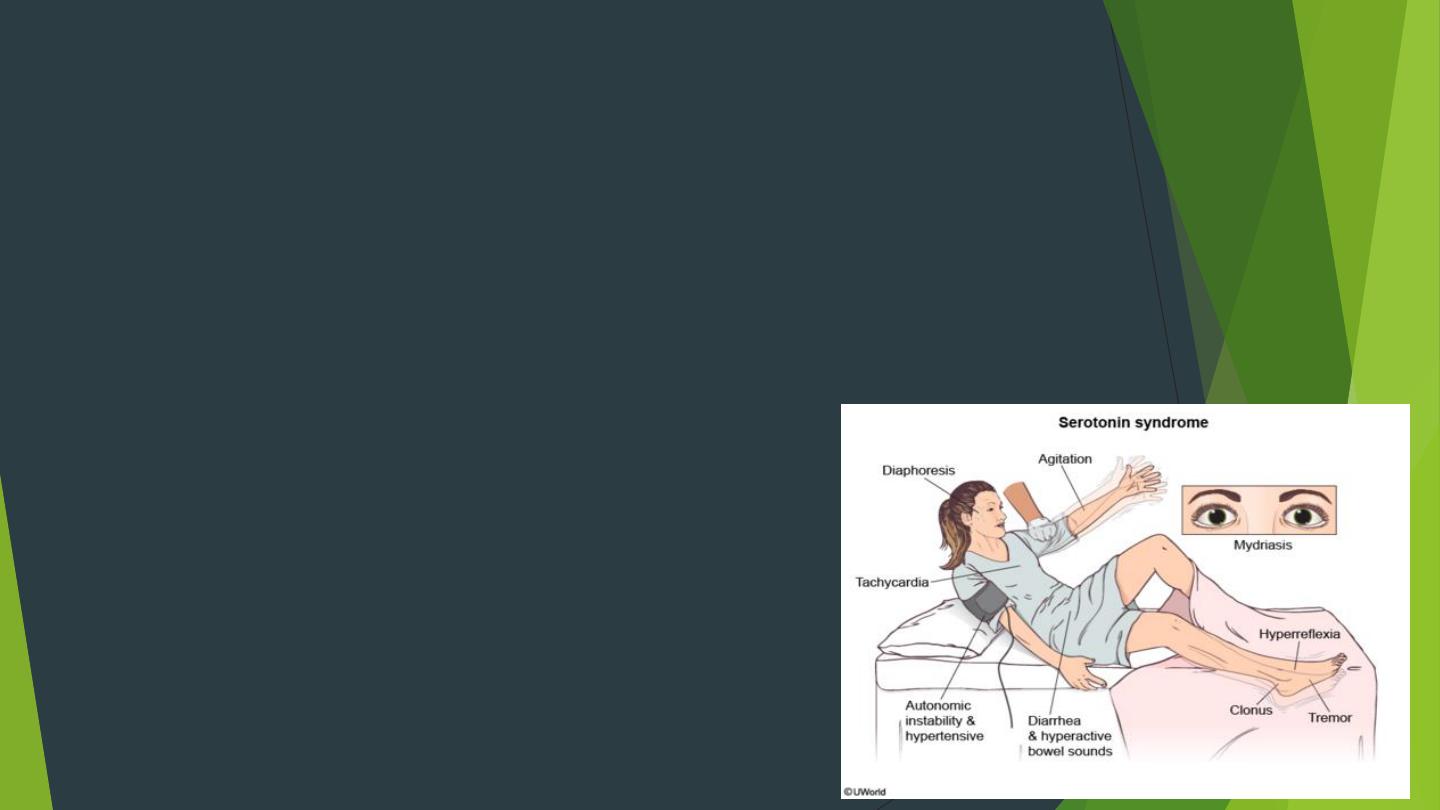
– Dangerous
“serotonin reaction”
may occur if given with MAOIs or TCA
(hyperthermia, muscle rigidity, cardiovascular collapse).

Atypical antidepressants
The pharmacological properties of atypical heterocyclic antidepressant agents
are similar to those of TCAs.
Mechanism of action
Trazodone: blocks mainly 5HT2A receptors in addition to H1, and α1
receptors.
It is highly sedating and can cause postural hypotension.
Mertazapine: blocks mainly 5HT2A receptors in addition to H1, and α2
receptors. It causes weight gain.
Maprotiline: selective blocker of NA reuptake. It is highly sedating and can
cause seizures.

Monoamine oxidase inhibitors (MAOIs)
Clorgyline, Selegiline, Pargyline, Moclobemide
Mechanism of action
They inhibit MAO enzyme leading to accumulation of active monoamines
(NA, 5-HT, dopamine) in neuronal tissue.
Most MAOIs are irreversible inhibitors. Recovery of MAO takes several
weeks. Moclobemide is a reversible inhibitor

Therapeutic uses
Major depression
: they are not used as a first-line, but usually reserved as a
last line after other classes of drugs have failed.
Selegiline
(selective MAO-B inhibitor) is used for treatment of Parkinsonism.
Adverse effects
–
CNS stimulation
: irritability, insomnia, tremors, hyperthermia, convulsions
–
Hepatotoxicity
: occurs more with the old members.
–
Orthostatic (postural) hypotension
and
sexual dysfunction

Interactions
Drug-drug interactions:
– Toxic synergism with tricyclic antidepressants and SSRIs.
– Potentiation of sympathomimetics (including cold remedies & nasal
decongestants).
Drug-food interactions: Hypertensive crisis (cheese reaction):
–
Tyramine
is an indirect sympathomimetic present in some food and normally
metabolized by MAO-A in the liver.
– When the patient takes MAO-A inhibitor or non-selective MAOIs, severe
hypertension can occur after eating tyramine-rich food e.g. fermented
cheese, yogurt, beer, herrings.
–
Treatment
: by giving combined α + β blockers (prazosin + propranolol).

N.B. There are 2 isotypes of MAO
enzyme:
MAO-A enzyme
– Present in the cytoplasm of neurons (CNS) and peripheral tissues (e.g. liver).
– It acts non-specifically on NA, 5- HT, and dopamine.
– Clorgyline is a specific inhibitor.
MAO-B enzyme
– Present mainly in the CNS and acts more on dopamine.
– Selegiline is a specific inhibitor.
Mood Stabilizing Drugs (treatment of
mania bipolar disorder)
Sodium valproate
is the only specific antimanic agent g and is the treatment
of choice in the acute stages .
Lithium
is the drug of choice for long-term .

Lithiumm carbonate
Mechanism of action
It ↓ cAMP in neuronal cells and ↓ NA release → ↓ neuronal firing f.
It inhibits many metabolic processes in the nerve tissue.
Therapeutic uses
Treatment of mania ( (valproate is the 1st choice).
Treatment a of
manic-depressive disorder
( bipolar depression). It is given
in the manic phase while TCA or SSRIs are given in the depressive phase.

Adverse effects
Lithium h has a very
narrow therapeutic index
, monitoring of plasma levels is
essential .
It has a
long plasma a half-life
being excreted entirely by the kidneys.
Toxicity may be precipitated by dehydration , renal failure, diuretics
(especially thiazide ) or ACE inhibitors .
– Anorexia, nausea , vomiting t and diarrhea.
– Nephrogenic
diabetes insipidus
leading to polyuria a and thirst.
– Hypotension and cardiac arrhythmia .
–
Thyroid
dysfunction
–
Fine tremors (
coarse tremors are seen with toxic levels).
– Teratogenicity.

Edith Lake Wilkinson (August 23, 1868
– July 19,
1957) was an artist who lived and painted
in
during the early
decades of the 20th century until she was committed
to an asylum for the mentally ill in 1924