The lacrimal system
The lacrimal system consists of:1- Secretory portion: Comprises the following:
a- The lacrimal gland: Which is divided into palpebral (near the temporal aspect of upper eyelid) and orbital (near the eyeball) lobes, and it is situated in the upper temporal angle of the orbit. ( for aqueous tear secretion)
b- Accessory lacrimal glands: glands of Krause and glands of wolfring. (for aqueous tear secretion)
c- Meibomian glands.(For oily secretion)
d- Glands of Zeis.(For oily secretion)
f- Goblet cells of conjunctiva. (For mucin secretion)
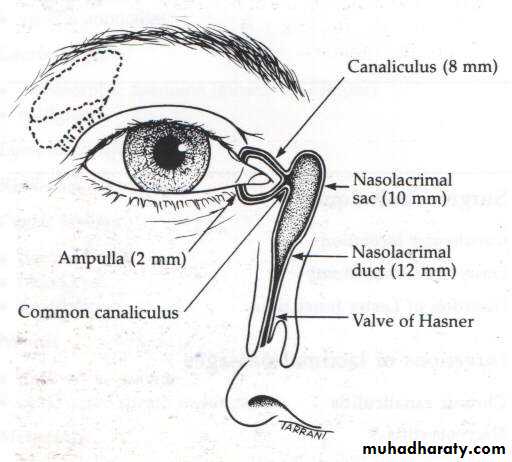
2- Drainage portion: Consists of:
a- Two puncti on the eyelid margins, one upper and one lower.b- Vertical canaliculi (Ampullae): 2mm in length.
c- Horizontal canaliculi: 8mm.
d- The lacrimal sac: 10mm long.
e- The nasolacrimal duct: 12mm, ends into valve of Hasner.
The tear film
The precorneal tear film has three layers:1- Superficial oily layer: Its main advantage is to prevent evaporation.
2- Middle aqueous layer: the thickest layer.
3- Inner mucin layer: Immediately adjacent to cornea: it convert corneal surface and converted it from hydrophobic into hydrophilic so the aqueous layer adherent to it.
Functions of tear:
1- Forms and maintains a smooth refracting surface over the cornea.2- Maintains a moist environment for the conjunctival and corneal epithelium, as dryness of the cornea and conjunctiva causes sloughing of their epithelium and it may ends with corneal ulcer.
3- Bactericidal properties, as it has lysozymes and Igs (IgA).
4- Lubricates the lids.
5- Transports metabolic products (especially CO2 & O2) for cornea as it is an avascular structure, so the tear film transports these nutrients from the atmosphere to the cornea and vice versa.
6- Provides a pathway for WBCs in case of injury (enhances the migration of WBCs).
7- Dilutes and washes away noxious stimuli.
Causes of excessive watering:
1- Lacrimation:Caused by reflex over-production of tear from stimulation of the ophthalmic branch of the trigeminal nerve by irritation of the cornea and conjunctiva, and it is initiated also due to emotional stimulation. Lacrimation is usually associated with symptoms of underlying cause and treatment is usually medical (e.g. conjunctivitis, keratitis, and ect).
2- Epiphora (Obstructive epiphora):
Caused by mechanical obstruction of tear drainage, it is characterized by excessive watering which is exacerbated by a cold atmosphere and is least in a warm dry atmosphere (due to evaporation during warm weather). Treatment in most cases by surgery.
Causes
Punctal stenosis
Canalicular obstruction
Acquired nasolacrimal duct obstruction
Congenital nasolacrimal duct obstruction
Acquired nasolacrimal duct obstruction
Causes:
a- idiopathic stenosis (most common cause).
b- Naso-orbital trauma.
c- Irradiation.
d- Wegener's granulomatosis.
e- Nasopharyngeal tumor.
Congenital nasolacrimal duct obstruction:
At birth, the lower end of the nasolacrimal duct (NLD) is frequently non-canalized (near the valve of hasner), but this is of no clinical significance in most neonates because it canalizes spontaneously soon after birth. Sometime the occlusion is continues and result in:
Signs:
a- Epiphora.b- Gentle pressure of the lacrimal sac causes reflex of purulent material from the puncti.
c- occasionally, acute dacryocystitis (uncommon).
Differential diagnosis of watery eye (lacrimation and epiphora) in neonates:
congenital drainage system obstruction.
Ophthalmia neonatorum. (neonatal conjunctivitis)
Congenital glaucoma. (very important to be remember)
Foreign body .
Treatment:
a- Massage: of the NLD, so increase the hydrostatic pressure and thereby ruptures the membranous obstruction. This is done as ten strokes applied four times daily.b- Probing: overcomes the obstructive membrane at Hasner's valve. It should not be performed until the age of 12-18 months because spontaneous canalization occurs in about 95% of cases.
Postoperative antibiotic drops are used four times daily for one week, if after six weeks there is no improvement, the probing should be repeated.
90% are cured by the first probing and further 6% by the second. Failure of surgery is due to congenital alteration of NLD anatomy or congenitally abscent.
Cases with persistent symptoms in spite of two satisfactory probing can be treated by DCR at preschool age.
Diseases of the lacrimal passages
Dacryocystitis: Is an acute or chronic inflammation of the lacrimal sac. The cause is obstruction of the lacrimal sac or nasolacrimal duct followed by microbial infection. (Staphylococci and Streptococci)
Acute dacryocystitis:
Is a suppurative inflammation of the lacrimal sac associated with cellulitis of the overlying tissues (tissues medial to medial canthus).
Signs and symptoms:
Acute onset of painful swelling, tenderness overlying the lacrimal sac combined with widespread cellulitis and associated constitutional symptoms.
Treatment:
- Local hot compresses and systemic antibiotics.
- Incision and drainage if there is abscess formation
Keratoconjunctivitis sicca Dry eye
Clinical featuresChronic irritation, foreign body sensation and recurrent conjunctivitis
Causes:
1-Sjogren’s syndrome; is an autoimmune disease (antinuclear antibody positive in 80%). Middle age female. Sometimes associated with dry mouth and connective tissue disorders
2-Damage to the lacrimal gland by inflammation (e.g. sarcodosis), trauma or tumor
3- Congenital absent of lacrimal gland
4- Blockage of secretary ducts in cicatricial conjunctivitis e.g. trachoma, chemical burn.
5-Mucin deficiency due to goblet gland destruction in hypovitaminosis A