1
Fifth stage
Radiology
Lec-2
.د
هديل
12/10/2015
Small & large bowel disease
Ba examination
Barium studies of the small intestine
Small bowel follow through (SBFT)
Routine investigation for delineation of all parts of the small bowel done with barium meal
after having a quick look at esophagus, stomach, and duodenum.
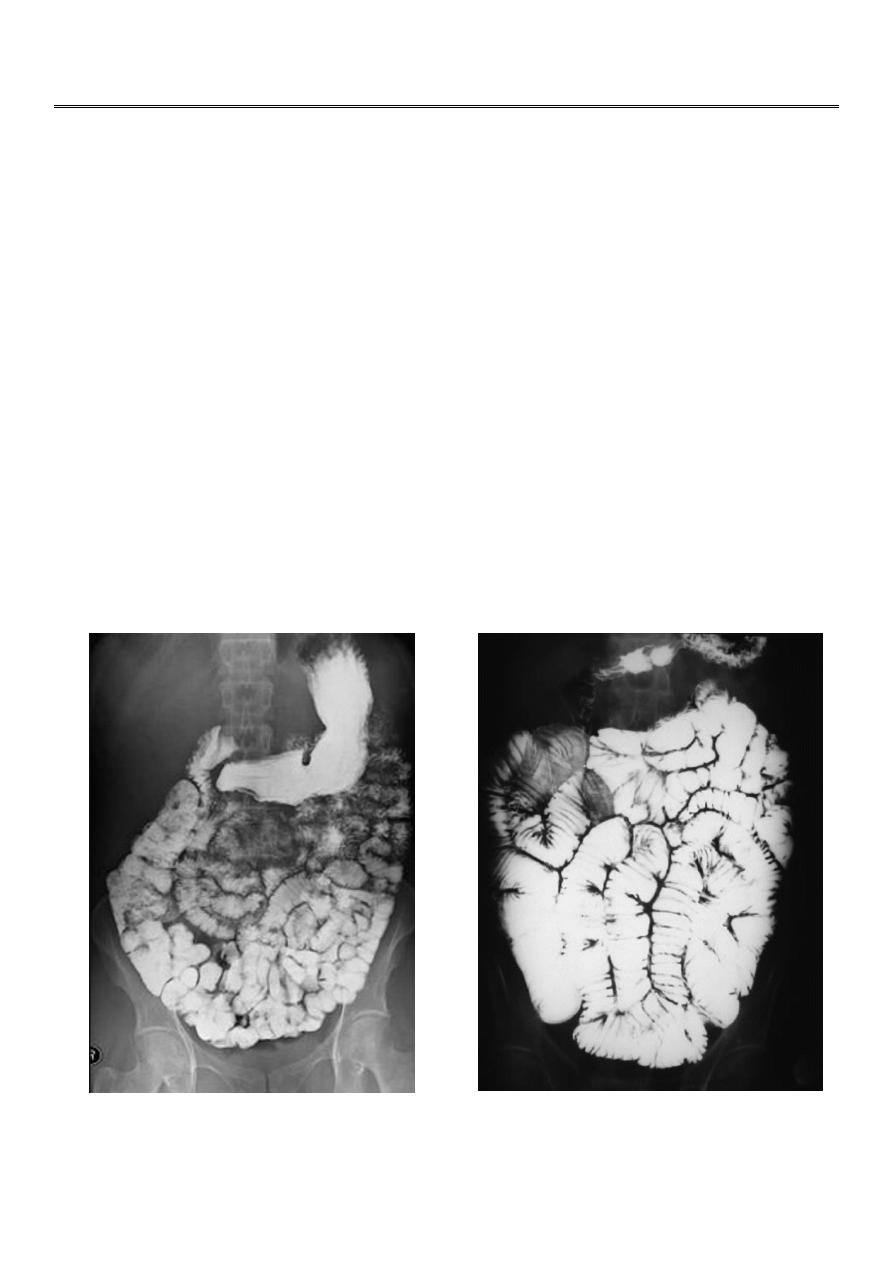
Radiographic features
On a normal barium study of the small bowel, the jejunum is located in the upper left
abdomen and the ileum in the lower right abdomen, to be continued by colon in ileo-caecal
region. The mucosa of the small bowel is characterized by the existence of the
valvulae conniventes which give the small bowel normal feathery appearance in ba-follow
through examination.

2
Indication of Ba –follow through examination
In the small intestine, a barium exam may reveal:
1. Inflammatory bowel disease (CD & UC).
2. Mal absorption syndromes.
3. Swelling and/or inflammation of the small intestine walls.
4. Tumors.
5. Ulcer.
Contraindications for a barium follow through may include:
1. Suspected bowel perforation.
2. Bowel obstruction.
3. Conditions where aspiration of barium is likely.
Crohn’s disease
Crohn’s disease remains idiopathic.
Radiographic features
The characteristic of Crohn’s disease is the presence of:
Skip lesions
Multiple discrete ulcers.
The frequency with which various parts of the gastrointestinal tract are affected varies
widely:
Small bowel: 70-80%
Small and large bowel: 50%
Large bowel only: 15-20%
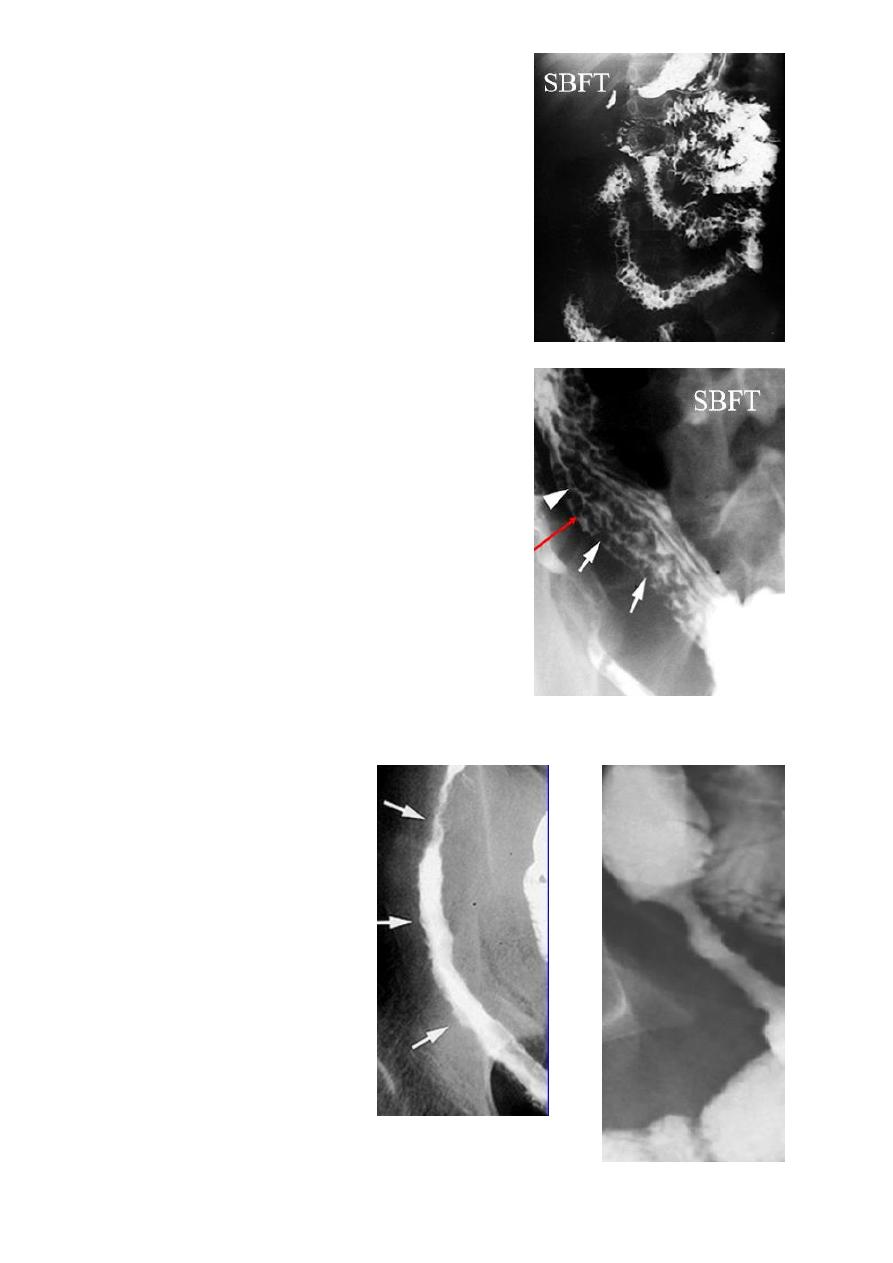
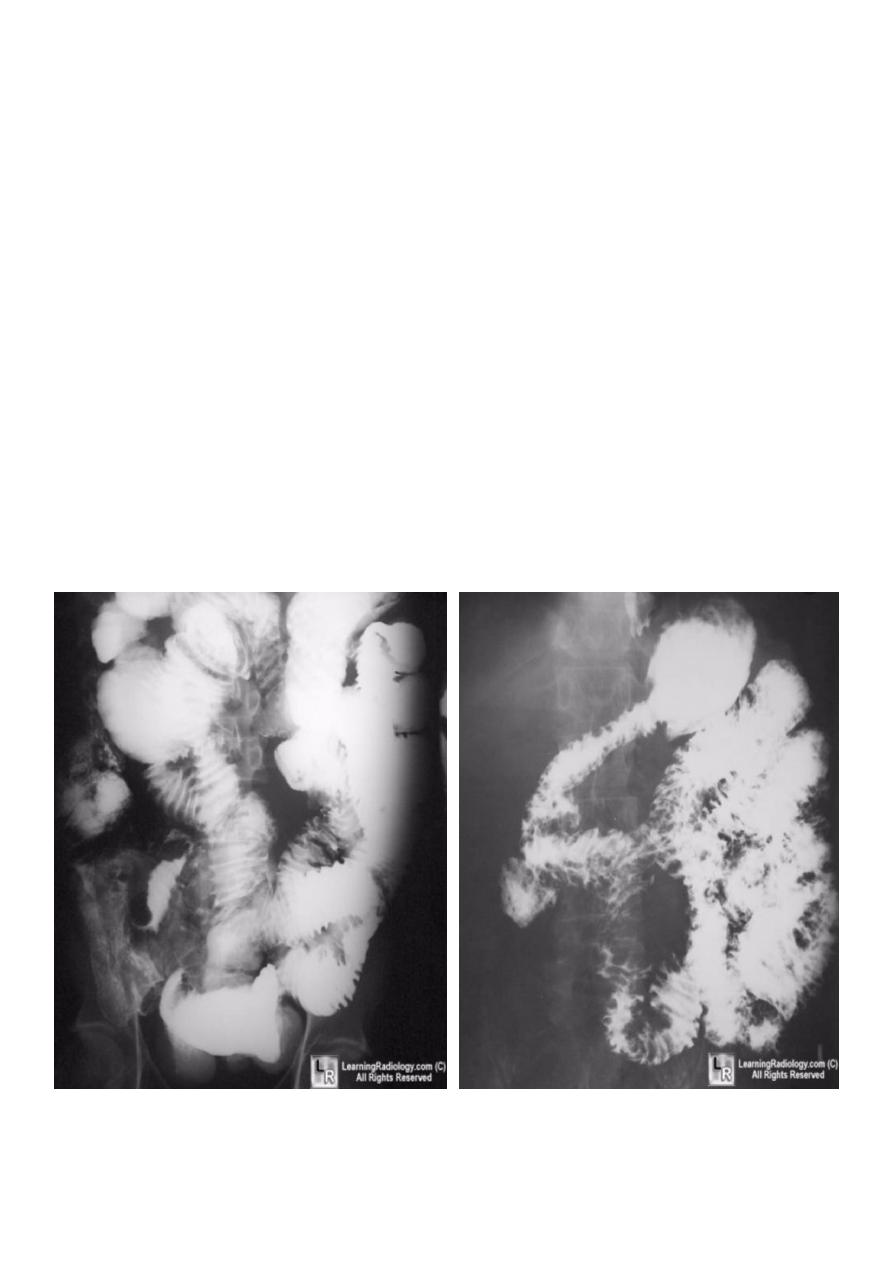
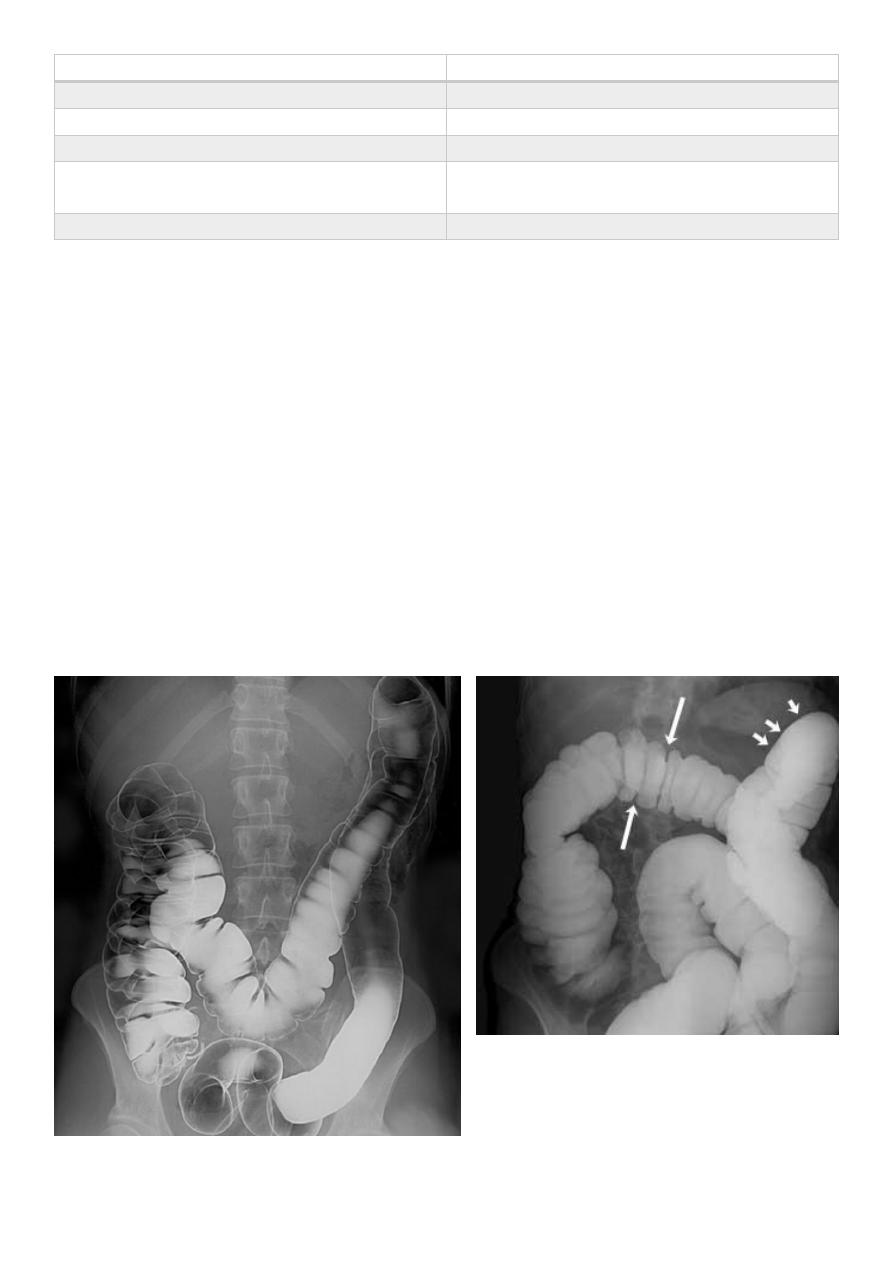
Barium small bowel follow-through findings of CD
Multiple mucosal ulcers aphthous ulcers
Longitudinal fissures
Multiple skip lesions
When severe leads to cobblestone appearance
May lead to sinus tracts and fistulae
Widely separated loops of bowel due to fibro-fatty proliferation
Thickened folds due to edema
Pseudo diverticula formation: due to contraction at the site of ulcer with ballooning of
the opposite site
3
Cobblestoning
Apthae enlarge, merge
Interspersed w/ edematous mucosa
Deep ulcers lead to fistulas
Pseudopolyps
Inflammatory
Cobblestoning
nodular filling defects
edematous mucosa surrounded by ulcerations
Postinflammatory
mucosal overgrowth during healing process
filiform
Stricturing
Active disease
“string sign”
edema, spasm
Fibrotic disease
irreversible strictures
lead to obstruction, fistulas

4
Ulcerative colitis (UC)
Is an inflammatory bowel disease which predominantly affects the colon, but also has extra
intestinal manifestation.
Radiographic features
Involvement of the rectum is almost always present (95%), with the disease involving variable
amounts of the more proximal colon, in continuity. The entire colon may be involved, in
which case edema of the terminal ileum may also be present (so-called back-wash ileitis).
In very severe cases, the colon becomes atonic, with marked dilatation, worsened by
bacterial overgrowth. This leads to toxic mega colon which although uncommon has a poor
prognosis.
Plain film
Nonspecific but may show evidence of mural thickening (more common), with thumb
printing also seen in more severe cases.
Fluoroscopy - Barium enema
Double contrast barium enema allows for detail
of the colonic mucosa, and also allows bowel
proximal to strictures to be assessed. It is
however contraindicated if acute severe colitis
is present due to the risk of perforation.
Mucosal inflammation lends a granular
appearance to the surface of the bowel. As
inflammation increases, the bowel wall and
haustra thicken.
Mucosal ulcers are undermined (button-shaped
ulcers). When most of the mucosa has been lost,
islands of mucosa remain giving it a pseudo-
polyp appearance.
In chronic cases the bowel becomes featureless
with loss of normal haustral markings, luminal
narrowing and bowel shortening (lead pipe
sign).
Colorectal carcinoma in the setting of ulcerative colitis is more frequently sessile and may
appear to be a simple stricture.
5
6
Toxic megacolon (TM)
Is a complication that can be seen in both types
of inflammatory bowel disease more in UC,
in infectious colitis, as well as in some other types
of colitis. It is serious acute abdominal condition,
more in UC > CD
Radiographic features OF TOXIC MEGACOLON
The colon (typically transverse colon) becomes
dilated to at least 6 cm (usually greater). There is
additional loss of haustral markings
Practical points
Barium studies and colonoscopy should be avoided,
due to the risk of perforation
Crohn's disease vs. ulcerative colitis
Due to the overlap in clinical presentation
of Crohn's disease (CD) and ulcerative colitis (UC),
imaging often has a role to play in distinguishing the
two. Distinguishing features include:
Bowel involved
CD: small bowel 70-80%, only 15-20% have
only colonic involvement
UC: rectal involvement 95%, with terminal
ileum only involved in pancolitis (backwash
ileitis)
Distribution
CD: skip lesions typical
UC: continuous disease from rectum up
Gender
CD: no gender preference
UC: male predilection
Colonic wall ((Terminal ileum involvement))
CD: involved (terminal ileatis)
UC: uncommon, backwash ileatis
7
Inflammatory Bowel Disease (IBD):
Crohn’s vs. Ulcerative Colitis (UC)
Crohn’s UC
• transmural • Mucosal
• skip areas • Continuous
• Rectal sparing • involves rectum
• may involve any region of GI tract • Usually limited to colon
Lymphoma of small bowel
Splaying & separation of the bowel loops due to enlarged LN
Thickening of the mucosa, irregular in outline (saw tooth pattern).
LATER stage could be present as sign of Mal absorption syndrome (flocculation &
segmentation of the Ba).
8
Malabsorption syndrome
Ba follow through findings
Loss of normal small bowel feathery appearance.
Dilated small bowel loops > 3.5 cm
Splaying & increase the distance between small
bowels loops
Flocculation & segmentation of the Ba
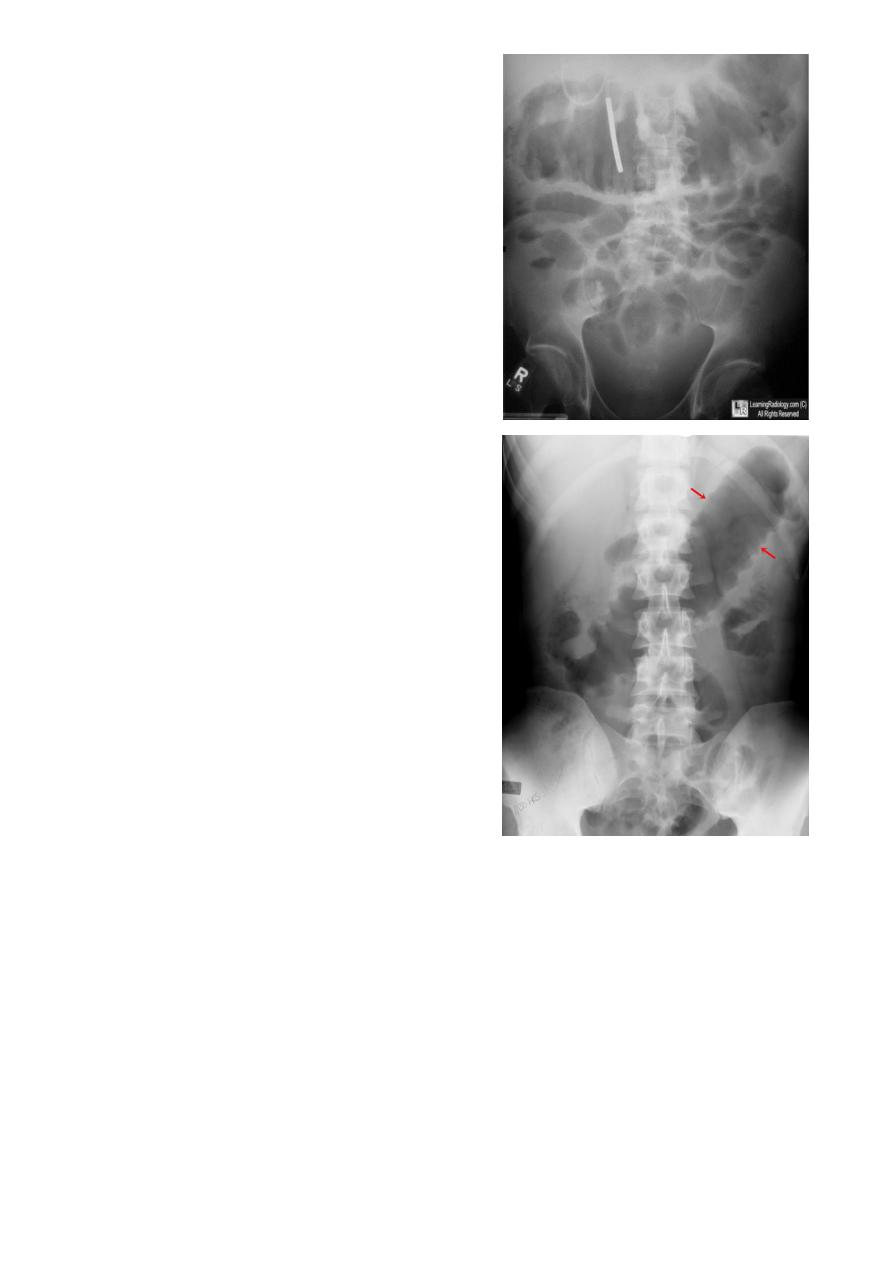
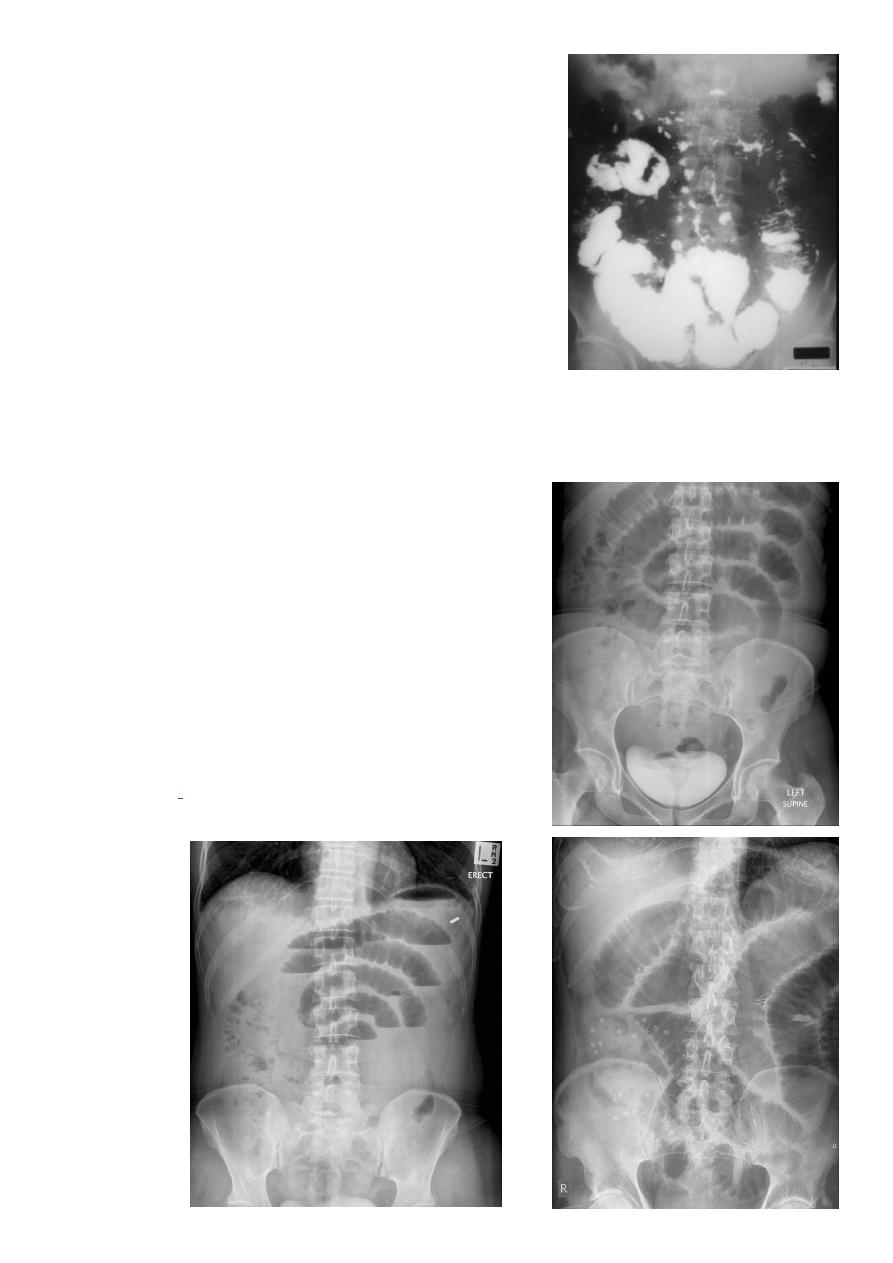
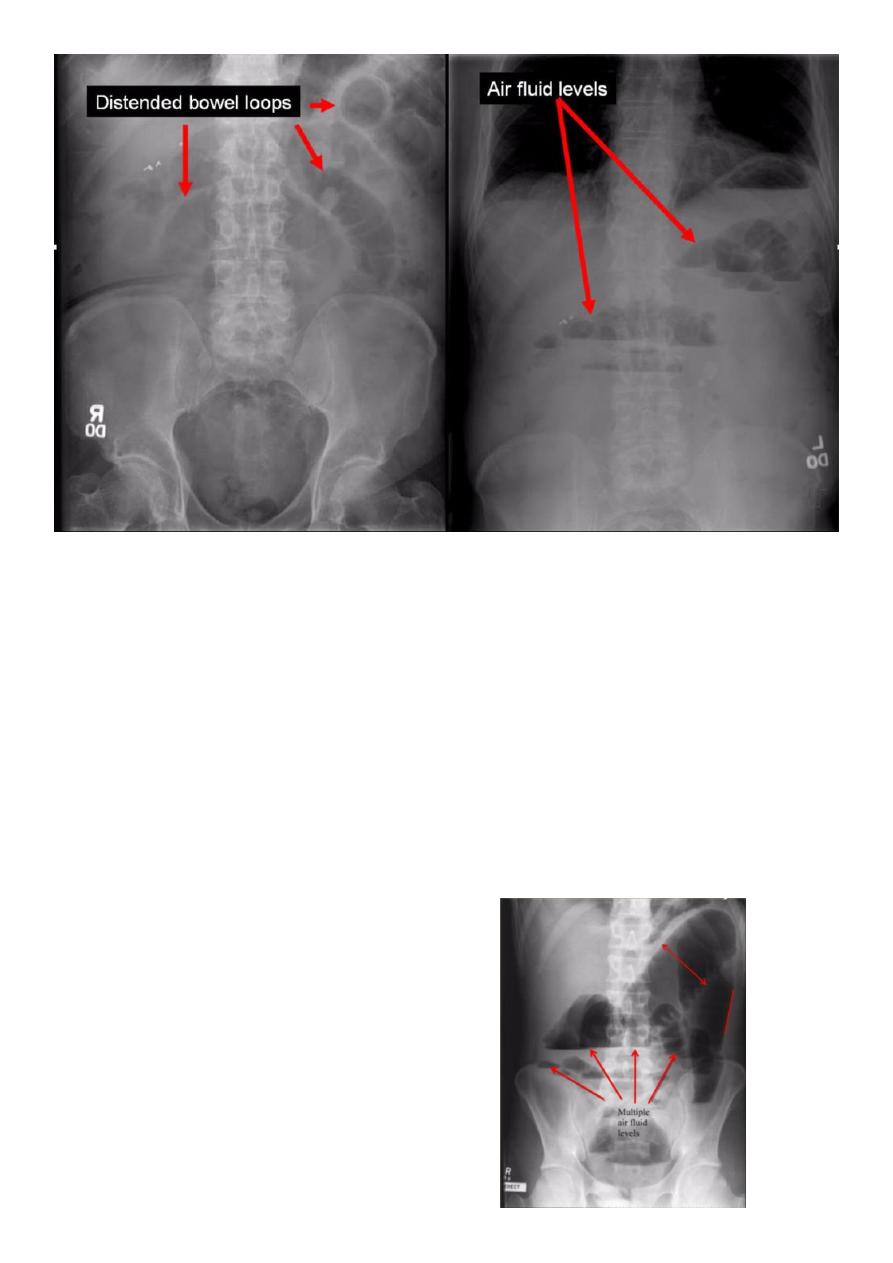
Small bowel obstruction
Accounts for 80% all mechanical intestinal obstruction; the remaining 20% result from large
bowel obstruction
Radiographic features
Abdominal radiograph
Abdominal radiographs are only 50-60% sensitive for
small bowel obstruction. In most cases, the abdominal
radiograph will have the following features:
Dilated loops of small bowel proximal to the
obstruction
Predominantly central dilated loops
Three instances of dilatation over 3 cm
conniventes are visible
Fluid levels if the study in erect position
9
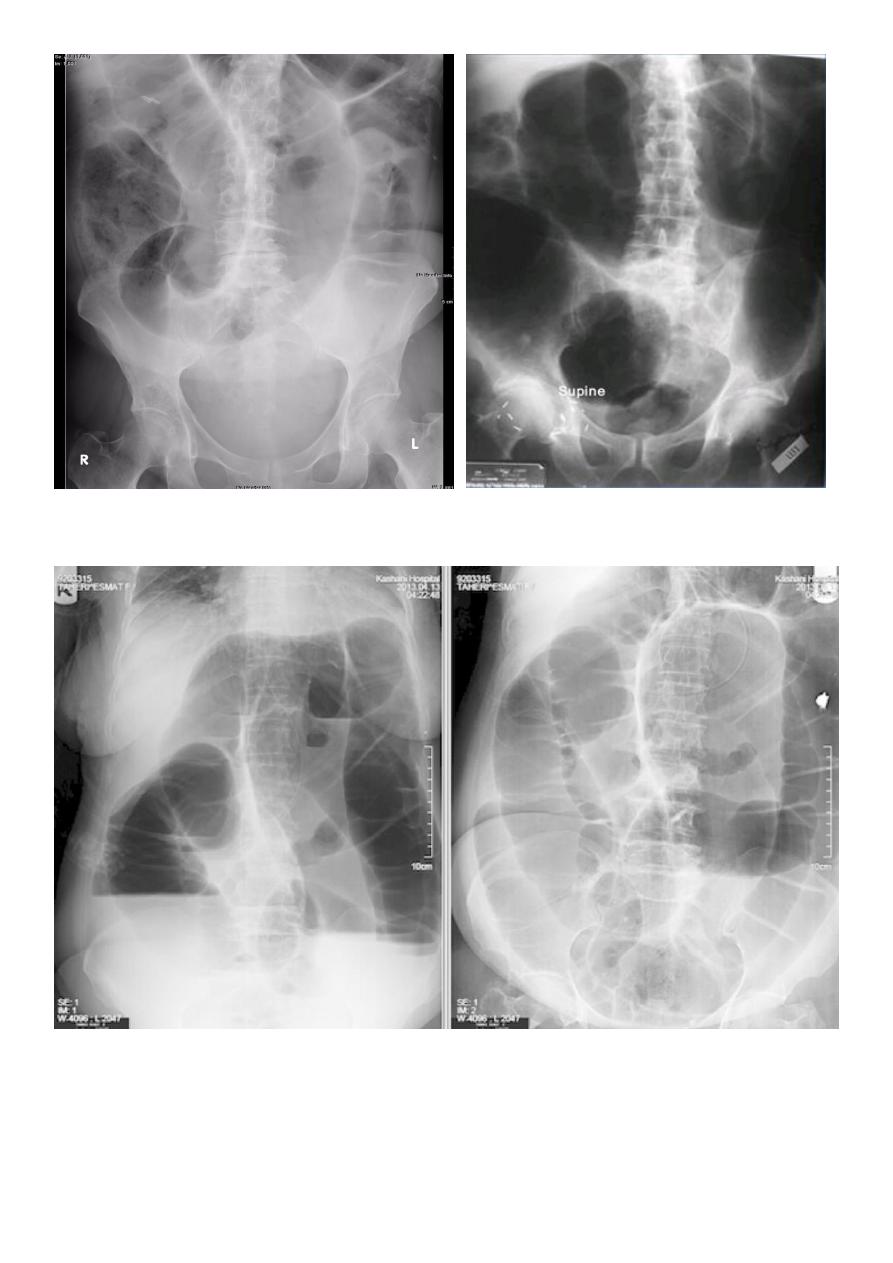
Large bowel obstruction (LBO)
Are often impressive on imaging, on account of the ability of the large bowel to massively
distend. This condition requires prompt diagnosis and treatment
Radiographic features
Colonic distension > small bowel.
Peripherally located.
Dilated loops less in no. than SBO.
Presence of haustra.
1. Dilated Colon > 6 CM
2. Effacement of haustrae peripherally located
3. Multiple Air Fluid Levels
DX: Small Bowel Obstruction
11
11
Large Bowel
Small Bowel
1- Peripheral
1- Central
2- Maximum diameter is 8 Cm.
2- Maximum diameter is 5 Cm.
3- Presence of haustration.
3- Vulvulae conivetae.
4- Colon is filled with feces which has
bubbly apperance
5- Air fluid levels are few and large.
4- Air fluid levels are many and small.
Ba –enema examination
A barium enema is an x-ray examination of the colon and rectum that helps a doctor identify
inflammation, polyps, or cancer.
Before a barium enema, you will need to empty your colon by following a restricted diet and
using a laxative or enema.
During the examination, a liquid called barium is delivered into the colon through the anus
and x-rays are taken.
After the procedure, you will go to the restroom to push out the barium; you may be asked
to take a laxative at home to get rid of any barium still in your body.
12
Colorectal carcinoma (CRC): is the most common cancer of the gastrointestinal tract and the
second most frequently diagnosed malignancy in adults.
Radiographic features
Colorectal cancers can be found anywhere from the caecum to the rectum, in the following
distribution:
Recto-sigmoid: 55%
Caecum and ascending colon: 20%
Ileocaecal valve: 2%
Transverse colon: 10%
Descending colon: 5%
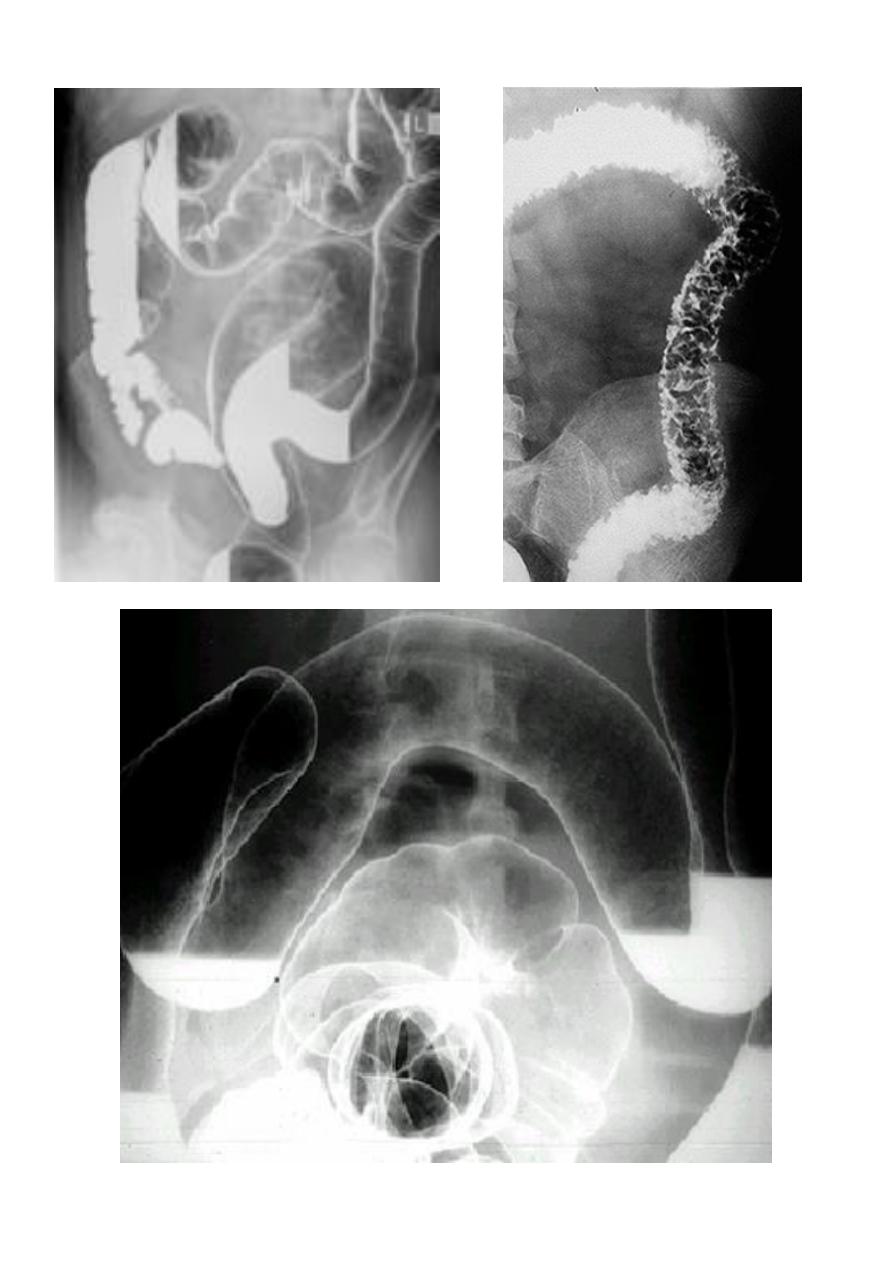
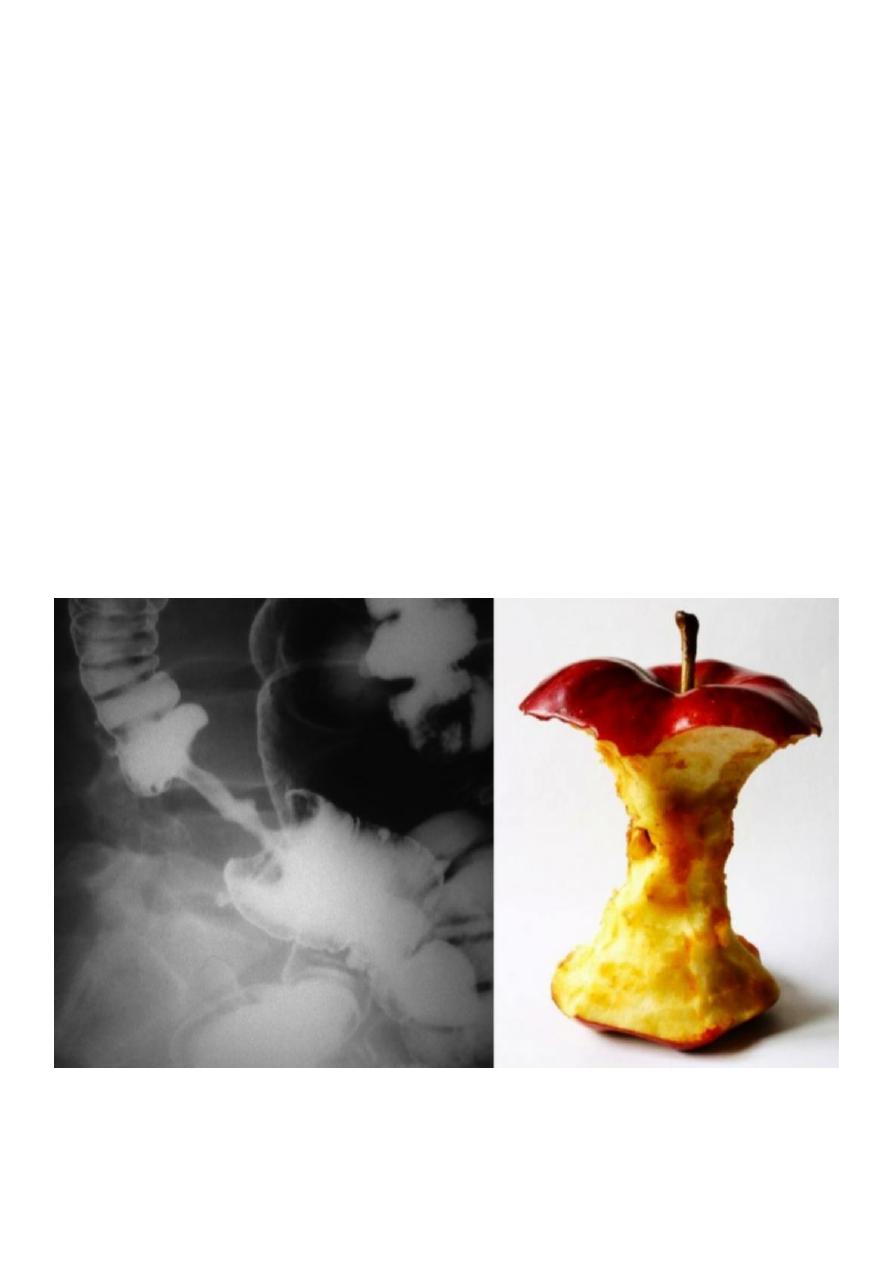
Barium enema 3 presentation:
1- Infiltrative (Apple core sign) lesion infiltrate bowel wall from outside
2- Ill-defined filling defect within the lumen of the bowel
3- Could be ulcerative nodule or ulcerative lesion.
13
14
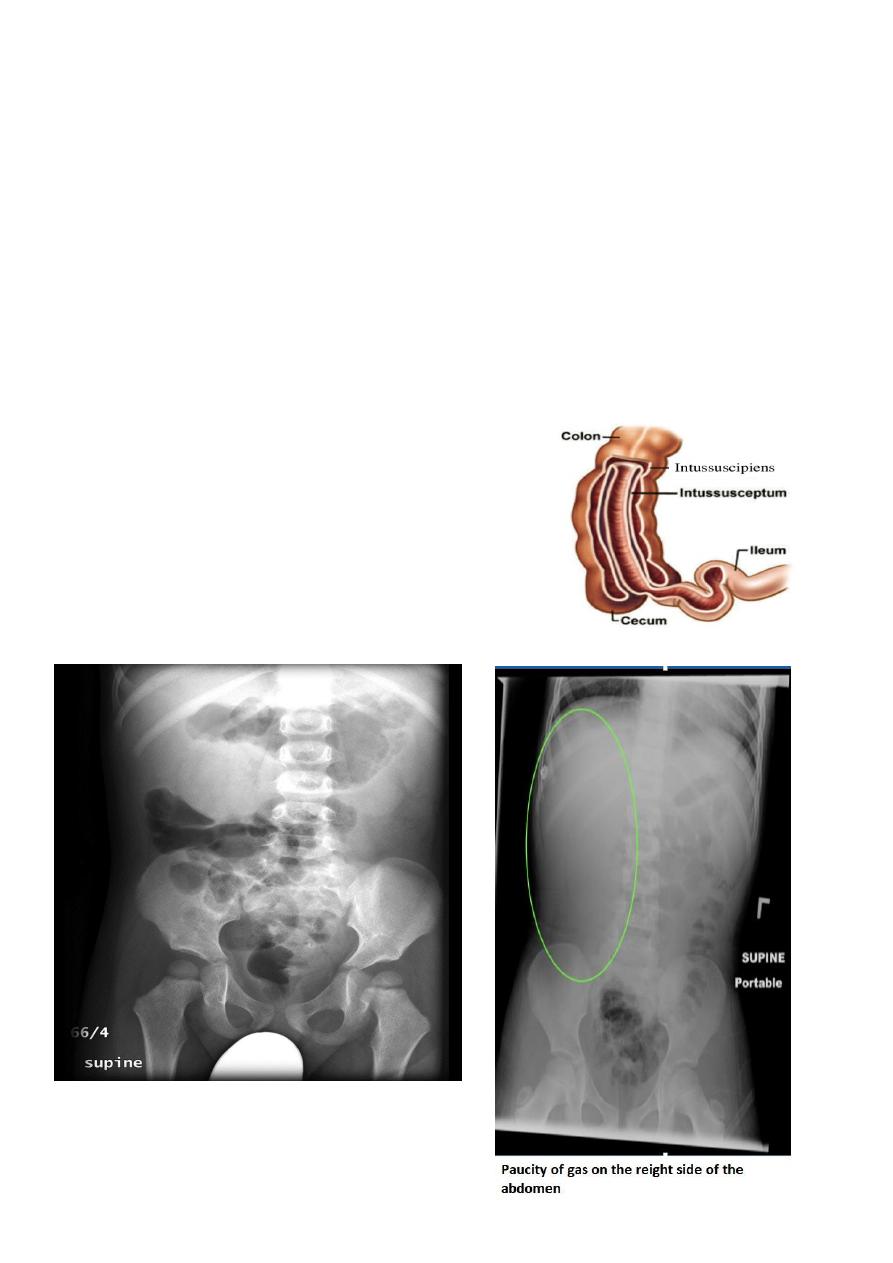
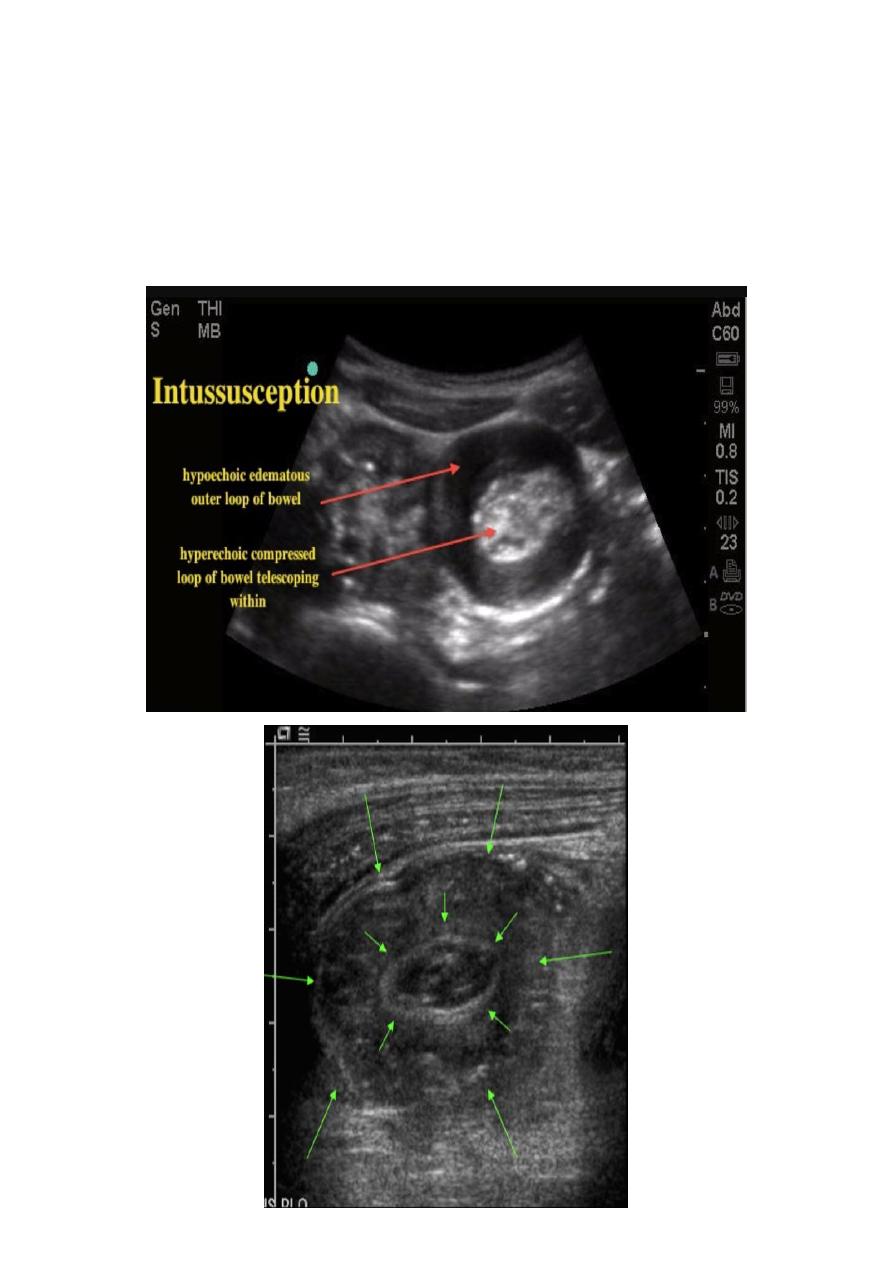
Intussusceptions
occurs when one segment of bowel is pulled into itself (or a neighboring loop of bowel) it is
an important cause of an acute abdomen in children.
Intussusceptions may also occur in the adult population where it is usually caused by a focal
lesion acting as a lead point.
Radiographic features
Intussusceptions can occur essentially anywhere, in children there is a strong predilection for
the ileo colic region
Abdominal plain film
Abdominal x-rays may demonstrate an elongated soft tissue mass (typically in the right upper
quadrant in children) with a bowel obstruction proximal to it.
The Anatomy of Intussusception
Intussusception occurs when a segment of the bowel, the
intussusceptum, telescopes into a more distant segment
of bowel, the intussuscipiens.
The most common type is ileo-colic ((in the picture))
followed by ileoileocolic, ileoileas and colocolic.
15
Ultrasound
A reliable screening tool for children at low risk for intussusceptions.
Ultrasound signs include:
Target sign (also known as the doughnut sign)
Pseudo kidney shape sign
16
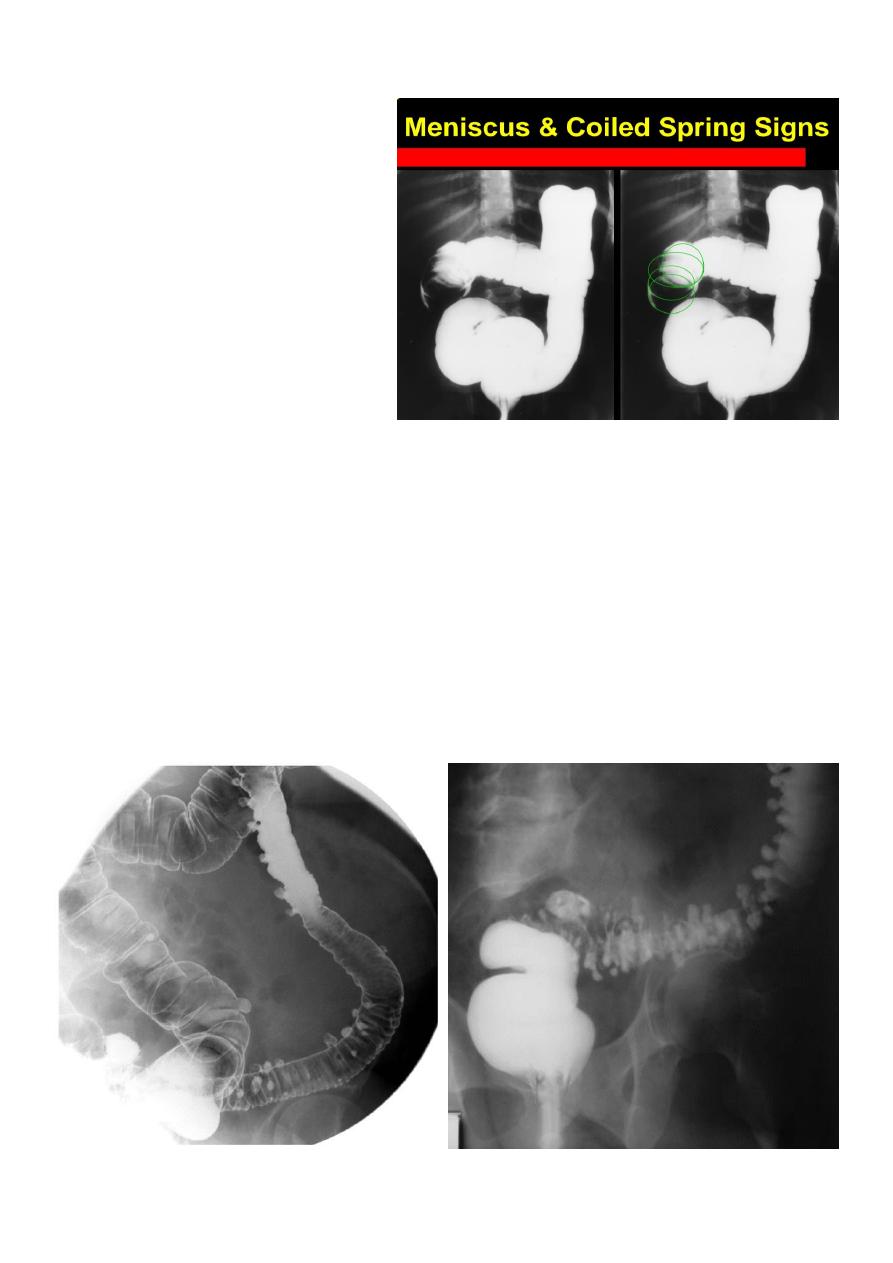
Contrast enema
A contrast enema remains the
gold standard, demonstrating
the intussusceptions as an
occluding mass prolapsing into
the lumen, giving the "coiled
spring” appearance.
The main contra-indication for
an enema is a perforation
Contrast enema is diagnostic &
therapeutic
Colonic diverticulosis
Refers to the presence of multiple diverticula. It is quite distinct from diverticulitis which
describes inflammation and infection of one or multiple diverticula.
Radiographic features
Diverticula range in size from a few millimeters to a few centimeters
Barium enema
Both single and double contrast barium enemas are able to demonstrate diverticula as
barium-filled out-pouchings.

17
Familial adenomatous polyposis syndrome
(FAPS) is characterized by the presence of hundreds
of adenomatous polyps in the colon. It is the most
common of the polyposis syndromes.
Radiographic features
FAPS has a varied imaging appearance and demonstrate
innumerable polyps. Imaging usually underestimates
the number of polyps because most are <5mm in size.
It is a predisposition to colorectal carcinoma (CRC)
18
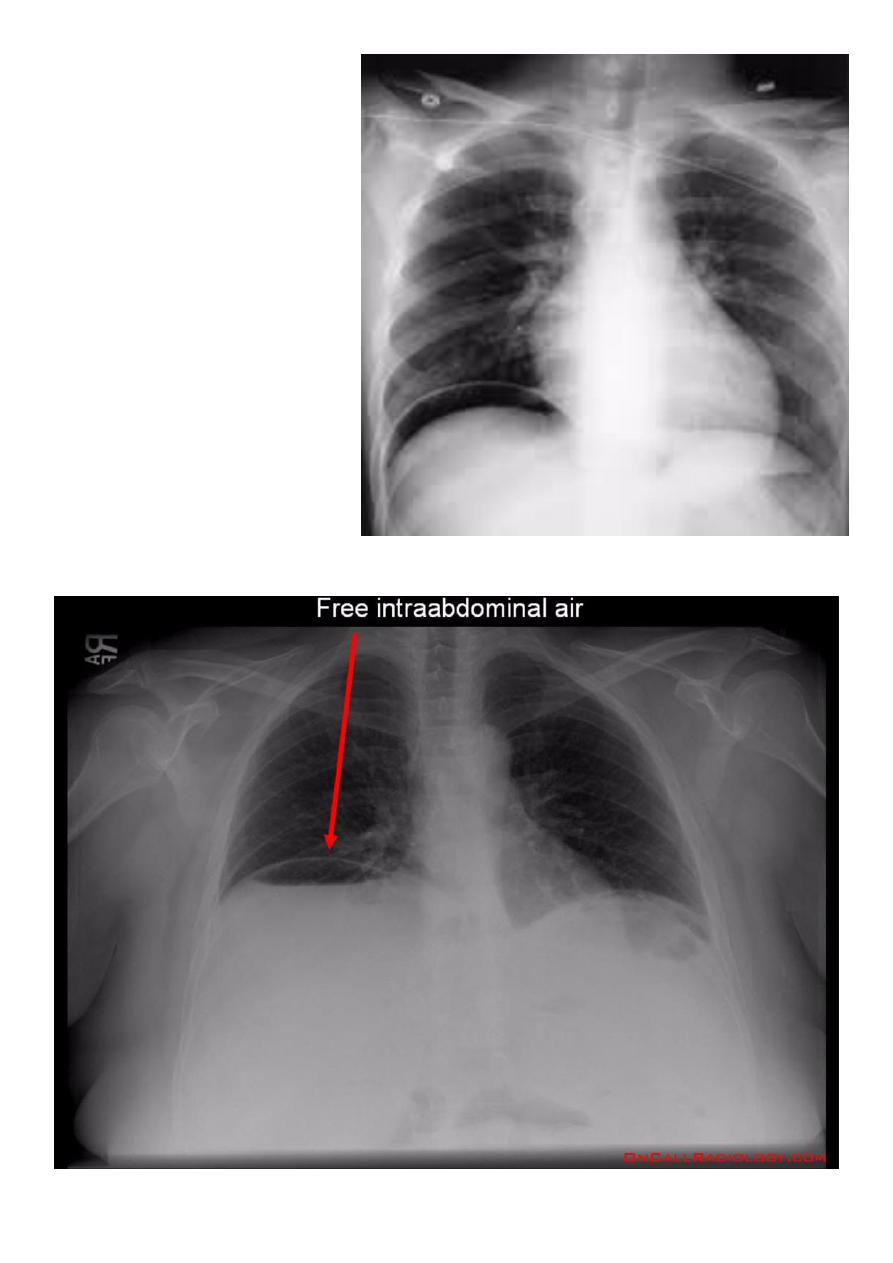
Pneumoperitoneum
Describes
as
gas
within
the peritoneal cavity, and is often
of a critical illness
Plain film
Chest radiograph
An erect chest x-ray is probably the
most sensitive plain radiograph for
the detection of free intra
peritoneal gas as crescent shape of
lucency below diaphragm, more in
the RT sided aspect.
Described as sub diaphragmatic
free gas
19
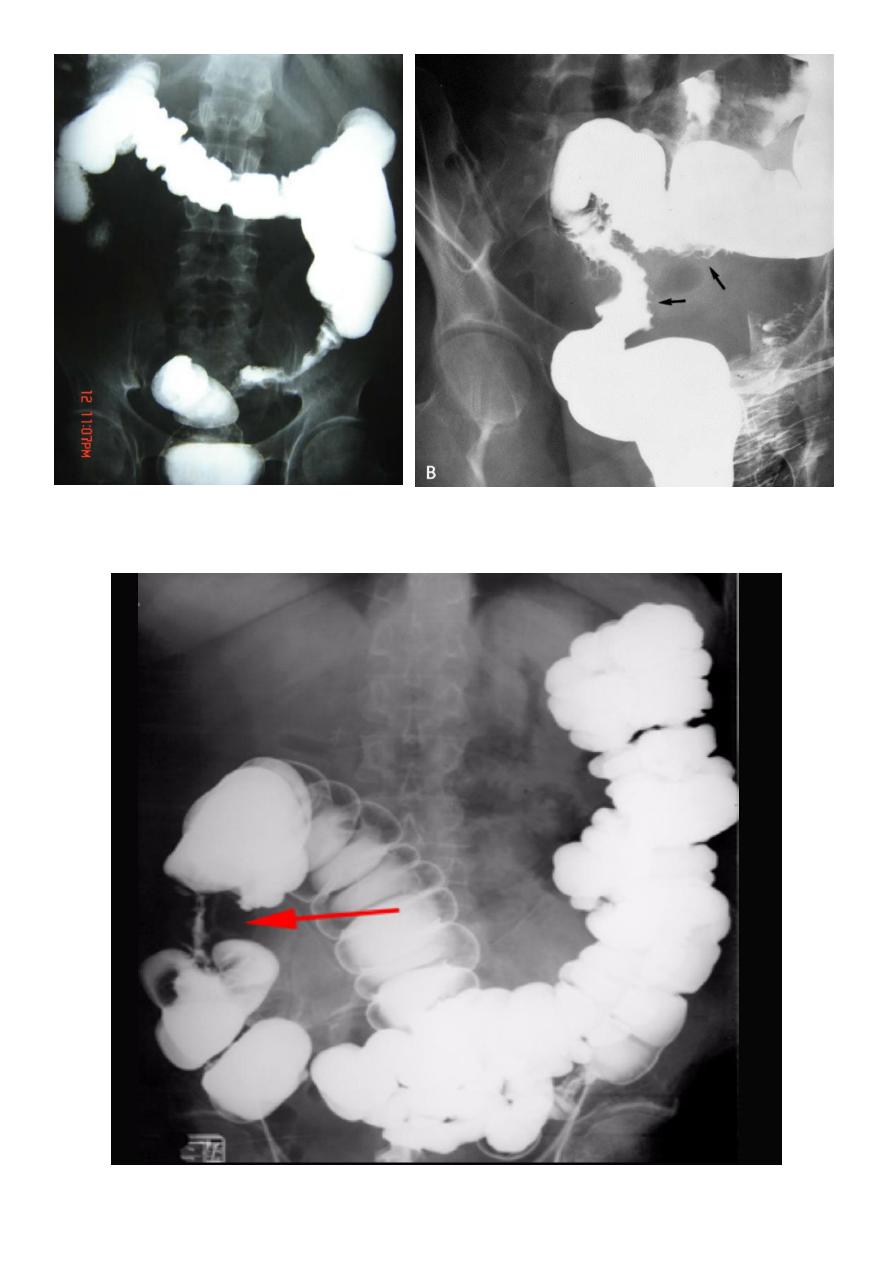
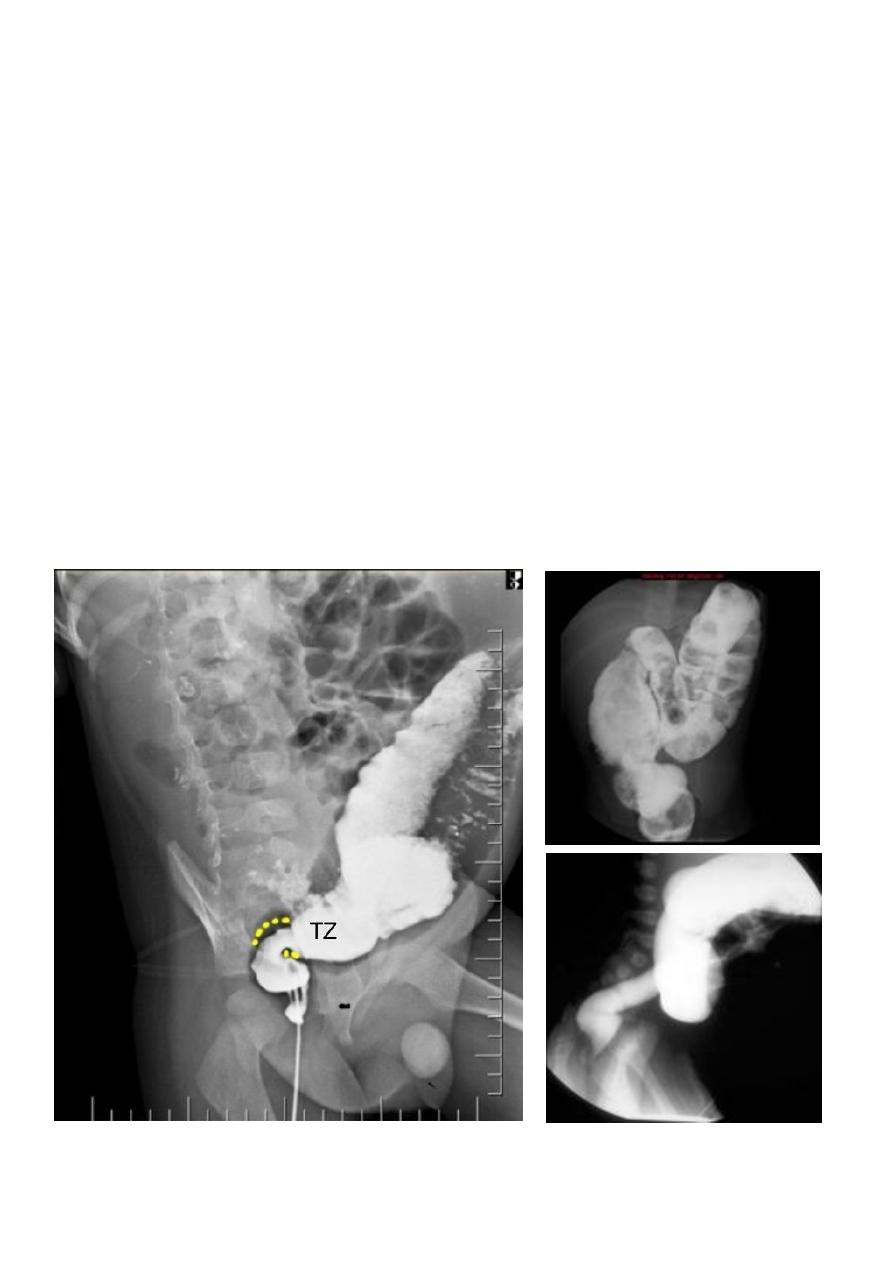
Hirschprung disease
The most common cause of neonatal colonic obstruction (~15-20%). It is commonly
characterized by a short segment of colonic aganglionosis affecting term neonates, especially
boys.
Contrast enema
A carefully performed contrast enema is indispensable in both the diagnosis of Hirschprung
disease but also in assessing the length of involvement. It should be noted however that the
depicted transition zone on the contrast enema is not accurate at determining the transition
between absent and present ganglion cells.
The affected segment is of small caliber with proximal dilatation Fasciculation/saw-tooth
irregularity of the aganglion segment is frequently seen
Views of particular importance include:
Early filling views that include rectum and sigmoid colon allowing for rectosigmoid ratio to
be determined.
Transition zone

21
Anal atresia (or imperforate anus)
Refers to a spectrum of ano rectal abnormalities ranging from a membranous separation to
complete absence of the anus.
Abdominal radiograph
Can be variable depending on the site of atresia (e.g high or low), level of impaction with
meconium and physiological effects such as straining
May show multiple dilated bowel loops with with absence of rectal gas
Invertogram
A coin/metal piece is placed over the expected anus and the baby is turned upside down (for
a minimum 3 minutes).
Distance of gas bubble in rectum from the metal piece is noted:
>3 cm: denotes high type
<3 cm: denotes low type