Urinary tract infectioncont,
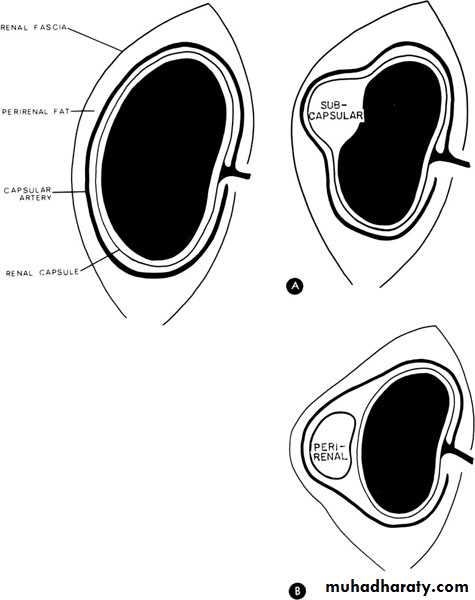
Perinephric abscessInfection and pus collection in the perinephric space within Gerota’s fascia
Source of infection
Hematogenous,lymphatic
infected peri renal hematoma or urinoma,
extension from a nearby infected focus like appendicitis
untreated pyonephrosis or renal abscess.
Rarely mycobacterial perinephric abscess may occur.
Clinical pictures
High swinging pyrexia, tenderness and fullness in the loin.The symptoms are marked if the infection started at lower pole because the upper pole is hidden by thoracic cage.
Investigations
GUE: normal unless the abscess is extended from renal pathology.
WBC: neutrophil leukocytosis.
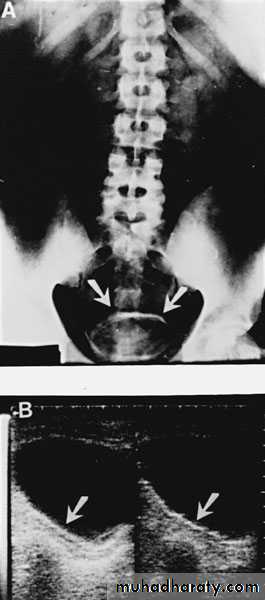
U/S: pus collection around the kidney with or without hydronephrosis.
KUB: obscured psoas shadow, spine scoliosis,.
CT scan & MRI: diagnostic.
Treatment
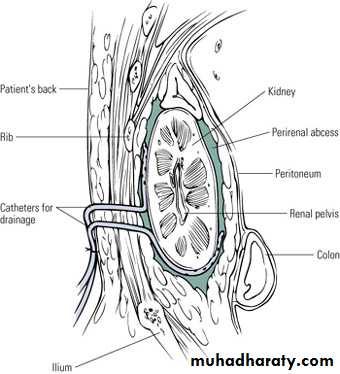
Drainage is the principle treatment of pus collection anywhere in the body.Under antibiotic cover lumber incision is made, all loculi destructed, pus drained and wound closed over a tube drain.
Drinage of perinephric abscess
Renal carbuncle(renal cortical abscess)
It arises as a result of blood born micro-organism especially staphylococcus aureus from a skin lesion in debilitated or immune compromised patient like diabetics. Rarely the abscess arises from infected cortical hematoma or cyst.Clinical pictures
Ill defined tender renal mass, persistent pyrexia and leukocytosis.Investigations
GUE: normal or pyuria.
U/S: cystic cortical lesion with internal echoes.
IVU: space occupying lesion, which may be confused with renal tumor.
CT scan & MRI: diagnostic.

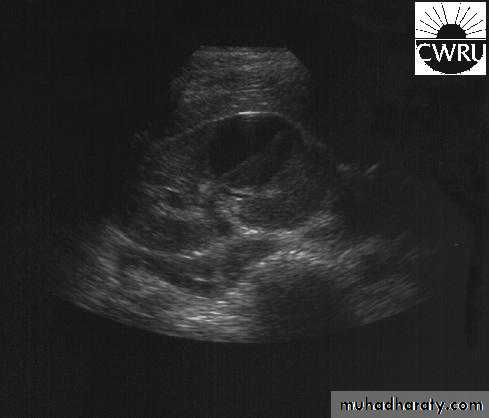
U/S cystic lesion with internal echoes (renal abscess)


Retrograde pyelography:
Left renal abscess
CT scan: right renal abscess

CT scan: Left renal abscess
TreatmentDrainage is the principle treatment of pus collection anywhere in the body.
If pus is too thick to be drained by percutaneous needle aspiraion
Under antibiotic cover lumber incision is made, all loculi destructed, pus drained and wound closed over a tube drain.
Specific infection of the kidney
Renal TuberculosisBacteria: Mycobacterium TB
Pathogenesis: Hematogenic
Start unilateral , late bilateral affection.
The 1st lesion starts usually in the pyramids
Chronic: Asymptomatic until late stage
TB granuloma, caseation, open to the calyces.
Renal destruction, calcification.
The ureteric upper & lower 1/3rd is affected
Ureteral & bladder involvement is commonly secondary
RENAL TB

Clinical picture
Always suspect if:Endemic area
Age : 20----30 year
Chronic symptoms
Non responsive UTI to adequate therapy.
Unexplained hematuria.
Night sweating, Wt loss
Chronic renal sinuses.
TB is the most common opportunistic infection in AIDS patients
Investigations
GUE : RBC , Sterile acid pyurea.
-ve urine C&S
Three successive morning urine samples for AFB.
24 hours urine collection for AFB.
TB culture & sensitivity.
ESR increased
WBC total & differential.
KUB: Renal calcification
IVU
CXR
Cystoscopy: for lower tract involvement.
Treatment
Medical:Surgical:
If complicated
No clinical control
Correct obstruction
Nephrectomy.Bilharziasis
Trematode: schistosoma haematobium
Male: female 3:1
Endemic in Nile valley, Iraq, & middle east in general.
Marshes & slow running fresh water is the habitat of the fresh water snail ( bulinus truncatus ) which is the intermediate host.
Clinical features
Urticaria ( swimming itch )Fever , sweating
Hematuria: intermittent, terminal
Lymphadenopathy & splenomegaly
Investigations
GUE : early morning samples for several consecutive days – ovae with terminal spinesLeukocytosis – eosinophilia
Cystoscopy
Bilharzial pseudotubercles , nodules, sandy patches, ulceration, fibrosis, granulomas, papillomas, carcinoma (SCC).

Imaging study
KUB
U/S

IVU


Treatment
Antimony e.g. praziquantel & metriphonatePapilloma : endoscopic removal
Carcinoma : radical cystectomy

Thank you