Page1
The oral cavity is lined by oral mucosa which is composed of epithelium
(stratified squamous epithelium) and lamina propria
Submucosa is found beneath mucosal layer which is a relatively vascular
connective tissue containing minor salivary gland in some areas
Oral mucosa is divided into:
1. Masticatory mucosa
: mostly located in gingiva and hard palate, it is paler in color
than the other lining mucosa and it is firmly attached to the underlying tissue.
2. Lining mucosa
: most common sites are the buccal mucosa, floor of the mouth,
ventral surface of the tongue. It is pinkish in colour due to reflection of the
underlying vascular bed
3. Specialized mucosa
: located on the dorsum of the tongue (due to the presence of
taste buds)
The reddish colour of mucosa is due to the underlying vascular bed and semitransparent
colorless epithelium, so any obstruction in this reflection may change colour of mucosa.
Why does oral mucosa appear white sometimes?
1.
Increased thickness of epithelium
covering the mucosa with increased production of
keratin (keratotic white lesions) ex.: lichen planus, leukoplakia, traumatic keratosis
2.
Imbibition of water
by upper layers of mucosa as in oral skin graft.
3.
Tissue necrosis
: This is characterized by formation of pseudomembrane composed of
dead epithelium, body cells, food debris, microorganisms, and fibrin. Ex.: Thrush
Classification of white and red lesions
U
(Memorize it before proceeding)
A. Normal :
leukoedema, fordyce’s granule, lineae alba
B. Developmental:
white spongy nevus
,
median rhomboid glossitis
C. Infection:
oral candidiasis, syphilis, measles
D. Traumatic:
nicotine stomatitis, traumatic keratosis, papillary hyperplasia
E. Blood dyscrasias:
anemia, Plummer Vinson syndrome
F. Drugs:
aspirin, vitamin A, drug reactions
G. Dermatological
: lichen planus, lupus erythematosus, psoriasis
H. Premalignant
: leukoplakia, erythroleukoplakia, s.m fibrosis
I. Miscellaneous:
oral skin graft, geographic tongue, hairy tongue
Oct 25, Nov 1 & 8
د. ﻋﺒﺎس
5 Sheets / 250 I.D.
ﻃﺐ ﻓﻢ
-
ف
١
3,4,5
Red & White lesions
part1, 2 &3
Page2
A. Normal
(Leukoedema\ Fordyce’s granules \Lineae Alba)
1. Leukoedema:
it is a normal anatomical variation discovered during routine oral
examination. The mucosa appears milky, white and thin, which usually disappears upon
stretching to distinguish it from other lesions.
Dx. Clinical examination and histopathology
Rx. Reassurance
2. Fordyce’s granules:
it is an ectopic sebaceous glands present in the buccal mucosa and
lips, appears as collection of submucosal yellowish plaque or clumpy area
Dx. Clinical examination
Rx. Reassurance
3. Lineae Alba:
horizontal streaks on buccal mucosa at the level of occlusal plane, extend
from the commissure of lips to the posterior teeth, associated with pressure, frictional
irritation or secondary to trauma from facial surface of teeth (bruxism), usually bilateral
Dx. Clinical examination
Rx. Treat underlying cause, prescribe keratolytic agent (retinal) which is a derivative of
vitamin A: 0.01~0.025 mg (for skin 0.1 mg is used for acne)
B. Developmental
(White spongy nevus\ Median rhomboid glossitis)
1. White spongy nevus:
hereditary condition due autosomal dominant gene, characterized
by white folds which us thickened with corrugated patches and irregular spongy texture.
Starts from infancy to the adolescence, affects floor of the mouth, nasal mucosa and anus
Dx. History, clinical examination and histopathology
Rx. Reassurance
2. Median rhomboid glossitis:
was formerly considered as developmental condition but
recently they’ve found that some cases respond well to antifungal treatment, so it may also
be considered as infection-caused lesion. This lesion is located anterior to the circumvallate
papillae, appears as reddish area with smooth depapillated surface, usually asymptomatic
but may cause burning sensation in some cases
Dx. Clinical examination + other investigation for candida (discussed later)
Rx. Antifungal therapy, soothing agent for burning sensation
Page3
C. Infective lesions
(Candidiasis\ Syphilis\ Measles)
1. Candidiasis (candidosis):
infection by Candida albicans, it is present in 30~50% of
population as normal flora or weak pathogen, considered as opportunistic pathogen. It has
two shapes: yeast (spores) and hyphae
Predisposing factors for candidiasis
1.
Xerostomia
2.
Systemic disease
3.
Diabetes mellitus
4.
Endocrine disorders
5.
Anemia (iron deficiency)
6.
Broad spectrum antibiotic administration
7.
Infancy (immature immune system)
8.
Old age (due to decrease immune function)
9.
Acidic saliva, due to carbohydrate rich food
10.
Decrease in immunity of body as in AIDS or
chemotherapy
Classification (Burket’s)
a.
Acute pseudomembranous candidiasis (thrush):
removable creamy white patch
affecting buccal mucosa or soft palate. It is easily removed by scraping which may result
in reddish area or pinpoint bleeding, or it may reveal the underlying cause which is
secondarily infected by candida. Occur in infancy due to immature immune system and
in old age due to decrease in immune system function. It is usually associated with
burning sensation
b.
Acute atrophic candidiasis (antibiotic sour mouth)
:
occur due to administration of
broad spectrum antibiotic, redness of the oral mucosa and depapillation of tongue.
c.
Chronic hyperplastic candidiasis (candidal leukoplakia):
it is a mixed red and white
lesion (speckled) associated with severe epithelia dystrophy. So, it is premalignant.
d.
Chronic atrophic candidiasis:
i.
Denture stomatitis: seen in patients wearing dentures at night, usually affecting
maxillary arch. Newton classified it into three types (pinpoint, simple diffuse and
papillary hyperplasia)
ii.
Angular cheilitis: characterized by lesions affecting corner of the mouth which
appear as reddish cracked and inflamed area, associated with reduced vertical
dimension of denture, causative microorganisms are: 20% Candida albicans, 20%
Staphylococcus aureus or 60% mixed
iii. Median rhomboid glossitis (mentioned before)
e.
Chronic multifocal candidiasis:
characterized by lesion affecting tongue (median
rhomboid glossitis) and posterior part of palate with angular cheilitis
f.
Mucocutaneous candidiasis:
this type is inherited type affecting skin, nail and m.m.
Dx. of candidiasis
1.
History and Clinical features
2.
Swab for gram stain and periodic acid Schiff to show candidal hyphae
3.
Culturing on Sabouraud dextrose agar
4.
Biopsy (candidal hypha at right angle to oral epithelium)
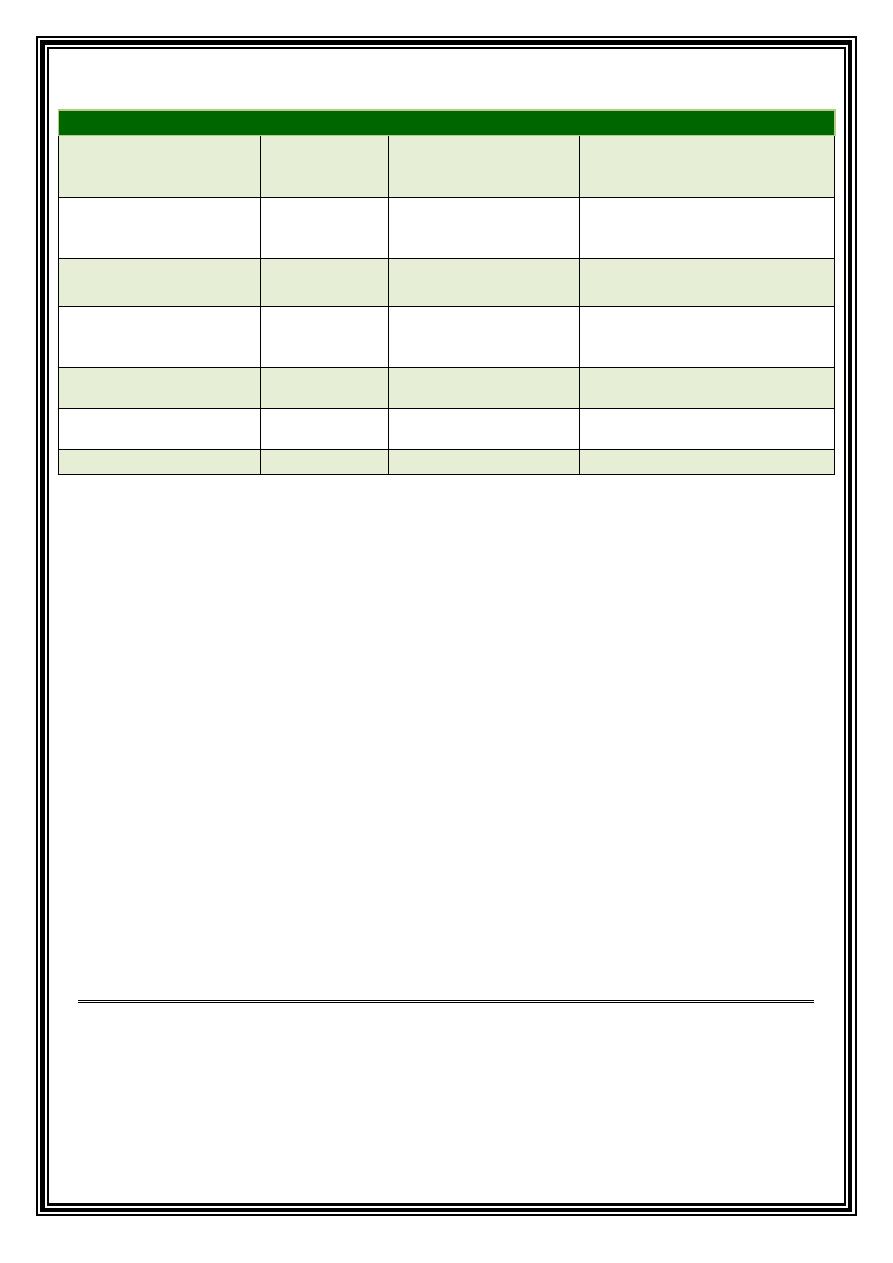
Rx. for candidiasis
1.
Search for underlying local or systemic condition
a.
Correct vertical dimension of the denture (for angular cheilitis)
b.
Reline ill-fitting denture and instruct patient not to wear it at night
Page4
2.
Antifungal therapy
2. Syphilis:
secondary syphilis is characterized by mucous patches which appear as
superficial white to yellow ulcer (snail tract ulcer), seen on palate, tonsils, buccal mucosa, in
addition to associated systemic manifestation such as generalized lymphadenopathy and
maculopapular rash.
Tertiary syphilis is characterized by:
a.
Gumma: swelling affecting palate followed by necrosis and destruction and
perforation of the palate.
b.
Syphilitic leukoplakia of the tongue (premalignant)
c.
Atrophic glossitis: depapillation of tongue in addition to shrinkage due to
endarteritis obliterans
Dx.
a.
History and clinical features
b.
dark field examination (U.V. light + silver stain) for primary syphilis
c.
Serum tests: non-specific (VDRL, Wassermann), specific (fluorescent treponemal
antibody absorption test FTA-ABS)
3. Measles or rubeola:
acute contagious viral infection mostly affecting children,
characterized by fever, lymphadenopathy, cough, nausea, photophobia, development of
rash affecting head, hair line, back of the ear, chest, back and extremities
Intraorally appears as greyish to white spot surrounded by red zone, mostly affecting buccal
mucosa seen in 97% of cases called (Kopeck’s spots), treated by bed rest.
Previous:
Introduction
part 2
Oct 4
Current:
Red and white lesion part 1
Oct 25
Next:
Red and white lesion
part 2
Nov 1
Later:
Red and white lesion
part 3
Nov 8
Generic Drug
Brand Name
Dosage
Considerations
0B
Nystatin
Mycostatin
100,000–200,000 IU 1x4
7-10 days
Tab 500,000 IU
Drops for infant
Powder for denture
Ketoconazole
(imidazole derivative)
Nizoral (tablets)
200 mg 1x1 or 1x2
10% gel
Interact with erythromycin
Not used with antacids
(acidity increases absorption)
Clotrimazole
(imidazole derivative)
Mycelex
10-mg oral troches 5/d
Fluconazole
(Azole derivatives)
Diflucan
(tablets)
100 mg 1x1 or 1x2
Not used as first line due to
resistance development
Itraconazole
Sporanox
100 mg 1x1
Potentiates phenytoin, oral
hypoglycemic drugs and warfarin
Amphotericin B
Tab or solution 100 mg
I.V. 25 mg
For severe cases
Gentian violet
Antifungal and antibacterial
Page5
D. Traumatic white lesion:
1. Traumatic keratosis
: occur in an isolated area of oral mucosa, appears whitish and
thickened, occur due to local irritation or an identifiable cause, such as: clasp, denture
flange, sharp edge, orthodontic appliance, malposed teeth (upper and lower wisdom teeth)
**Treatment: remove the cause and follow up, biopsy should be taken if lesion persists
2. Nicotinic stomatitis (not premalignant):
Localized to the palate in heavy smoker
(cigarette, cigar and pipe)
Early lesion appear reddish subsequently develops into whitish thickened fissured lesion
affecting mainly the palate, sometimes local thickening around orifice of salivary gland with
sometimes red spot at the center (Inflamed minor salivary gland), sometimes may stain
brown due to tar
**Dx.: clinical, history
**Treatment: stop smoking and follow up
3. Papillary hyperplasia of palate:
seen in denture (ill-fitting or rocky), usually symptomless,
polypoid granulated erythematous elevations
**Dx: presence of irritant(denture)
**Treatment: remake denture and follow up, biopsy should be taken if lesion persists
E. Blood Dyscrasias
1. Anemia:
oral examination shows pallor in oral mucosa + atrophic glossitis (depapillation)
2. Plummer Vinson syndrome (premalignant condition)
(Paterson Brown Kelly syndrome,
Sideropenic dysphagia): Affecting mid age female and is a triad of:
a.
Fe deficiency anemia
b.
Dysphagia due to post cricoid web (oral, pharyngeal and esophageal ca. may occur)
c.
Glossitis
**Dx.
U
clinically
U
(glossitis, burning, angular cheilitis, koilonychia-spoon shaped nails- and
other symptoms of Fe deficiency anemia)
U
Investigations
U
: Barium swallow-shows esophageal web-
**Treatment: refer to physician to treat underlying cause
Page6
F. Drugs (Vit. A def,
Aspirin, Drug reactions)
1. Vitamin A deficiency:
white lesion or leukoplakic lesion in oral cavity and other parts
(taste, retina-Night blindness- and skin)
Treatment: supplements, Found in vegetable (Carotene, found in carrot)
2. Aspirin burn:
chemical burn happens when aspirin comes accidentally in contact with
mucobuccal fold and sulcus to relief pulpitis, periapical abscess and periosteitis.
Dx. History of pain + using aspirin
clinically: irregular pseudomembranous white lesion, painful, adjacent to offending
area the entire cheek mucosa is affected
3. Drug reactions(3 types)
a.Lichenoid drug reaction:
mimic L. planus clinically & hist. but with eosinophil in submucosa
Etiology of Lichenoid drug reaction: variety of drugs:
A.
Antihypertensive (thiazide, alpha and beta blocker..... practolol, labetalol, L-dopa)
B.
Hypoglycemic agent( chlorpropamide, tolbutamide)
C.
Antibiotics (tetracycline, Erythromycin, Dapsone)
D.
Anti-Rheumatoid arthritis (gold salt)
E.
Anti-malarial drugs (chloroquine)
F.
Penicillamine (chelating agent)
G.
Developer solution
H.
Iodine
Clinically: affecting mouth, skin, back and extremities
b. Stomatitis venenata (contact stomatitis)
:
U
Localized
U
, irritant could be any restoration
(amalgam, Cr-Co, lip stick, face powder, tooth paste-cinnamon-, composite, gold, acrylic)
c. Stomatitis medicamentosa:
U
Diffuse
U
oral and other part of body…clinically similar to
erythema multiforme
G. Dermatological
(lichen planus, Psoriasis, SLE)
1. Lichen Planus:
mucocutaneous disorder, affecting mouth and other parts of the body
Both oral and skin lesion might be seen together, oral may precede skin lesion or vice versa
**Varieties of lichen planus (10 varieties)
a)
Reticular..... as network lace like of elevated white lines on buccal mucosa bilaterally
Chief complaint: roughness, brownish pig (pigmented l. planus)
b)
Erosive..... Either minor or major.. diffuse erosion with well demarcated white lines
at periphery, painful, burning ... premalignant
c)
Desquamative gingivitis... diffuse desquamation, very painful, resist treatment
Page7
d)
Papular.... aggregation of many papules within o. cavity
e)
Bullous.... represent acute phase of disease... may rupture
f)
Atrophic glossitis...... depapillated dorsum of the tongue
g)
Atrophic..... painful , chronic red lesion
h)
Leukoplakia-like.... appear as w. patch
i)
Annular... circle like
j)
Linear lesion
**Etiology of lichen planus :
I. hyper sensitivity reaction,
II. Immunological reaction, recently …is associated with lichen planus antigen,
III. Hepatitis C
Note: Grinspan's syndrome= D.M+ oral Lichen planus+ Essential hypertension
**Skin lesions: development of violet polygonal flat-topped papules affecting flexure aspect
of arm and lumbar region, pruritus
**Other areas: Genital same as oral, Nails ( longitudinal fissuring and grooving)
**Chief complaint of patient: Pruritus(skin), burning and roughness(oral)
**Lesion examined by lens shows white lines of thickened granular layer (Wickham stria)
**DX.:
Clinical feature, Histopathology(pathognomic) acanthosis, hyperkeratosis, saw tooth Rete
pegs, submucosal bands of T-cell (Differs from SLE where there is no t-cells),
Immunofluorescence: shaggy bands of florescence along basement membrane
**Treatment
I. Reassurance in asymptomatic
II. Topical corticosteroid (Kenalog in Orabase, clobetasol, intralesional in erosive type)
III. Keratolytic agent: Tretinoin(retinoic acid)0.025 mg 1x2……. Also used for Acne 0.1 mg,
Isotretinoin... topical , Etretinate (teratogenic), Tema-Retin(systemic)
IV. In resistant cases... cyclosporine(cytotoxic)
V. Cryotherapy or LASER
Symptomatic lichen planus lesion treatment :
a. Antihistamine mouth wash
b. Search for systemic cause
Previous:
Red and white lesion
part 1
Oct 25
Current:
Red and white lesion part 2
Nov 1
Next:
Red and white lesion
part 3
Nov 8
Later:
Oral Ulcer
part 1
Dec 6
Page8
G. Dermatological
(lichen planus, Psoriasis, lupus)…….contd.
2. Psoriasis:
starts in 2nd and 3rd decade of life characterized by development of
papule and plaques that are covered by scale, if scale is scraped off, tiny pin point
area of bleeding called Auspitz sign is seen.
Lesions occur bilaterally and symmetrical mostly affecting scalp, elbow, knee and
area of local trauma (Koebner's phenomenon).
Severe forms (postural psoriasis): +TMJ involvement called (Arthritic psoriasis)
White plaque or erythematous ulceration in addition to development of geographic
tongue and fissured tongue
*Treatment: according to severity
1.
No treatment in mid cases
2.
Moderate cases: topical corticosteroids
3.
Severe: systemic retinoids, cyclosporine ,methotrexate and UV light
4.
Symptomatic treatment: topical analgesia
=========
3. Lupus Erythematous:
Autoimmune ,three types (Discoid, sub-acute and SLE)
a. Discoid:
common form occurs in 3rd and 4th decades, characterized by:
•
Oral lesion: oral ulceration on erythematous base with white radiating
lesion at periphery and is not well demarcated
•
Skin lesion: erythematous macule affecting malar region and bridge of the
nose (Butterfly lesion) considered diagnostic for LE
b. Subacute:
mild form of lupus, involves legs & trunk
c. SLE:
middle form, skin+ oral+ internal organs (joints, blood vessels, bone
marrow)
Dx. of lupus :
1- History,
2-Clinical features (butterfly lesion)
3-Biopsy: ( H&E )& Immunofluorescence (antibodies attached to basement
membrane)
4-Other investigations: C.T. disorders, +ve antinuclear antibody, +ve RF, false +ve
for Syphilis,
▲ESR, if involves bone marrow>>> ▼R.B.C, ▼W.B.C, ▼platelets
Treatment: corticosteroid, antimalarial drugs>> chloroquine
Page9
H. Premalignant (leukoplakia, erythroleukoplakia, s.m. fibrosis)
1. Leukoplakia
: White patch or plaque that cannot be characterized clinically or
pathologically for any other disease
Clinical features: affecting middle and older aged people (majority in 40's)
Predisposing factors
1-Chemical and mechanical irritation
2-Tobacco (all types)>> the main cause is smoking
3-Alcohol
4-Infection: chronic hyperplastic candidiasis, 3
P
et
P
syphilis,
5- Avitaminosis A&B
6-Hormonal
Clinically: whitish or greyish small well circumscribed lesion on cheek mucosa and
tongue (mainly), lip, palate, floor of the mouth, buccal mucosa
Varieties: homogenous, Nodular, Verrucous, Proliferative
a. Homogenous (thick):
Well defined white patch, localized or generalized more
extensive slightly elevated fissured or corrugated on tongue
Differential dx : hairy leukoplakia, leukoplakia
b. Nodular (speckled):
Non homogenous mixed red and white lesion in which
keratotic white patch or nodules are distributed over an erythematous
background and is associated with high malignancy transformation rate
c. Verrucous (verruciform):
thick white lesion with papillary surface
d. Proliferative verrucous leukoplakia (P.V.L)
extensive papillary white plaque
involving multiple mucosal sites, may transform into Squamous cell carcinoma or
verrucous carcinoma or severe dysplasia.
*If dysplastic changes involve all layers of epithelium called ca in situ
Dx. Clinical, biopsy
Treatment :
1-remove any local factor and underlying systemic condition
2-Surgical excision of small lesion (dx and treatment)
3-Keratolytic agent
4-Gingival leukoplakia: by cryotherapy, LASER
U
*NO
U
TREATMENT SHOULD BE GIVEN
U
BEFORE
U
BIOPSY
Page10
2. Erythro leukoplakia
Bright red velvety plaque or patch that cannot be diagnosed clinically and
pathologically as any other condition, sometime slightly depressed so called
(erythroplasia)
*Red lesions are due to allergy or infection
Uncommon in mouth, but caries highest risk of malignant transformation, sometimes
lesion is already malignant on first biopsy
Clinical types:
1. Homogenous 2. Granular (speckled) 3. Leukoplakia interspersed
with patches of Erythroplakia
Dx.:
Clinical: Occur in old man 6th and 7th decade of life
Sites: floor of the mouth, ventrum of the tongue, soft palate, tonsillar region
Histopathological study shows sever epithelial dysplasia, carcinoma in situ and
squamous cell carcinoma
TREATMENT depends on biopsy
3. Submucosal fibrosis
: Slowly progressive chronic fibrotic disease of oral cavity and
oropharyngeal region, characterized by: fibroelastic changes, inflammation of
mucosa, progressive inability to open mouth, swallow, or speak
*Is a premalignant oral lesion
Etiology: spicy food, betel nuts (psychoactive)
Dx.
1. History (search for abnormal dietary habit)
2. Clinically: burning, Increase or decrease salivation, vascular lesion, submucosal
whitish opaque band, limitation in mouth opening
3. Biopsy
I. Miscellaneous (Oral skin graft, Geographic tongue)
1.Oral skin graft:
pieces of skin grafted intraoral cavity for replacement of surgically
removed lesion, treatment of oroantral fistula, appear white due to imbibition of
water by stratum corneum
Previous:
Red and white lesion
part 2
Nov 1
Current:
Red and white lesion part 3
Nov 8
Next:
Oral Ulcer
part 1
Dec 6
Later:
Oral Ulcer
part 2
Dec 13