LEC:4 د. علي الشالجي
Brain Tumors
Classification
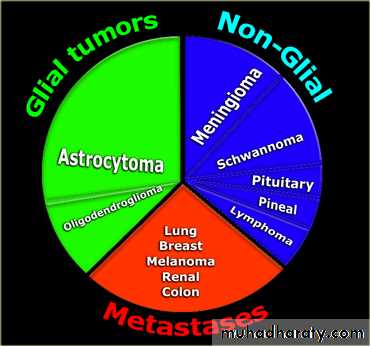
Brain tumors are classified into 2 types:
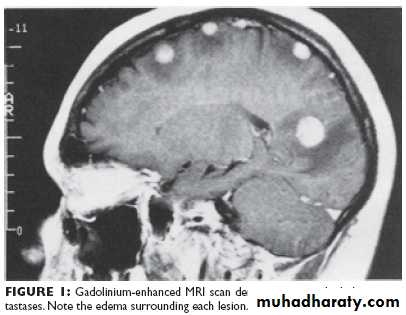
Secondary tumors:These are the most common brain tumors; the primary tumor is mostly in the breast or in the lung. It is usually multiple lesions in the brain, CTscan will show multiple lesions surrounded by oedema. Once diagnosed the Rx is usually radiotherapy or cytotoxic dugs.
Surgery has a limited role in the management of secondary brain tumors , and is used only for a single relatively big metastasis that is excisable as palliative Rx or for multiple lesions without an obvious primary lesion so we do diagnostic biopsy.
2- Primary tumors:
These are usually single (not multiple), can be benign or multiple malignant, but even in malignant tumors, there is no distant metastasis. And if it occurs, isusually local in the malignant there is usually recurrence after removal of the tumor.
Classification of the primary tumors
Depends on the site of origin:Gliomas
These are the most common primary tumors they arise form the glial cells which are part of the supportive tissue of the brain
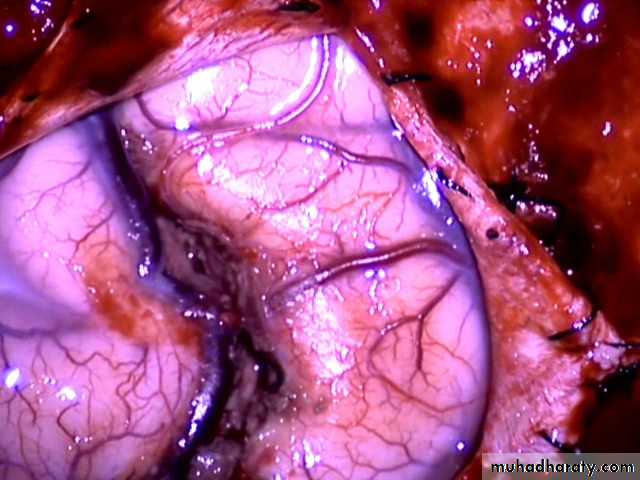
(LOW GRADE GLIOMA (INTRAOPERATIVE)
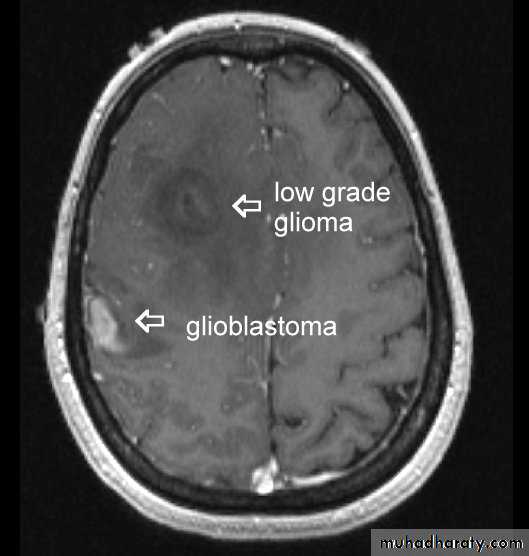
There are many types of glioma with different degrees of malignancy:
Astrocytomas:have 4 grades I -> IV. These are the most common gliomas, there are 4 grade of astrocytoma depending on the degree of malignancy, it can affect any age , usually yellow - whitish in color affecting both cerebrum and cerebellum , it can affect ages from 2 months ~ 95 years.

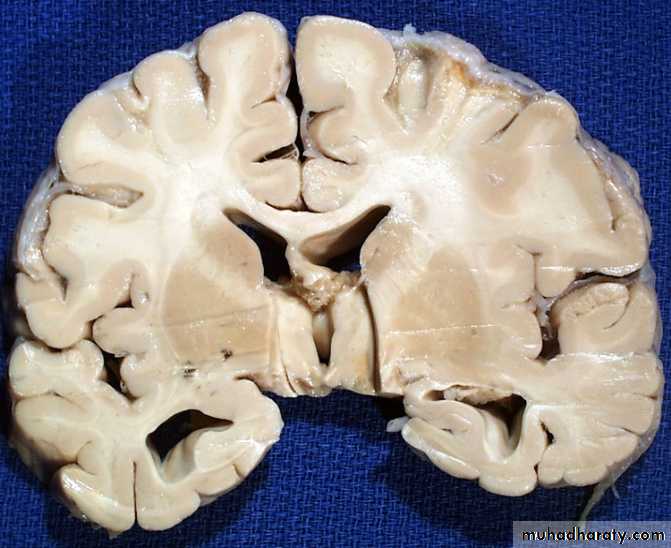
Glioblastoma multiformis:
The most malignant brain tumor, rapidly growing , red in color, highly vascular mainly affecting the cerebrum , some pathologists classify it as astrocytoma grade IV.Medulloblastoma:
Tumor of childhood, affecting the posterior fossa, usually a midline tumor & highly malignant.
Oligodendroglioma:
this is relatively benign, affecting mainly the cerebrum, carries the best prognosis of glioma, if treated properly by surgery & radiotherapy.
Ependymoma:
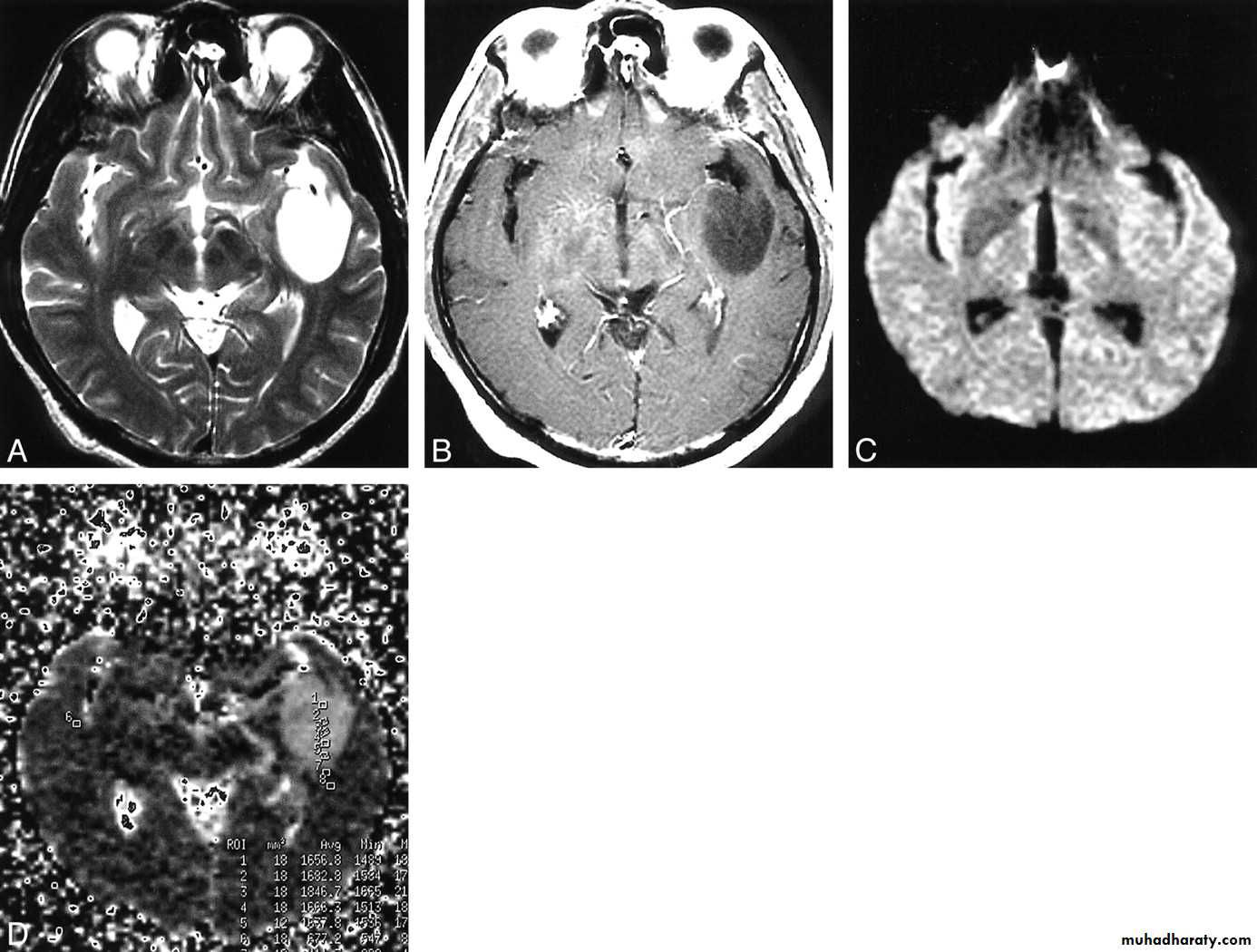
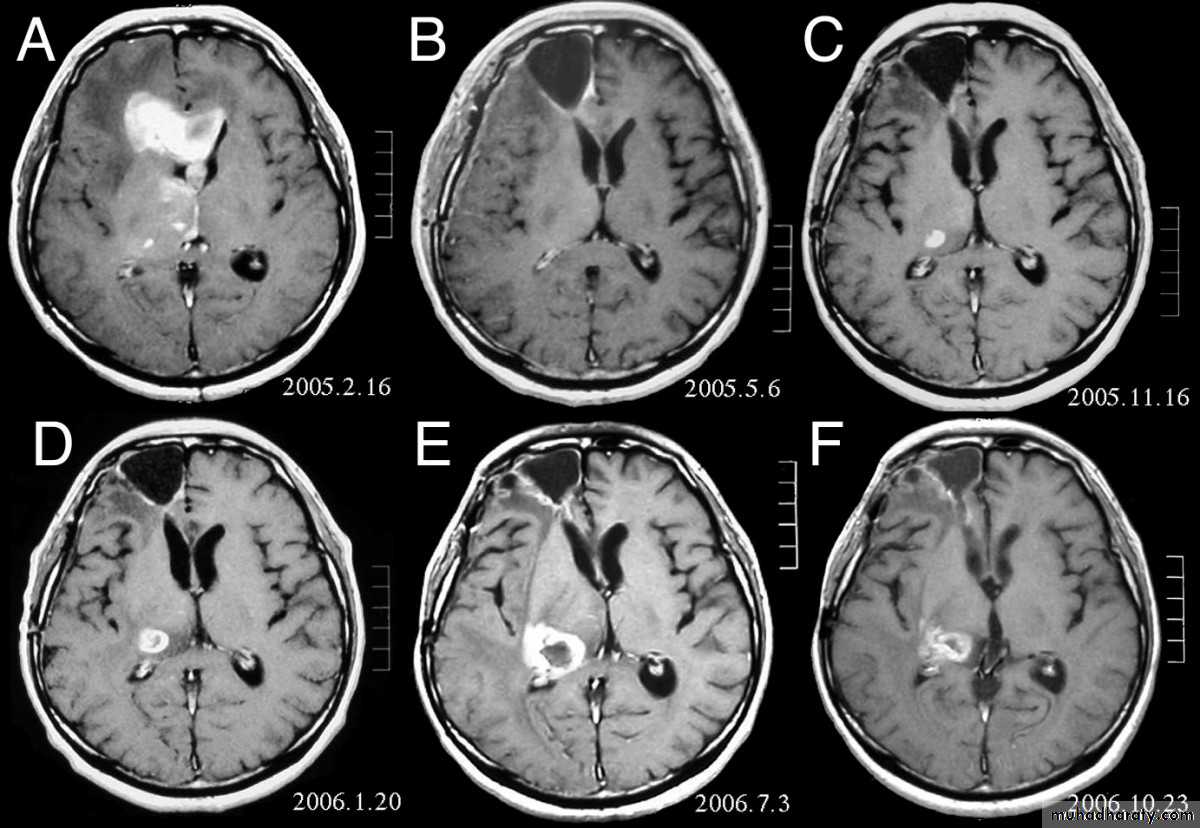
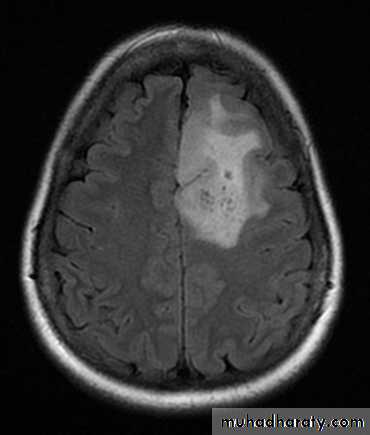
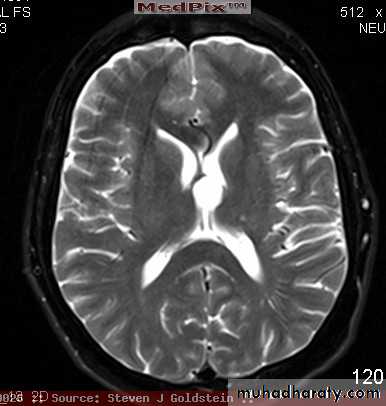
arise from the epidermal lining of the ventricular system, usually whitish in color & can lead to early hydrocephalusCT scan of all gliomas shows usually hyperdense lesion, irregular in shape, surrounded by edema & may be enhanced with or without cystic degeneration.
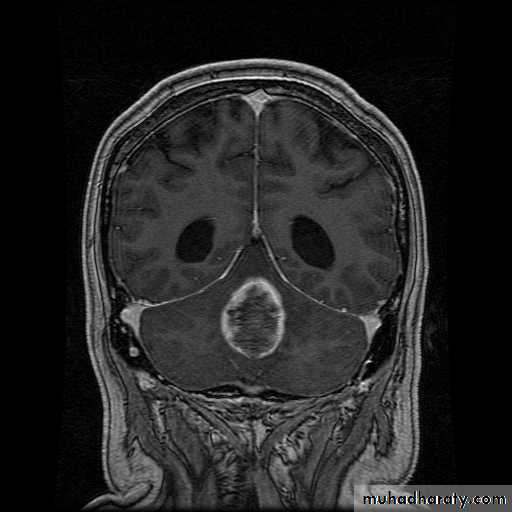
( CORONAL MRI )
Note: all gliomas are dealt with by surgical intervention ,by excision of the tumor followed by radiotherapy , but prognosis is not very good & fluctuates from 5 years survival of less than 5% in Glioblastoma multiformis to up to 100% 5 years survival in Oligodendroglioma treated by surgery & successive radiotherapy.
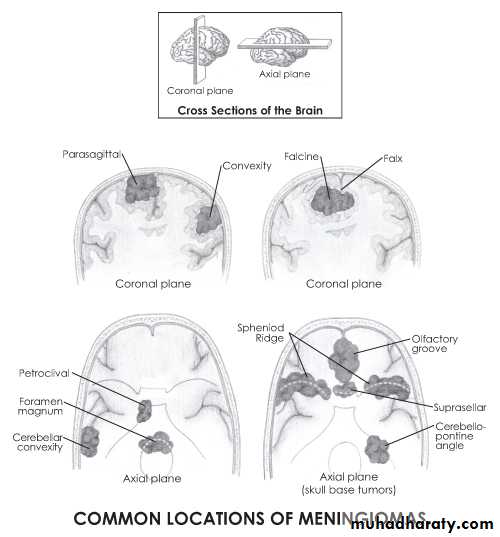
Meningiomas:
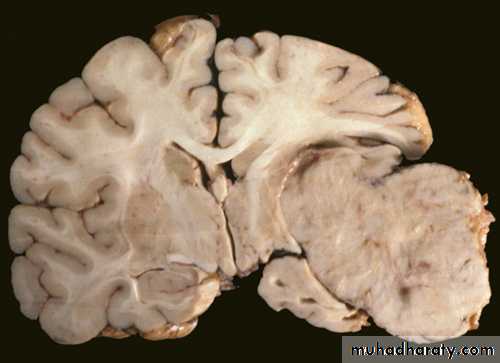
- Arise from the arachnoidal cells, mainly arachnoidal villi, more along the venous sinuses.
- Usually big , lobulated , very vascular, gray to red in color, it is usually benign & complete removal can lead to complete recovery & excellent prognosis:
- CT scan will show hyperdense , circular ,well - circumscribed lesions.
Blood vessels tumor:
Angioblastoma:usually affects the cerebellum & sometimes the retina.
Angiomas:
- usually congenital & of many types capillary, venous, or arteriovenous.
- It's a mass of tortuous blood vessels, supplied by one artery & drain by 1 vein it is usually presented by epilepsy.4- Pituitary & 3rd ventricular tumors :
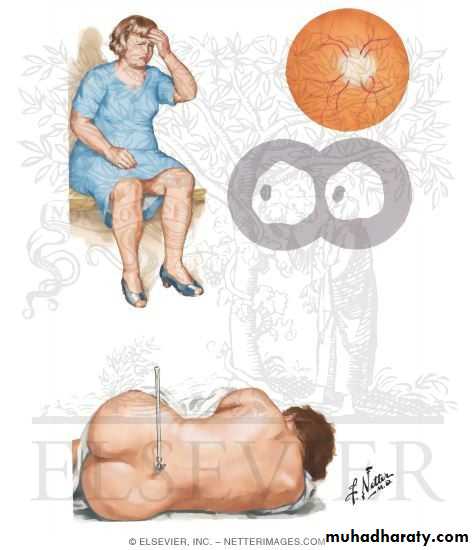
Pituitary tumors :Local mass effect :
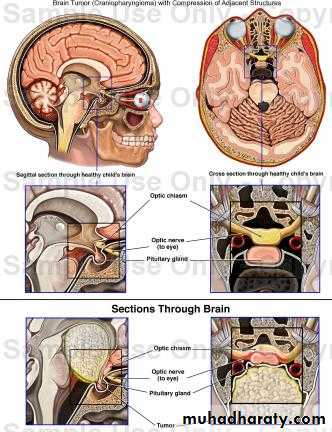
Visual field disturbance ( bitemporal heminopia ) due to compression of optiac chiasmaHeadache due to expansion of pituitary fossa with dural stretching
Hormone difficiency ( hypo-pituitarism )
Hormon excess
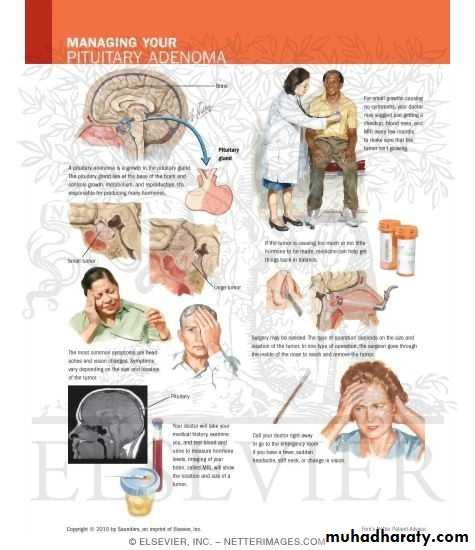
(PITIUTARY TUMOR)
They are named according to their sites on light microscopy
Chromophobe aedenomas(80%): presented by picture of hypopituitarism due to the destruction of the pituitary gland. and visual disturbance : bitemporal heminopia due to tumor compression on optic chiasmaChromophil adenomas ( 15% ): these are secretary tumors can lead to gigantism in childhood or acromegaly in adults
Prolactinomas: these are prolactine secreting tumors
in females they present with amenorrhea, infertility & galactorrhea,
males present with gynecomastia & frontal boldness.
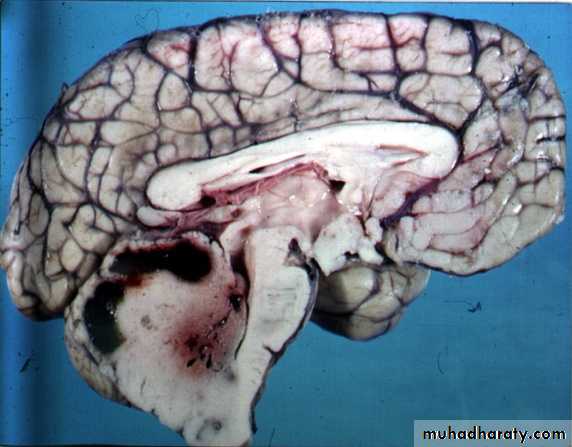
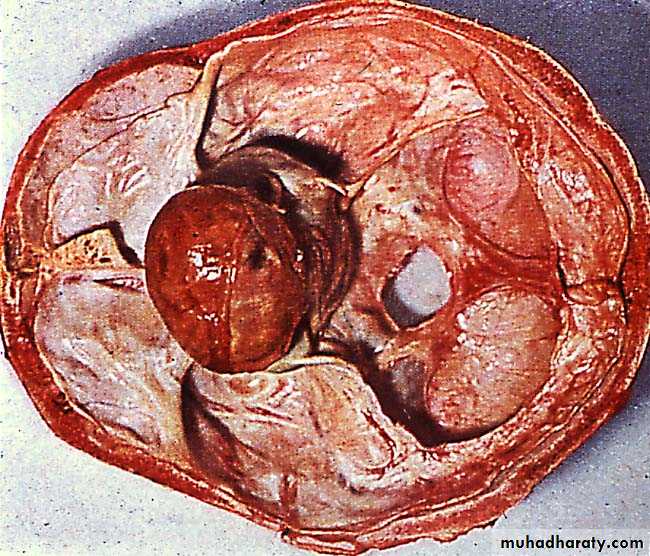
Craniopharyngiomas: arise from the remnant of the buccal ectoderm of the pharyngeal pouch , can present at any age 90% are cystic containing dark brown fluid like engine oil , full of cholesterolclinically presented by visual disturbances as bitemporal hemianopia with hydrocephalus
CT scan will show mixed hyper and hypodense lesions , with cystic components with or without hydrocephalus.RX is usually surgical by craniotomy or trans-sphenoida approach.
Colloid cyst of 3rd ventricle: small cystic tumor, it can lead to early
hydrocephalus (huge) although it is very small tumor
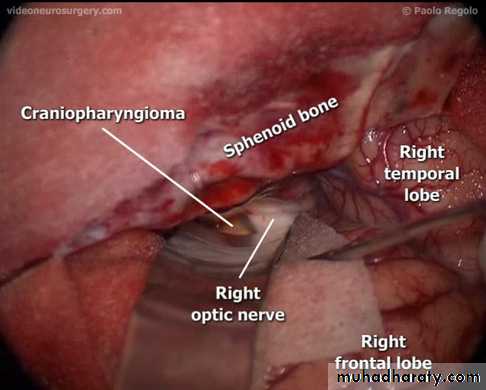
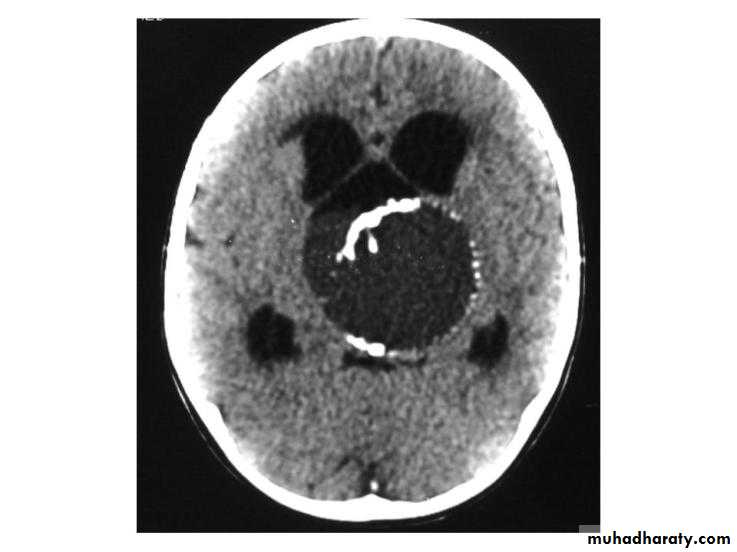
CRANIOPHARYNGIOMA (INTRA-OPERATIVE) / CT-SCAN
8th nerve tumors (acoustic, neuroma or shwannoma )
these are relatively common tumors , usually benign , although recurrence is reported , it arises in the Mcerebello-pontine angle
- it usually presents by unilateral deafness or difficulty in balance, or trigeminal anesthesia or facial palsy ( it is a benign tumor in malignant place).
* Unilateral deafness in young is highly diagnostic sign of this tumor.

SKULL X-RAY FOR A PATIENT WITH PITIUTARY TUMOR ( ERROSION OF SELLA TURSICA )
Investigations for pituitary tumors :MRI
Visual field Mapping to look for evidence of bitemporal heminopia
Hormonal assessment
Treatment
Tumors that produce pressure on optic chiasma : treated by intracapsular removal by trans-sphenoidal route
Prolactinomas : usually responde to dopamine agonist ( like : cabergoline )

Benign intracranial hypertension ( Pseudo-tumor cerebri )

It is a syndrome that is defined by five criteria:
1-Increased intracranial pressure
2-Normal or small sized ventricles by neuroimaging3-No evidence of an intracranial mass
4-Normal CSF composition
5-Papilledema
It affects females > males usually around or < 40 years, obese & the patient usually has a severe headache with papilledema & rarely 6 nerve palsy but not focal signs
Clinical Feature
Diagnosis:
CT scan is usually –ve , so diagnosis is made by examination of other causes of increase ICP. It is usually a self-limited disease, but rarely papilledema is so severe & can lead to secondary optic nerve atrophy & blindness.
Treatment:
Steroids : In heavy doses, especially in early disease (IV or IM).Analgesics.
Diuretics.
Lumbar puncture: repeatedly for diagnostic & therapeutic purposes
Very occasionally we may need to do lumbp-peritoneal shunt.
* We do lumbo-peritoneal shunt because the ventricle is very small and there is a difficulty to see it.