1
Fifth stage
Surgery
Lec-3
.د
بسام
6/12/2015
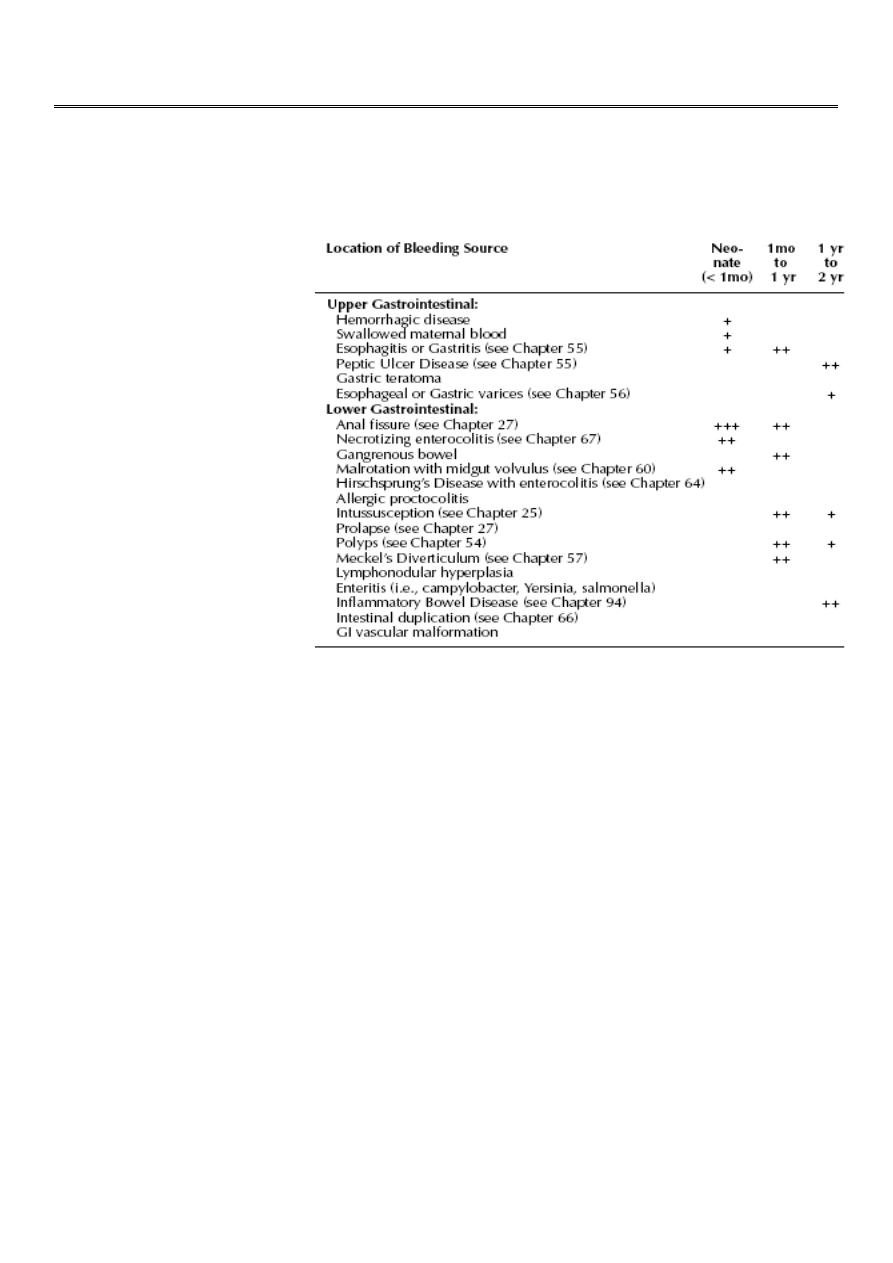
Bleeding from Alimentary Canal
Introduction
Hemorrhage can occur
from any part of the
G.I.T. and at any age.
Sometime massive and
sometimes it’s a sign
of other medical or
surgical pathology.
Symptoms depends on
level and rate of
bleeding.
Causes of GIT bleeding
1- Blood in vomitus:
A- Coffee Ground vomiting:
Pyloric stenosis.
Reflux esophagitis.
Nonspecific gastritis.
Mallory Weiss syndrome.
B- Hematemesis (frank blood):
Esophageal varices.
Peptic ulcer.
C- Other:
Nasal bleeding.
NGT. Ulceration.
D- Rare causes:
Tonsil aneurysm.
Foreign body perforation of aorta.

2
2- Occult Blood
A- Reflux esophagitis.
B- Haemangioma of bowel.
C- Polyps of the bowel.
D- Inflammatory bowel disease.
3- Rectal Bleeding
A- Neonatal
Necrotizing enterocollitis.
Volvulus with ischemia.
Hemorrhagic disease of newborn.
Gastroenteritis.
Anal fissure.
Maternal blood.
B- Sick child with acute abdomen:
Intussusceptions.
Gastroenteritis.
Henoch-schonlein purpura.
C- Major hemorrhage:
Esophageal varices.
Acute peptic ulcer.
Gastric erosion.
Duodenal ulcer.
Meckel’s diverticulum.
Tubular duplications.
D- Small amount of bright blood in a well-child:
Anal fissure.
Polyps.
Unrecognized prolapse.
Hemorrhoids.
Idiopathic.
E- Chronic illness with diarrhea:
Crohn’s disease.
Ulcerative colitis.
Nonspecific colitis

3
Classifications
*Blood in vomitus
1- Coffee ground vomiting: Blood mixed with gastric content.
A. Pyloric stenosis.
1:600 infant
1 month old infant
3 cardinal sign?
B. Reflux esophagitis.
Mucosal ulceration
Effortless vomiting
Treatment:
o Positioning.
o Reduce gastric acid
o Surgery
C. Nonspecific gastritis.
D. Mallory Weiss syndrome.
Occur in any child who vomit or retch continually.
Split in upper gastric mucosa.
Respond to medical treatment.
2- Hematemesis: large amounts of frank blood/significant blood in stomach.
A. Esophageal varices: secondary to portal hypertension.
Intrahepatic secondary to:
o Biliary atresia.
o Inborn error diseas.
o Chronic viral hepatitis.
o Cystic fibrosis.
Extra hepatic secondary to portal vein thrombosis in neonate.
Treatment:
Endoscopic.
Sengstaken-blakemor tube in massive bleeding.
Surgery either over sewing of the varices or shunt procedure.

4
B. Peptic ulcer:
Stress ulcer secondary to burn, cerebral tumor and head injury. It cause diffuse
ulceration, sometimes duodenal.
Drugs.
H-pylori in adolescent.
Treatment:
Resuscitation.
Endoscopy.
Treat the cause.
Surgery rarely required.
3- Other causes:
Nose bleed.
N.G.T. ulceration.
4- Rare causes:
Aneurysm in tonsil bed.
Foreign body perforation of aorta.
*Occult bleeding:
It cause iron deficiency anemia.
1. Reflux esophagitis.
2. Bowel haemangioma.
3. Polyps.
4. Inflammatory bowel disease.
Rectal bleeding
A- Neonatal bleeding
Surgical Conditions:
1-Necrotising Enterocollitis (NEC):
It’s common in extreme premature baby.
Incidence increase with the advance nursing care.
Radiological finding:
o Pneumatosis intestinalis
o Portal v.gase.
o Pneumoperitonium

5
Treatment:
o Adequate ventillatory care.
o Resting for GIT.
o Antibiotics.
o Surgery if full bowel necrosis or no response to supportive treatment.
2- Volvolus neonatorum with ischemia:
Any age can be affected but mainly neonate.
Predisposing factors are malrotation with narrow mesentery
Which allow easily twisting of the entire mid gut.
Clinical features:
o Bile stained vomitus.
o Failure to pass meconium.
o Mild abdominal distention.
o midgut ischemia may cause shock and rectal bleeding(late sign).
Treatment:
o Urgent surgery by de twisting and ladd procedure.
o If mid gut gangrene it carry high mortality rate.
Non-surgical conditions:
1. Hemorrhagic disease of newborn.
2. Gastroenteritis
3. Anal fissure.
4. Swallowed blood.
B- Small amount of blood in a well-child:
It’s the most common group.
1- Anal fissure:
Secondary to constipation, usually in the midline.
Pain on defecation &bright red blood on the stool.
The can be seen by inspection.
Do not do rectal examination?
Sometimes a sentinel pile is visible.
Treatment:
o Treat the constipation.
o Local anesthetics.
o Surgery rarely indicated.
2- Polyps:
Suspected in painless bleeding.
Juvenile polyp.

6
3- Rectal prolapse:
Easy diagnosis by history and examination.
Secondary to chronic diarrhea, constipation, malabsorption and cystic fibrosis.
4- Hemorrhoids:
Rare in children.
Cause painless fresh bleeding.
Usually treated conservatively.
5- Idiopathic.
C- An ill child with an acute abdominal conditions:
1- Intussusception:
Vomiting, colic, screaming attacks and palpable sausage massper abdomen.
Current jelly stool (mixture of blood and mucus).
Treatment: Reduction, either surgical, hydrostatic or pneumatic.
2- Gastroenteritis:
In sever GE blood mixed with stool.
3- henoch-schonlein purpura:
Cause arthralgia.
Skin rash
Abdominal pain.
Rectal bleeding.
D- Chronic illness with diarrhea.
A- Crohn’s disease:
Fever, weight loss, and chronic blood loss.
Any part of bowel could be affected.
B- Ulcerative colitis:
Diarrhea more common, mixed with blood.
C- Nonspecific colitis.
E- Major hemorrhage per rectum:
1- Meckel’s diverticulum:
2% of population.
2 type of mucosa (ectopic gastric mucosa).
2 feet from iliocecal valve.
2 inches in length.
Gastric mucosa produce acid that cause ileal mucosal ulceration.

7
Clinical fetures:
Painless brick-red stool with associated anemia.
Blood transfusion may be required.
Bleeding stop spontaneously.
Diagnosis by isotope study or laparoscopy.
Treatment by resection with end to end anastomosis.
Complication:
1- Bleeding.
2- Intussusception.
3- Small bowel obstruction.
4- Diverticulitis.
5- Peptic ulceration with ilial perforation.
6- Strangulation.
2- Tubular duplications:
Less common.
Usually small bowel affected in the mesenteric side.
Communicate with the bowel.
May contain gastric mucosa and cause bleeding secondary to ulcer.
Diagnosed either by isotope study or laparoscopy.
3- Esophageal varices.
4- Acute peptic ulceration.
5- Gastric erosion.
6- Duodenal ulcer.