Lec: 3
د. باسل3/11/2013
العدد (4)
Chronic Tonsillitis
Usually follows acute or subacute attacks of tonsillitis, and is more common in children between the age of 4-15 years. There is a chronic inflammatory hypertrophy, usually associated with adenoid enlargement.
Clinical picture:
Persistent or recurrent sore throat.
Persistent cervical adenitis.
Marked tonsillar enlargement with congested anterior pillars.
Treatment is usually surgical( tonsillectomy ) if symptoms persist.
Tonsillectomy operation


Indications for tonsillectomy
The indications for tonsillectomy are subject of some controversy.1. Recurrent attacks of acute tonsillitis which are frequent and severe enough to interfere with the patient's general health (5-6 attacks/year for at least two successive years).
2. Peritonsillar abscess (quinsy) especially if occurred more than once.
3. Sleep apnea syndrome: Such children have tonsils, which meet in the mid-line and cause gross difficulty in breathing.
4. Tonsillectomy for biopsy purposes when the tonsil is thought to be the site of neoplasm.
Others:
1. Diphtheria carriers.
2. Recurrent attacks of otitis media.
3. Acute rheumatic fever and acute nephritis if streptococcus tonsillitis has been responsible for recurrence.
Contraindications
1. Bleeding disorders or clotting problems.
2. Acutely inflamed tonsil and recent upper respiratory tract infection. It is safer to wait 2-3 weeks because of greatly increased risk of postoperative haemorrhage and pulmonary complications respectively.
3. Epidemic of poliomyelitis: There is evidence that the virus may gain access to the exposed nerve sheaths and so give rise to the move fatal bulbar form of the disease
4. Cleft palate: because tonsillectomy leads to scarring of the soft palate which affects repair and speech.
Postoperative care
1. Nursing of patient in tonsillectomy position (head down lateral position).
2. Careful monitoring of vital signs. So that any haemorrhage can be detected.
3. Analgesia: paracetamol. NSAID should be avoided due to its effect on the coagulation process.
4. Encourage the patient to move the muscles of the throat by swallowing, talking and dinking. This movement will help in shedding of the slough from the tonsillar fossae allowing healing to take place.
5. Patients should be warned that referred otalgia may be a predominate complaint following tonsillectomy.
Complications
1. Haemorrhage
a. Primary: Occurs at the time of operation. It's due to recent infection, previous quinsy or severe scarring. It's controlled by ligation or diathermy. Excessive bleeding from both fossae raises the question of coagulation defect. Here blood transfusion may be necessary.
b. Reactionary haemorrhage, occurs within 24 hours after the operation. It's due to inadequate haemostasis at the time of operation. It's treated by preparing a blood and early return to the theatre where the vessel is ligated.
c. Secondary:- Occurs some 5-8 days after the operation. It's due to infection often associated with a refusal of the patient to eat or an URTI at the time of surgery. The patient should be readmitted to the hospital and a course of antibiotics is ordered.
2. Trauma: capped or carious teeth are at risk during tonsillectomy. Insertion of the mouth gag can lead to dislocation of the TMJ.
3. Infection: Pyrexia is not uncommon at the morning after tonsillectomy. Prolongation of the pyrexia is a sign of infection which if untreated may lead to secondary haemorrhage.
4. Otitis media: It should be distinguished from referred otalgia.
5. Chest complications: It's more likely to occur if the patient has an URTI at the time of operation or due to inhalation of blood or broken tooth.
Membranous Pharyngitis
1- Viral infection: Infectious mononucleosis.
2- Bacterial: Diphtheria and scarlet fever.
3- Fungal: Candidiasis.
4- Spirochaetes: Vincent's angina.
5- Blood dyscrasia: Agranulocytosis and leukaemia.
Infectious Mononucleosis (Glandular Fever)
It is a systemic infection by Epstein Barr virus which spread by droplet transmission with the mouth. It is a disease of young adults and characterized by an increase in atypical lymphocytes.Clinical Picture
It is characterized by prodromal period, followed by severe sore throat, odynophagia and low grade fever. On examination, the tonsils are covered by characteristic plaque, and petechial hemorrhagic spots on the palate. Transient maculopapular rash and this will almost invariably be seen if ampicillin is mistakenly prescribed.Generalized lymphadenopathy and Spleenomegaly in 50% of cases.
Investigations
1. CBP increase in atypical lymphocytes (mononuclear cells).2. Positive Paul-Bunnell and monospot tests.
Treatment
Is non specific
1. Antipyretics & analgesics.
2. Antibiotics play no role in treatment and ampicillin should never be used as it will cause a skin rash.


Infectious mononucleosis
DiphtheriaIt is a specific infection by Corynebacterium diphtheriae which is disseminated by droplet. Children are mostly affected with a mortality of 10%.
Clinical Picture
The disease has incubation period of 4 days. The patient is severely ill, although the temperature seldom rises above 38 oC.
On examination
The disease is characterized by the appearance of a membrane on the tonsils, soft palate and posterior pharyngeal wall. The disease may spread to affect the nasal cavities and nasopharynx. The membrane is usually grey in colour, firmly attached to the mucosa and leaves a bleeding surface when it's removed.
Tender and enlarged cervical lymphadenopathy.
Investigation
Swab is taken for bacteriological examination including part of the membrane.
Complications
Laryngeal obstruction and stridor which may need tracheostomy.
Myocarditis and neuritis. The exotoxin produced by the microorganism is toxic to the heart and nerves. Neuritis is in form of paralysis of soft palate and ocular muscles.
Treatment
Antitoxin: intravenous 20,000-100,000 units depending on the severity of the infection.Systemic I.V. penicillin. Erythromycin is used in penicillin sensitive individuals.


Chronic Pharyngitis
Non-Specific Chronic PharyngitisIt is a chronic and irreversible inflammation of the mucous membrane of the pharynx with hyperplasia of its various elements. The normal lymphoid tissues on the posterior pharyngeal wall undergo hypertrophy so called granular pharyngitis, and the lymphoid tissue in the posterior tonsillar pillar may undergo an overgrowth forming the lateral pharyngeal band.
Aetiology
The aetiology is usually obscure:
1- Recurrent attacks of acute pharyngitis.
2- Persistant neighbourhood infection as chronic sepsis in the nose and sinuses, teeth and gums. Bronchiactasis is said to be associated with chronic pharyngitis.
3- Exogenous irritants such as tobacco, alcohol and industrial fumes.
4- Gastroesophageal reflux disease.
5- Allergic factors.
Clinical picture
1. Discomfort and painful throat without fever or constitutional symptoms of tonsillitis and the condition persists for weeks or months.
2. Foreign body sensation in the throat.
3. Tendency to clear the throat, which results from postnasal drip bathing the posterior pharyngeal wall.
4. Tiring of voice (not hoarseness).
Examination
Simple (catarrhal) type: redness and congestion of the pharyngeal mucosa. The uvula may appear enlarged or elongated.
Hypertrophic (granular) type: small nodules are scattered on the posterior pharyngeal wall giving a granular appearance. The lateral pharyngeal bands may be prominent.
Treatment
1. Treat the cause: Appropriate treatment of postnasal drip –if present- ( by intranasal steroid), and acid reflux (by proton pump inhibitor).
2. Altering the patient habit in regard to smoking, alcoholism and food.
3. Reassurance by the exclusion of malignancy.
4. Soothing gargles such as crushed soluble aspirin.
5. Antibiotics if there is fever.
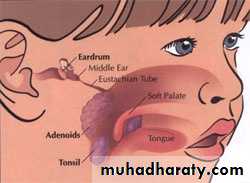
Adenoids
A hypertrophy of the nasopharyngeal tonsil, sufficient to produce symptoms, most commonly between 3-7 years of age.
Anatomy
The adenoids lie between the roof and posterior wall of the nasopharynx. Adenoids are present at birth, hypertrophy occurs in earlier years of childhood, maximum bulk is obtained at 6 years and atrophy at puberty.
Adenoids differ from tonsillar tissue in that it's bounded by no capsule, contains no crypts and covered by ciliated epithelium.

Symptoms
A-NasalNasal obstruction, mouth breathing, snoring and in severe cases obstructive sleep apnea.
Persistent nasal discharge & postnasal drip. The child may be described as " always having a cold".
Nasal speech (rhinolalia clausa).
B- Aural
Spread of infection along the auditory tubes producing recurrent attacks of otitis media and otitis media with effusion.
C-General
1. The infant tires easily, takes insufficient food and fails to thrive.
2. Mental dullness due to poor breathing and deafness.
3. Nocturnal enuresis and night terrors.
4. Pharyngitis and recurrent URTI.
Examination
1. Adenoid facies.
1. Open mouth.
2. Prominent upper incisor teeth.
3. Short upper lip.
4. Thin nose.
5. Hypoplastic maxilla.
6. High arched palate.
7. Dull expression due to hypoxia and deafness.
2. Mucoid and mucopus discharge from the nose with postnasal catarrh.
3. Posterior rhinoscopy and fibroptic endoscopy: lobulated mass, which occasionally extends laterally to the openings of the Eustachian tubes.
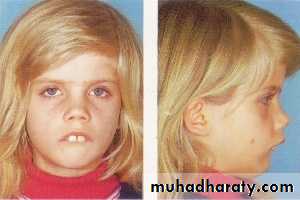

Adenoid facies

Investigations
X-ray of the postnasal space
Complications
1. Persistent snoring and sleep apnea syndrome.2. Recurrent URTI.
3. Recurrent attacks of acute otitis media and otitis media with effusion.
4. Orthodontic disturbances.
5. Speech problems (rhinolalia clausa).
6. Failure to thrive in infants.
Treatment
1. Conservative: in mild symptoms by
a. Treatment of allergy and sinusitis.
b. Local nasal steroids.
2. Surgical: if no response to medical treatment by Adenoidectomy + tonsillectomy + myringotomy
Contraindications
Cleft palate
As tonsillectomy
Complications
1. Haemorrhage (Primary, reactionary or secondary): It's treated by returning the child to the theatre where a post nasal pack is inserted under G.A. If blood loss is severe, a blood transfusion will be required.
2. Trauma to the uvula, soft palate and Eustachian cushions.
3. Hypernasality(Rhinolalia aperta): When the soft palate is insufficient to close the nasopharynx during speech. It occurs in case of submucosal cleft palate or after excessive scaring of the soft palate.
4. Incomplete removal and recurrence: Occurs because the adenoids are not encapsulated and its removal is a blind procedure.