General and Local Anesthesia
General AnesthesiaTerminology:
-Surgery-Operation
-Operating room (theater)
-Anesthesia/ Anesthetist

• (Operating Room/ Theater)

• (Operating Room/ Theater)
(Endotracheal tube/Endotracheal intubation)
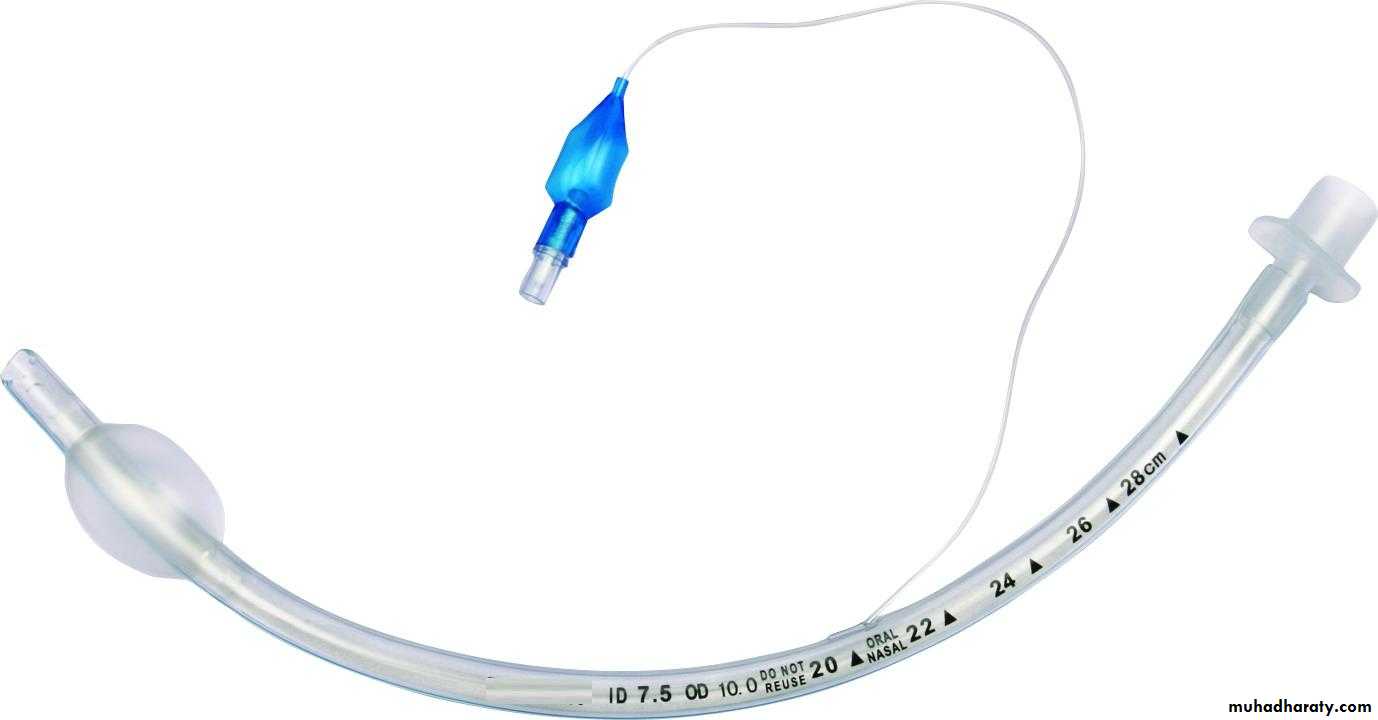
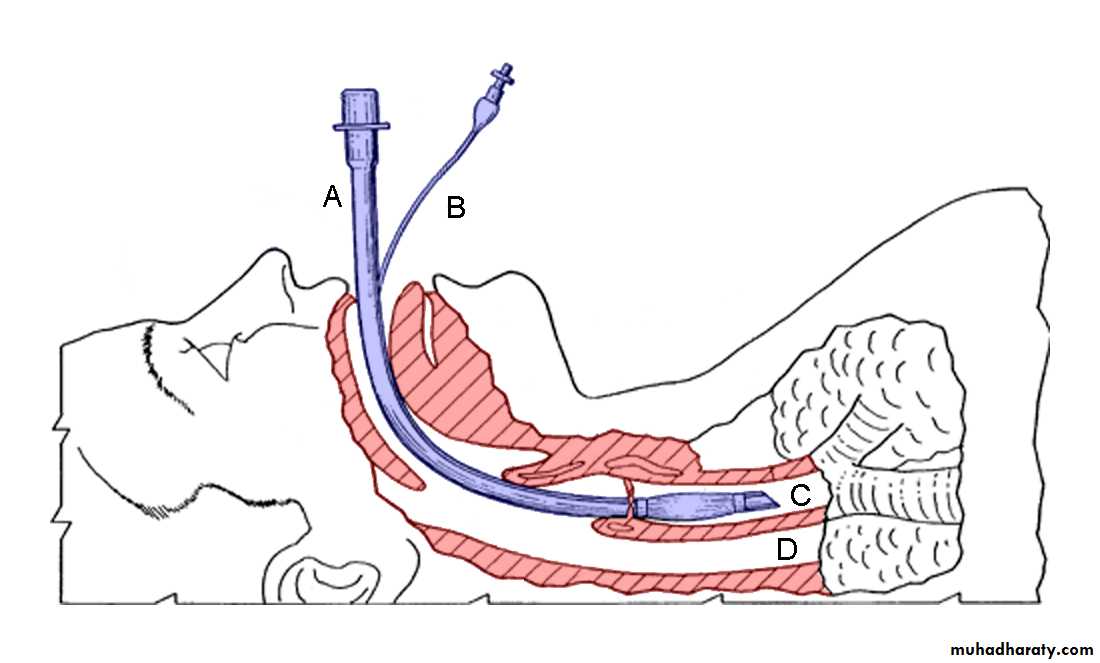
• (Endotracheal tube/Endotracheal intubation)

• (Endotracheal tube/Endotracheal intubation)

• (Endotracheal tube/Endotracheal intubation)

• (Laryngoscope)

• (Ambo Bag)

• (Ambo Bag)

• (Ventilator)
(Airway tube)
General Anesthesia:= Inducing
-Quick-Safe
-Easily reversible
Unconsciousness for any desired period of time.
Drugs in Anesthesia are given:
1- Before surgery2-During surgery:
-Unconsciousness-Analgesia
-Muscle relaxation
3-After surgery:
-Reversal of neuromuscular block-Relief of pain
other
Stages of General anesthesia:
Stage One: Analgesia
Stage two: Delirium*Stage Three: Surgical anesthesia 4 plans
Stage Four: Medullary paralysis, death
*Ether to non Pre-medicated patient
1-Before surgery: (Premedication)A- Anxiolysis and Amnesia.
Patient is apprehensive clear explanation of what to expect-Reassurance.
Very anxious patient can be helped by benzodiazepines
B-Analgesia for patient in pain.Or to:
Prevent post operative pain
-Parenteral opiates morphine
C-Drying of bronchial secretions.
Anti muscarinic drugsRarely used
Glycopyrronium is used one hour before surgery
Gastric content can lead to pulmonary aspiration:
-Single dose of anti acid-Ranitidine
-Metoclopramide
*Fasting for at least 6 hours before anesthesia
2-During surgery:The Aim is to induce:
-Analgesia-Unconsciousness
-Muscle relaxation (Intra abdominal surgery)
General anesthesia will include two steps:
A- Induction of anesthesia.
B- Maintenance.A-Induction: Usually IV (Pre-Oxygenated patient)
-Small doses of opiates-Fentanyl
-Followed by Thiopental (Ultra short acting Barbiturate)
or: Propofol
----Airway patency is maintained
(Oral airway + face mask)Or
(Endotracheal tube)
Endotracheal tube insertion require paralysis
with Neuromuscular BlockInhalation induction Sevoflurane
*(less common)B-Maintenance: (Inhalation)
-Nitrous oxide (N2O) and Oxygen
-Volatile agents +Oxygen + Air.-Isoflurane
-Sevoflurane
-Halothane
Or
Continuous iv infusion of Propofol (IV)
*(Less Common)
3-After surgery:
-Patient is not left alone until consciousness regained:-Effect of neuromuscular blockade either wane off or reverted by Antidote.
-Relief of painDissociative Anesthesia:
-Profound Analgesia
-Antegrade Amnesia
-Minimal Hypnosis
Mode of action:
On brain primarily on midbrain reticular formation system.Lipid solubility is important as the more lipid soluble is the drug the more its effect on the brain.
GABA receptor activation is also another proposed mechanism
Individual Anesthetics:1-Gases and Volatile Agents:
(Inhalation anesthesia)Effect correlate with the partial pressure of anesthetic agent.
*Agents with law solubility in blood provide rapid effect-N2O (Nitrous Oxide)
-Sevoflurane

When discontinued it moves from the tissue to the blood to the alveoli.
10 % of the expired volume and can lead to hypoxia.Treated by oxygen (Diffusion hypoxia)
*Fast Induction*Fast Elimination
Nitrous Oxide (N2O):
Gas used since 1844-Not inflammable
-Not explosive-Light anesthesia

• (Nitrous Oxide)
Advantages of Nitrous Oxide: (N2O)-Strong Analgesic action
50 % N2O in Oxygen provide profound analgesia.-Recovery is very fast
-Around 4 minutesDisadvantages of Nitrous Oxide : (N2O)
-Expensive-Must be used with more potent drug to produce surgical anesthesia.
***Post operative nausea and vomiting
Uses:
Use d to maintain surgical anesthesia with other agents e.g. IsofluraneDosage of Nitrous Oxide (N2O):
-Maintain anesthesia mixed with at least 30 % O2
-Analgesia: 50 % N2O + 50% O2Contra indications of Nitrous Oxide (N2O):
-Any closed distended air filled space will expand-Intra ocular surgery
-Middle ear
-lung
Precaution of Nitrous Oxide (N2O):
Adverse reactions:-Nausea and vomiting
*When used for more than 4 hours-Megaloblastic changes in blood.
-Teratogenicity to staff?
Halogenated anesthetics:
(Volatile Agents)
-Halothane
-Isoflurane-Sevoflurane
Isoflurane:
-Volatile colorless liquid-Not flammable under normal conditions
-Pungent odor
-Can cause bronchial irritation
-Minimally metabolized (o.2 %)


• (Vaporizer)
Effects of Isoflurane:
-Respiratory depression-Increased respiratory rate and tidal volume
CVS:
-Slight depression in CVS-And cardiac output
-Reduce Blood Pressure and peripheral vasodilatation.
Sevoflurane:
Chemical analogue to IsofluraneEnflurane causes more respiratory depression
Desflurane
Halothane (Fluothane):-Slow recovery
-Decrease cardiac output
-Sensitize heart to catecholamine (Arrhythmia)
-20% metabolized and induce liver enzymes
-Fever, anorexia, nausea, vomiting
***Hepatic damage (rare but serious)
Hepatitis is reported adverse reaction in 1:50000
Immune reaction



Oxygen in anesthesia:
-Supplementary O2 is always useful-With inhalation agents to prevent hypoxia
O2 concentration is 30%.... not exceed 80 %
Atmospheric pollution in operating theater:
-Fetal malformation-Miscarriages increased
-Hepatitis
Intravenous anesthesia:
Extremely rapid induction*It is common practice to use iv induction and inhalation agents for maintenance.
When volatile anesthesia is stopped it is eliminated quickly through the lungs.Propofol:
-Inductions within 30 sec
-Recovery is rapid
-Nausea and vomiting are extremely rare

(Propofol Emulsion)

(Propofol Emulsion)
Thiopental (Pentothal) :-Very short acting barbiturate
-Induces anesthesia smoothlyDose is 3-5 mg /kg
-Half life = 4 min allows swift recovery after a single dosage (Patient is awake after 10-15 min)
-Terminal half = life is 11 hours very prolonged recovery after repeated dosage or infusion

(Thiopental)
Metabolized in the liverPh = 11 Can damage tissue if exrtravasated
CNS:
-No analgesia-Decrease intracranial pressure
CVS:
-Hypotension-Tachycardia
-Decrease respiratory rate
Ketamine (Ketalar):
-Hallucinogen
-Trance like state
-Dissociative anesthesia
-Sedation amnesia dissociation
-Analgesia
15 min after a single IV injection
Can be given IM
Used for Minor surgical interventions
Tachycardia*Increased blood pressure
Cardiac output
Has an advantage in Shocked patients
Bronchodilatation.


(Ketamine)
Disadvantages of Ketamine:
-No muscle relaxation
*Increase intracranial and intra ocular pressure-Hallucination during recovery
***Decrease by diazepam
Usage:
Induction as a soul agent in minimal surgery1-2 mg/kg over 60 sec
5-10 mg/kg IM
Contra indication of Ketamine:
-Hypertension-Congestive cardiac failure
-Cerebral trauma
-Increased intracranial pressure
-Pregnancy (Contra indication in pregnancy)
Muscle relaxants in Anesthesia:
***Abdominal surgery requires muscle relaxation
(Deep general anesthesia can cause relaxation)
Neuromuscular blocking agents
*Deep general anesthesia is not advisedLight general anesthesia + selective neuromuscular block
Tracheal intubation + Quick recovery***Mechanical ventilation is always used
-Technical skill is required
***Neuromuscular block should only be given after induction of anesthesia
Curare was an arrow poisonComplete paralysis of all voluntary muscles
Movement is impossible
Mechanisms of muscle relaxants:
Acetylcholine is released after nerve impulse
Leads to activation of receptors on motor end plate
Natural substances that prevent release of ach at nerve ending:
Botulinum toxin
1- Competitive relaxants:
Atracurium, MivacuriumPancuronium, Vecuronium
-Competitive antagonists to ach.
-Flaccid paralysis
Reversal of anticholinesterases drugs is by
Neostigmine
Prevent destruction of ach
Pancuronium bromide =(trademarked as Pavulon)
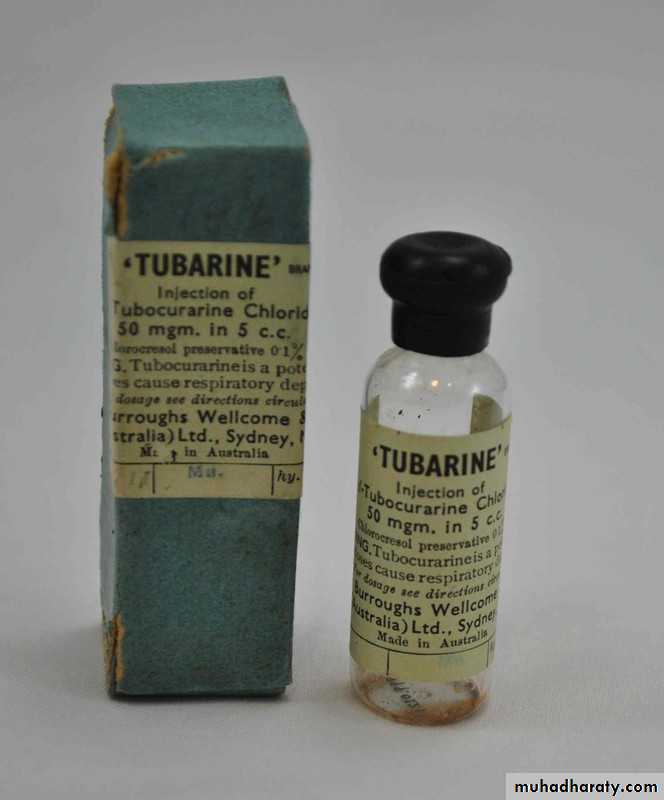
Tubocurarine:
*Can cause Hypotension
*Not used in many countries
Atracurium (Atracurium besylate):
-Altered in the body spontaneously in the body to inactive form-T ½ = 30 min
-By passive chemical process
(Hofmann elimination)
Duration of action = 15-30 min
Hepatic and renal disease
Vecuronium
Full blockade after 3 min
20-30 min duration

(Pancuronium/Pavulon )
2- By Depolarization:
Suxamethonium = Succinylcholine = Scoline
Contraction +relaxationShortest duration of action
Tracheal intubation in less than 60 secTotal paralysis for 4 minutes
If intubation is impossible recovery is rapid

(succinylcholine = scoline)
Suxamethonium (succinylcholine)=scoline
-Destroyed by pseudocholinesterase
-Hereditary deficiency-Scoline apnea
-Muscle fasciculation then paralysis
-Muscle pain 1-3 days
***Most rapid onset
Antagonism of Neuromuscular Blocking agents:
-Anti cholinesterase drugsNeostigmine IV + Glycopyrronium = (or Atropine)
Glycopyrronium bromide = Glycopyrrolate
Glycopyrronium bromide is a medication of the muscarinic anticholinergic group. It does not cross the blood–brain barrier and consequently has no to few central effects
*To prevent bradycardia due to parasympathetic action
-Act within 4 minutes-Effect lasts 30 min
-Neostigmine can itself cause paralysis in overdose = depolarization



Local Anesthesia
Local Anesthesia:Cocaine 1884 Carl Koller;
-Water soluble-Rapid onset
-Sterilizable by heat
Mode of action of local anesthesia:
Prevent the initiation and propagation of the action potential (nerve impulse)Reducing the passage of sodium through voltage gated sodium channel
They rise the threshold for excitability and block conduction
(Mechanism of action of local anesthesia)
The distribution of a single dose la is determined by diffusion into the tissue
Plasma half life is few mintsBy infiltration local anesthesia act within 5 min
And have a useful duration of effect for 1-1.5 horsCan be doubled by vasoconstriction
Local anesthesia is used as an acid salt = HCLDissociate in Basic Media
Liberating the active compound HCL
Free base
In abnormally acidic media (abscess)
This dissociation can be delayed***Also risk of spreading infection
Absorption of topical anesthesia on mucus membrane can be extremely rapid and give plasma concentration comparable to injection
*This is important specially in urethra
Chemical classification of local anesthetics:1-Esters:
Cocaine, Procaine, tetracaine, Benzocaine2-Amides:
Lignocaine (Xylocaine) LidocainePrilocaine, Pupivacaine

(Xylocaine = Lidocaine)
Effect is terminated by removing the local anesthetic from the circulation.Delaying this will increase the duration of action of la and decrease systemic absorption.
Most la cause dilatation with the exception of cocaine
Addition of epinephrine (Adrenaline) increase the duration of lidocaine
Never use adrenaline in
Extremities = fingertipsNose , toes, ..etc
Can lead to Gangrene!
Uses of local anesthesia:
1- Surface anesthesia: solution jelly cream2- Infiltration anesthesia
3- Regional anesthesia
-Nerve block
-Intravenous regional anesthesia-Epidural anesthesia
-Intrathecal ( Spinal anesthesia)
