Page1
Oral ulcer:
an area of discontinuity of epithelial surface.
Erosion
: a shallow defect with loss of epithelial layers down to (and
sometime invading) the basal layer.
When we examine ulcer we check for edge, base, shape, size, onset and duration
I. Primary
: starts as ulcer from the beginning
1. Traumatic ulcers:
A. Physical: hot, cold
B. Mechanical: check bite, orthodontic appliance, prosthesis,
sharp edge of broken tooth, retained root
C. Chemical: CMCP, phenol, H2O2, Sodium hypochlorite
D. Electrical burn
2. Infective ulcers:
A. Acute: ANUG and Cancrum oris (noma)
B. Chronic: TB , syphilis and histoplasmosis
II. Miscellaneous ulcers
(Aphthous ulcer, Behcet Syndrome, EM, IBD,
neoplastic ulcers, ulcers associated with blood dyscrasias)
III. Secondary
: starts as vesicle or bulla then rupture to form ulcer
Traumatic ulcer
(Physical, chemical, mechanical, electrical):
It is painful
with greyish to yellow base with red rim, healing takes place with 3-4 days
if the causative factor is removed
**Oral ulcer that doesn't heal spontaneously after the removal of the cause> Biopsy
Dx. Demonstration of the irritant, local factors, history
Treatment: Removal of the cause, diphenhydramine mouth wash,
lidocaine 4%gel, protection of the ulcer with Orabase
Dec 6, 13, 20, 27
د. ﻋﺒﺎس
10 Sheets / 500 I.D.
ﻃﺐ ﻓﻢ
-
ف
1
6,7,8,9
Oral Ulcer
part1, 2, 3 and 4
Page2
Acute infective ulcers (ANUG and Noma)
1. ANUG
Bacterial infection caused by Fusobacterium nucleatum, Bacillus fusiform
and Borrelia vincenti, Mostly affecting marginal and interdental gingiva
which is characterized by ulcerative lesions with necrosis in addition to the
presence of local and systemic factors
Local: poor oral hygiene, pericoronitis
Systemic: HIV, Infectious mononucleosis
This disease is characterized by rapid destruction with fever, malaise,
metallic taste, halitosis, gingival bleeding, crater lesions affecting marginal
and interdental gingiva and sometimes exposure of the underlying bone
Dx.: History, clinical features, microbiology
Treatment: Improve oral hygiene, ampicillin 250mg 1x3 1week, Flagyl
200mg 1x3
2. Noma
Acute progressive destructive condition occur in children who are severely
dehydrated or with malnourishment or systemic condition (leukemia,
Infectious mononucleosis, severe serious illness)
According to "Koch" postulate, inoculation of these microorganisms must produce
the disease in susceptible animals, however; on experimental animal the bacteria
do not cause this disease
ﺍﻟﻌﺎﻟﻢ
"
ﻭ،ﻪﻟ ﺐﺒﺴﻤﻟﺍ ﺏﻭﺮﻜﻴﻤﻟﺍ ﻊﻣ ﺽﺮﻤﻟﺍ ﻂﺑﺮﻟ ﺓﺪﻋﺎﻗ ﻊﺿ ﻭ"ﺥﻮﻛ
:ﻣﻤﺎ ﻗﺎﻟﻪ
ﺇﻥ
ﺍﻟﻤﻴﻜﺮﻭﺏ ﺍﻟﺬﻱ ﻳﺴﺒﺐ ﺍﻟﻤﺮﺽ ﻟﻺﻧﺴﺎﻥ ﻳﺠﺐ
ﺍﻥ ﻳﺴﺒﺐ ﻧﻔﺲ ﺍﻟﻤﺮﺽ ﻟﻠﺤﻴﻮﺍﻧﺎﺕ ﺍﻟﻤﻘﺎﺭﺑﺔ ﻟﻺﻧﺴﺎﻥ ﻓﻴﻤﺎ ﻟﻮ ﺗﻢ ﺣﻘﻨﻬﺎ ﺑﻨﻔﺲ ﺍﻟﻤﻴﻜﺮﻭﺏ
،
ﻭﻫﻮ ﻣﺎ ﻻ ﻧﺮﺍﻩ ﻓﻲ ﺣﺎﻟﺔ
ANUG
Page3
This lesion starts as ANUG then the lesion either go facially or lingually,
extension of this lesion may lead to fever, destruction and erosion of soft
tissue covering
Clinically may present as destructive lesion with blue to black color, local
and systemic features
Caused by: Fusobacteria nucleatum, Prevotella intermedia, Bacillus
fusiform, Borrelia vincentii and Streptococcus spp.
Dx. History, clinical, microbiology
Treatment: correction of systemic condition, hydration, plastic surgery
Chronic infective ulcers (TB, Syphilis and histoplasmosis)
1. TB
Usually the results of postprimary pulmonary sources , characterized by
chronic oral ulcer with deep undermining border affecting posterior part
of the tongue (due to sputum from cough), Also characterized by granular,
nodular, leukoplakic-like lesion
Primary oral lesion is rare
May also affect: lymph node (scrofula), Skin (lupus vulgaris), Bone (TB
osteomyelitis)
Dx.: History, clinically, sputum, x-ray, PCR, biopsy (shows caseous necrosis)
Treatment:
1
P
st
P
line: Isoniazid, rifampicin, pyrazinamide (for 2 months)
2
P
nd
P
line: Isoniazid, rifampicin (for 4 months)
Isoniazid (INH) causes vit. B6 deficiency, Rifampicin causes orange
secretion
Ethambutol and Streptomycin may be used in resistant cases
Page4
2. Syphilis (Acquired and congenital)
A. Acquired: affecting young adults and has many clinical varieties
according to types of lesions and course of the disease
Primary
1. Chancre: painless ulcer affecting genital area + tip of tongue and
lower lip (highly infectious), self-limiting and disappear after few
week, start as papule and enlarge to form patch then ulcerate, 5mm
to several cm
2. Lymph nodes: firm large non tender
Dx.: dark field examination (U.V. light + silver stain)
Secondary
Mucous patch after 3~6 months, systemic manifestation, fever,
generalized lymph adenopathy+ maculopapular eruption
Oral mucous patch yellowish with superficial erosion, posterior
aspect of oral cavity and tonsillar region (snail track)
Dx.: Serum tests: non-specific (VDRL, Wassermann), specific
(fluorescent treponemal antibody absorption test FTA-ABS)
Tertiary (non- infectious lesions)
1. Gumma affecting any part (specially palate and tongue), In palate
start as swelling followed by necrosis and ulcer> perforation
2. Red atrophic lesion (glossitis) due to endarteritis
3. Syphilitic leukoplakia (premalignant)
Syphilis may also affect spinal cord (tabes dorsalis), Aorta (aneurysm)
D.D. of palatal perforation:
TB, Gumma, trauma, cleft, surgical, Wigner, ca of sinus
Page5
Treatment:
If infection occurred in less than 1 year: benzathine 2.4 megaunit
Allergic>Tetracycline 500 1x4 50 days
Can't take oral tetra>erythromycin 500 1x4 50 days
If more than 1 year > increase treatment one month
B. Congenital syphilis (not contagious)
Hutchinson triad:
1. CNVIII deafness
2. Keratoconjunctivitis
3. Hutchinson incisor (peg or screw driver incisors and mulberry molars)
Others: saddle nose , high palate, atrophic glossitis
3. Histoplasmosis (Most common sys. fungal infection by H. capsulatum)
Infection from inhalation of contaminated dust from infected bird and bat
Primary is mild and self-limiting pulmonary disease that heals with fibrosis
and calcification similar to TB , sometimes may progress> cavitation in lung
and dissemination to liver, spleen, meningis, bone marrow (anemia and
leukopenia) , Immune compromised patient develop disseminated form
Oral lesion secondarily to pulmonary: Papular, nodular, or ulcerative, or
vegetation (fungus like), lymph nodes are enlarged and firm
Dx. Culture of exudate on Sabouraud agar, biopsy
(shows caseous necrosis)
Treatment: ketoconazole, itraconazole 6~12 months
Immune compromised> amphotericin-B 10 weeks
(monitor renal and
hepatic function)
Previous:
Red and white lesion
part 3
Nov 8
Current:
Oral Ulcer
part 1
Dec 6
Next:
Oral Ulcer
part 2
Dec 13
Later:
Oral Ulcer
part 3
Dec 20
Page6
II. Miscellaneous oral ulcers:
(Aphthous, Behcet, EM, IBD,
neoplastic ulcers, ulcers associated with blood dyscrasias)
1.
Recurrent aphthous ulcer
:
most common disease affecting the oral
cavity after caries and periodontal disease. Occur in 15-20% of general
population. It is defined as a disorder characterized by recurrent painful
necrotizing ulceration of different sizes involving buccal mucosa, floor of
the mouth, ventral surface of the tongue, palate and tonsillar region
with pseudomembrane (grey-yellow) covering it, around which there is
a circular inflammatory hallow (margin), shape of the lesion is round
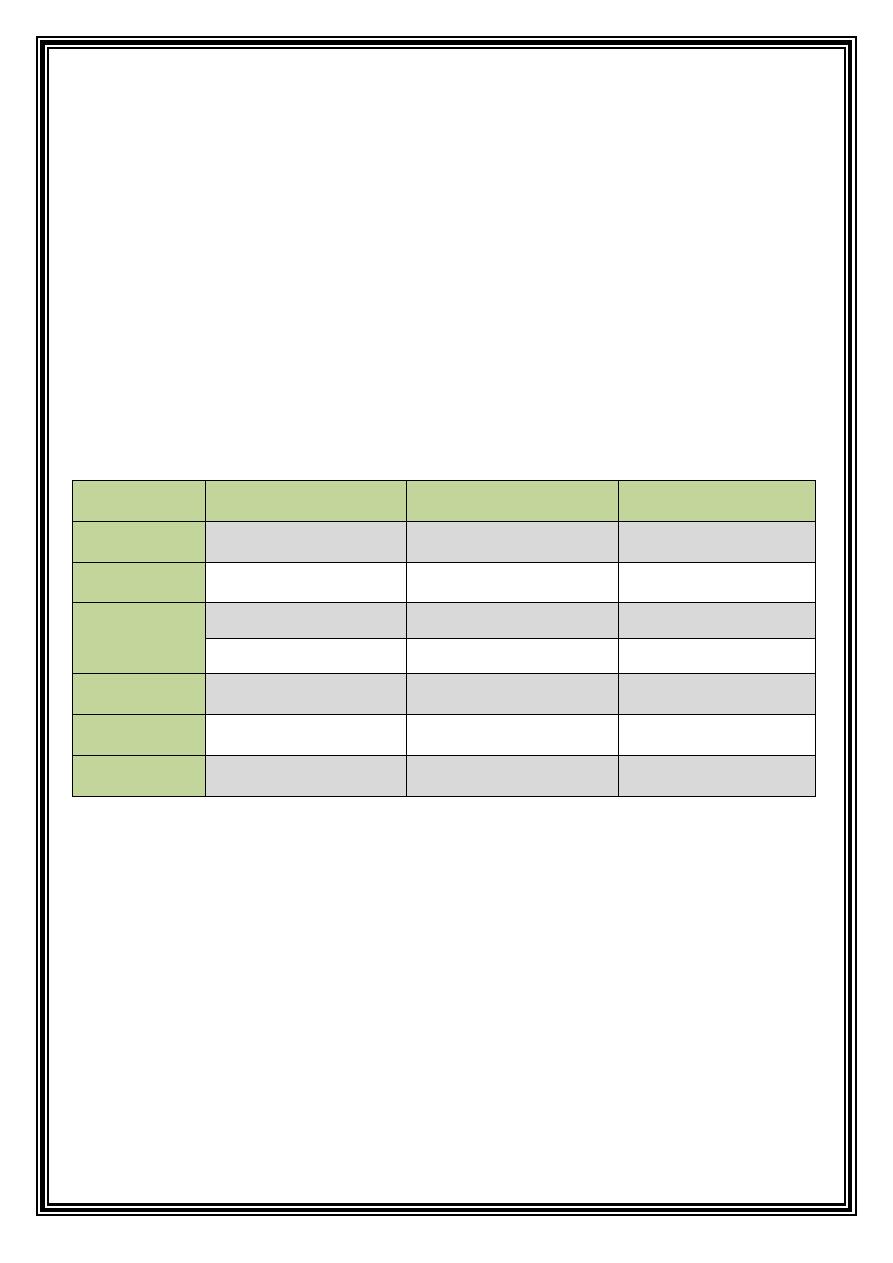
oval. It has 3 clinical varieties:
Minor AU
0B
Major AU*
Herpetiform AU
2B
Site
Non keratinized epi
1B
Mainly keratinized epi
Anywhere
Diameter
5-10 mm
>1 cm
1-4 mm
Healing
1ry intention
2ry intention
1ry intention
7-14 days
Weeks-months
7-10 days
Prevalence
80% of cases
10-15% of cases
10% of cases
Number
1-5 ulcers
1-3 ulcers
Up to 100 (groups)
Severity
Painful
Very painful
painful
* Major AU = (Sutton’s disease) = (Periadenitis Mucosa Necrotica Recurrence)
Cause of RAU is unknown but it was thought to be due to:
1. Primary immune dysregulation: Dysfunction of cytotoxic stimulating
effect of T-helper (CD4 and CD8) as in AIDS
2. Decrease mucosal barrier: this is why smokers don’t develop RAU
(smoking causes keratinization> increased mucosal barrier)
3. Antigen exposure: like viral or bacterial infections
Page7
Predisposing factors for RAU
1. Trauma: after L.A., Sharp food or teeth brushing
2. Stress and anxiety: specially before oral medicine exams
3. Systemic diseases and conditions:
a. Behcet syndrome
b. Cyclic neutropenia
c. Relative IgA deficiency
d. Drugs: NSAID and methotrexate
e. Immunocompromised patients: as in AIDS
f. FAPA: periodic Fever, Aphthous, Pharyngitis, Adenitis
g. MAGIC: (mouth and genital ulcer with inflamed cartilage)
h. Inflammatory bowel disease (Crohn’s, ulcerative colitis, celiac)
4. Immunological reaction: immune complex type of reaction
5. Infections: Streptococcus sanguis and Lactobacillus fermentum
6. Genetic predisposition:
expression of certain antigens: HLA-B12, CW7
7. Hematological causes
8. Allergy to food and medications (exclude allergy before diagnosis
by patch test)
Diagnosis of RAU
1. Good history and clinical examination
2. hematological investigations to exclude systemic conditions
3. Biopsy is nonspecific (shows necrosis)
Page8
Treatment:
it aims to prevent secondary infection, accelerate healing
and remove etiological factor if possible
1.
Xylocaine
gel or solution 2%
2.
Diphenhydramine
mouth wash 12.5mg/5ml
3.
Chlorhexidine
(antiseptic to prevent infection) mouth wash 0.2% , instruct
the patient not to wash his mouth for half an hour
4.
Tetracycline
capsule dissolved in 15 ml water but leads to fungal infection
and discoloration by time
5.
Kenalog in Orabase:
1x4 Kenalog= Triamcinolone acetonide 0.025%,
Orabase=Carmelose + pectin + gelatin (keeps drug contacted to tissue)
6.
Potent topical fluocinonide
(Lidex®) 0.05% paste
7.
Ultra potent corticosteroids
: Clobetasol (Temovate®) 0.05%
8.
Intralesional
: triacetonide diacetate
9.
Prednisolone
: start with 60 mg 1x2 , then taper to 40, 30, 20, 10 then stop
10.
Amlexanox
(Aphthasol®) 0.5% in Orabase, mouth rinse (antiallergic)
11.
Levamisole
(Ketrax®) 50mg for cases responding to it
Resistant cases
1.
Colchicine
0.6 tab 1x2
2.
Pentoxifylline
400mg once daily
3.
Dapsone
50-100 mg (causes bone marrow suppression)
4.
Thalidomide
100-200mg : teratogenic, women must take contraceptive
pills 4 weeks before and after taking this drug
Page9
2. Behcet syndrome (old silk road disease):
chronic relapsing disease
characterized by recurrent oral ulcers, genital ulcers, skin manifestation, ocular lesion
in addition to the affection of other organs in the body such as CVS, brain and lungs,
characterized by vasculitis of small and medium size arteries and veins.
Clinical varieties:
Mucocutaneous, arthritic, ocular and neurologic
• Oral lesion: usually similar to minor and major aphthous ulcers, it may be small or
giant, round or oval, with yellow base and red rim, present in 90% of cases
anywhere within the oral cavity. Oral involvement is common in all varieties
• Genital lesions: mainly affecting vulva in female, testes in male or anal region
• Skin lesion: is characterized by “Acneform skin rash”, pustular rash, erythema
nodosum (red tender lump affecting the legs, ankles and sometimes trunk, neck
and faces, may be associated with folliculitis)
• Ocular lesion: anterior uveitis (blurred vision, tearing, redness) and posterior
uveitis (retinal involvement and blindness)
• CNS involvement: leads to “aseptic meningitis” or “sterile meningitis”
Diagnosis of Behcet syndrome:
•
U
Major criteria
U
: Recurrent oro-genital ulcers, Skin lesions ,Ocular lesion,
Pathergy -pin prick- test (intracutaneous injection or needle stick, after
24-48 hours, a sterile nodule will be formed)
•
U
Minor criteria
U
: CNS involvement, family history, lab investigation
(leukocytosis, eosinophilia, increased ESR)
Treatment
• Topical corticosteroids are the drugs of choice
• Systemic steroids (injection or tab) :prednisolone 60-80 mg
• Colchicine 0.5-2 mg , Dapsone 25mg
• Cytotoxic drugs: for skin involvement Azathioprine (Imuran) 100 mg
Previous:
Oral Ulcer
part 1
Dec 6
Current:
Oral Ulcer
part 2
Dec 13
Next:
Oral Ulcer
part 3
Dec 20
Later:
Oral Ulcer
part 4
Dec 27
Page10
II. Miscellaneous oral ulcers: cont’d
3. Erythema multiforme
:
Acute inflammatory self-limiting disease
characterized by acute recurrent multiple oral ulceration or erosions.
The mild form of E.M. is self-limiting and confined to the oral and skin lesion,
whereas the major variant represents either
Steven Jonson syndrome
or
Toxic
Epidermal NecrolySis (TENS)
Clinical features:
characterized by prodromal symptoms of fever, malaise, sore
mouth in addition to oral and skin lesion
Oral lesions:
may affect buccal mucosa, floor of the mouth which is
characterized by vesicular eruption and fused erosion and ulcerations on
erythematous base which on the lip become crusted with blood.
DD of bloody crusted lip:
Trauma, SJS, HSV
Skin lesion
called
target, iris or bulls eye
lesion which is characterized by
concentric erythematous patches containing peripheral zones of pallor and
surrounded by erythematous inflammatory ring up to few cm
Etiology
: cause of E.M is immunologically mediated condition characterized by
immune complex or cell mediated hypersensitivity reaction
Predisposing factors may include:
1. Infection by herpes simples virus , histoplasmosis, Mycoplasma
2. Drugs such as sulfa group , barbiturate, digoxin, -oxicam gp., iodine
3. Recent vaccination or chemotherapy, progesterone intake , IBD
4. Psychological stress and emotions
Dx
.
1. History
2. Clinical examination (mainly diagnostic with pathognomonic skin lesion, iris)
3. Serological test to show anti body against herpes in case of viral infection
Rx.
1. Alermine “Diphenhydramine” mouth wash to decrease pain
2. Topical corticosteroid
3. In severe cases, treated by short course of systemic corticosteroids
Page11
4. Recently, E.M is treated by Dapsone and thalidomide
**The severe or major form of E.M is called
Steven Jonson syndrome
which is
characterized by oral and skin manifestation also involving genital and ocular area.
Whereas
TENS
is a life threatening condition characterized by severe degradation
of skin and oral mucosa -like third degree burn- so those patients treated in burns
department of hospital
Both SJS and TENS mainly associated with hypersensitivity and infection
4. Inflammatory bowel disease:
General classifications of inflammation
affecting large or small intestine, these are ulcerative colitis and Crohn’s disease
Both diseases ate of interest to the
dentist because
of associated oral finding and
dental management of the medical problem which treated by corticosteroid
A. Ulcerative colitis:
it involves mucosa and submucosa of colon , characterized by oral
lesion similar to minor and major varieties of aphthous ulcer, general symptoms such as
lower abdominal pain (cramp) and frequent bloody diarrhea due to sloughing of mucosa of
the colon
Dx
.
1. Careful history and clinical examination
2. GIT radiograph (Barium enema)
3. Endoscopy: This involves direct visualization of intestinal mucosa
4. Most important is “sigmoidoscope” show multiple mucosal ulcer covered by blood
Rx.
1. Drug of choice is
Sulfasalazine
“anti-inflammatory” containing 5-aminosalycilic acid
2. Corticosteroid and ACTH
3. Third line of Rx.is immune suppressive (azathioprine, cyclosporin, mercaptopurine)
4. Surgical treatment 15-20% of patients respond to surgical treatment as colectomy
Page12
B. Crohn’s disease
“regional enteritis”: inflammatory condition involving all layers
of gut, has 2 types (perforating and non-perforating). Cause is unknown.
Oral manifestations are:
1. Recurrent aphthous ulcers
2. Diffuse swelling of the lip and face
3. Inflammatory hyperplasia of the oral mucosa with cobble stone pattern
4. Indurated polypoid tag like lesion in vestibule and retromolar pad area
5. Diffused gingivitis
6. Angular cheilitis and glossitis
7. All oral manifestation of anemia (depapillation of the tongue, burning mouth
sensation, pallor of oral mucosa)
8. Persistent deep linear ulceration with hyperplastic margins
9. Localized mucocele formation (mucocele forms because Crohn’s disease is non
caseating disease leads to formation of granulation tissue which lead to
destruction of the duct of salivary gland)
Rx.
1. Palliative treatment with mouth washes Alermine
2. Topical corticosteroid
3. Dexon serum as mouth washes (if used more than 2weeks leads to systemic
absorption)
5. Neoplastic malignant ulcer
Chronic ulcer with raised rolled everted edges with pseudomembrane “yellow to
grey” , mainly affecting the lower lip lateral border of the tongue, floor of the mouth
(the ulcer may be exophytic) more common in male, middle age, the ulcer is painless
then become painful
Dx.
1. History and clinical features : raised rolled ulcer with everted edges, hard and
indurated, fixed “fixation and induration is due to invasion of underlying
connective tissue”
2. Biopsy (Toluidine blue used before biopsy to show the border of the lesion)
Page13
6. Oral ulceration associated with blood dyscrasia
A. Cyclic neutropenia
:
rare disorder occur secondary to periodic failure of stem
cell in the bone marrow. It is characterized by transient severe neutropenia that
occur approximately every 21 day, the low neutrophil count lasts 3-7 days then
returns to normal
Clinical manifestation:
major sign and symptoms are related to infection
occurring due to neutropenic episode, which is characterized by fever,
stomatitis, laryngitis, skin abscess, upper respiratory tract infection
(pharyngitis)
Oral manifestation
: oral ulcer large deep scarring ulcer similar to major
aphthous and periodontal manifestation ranging from marginal gingiva to
periodontitis, with severe bone loss
Rx
.: by corticosteroid, ACTH , G-CSF (granulocyte colony stimulating factor)
B. Uremic stomatitis
due to retention of urea
Oral manifestation
1. Gingivitis
2. Stomatitis
3. Xerostomia
4. Periodontitis
5. Ammonia like taste and smell
6. Red oral mucosa with ulceration (In skin residual urea crystals deposit in
subepithelial area after vaporization forming Uremic frost)
Previous:
Oral Ulcer
part 2
Dec 13
Current:
Oral Ulcer
part 3
Dec 20
Next:
Oral Ulcer
part 4
Dec 27
Later:
here goes the coffee job, HAPPY MID YEAR EXAMS!
Page14
III. Secondary oral ulcers:
Vesiculobullous lesions affect the mouth and tend to break down rapidly and present
as ulcerative, vesicular and bullous lesion (UVB)
UVB lesions are classified as infective, miscellaneous and autoimmune
1. Infective UVB lesions
:
including infections of herpes and Coxsackie virus
A. herpes virus:
DNA virus, 80 types, most common are:
1. HSV1
:
causes primary and secondary herpetic lesions (above the waist)
a. Primary lesion: herpetic gingivostomatitis, in fingers called herpetic whitlow
b. Recurrent : herpes labialis or cold sore
Recent studied found an association with Bell’s palsy and erythema multiforme
2. HSV2
: genital virus affecting areas below the waist, it is considered as oncogenic
virus due to association with cervical carcinoma
Both HSV1 and HSV2 cause oral lesions because this virus affects tissue of
ectodermal origin (mucous membrane, skin, eye, CNS)
3. VZV:
Primary: chicken pox, Recurrent : shingles or herpes zoster
4. CMV:
causes oral ulcer and salivary gland disease in AIDS patients
5. EBV:
causes infectious mononucleosis, hairy leukoplakia, nasopharyngeal
carcinoma and Burkitt’s lymphoma (African lymphoma)
6. HH6:
associated with multiple sclerosis
7. HH7:
isolated from saliva, not associated with specific disease
8. HH8:
associated with Kaposi sarcoma specially in AIDS patients
All types can remain latent in the host neural cell as latent virus, when the body
resistance decrease due to any reason the virus is reactivated and infection recurs.
Latency
: character of all herpes viruses, the virus transport from mucosa or
cutaneous nerve ending by the nerve to the ganglia, herpes gene remain in non-
replicating state which is then reactivated upon suppress in immunity
Page15
Primary herpetic gingivostomatitis:
Common viral infection caused by HSV1, affecting children and rarely adults. It does
not occur before age of 6months due to circulating maternal antibodies.
The disease start by: fever, malaise, lymphadenopathy, headache and sore throat,
prodromal period of tingling, burning sensation and erythema
After 2-10 days, vesicular eruption appears, starting as small vesicle that fuse
together and rupture to form ulcers (yellowish with red margins) crusted with blood,
heal within 7-10 days, acne may be seen after 2-3 days which develop as papule
changing to vesicle, at the same time the gingiva is bright red in color and edematous
Dx.
1. History and clinical features
2. Cytology: fresh vesicle is opened and scraped, stained by Giemsa stain to see
multinucleated giant cells (ballooning degeneration)
3. Isolation of the virus from saliva and special culture
4. Detection of antibody titter (serology), electron microscope, PCR and ELISA
Rx. ----------------------> Steroids are contraindicated
1. Supportive treatment, hydration of the patient, analgesics , antipyretics
2. Antibiotic to prevent secondary infection
3. Acyclovir: Zovirax® 200 mg 1x5 , For child dose=age/20*dose
4. Topical acyclovir cream 5%
5. Other antiviral drugs: valacyclovir or famciclovir 500 mg 1x1 or 1x2
6. Xylocaine gel, Alermine mouth wash, ice cream (contains milk and sugar)
7. Vaccination against HSV
Page16
Recurrent herpes infection
Attenuated version of post primary herpetic infection with no systemic involvement
(no fever, no lymphadenopathy.
Usually affects circumoral area, if occur on lip called herpes labialis, if occur
intraorally it will affect the immobile mucosa (hard palate and gingiva)
Dx
. History and clinical features
Rx
. prevention of predisposing factors, acyclovir 500 mg 1x2, Penciclovir cream
1%, Famciclovir 500mg tab 1x3
When treating patient with active herpetic lesion, beware of:
1. An injury to the hand of dentist or dental staff leads to Herpetic whitlow
2. Ocular herpetic lesion may occur due to infected salivary droplets coming
in contact with cornea, leading to ulceration of the cornea.
Both can be prevented by wearing eye glasses, gloves, and face mask
** Herpes simplex infection in immunocompromised patient is characterized by oral
ulcers resistant to drugs
VZV
: causes primary and recurrent infection
Chicken pox:
generalized primary infection with VZV occur when the patient contact
with the virus causing generalized maculopapular eruption with pruritic vesicles that
readily rupture
Herpes zoster “shingles”
: has prodromal phase 2-4 days, when shooting pain,
parasthesia. Burning and tenderness along the distribution of the affected nerve,
unilateral vesicle son erythematous base which then appear in clusters, the vesicles
then rupture and haling occur within 2-4 weeks with some scarring. The most
commonly affected nerves in addition to trigeminal nerve are C3, T5, L1, and L2
Complications:
1. Post herpetic neuralgia:
pain remains after a month after the mucocutaneous
lesion have healed, occur due to inflammation and fibrosis. It can be prevented
by: anti-inflammatory, corticosteroids, antiviral “acyclovir”
2. Ramsay hunt syndrome:
rare form of the disease affecting motor and sensory
nerves, characterized by Bell’s palsy, unilateral vesicles on external ear and
vesicles on the oral mucosa.
Page17
3. Herpes zoster ophthalmicus:
serious complication if the disease involves
ophthalmic branch of trigeminal nerve, it needs high dose of acyclovir to
prevent blindness : 800mg 1x5
Dx
. of complications History, clinical feature, cytology and isolation of the virus
Rx
. supportive treatment and antiviral drugs
B. Coxsackie virus:
3types associated with oral lesion (all of type A)
1. Herpangina
: caused by cox A4 virus, mainly affecting the children. The
infection is confined to the posterior aspect of the pharynx, tonsillar region,
and soft palate. It is characterized by transient vesicular eruptions which lead
to ulceration after rupturing. Patients complaint of sore throat, dysphagia, sore
mouth, the lesion is mild , Rx. supportive
2. Acute lymphonodular pharyngitis
: variant of herpangina, caused by cox A10
virus, distribute on the posterior aspect of the oral cavity, appears as white-
yellowish nodule which not progress to vesicle or ulcer, Rx. supportive
3. Hand foot and mouth disease:
caused by cox A16 virus, characterized by low
grade fever, oral and vesicle ulceration, non-pruritic maculopapular eruption
on the flexure surface of hand (palms) and feet (soles), may also affect hard
palate, tongue and oral mucosa. Rx. supportive (paracetamol and hydration)
2. Miscellaneous UVB:
Bullous and erosive lichen planus and epidermolysis bullosa (EB)
Epidermolysis bullosa:
group of mechanobullous diseases characterized by
lesion after trauma, it has many types: EB junctions, EB equiseta, EB dystrophic
EB dystrophic has two types: dominant and recessive (premalignant with oral
lesions and enamel hypoplasia) , leads to destruction of affected hands and feet.
Rx
. Steroids
Page18
3. Autoimmune UVB lesions:
A. pemphigus:
defined as life threatening disease causing blister and erosion of the
skin and mucous membrane. Autoantibodies attacks epithelial desmosomal
glycoprotein, which cause loss of cell to cell adhesion, resulting in acantholysis with
the formation of intraepithelial bulla or vesicles. Mostly affects 5-6
P
th
P
decade of life in
Mediterranean and Ashkenazy Jewish population due to association with MHC
complex HLADR or HLADQW3. Familial pemphigus also reported.
Types: vulgaris, vegetans, foliaceous, erythematous, paraneoplastic, drug associated
1. Pemphigus vulgaris
: most common, 80% of cases due to binding of IgG antibody
to desmoglein 3,
Clinical manifestation are:
a. Classical lesion is thin walled bullous aries on normal skin or mucosa, the bulla
rapidly rupture leading to large area denuded of skin
b. Characteristic signs:
i. Application of pressure on intact bulla will lead to enlargement of the bulla
due to extension to adjacent apparently normal tissue
ii. Pressure on apparently normal area leads to formation of new bulla, this is
called Nikolsky sign (also positive for epidermolysis bullosa)
c. Oral manifestation: 80-90% of patients with pemphigus vulgaris have oral
lesion during course of disease, in 60% oral lesion is first sign. The lesion most
commonly starts on buccal mucosa, area of trauma along occlusal line, palate
and gingiva (called desquamative gingivitis)
DD of desquamative gingivitis: Pemphigus vulgaris, Bullous pemphigus, Mucous
membrane pemphigoid, Erosive lichen planus
Pemphigus vulgaris is fatal due to:
1. High dose of corticosteroids
2. Electrolytes imbalance (dehydration)
3. Secondary infection, bacteriemia and septicemia
Dx.
1. History and clinical examination
2. +ve Nikolsky sign
3. Two biopsies : for H&E stain + fresh frozen for immunofluorescent technique
4. ELISA: to detect antibodies to desmoglein 3
Page19
Rx.
1. Corticosteroid (systemic) 2mg/kg
2. Chemotherapy Azathioprine (Imuran®) 50mg 2-4/day
3. Tetracycline, dapsone 50-60mg, parenteral gold
4. Plasmapheresis: wash out antibodies from the plasma (also for drug toxication)
5. 8- Methoxypsoralien followed by exposure of peripheral blood to UV light
2. Pemphigus paraneoplastic
: severe form associated with underlying malignancy
(non-Hodgkin’s lymphoma, leukemia) causing severe blisters and erosion,
treatment is difficult, patients die from underlying tumor or respiratory failure
due to acantholysis of respiratory epithelium.
3. Drug related pemphigus
: rifampicin, captopril, diclofenac sodium, garlic
Rx
. withdrawal of the drug, steroid
B. Pemphigoid:
(includes bullous pemphigoid and
mucous membrane pemphigoid)
1. Bullous pemphigoid:
the most common subepithelial blistering disease, age ≥ 60
2. Mucous membrane pemphigoid:
(cicatricial pemphigoid): chronic autoimmune
disease, affects the mucous membrane of patients over 60 years old leading to
mucosal ulceration and subsequent scarring -cicatricial means scar forming-. The
primary mucous membrane pemphigoid occur when autoantibody is directed
against protein (laminin) in the basement membrane zone, acting with
complement and neutrophil causing sub epithelial split and subsequent bullous
formation
Clinical manifestation:
affects any mucosal surface, first is oral mucosa, second
most common site is conjunctiva (leading to symblepharon, or blindness due to
corneal damage). Also affects genital mucosa, larynx, pharynx and esophagus, skin
lesion 20-30% of disease, oral lesion 90% of cases with desquamative gingivitis
Dx.
1. History and clinical feature, -ve Nikolsky sign
2. Biopsy (direct immunofluorescent technique)
3. Treatment: topical corticosteroids, dapsone recently is used
Rx
. topical or intralesional corticosteroid, dapsone is found to be effective
Previous:
Oral Ulcer
part 3
Dec 20
Current:
Oral Ulcer
part 4
Dec 27