


Pediatric infectious diseases
Hasanein Ghali, MDDepartment of Pediatrics
College of Medicine – University of Baghdad
December, 22nd, 2015
December 22, 2015
1
Measles
December 22, 20152
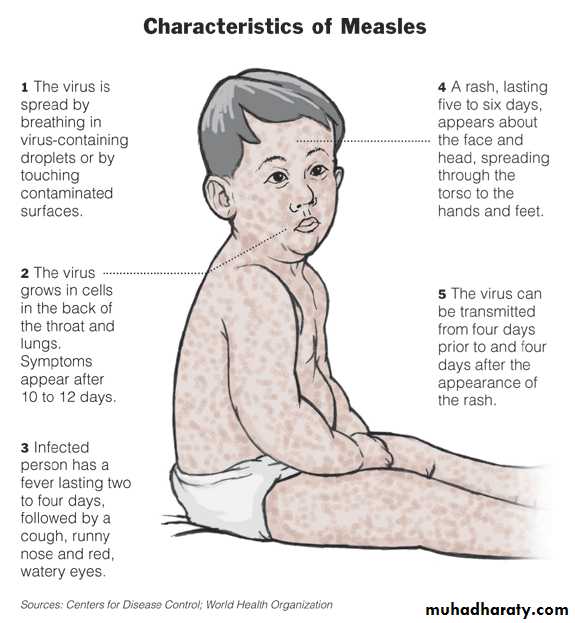
• Highly contagious, was once an inevitable experience during childhood.
• Due to wide spread vaccination, endemic transmission has been interrupted• Single stranded, Lipid enveloped RNA virus
• Family paramyxoviridae, Genus morbillivirus.
December 22, 2015
3Introduction
December 22, 2015
4
• Mode of transmission: Respiratory droplets, 2 days before symptoms to 4 days after rash.
• Immunocompromised patients may shed virus for longer period and should be isolated for the duration of their disease.
• Approximately 90% of exposed susceptible individuals experience measles.
• Face-to-face contact is not necessary.
Transmission
December 22, 2015
5• Incubation period: 8 -12 days.
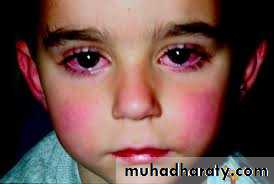
• Fever and malaise.
• Coryza, Conjunctivitis (photophobia) and Cough follow within 24 hours.
• Kopliks spot: (50%-70%) Appears 1 – 4 days prior to rash on the buccal mucosa adjacent to the molars within 48 hours and increase in no. during 3-4 days.
• They are 1 -3 mm, Red spots with blue-white centers.
Clinical course
Clinical courseThey are infrequently identified, but pathognomonic for measles, emphasizing the need for careful inspection of the oropharynx in any child with fever.
They disappear on the second day of the measles rash.
December 22, 2015
6
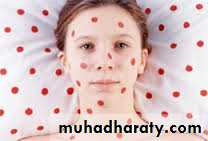
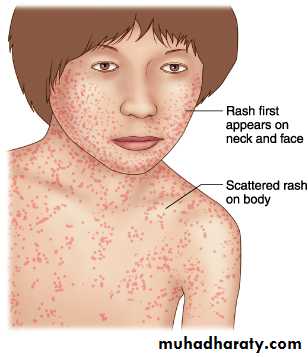
• Rash: In the 4th day of illness, Red to purple papules appears on the forehead, gradually spread downward reaching the feet by the 3rd day. Coalescence of lesions is common on the face and upper body.
• After it reaches its peak, it begins fading from the top downward as it had appeared within 1 week or less.
• Of the major symptoms of measles, the cough lasts the longest, often up to 10 days.
December 22, 2015
7
Clinical course
Other forms
Mild form is seen in infants having maternal antibodies, children recently received gamma globulins and individuals immunized previously and posses some levels of antibodies insufficient to prevent infection but adequate to modify its course.An atypical measles syndrome: High fever, pulmonary infiltrates and no or unusual rash has been reported in immunocompromised individual.
December 22, 2015
8Complications
Otitis media, pneumonia (primary or secondary), persistent bronchitis, and diarrhea especially among poorly nourished children. Encephalitis is rare with poor prognosis.A delayed degenerative disorder, (SSPE) Sub acute Sclerosing PanEncephalitis: Personality changes, seizures, coma, and death, may occur in about 9 -11 years following measles.
December 22, 2015
9Diagnosis
Clinical and epidemiological findings.
Virus isolation from specimens obtained in the first few days.
Other findings in the acute phase include reduction in the total WBC, with lymphocytes decrease more than neutrophils.
December 22, 2015
10
• No specific antiviral therapy, only supportive.
• Vitamin A administered to all children diagnosed with measles in communities where the vitamin A deficiency is a recognized problem.• Vitamin A deficiency in children is associated with increased mortality from a variety of infectious diseases, including measles.
December 22, 2015
11
Management
• Control of outbreaks: administration to vaccine within 72 hours of exposure.
• Infants younger than 12 months of age and those who are immunocompromised or pregnant should receive appropriate dose of immune globulin.December 22, 2015
12
• Management
• In Iraq, the immunization schedule includes giving measles vaccine at the age of 9 months, followed by MMR at the age of 15 months.
December 22, 2015
13
• Measles vaccine
December 22, 2015
14
December 22, 2015
15

December 22, 2015
16
December 22, 2015
17

December 22, 2015
18
December 22, 2015
19
December 22, 2015
20

December 22, 2015
21
December 22, 2015
22
December 22, 2015
23

December 22, 2015
24
December 22, 2015
25

December 22, 2015
26Rubella
December 22, 201527
Introduction
German measles or 3-day measles.Mild disease of children but more severe in adults.
Major significance is the transplacental infection and fetal damage (congenital rubella syndrome).
Single stranded RNA virus with a lipid envelope.
Family Togaviridae, genus Rubivirus.
Infectivity: 10 d after infection – 14 d after rash
December 22, 2015
28
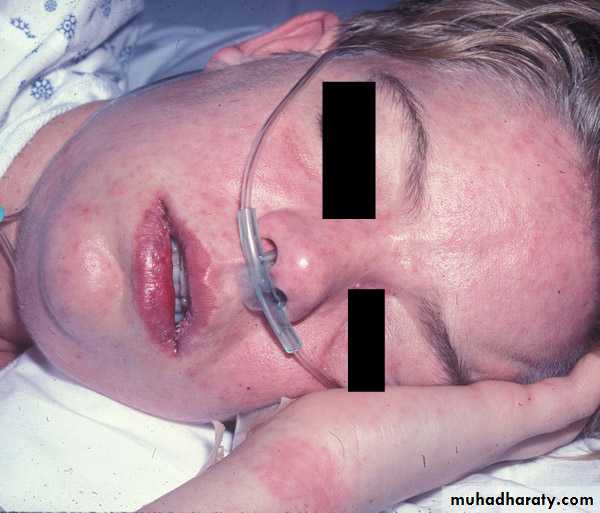
Clinical course
• The incubation period: 14 -21 days.
• Mild illness, clinical features are neither distinctive nor diagnostic.
• Many infections are subclinical.
• One – five days prodrome of low grade fever,
• In children, the prodrome may be absent or unnoticed.
December 22, 2015
29
Clinical course
• Forchheimer spots, pinpoint red macules on the soft palate early in illness, are helpful but not pathognomonic.• The characteristic occipital and post auricular LAP is highly variable and not specific for rubella.
• The exanthem which last about three days appears on the face first as numerous discrete rose pink maculopapules which rapidly spread downward to involve the trunk and extremities.
December 22, 2015
30
Clinical course
• Second day, the facial eruption fades while the lesions of the trunk coalesce. The rash disappears usually on the third day without scaling or peeling.• In adolescent and young adults, occipital tenderness when combing the hair, bleeding gums after brushing he teeth, transient polyarthralgia and arthritis.
December 22, 2015
31
Complications
1- Encephalitis, more in children.
2- Thrombocytopenia .
3- Arthritis or arthralgia involving the knees, ankle or hands, especially young women, remains the most serious complication of rubella in non pregnant women. Joint manifestation, if occur in children, are usually benign and transient.
December 22, 2015
32
Complications
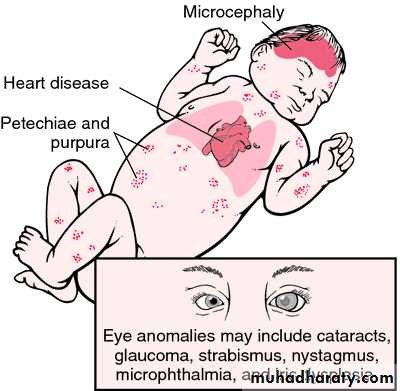
4- Congenital rubella syndrome (1941): Due to Maternal infection in the first 8 wks. This syndrome is characterized by Nerve deafness (the single most common finding), IUGR, Retinal findings (salt and pepper retinopathy), Cardiac abnormalities (patent ductus arteriosus and valvular diseases), Interstitial pneumonitis, Meningoencephalitis and Interstitial nephritis.December 22, 2015
33
• Clinical and epidemiological.
• Antibody titers.• Leukopenia and thrombocytopenia
December 22, 2015
34
Diagnosis
• No care beyond antipyretics and analgesics.
• The treatment is mainly supportive.• Patients should be isolated from susceptible individuals for 7 days after the onset of rash.
• Management of CRS is more complex and requires pediatric, cardiac, audiologic, ophthalmologic, and neurologic evaluation and follow up.
December 22, 2015
35
Treatment
• In Iraq, the immunization scheduled includes giving rubella vaccine at the age of 15 months and for females, at the child bearing age.
• Exposure to pregnant women is of concern.
December 22, 2015
36
Prevention
December 22, 2015
37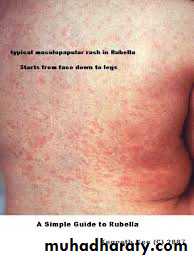
December 22, 2015
38
December 22, 2015
39

December 22, 2015
40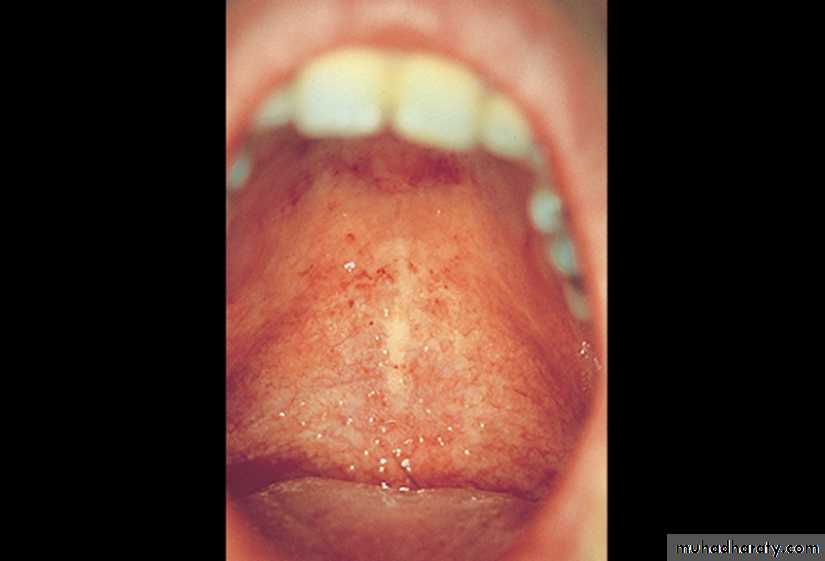

December 22, 2015
41

December 22, 2015
42
December 22, 2015
43
December 22, 2015
44
Mumps
December 22, 201545
Introduction
An acute self-limited infection.Family paramyxoviridae, genus rubulavirus.
It is a single stranded pleomorphic RNA virus.
Endemic in developing world, warranting continued vaccine protection.
Transmission: Respiratory droplets
Virus appears in the saliva from up to 7 days before to as long as 7 days after the onset of swelling.
Incubation period: 12-25 days.
December 22, 2015
46December 22, 2015
47Target organs
1- Salivary glands, CNS, pancreas and testes.
2- Thyroid, ovaries, heart, kidneys, liver and joint.
Clinical course
• The presentation ranges from asymptomatic or nonspecific to the typical illness associated with Parotitis with or without complications.• A prodrome of fever, headache, vomiting and achiness lasts for 1–2 days.
• Parotitis then appears, unilateral initially but become bilateral in 70% of cases.
• Ingestion of acidic food enhance pain in the parotid area.
December 22, 2015
48Clinical course
• The angle of the jaw is obscured and the ear lobe may be lifted upward and outward.• The opening of the stensen duct may be red and edematous.
• The swelling peaks in 3 days, subsided in 7 days. Fever resolves in 3-5 days. Submandibular salivary glands may also be involved and swollen without parotid involvement.
December 22, 2015
49
Complications
1- CNS complications: Meningitis or meningoencephalitis is most common complication along with gonadal involvement.Before, along with, or following Parotitis.
fever, malaise and lethargy in infants, while in older; headache, vomiting, and meningeal signs.
10%-30% clinical, 40%-60% lab
December 22, 2015
50
• CSF examination: White blood cell pleocytosis with a predominance of lymphocytes. The glucose is normal in most of the cases and low (hypoglycorrhachia) in 10 – 20%, while the protein is normal or mildly elevated.
• Other CNS complications include transverse myelitis, aqueduct stenosis and facial palsy.
Complications
December 22, 2015
51
Complications
2- Gonadal involvement: in young adolescent males, epidymo-orchitis is 2nd only to Parotitis as common.Involvement in prepubescent male is extremely rare, but following puberty it occurs in 30-40 % of male.
Atrophy may occur but sterility is rare.
Oophoritis is uncommon in post pubertal females,
December 22, 2015
52Complications
3- Endocrine: Pancreatitis and Thyroiditis.4- Cardiac: Myocarditis.
5- Joints: Arthralgia, monoarthritis, and polyarthritis.
6- Pulmonary: pneumonitis.
7- Renal: Nephritis.
8- Hematological: Thrombocytopenia.
9- Ophthalmic: Optic neuritis and conjunctivitis.
December 22, 2015
53
Diagnosis
History of exposure, incubation period and clinical findings.Raised serum amylase, leukopenia and relative lymphocytosis
Viral isolation.
Antibody titer.
December 22, 2015
54
• Pain
• Antipyretics• Adequate hydration
• the outcome of mumps is excellent even when complicated by meningitis or encephalitis, although fatal cases of CNS involvement have been reported.
December 22, 2015
55
Treatment
December 22, 2015
56• MMR: two-dose vaccine schedule, at 15 months and 4-6 yrs.
• If the second dose was not given at 4-6 yr, it should be given before puberty
• 64% vs. 88% protection, long lasting.
Prevention

December 22, 2015
57
December 22, 2015
58
December 22, 2015
59
December 22, 2015
60

December 22, 2015
61
December 22, 2015
62
December 22, 2015
63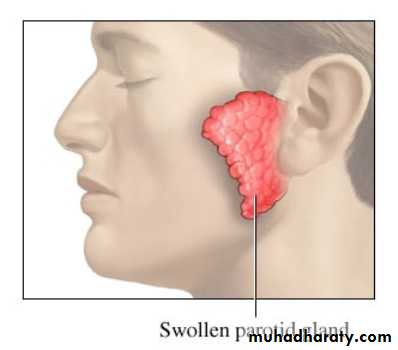
December 22, 2015
64
December 22, 2015
65December 22, 2015
66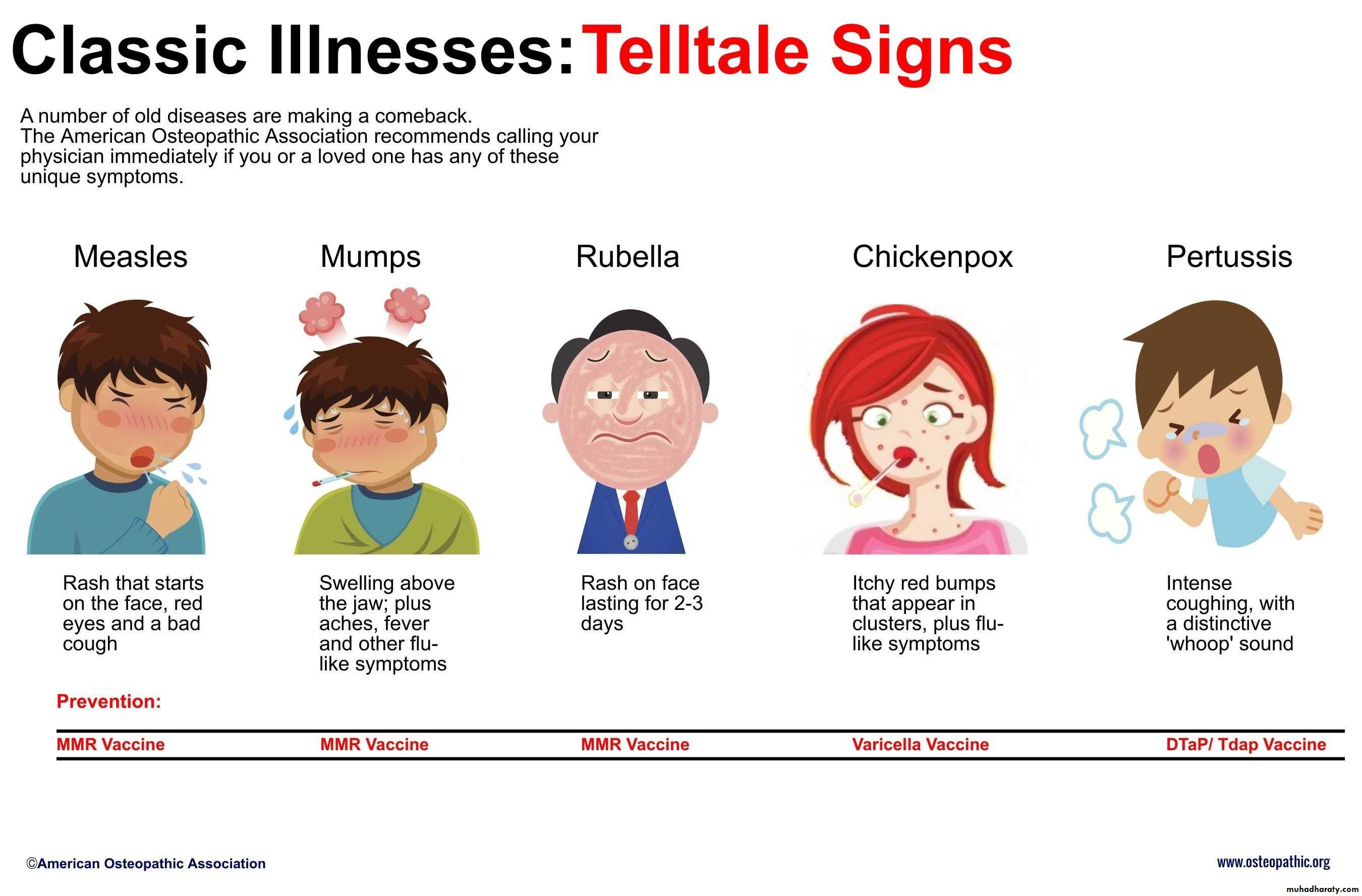
Thank you
December 22, 201567