Spinal Cord Compression
DescriptionIn order to understand spinal cord compression, it is useful to understand the structure of the spinal cord and to understand the difference between the spinal cord and the vertebral column . The vertebral column includes the bony structure surrounding the spinal cord and the spinal cord itself. Also an important part of the vertebral column, the intervertebral disks, are found between vertebrae. They act as shock absorbers. The spinal cord, however, is the series of nerves that runs down the hollow part of the vertebrae. Thus, the bony vertebrae and shock-absorbing disks protect the spinal cord from physical damage and compression.
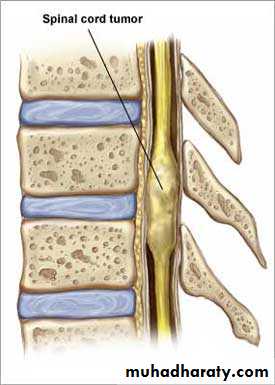
Spinal cord compression occurs when something presses down with sufficient force on the nerves within the spinal cord so that they lose their ability to function properly. Although trauma, degenerative back disease, and genetic disorders can cause pressure on the spinal cord, the term spinal cord compression is usually reserved for cases in which the presence of a tumor results in pressure on the spinal cord. The tumor may originate in a number of areas and either directly or indirectly put pressure on the cord.
Causes
The most common cause of cancerous spinal cord compression is a vertebral metastasis . A metastasis is a cancerous lesion that arises from another tumor somewhere else in the body. Vertebral metastases account for 85% of cases of spinal cord compression, and 70% of those metastases occur in the thoracic vertebrae. About 5% to 10% of patients with cancer will develop metastases to the spinal cord. Tumors may also grow from the nerves themselves, from the connective tissue surrounding the nerves, or, rarely, from the bony vertebrae themselves. Tumors that grow from outside the vertebral column may cause pressure by either growing into the hollow space in the vertebral column or by pressuring the vertebrae into an abnormal conformation. More rarely, tumors in the vertebrae may cause compression indirectly by causing the vertebrae to collapse. Tumors that originate in the spinal cord or in the connective tissue overlying the spinal cord cause direct pressure because there is a limited area in which they can grow before impinging on the cord directly.
Tumors that commonly cause cord compression are lung cancer (non-small cell type), breast cancer , prostate cancer , renal cell carcinoma , thyroid cancer , lymphoma and multiple myeloma .

Extradural tumors
Intradural intramedullary tumors
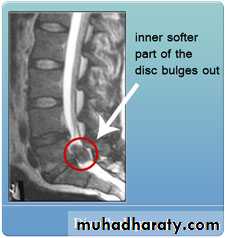
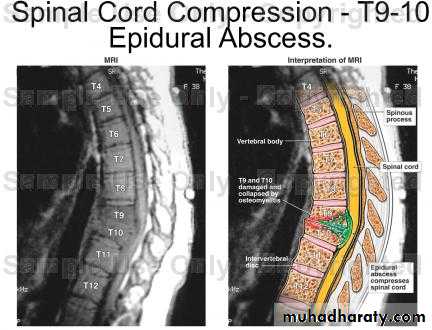
Spinal cord compression develops when the spinal cord is compressed by bone fragments from a vertebral fracture, an abscess , ruptured intervertebral disc or lesion. It is regarded as a medical emergency independent of its cause, and requires swift diagnosis and treatment to prevent long-term disability due to irreversible spinal cord injury .
These are common conditions that may cause spinal cord compression:
Osteoarthritis
Abnormal spine alignment
Injury to the spine
Certain bone diseases
Rheumatoid arthritis
Infection
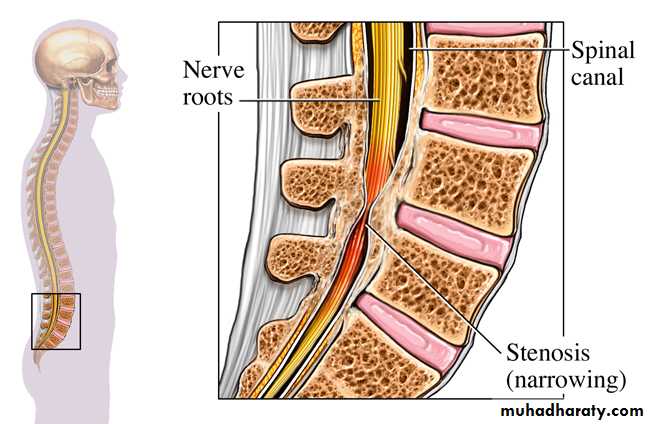
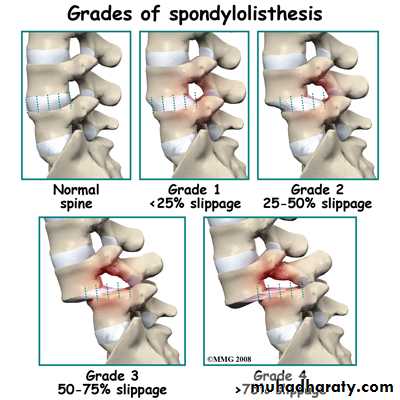
Spondylolisthesis
Clinically
Anatomical reviewVertebrae are, in order, divided into cervical, thoracic , lumbar, and sacral sections. The cervical vertebrae correspond to the neck, the thoracic vertebrae correspond to most of the torso , the lumbar vertebrae are found in the low back, and the sacral vertebrae correspond to the area of the buttocks. There are seven cervical, twelve thoracic, five lumbar, and five sacral vertebrae (although the sacrum is one bony structure and contains no inter-vertebral disks). The level of compression is indicated by using the first letter of the type of vertebra and then the number of the vertebra within the group. The topmost vertebrae are numbered lowest, so the first cervical vertebra is the vertebra closest to the head, and is known as C1. C7 is the cervical vertebra furthest down the spine. Compression of the spinal cord in this region would be known as compression at C7. The closer the compression is to the head, the more symptoms the patient is likely to have, since compression of the spinal cord affects all the levels of nerves below the area of compression that are part of the same nerve branch. For example, if movement were affected at C2 and below, a person would have difficulty using both arms and legs, whereas compression at T12 might result in just difficulty using the legs.
Anatomical review
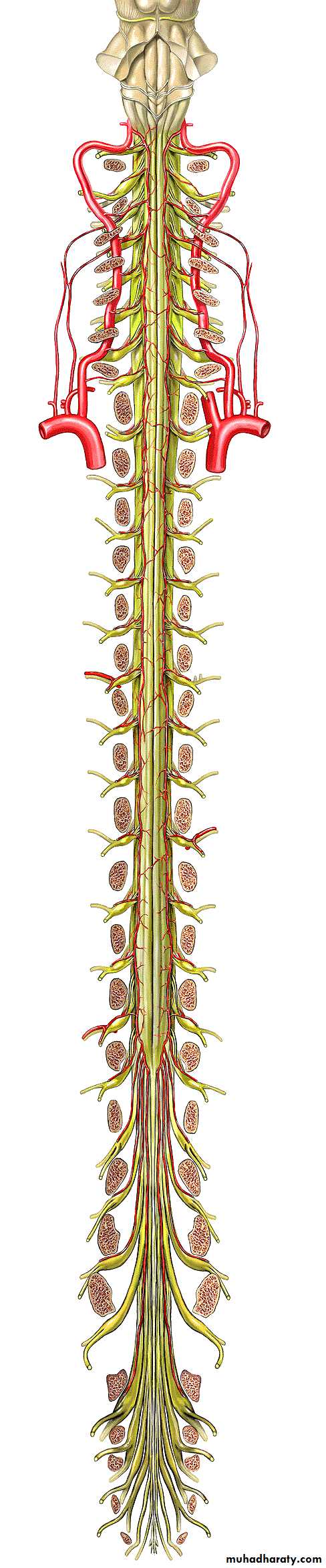
Spinal cord lies within protective covering of vertebral column.Begins just below foramen magnum of the skull.Ends opposite 2nd lumbar vertebra.Below L2 continue as a leash of nerve roots known as cauda equina.Prolongation of the pia matter forms filum terminale.
Symptoms
Importantly, the first symptom patients usually display prior to actual spinal cord compression is pain, especially pain that is not relieved by lying down, and which has lasted one month or more. This kind of pain should be sufficient to suspect imminent spinal cord compression due to cancerous causes. Also, there may be damage to nerve roots at the level of compression that can lead to symptoms in other parts of the body. For example, if the cord compression is in the lower part of the spine, then parts of the legs may be affected with numbness, tingling and loss of power and movement. Similarly, if the problem lies in the upper part of the spinal column, there may be a loss of power and sensation in parts of the arms or hands. If the cord compression becomes more severe, it can affect lower muscle functions such as bowel and bladder .Symptoms suggestive of cord compression are back pain , a dermatome of increased sensation, paralysis of limbs below the level of compression, decreased sensation below the level of compression, urinary and fecal incontinence and/or urinary retention .Lhermitte's sign (intermittent shooting electrical sensation) and hyperreflexia may be present.
Management
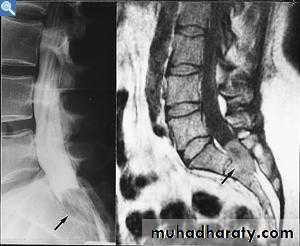
Diagnosis is by X-rays but preferably magnetic resonance imaging (MRI) of the whole spine. The most common causes of cord compression are tumors, but abscesses and granulomas (e.g. in tuberculosis ) are equally capable of producing the syndrome.If symptoms develop, prompt diagnosis and rapid treatment are crucial in order to avoid any permanent damage to the sensitive nerve tissue of the spinal cord. Usually, magnetic resonance imaging (MRI) or computed tomography (CT) scans will be performed to confirm cord compression and fully define the level and extent of the lesion.
Treatments
The goal of therapy for spinal cord compression includes pain control, avoidance of complications, preserving or improving neurologic functions, or reversing impaired neurologic functions. Treatment usually involves treatment of the underlying tumor. For most patients with cancer-induced compression, radiation therapy is the treatment of choice. However, if radiation therapy is unavailable or if neurologic signs worsen despite medical therapy, surgical decompression should be performed. Surgery is also indicated when a biopsy is needed, when the spine is unstable, when tumors have recurred after radiation therapy, or when any abscess is present. Finally, in some tumors known to be highly chemo responsive, chemotherapy alone or in combination with other modalities may be used.
High-dose corticosteroids (oral or IV dexamethasone ) may be promptly administered in order to reduce inflammation and pressure
Dexamethasone (a potent glucocorticoid ) in doses of 16 mg/day may reduce edema around the lesion and protect the cord from injury. It may be given orally or intravenously for this indication.
Surgery is indicated in localized compression as long as there is some hope of regaining function. It is also occasionally indicated in patients with little hope of regaining function but with uncontrolled pain. Postoperative radiation is delivered within 2-3 weeks of surgical decompression. Emergency radiation therapy (usually 20 Gray in 5 fractions, 30 Gray in 10 fractions or 8 Gray in 1 fraction) is the mainstay of treatment for malignant spinal cord compression. It is very effective as pain control and local disease control. Some tumours are
highly sensitive to chemotherapy (e.g. lymphomas, small-cell lung cancer) and may be treated with chemotherapy alone.
Prognosis
Once complete paralysis has been present for more than about 24 hours before treatment, the chances of useful recovery are greatly diminished, although slow recovery, sometimes months after radiotherapy, is well recognized.
The median survival of patients with metastatic spinal cord compression is about 12 weeks, reflecting the generally advanced nature of the underlying malignant disease.