Detection of Periodontal Disease
Clinical Examination: should include an evaluation of the soft tissue for sign inflammation (redness, bleeding, swelling & pus) & periodontal probing.Radiographic Examination:
Dental radiographs provide an overview of the amount of bone present & indicate the pattern, distribution & severity of bone loss.The bitewing radiograph is the view of choice for the evaluation of periodontal disease.
In addition to the periapical radiograph with paralleling technique could be used also, to evaluate the height of crestal bone is accurately recorded in relation to the tooth root.
Use of bisecting technique resulted in dimensional distortion of the bone due to the vertical angulation.

The normal alveolar crest lies 1 to 1.5 mm below the adjacent CEJs and forms a sharp angle with the lamina dura of the
adjacent tooth.
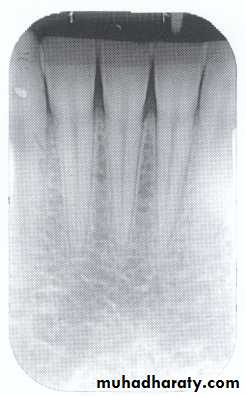
Between the anterior teeth the alveolar crest normally is pointed and well corticated.
Amount of bone loss
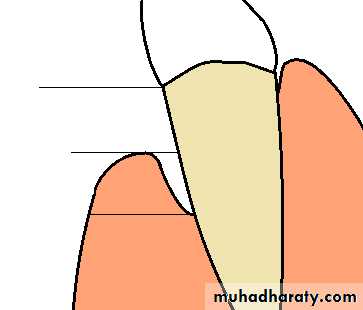
Normal alveolar bone level is 1 - 1.5mm from CEJ.CEJ
Crest of the remaining crest
YThe amount of bone loss = Y – 1 mm
Bone loss
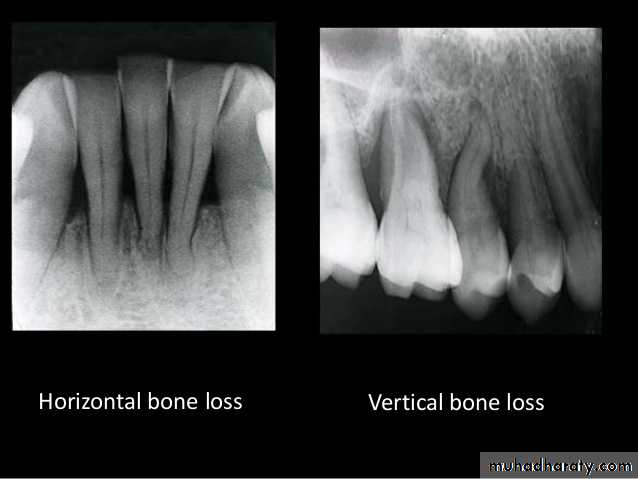
Direction :
Intercrestal bone should be parallel with line dawn from the CEJ of one tooth to that of the contacting tooth.1. Horizontal bone loss:- When loss occurs on a plane that is parallel with a line drown.

2.Vertical bone loss:- when there is greater bone loss in one tooth than on the adjacent tooth, so the bone level is not parallel with a line joining the CEJ.
Vertical osseous defects can be divided into two primary types: Interproximal crater is a two-walled, trough like depression
that forms in the crest of the interdental bone between adjacent teeth.
The Infrabony defect is a vertical deformity within bone that extends apically along the root from the alveolar crest.
Types of infrabony defect (to design the treatment plan) :
Three-walled :surrounded by three bony walls.
Two-walled when both buccal and lingual cortical plates remain.
One-walled when one of these plates has been resorbed .

A two-walled infrabony defect has one
side wall remaining and one wall lost.
Interproximal crater
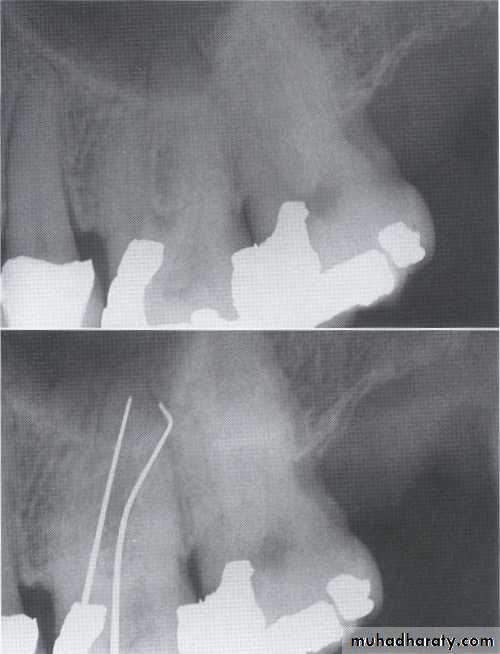
Often infrabony defects are difficult or impossible to recognize on a radiograph because one or both of the cortical bony plates remain superimposed with the defect.
Clinical and surgical inspections are the best means of determining the number of remaining
bony walls.
Visualization of the depth of pockets
may be aided by inserting a gutta-percha
point.
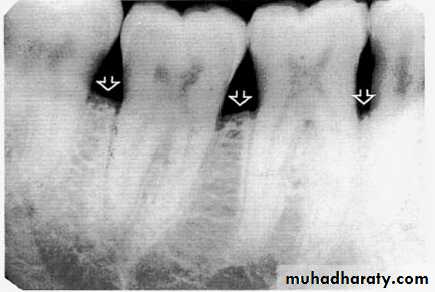
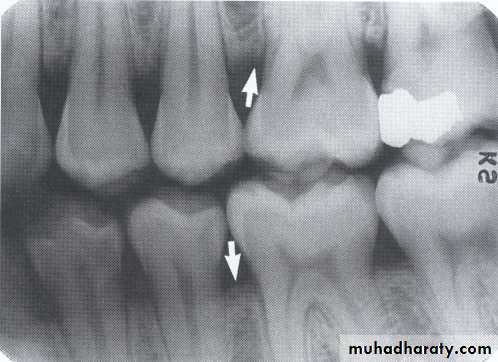
3.Furcation involvements:
Bone loss in the furcation area of the roots which is evidence of advanced disease in multirootedteeth.
Initially seen as widening of the PL space at the crest of
the furcation . As lesion progresses, the bone
loss progresses apically.
Mild/moderate/sever.




Bone loss
• Distribution: either localized or generalized, depend on the area involved.• Localized bone loss occurs in the isolated area.
• Generalized type occurs evenly throughout the dental arches.
•

Bone loss
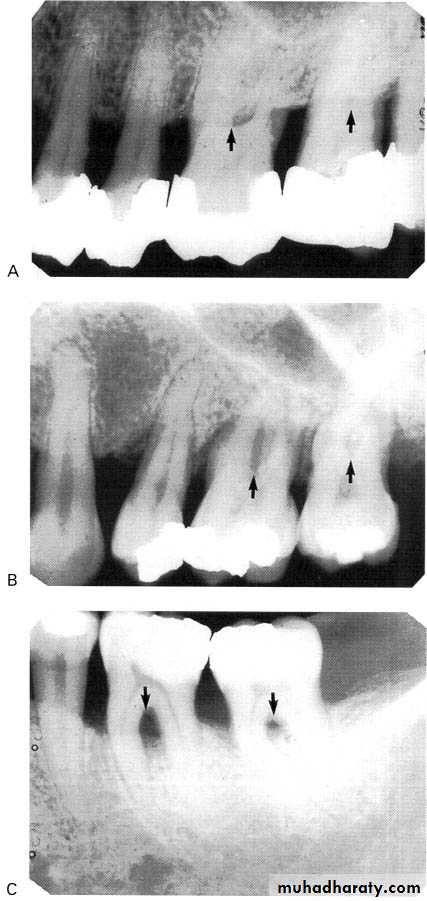
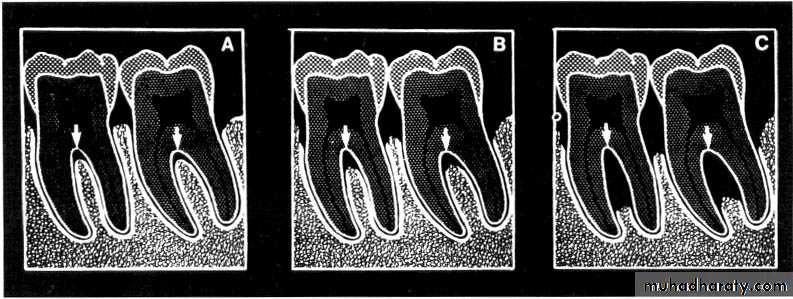
• Severity: classified toMild bone loss: crestal changes (The anterior regions show blunting of the alveolar crests and slight loss of alveolar bone height.Posteriorly show loss of the normally sharp angle between the lamina dura and alveolar crest).
• Moderate bone loss: bone loss of 10-33%.
• Severe bone loss: bone loss of 33% or more.
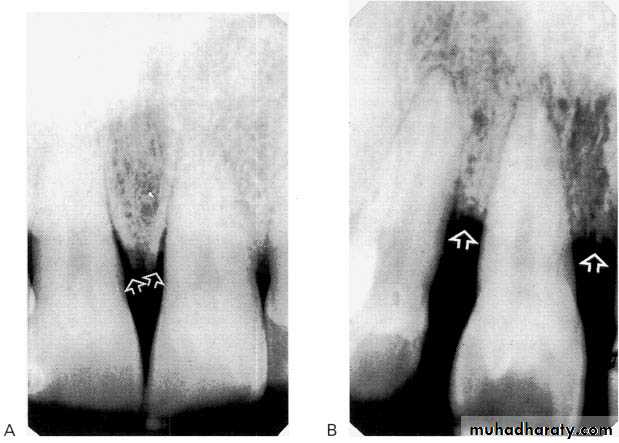
A:moderate,B:sever.
Mild bone loss
Classification of Periodontal DiseaseType-I: there is no bone loss associated with this type but only gingivitis, & no radiographic changes are seen.
Type-II: there is mild periodontitis, & mild crestal changes.
Type-III: the bone loss is moderate about 10-33%. The pattern bone loss may be localized or generalized, vertical or horizontal. Furcation area of multirooted teeth may be involved.
Type-IV: its advanced periodontitis, with more than 33% of bone loss is seen.

Predisposing Factors
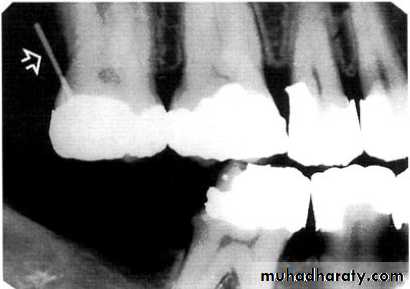
A-Calculus:It is a stone-like concretion that forms on the crown & roots of the teeth due to the calcification of bacterial plaque.
Its appear as radiopaque on the dental radiograph.
its either pointed or irregular radiopaque projection extending from the proximal root surface.
Calculus may be seen as a ring-like radiopacity encircling the cervical portion of the tooth.

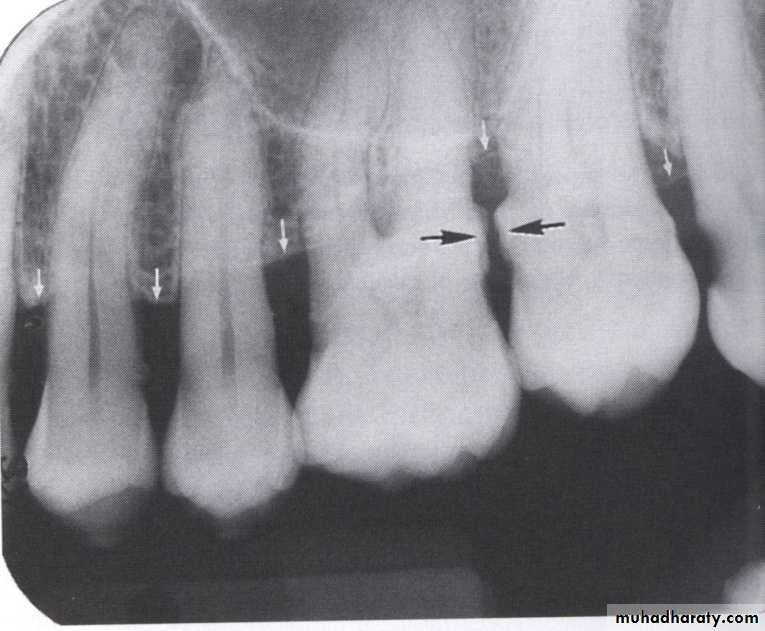
CALCULUS
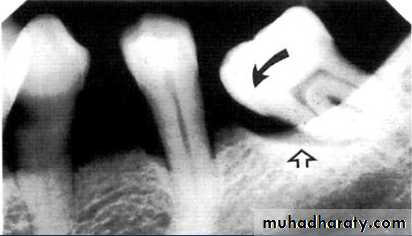
Predisposing Factors• B-Defective Restoration;
• Faulty dental restoration act as potential food traps & lead to the accumulation of food debris & bacteria.
• Radiographically; the defective filling identified with open or loose contacts, poor contour, uneven marginal ridges over-hangs.

caries
Overhang rest.