IV FluidsIntravenous Fluids

Intravenous administration refers to the introduction of fluids directly into the venous blood stream.
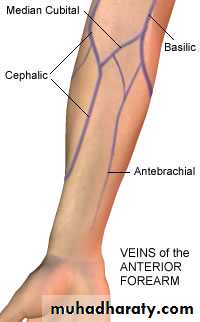
Administrating sterile fluid into a Suitable vein which could be:
-Arm vein e.g., Ante-cubital fossa, wrist….-Scalp vein in an infant.
-Other veins, ex saphenous vein…. ex. Burns through venesectionIV Fluids:



Aims (Indications) of intravenous fluids:
*(Water and electrolytes loss = gain).1- To correct or prevent fluid and electrolyte imbalance (dehydration, bleeding, burn, post operation).
2- To correct or prevent nutritional imbalance.
3- To provide IV medication.
There are two components to fluid therapy:
1- Maintenance therapy: replaces normal ongoing losses.Maintenance therapy is usually undertaken when the individual is not expected to eat or drink normally for a longer time (e.g., preoperatively, or on a ventilator).
2- Replacement therapy: corrects any existing water and electrolyte deficits.
• In order to administrate iv fluid we need:
1-The sterile Fluid:

2-Container:
either a Plastic bag or Glass container

• 3-IV infusion Set:
1-Insertion spike. 2- Drip chamber (filter). 3- Rate Control clamp (regulator). 4- Rubber injection portal. 5- Plastic tube. 6- Needle adaptor.• “Adult or pediatrics”





Pediatric Infusion Set

Infusion Pump

Infusion Pump
4-Needle or Cannula-Venesection set
Needle gage: 14-16-21-33
-Cannulacolor







Indications of IV fluids???
1-DehydrationIn a patient who Can Not tolerate oral therapy or in severe cases.
2-Hypovolaemic shock-Bleeding.
-Burns.
3-Post operative patients:
-After surgery4-Administration of drugs
5-Parentral NutritionTotal Parenteral nutrition
Complications of IV fluids???Complications of IV fluids:
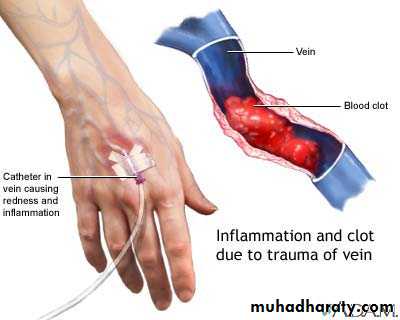
1- Phlebitis, thrombophlebitis.2- Sepsis.
3- Extravasation.
4- Air in tube/air embolus.
5-Glucose and electrolyte disturbances.
Na, k, Hypoglycemia, Hyperglycemia, Hyponitraemia
6- Circulatory overload, hypertension and pulmonary edema.
(rapid administration in pediatrics ,heart failure).
• 1-Glucose and electrolyte disturbances:
• -Na, K
• -Hypoglycemia
• -Hyperglycemia
• -Hyponatremia
• ………..etc
2-Circulatory disturbances:
-Heart failure-Rapid administration.
Pediatrics3-Hypertension
• 4-Local complications:• Thromophlebitis Cellulitis infections
• Leaving cannula for more than 3 days:
• -Redness
• -Hotness
• -Tenderness
Other less common complications:
-Septicemia-Air embolism
1-Crystalloids:
-Water-Electrolytes
-Glucose
Types of IV fluids:
2-Colloids“Plasma expanders”
Gelatin, starch……etcParentral nutrition
Colloids are a form of suspension of high molecular weight molecules.
Can be separated by physical meansCentrifugation
Albumin , Gelatin, Starch• Isotonic:
• 285-295 mOsm/kg• Osmotic pressure = normal body
• Hypertonic: higher than the body
• Hypotonic: lower than body
Crystalloids:
Isotonic Solutions:
1-Normal saline:0.9 % NaCl
2-Dextrose water 5 %
Glucose???3-Dextrose Saline:
0.9%1/3 = 0.3 % NaCl + 5 % Dextrose
1/5 = 0.18 % NaCl + 5% Dextrose4-Dextrose In saline:
0.9 % NaCl + 5 % Dextrose5-Compound sodium lactate solution
-Hartman's solution-Ringers lactate solution
K, Ca, Lactate
• One liter of lactated Ringer's solution contains:• 130 mEq of sodium ion = 130 mmol/L
• 109 mEq of chloride ion = 109 mmol/L
• 28 mEq of lactate = 28 mmol/L
• 4 mEq of potassium ion = 4 mmol/L
• 3 mEq of calcium ion = 1.5 mmol/L
• Generally, the sodium, chloride, potassium and lactate come from NaCl (sodium chloride), NaC3H5O3 (sodium lactate), CaCl2 (calcium chloride), and KCl (potassium chloride).
• There are slight variations for the composition for Ringer's as supplied by different manufacturers..
• Although its pH is 6.5, it is an alkalizing solution.
-Hypertonic glucose 10% 20 % 50%
Hypertonic:-Mannitol 5% (isotonic)
( 10% 20%) Hypertonic
-Brain edema
-laxative
Mannitol:
Conc. (%)
g/100 mLmOsmol/liter (calc.)
pH*
5
5
274
6.3 (4.5 to 7.0)
10
10
549
6.3 (4.5 to 7.0)
15
15
823
6.3 (4.5 to 7.0)
20
20
1098
6.3 (4.5 to 7.0)
25
25
1372
5.9 (4.5 to 7.0)
Mannitol
When administered intravenously mannitol is confined to the extracellular space, only slightly metabolized and rapidly excreted by the kidney.
The drug is freely filtered by the glomeruli with less than 10% tubular reabsorption; it is not secreted by tubular cells.
Mannitol induces diuresis by elevating the osmolarity of the glomerular filtrate and thereby preventing tubular reabsorption of water.
Therapeutic Use of mannitol:
Promotion of diuresis in the prevention or treatment of the oliguric phase of acute renal failure before irreversible renal failure becomes established.
Reduction of intracranial pressure and brain mass.
Reduction of high intraocular pressure when the pressure cannot be lowered by other means.Promotion of urinary excretion of toxic materials.
• Dose calculation of IVF:• -60-70 % of body is water
• Blood is 5 liters:
• Average adult requirement is 2-3 litters /24 hours
• 2000-3000 ml
Each 1 ml = 15 drops