Gastrointestinal Diseases
Objectives of the lecture:Normal GIT phenomena
Major signs & symptoms of GIT diseases
What’s diarrhea, its types & causes
Dehydration. How to assess? How to treat?
• Normal Digestive Tract Phenomena :
GI function varies with maturity; what is a physiologic event in a newborn or infant might be a pathologic symptom at an older age.short lingual frenulum (tongue-tie) may be worrisome to parents but rarely interferes with eating or speech, generally requiring no Rx.
Surface furrowing of tongue (a geographic or scrotal tongue) is usually a normal finding.
bifid uvula:normal or associated with a submucous cleft palate.
Regurgitation, the result of GER, occurs commonly in the 1st yr. Effortless reg. can dribble out of an infant's mouth but may be forceful. Episodes can occur from <1 - several times daily. It gradually resolves in 80% of infants by 6 mo & in 90% by 12 mo.

Tongue tie

Geographical tongue

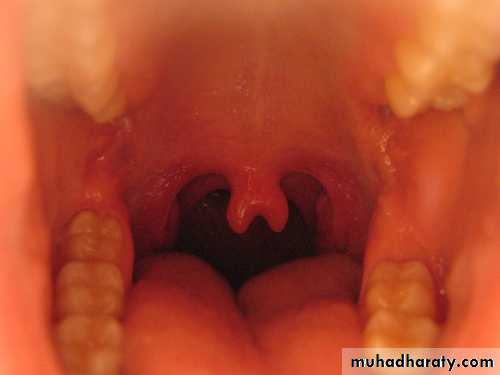
Bifid uvula
• The number, color, and consistency of stools can vary greatly in the same infant & between infants of similar age without apparent explanation. The earliest stools after birth consist of meconium, a dark, viscous material that is normally passed within the 1st 48 hr of life. With the onset of feeding, meconium is replaced by green-brown transition stools, often containing curds, and, after 4-5 days, by yellow-brown milk stools.• Stool frequency is extremely variable in normal infants and can vary from none to 7 per day. Breast-fed infants can have frequent small, loose stools early (transition stools), and then after 2-3 wk can have very infrequent soft stools. Some nursing infants might not pass any stool for 1-2 wk and then have a normal soft bowel movement.
The color of stool has little significance except for the presence of blood or absence of bilirubin products (white-gray rather than yellow-brown).


meconium

Acholic stool

Bloody stool
protuberant abdomen is often noted in infants and toddlers, especially after large feedings. This can result from the combination of weak abdominal musculature, relatively large abdominal organs, & lordotic stance.In the 1st yr of life, it is common to palpate the liver 1-2 cm BCM.
A Riedel lobe is a thin projection of the right lobe of the liver that may be palpated .A soft spleen tip might also be palpable as a normal finding. In thin young children, the vertebral column is easily palpable, and an overlying structure may be mistaken for a mass.
Pulsation of the aorta can be appreciated.
Normal stool can often be palpated in the left lower quadrant in the descending or sigmoid colon.Blood loss from GIT is never normal, but swallowed blood may be misinterpreted as GI bleeding. Maternal blood may be ingested at the time of birth or later by a nursing infant if there is bleeding near the mother's nipple. Nasal or oropharyngeal bleeding is occasionally mistaken for GI bleeding .
Red dyes in foods or drinks can turn the stool red .
Jaundice is common in neonates, especially among premature infants, It could be physiological or pathological.
• Major Symptoms and Signs of GIT Disorders:
• Disorders of organs outside GIT can produce symptoms and signs that mimic GIT disorders & should be considered in DDx.Dysphagia(Difficulty in swallowing ):
• .
• Painful swallowing is termed odynophagia.
Globus is the sensation of something stuck in the throat without a clear etiology. It is classified as:
• Oropharyngeal dysphagia(transfer dysphagia) occurs when the transfer of the food bolus from the mouth to the esophagus is impaired.The striated muscles of the mouth, pharynx &UES are affected. Neurologic & muscular disorders are causes . The most serious complic. is life-threatening aspiration.
• Esophageal dysphagia occurs when there is difficulty in transporting the food bolus down the esophagus. ED can result from neuromuscular disorders or mechanical obstruction.
• Regurgitation(spitting): effortless movement of stomach contents into esophagus & mouth.
• Anorexia: prolonged lack of appetite.
• Vomiting:
• highly coordinated reflex process that may be preceded by increased salivation & begins with involuntary retching. Violent descent of the diaphragm & constriction of the abdominal ms with relaxation of the gastric cardia actively force gastric contents back up the esophagus.
• Vomiting caused by obstruction of the GIT is probably mediated by intestinal ns stimulating the vomiting center .It is either bilious or non bilious. CNS or metabolic derangements can lead to severe, persistent emesis.
• Cyclic vomiting is a syndrome with numerous episodes of vomiting interspersed with well intervals.
• Diarrhea :
defined as xs loss of fluid & electrolyte in stool. Acute diarrhea is defined as sudden onset of excessively loose stools of >10 mL/kg/d in infants & >200 g/24 hr in older children & lasts <14 days. If lasts >14ds chronic or persistent diarrhea.
Steatorrhea xs fat in stool is a symptom of malabsorption. Disorders that interfere with absorption in the small bowel voluminous diarrhea
Large bowel lower-volume diarrhea.
Dysentery (small-volume, frequent bloody stools + mucus, tenesmus & urgency) predominant symptom of colitis.
Movement of water across the GIT mucosa is passive. Many nutrients, including glucose & most AAs, are absorbed by active, carrier-mediated transport, coupled with Na+ transport. The osmotic gradient created promotes the absorption of water. Movement of water, in turn, carries small solutes such as Na+ & Cl-. This is known as solvent drag & appears to be an important route for Na absorption during normal digestion & it is the base for oral rehydration solution(ORS).
• The pathophysiologic mechanisms for diarrhea are:
• 1.osmotic diarrhea(OD)The ingestion of a poorly absorbable, osmotically active subs & its presence in the bowel lumen create an osmotic gradient that encourages movement of H2O into lumen & subsequently into stool. Electrolyte losses increase because they will follow H2O into lumen through solvent drag .
Two main groups of poorly absorbed solutes exist, the ingestion of which result in OD:
1st normal dietary components that may be malabsorbed ( transiently or permanently). E.g. , disaccharides are usually hydrolyzed to monosaccharides before they are absorbed. If a mucosal disaccharidase is deficient, then the disaccharide will be malabsorbed & will produce diarrhea.Medium-chain triglycerides also osmotically active, Malabsorption of long-chain triglycerides (LCTs) does not lead to OD because LCTs are large hydrophobic molecules.
Protein malabsorption does not appear to be associated with diarrhea except in the rare instance of congenital trypsinogen or enterokinase deficiency.
2nd substances that are transported in limited amounts, even by healthy individuals. This includes Mg, PO4, & sulfates. Because these ions invariably lead to diarrhea when given in large amounts, they are used as cathartics. Another e.g. lactulose
The key character of OD is its association with the ingestion of the offending solute. When a pt who has OD is given no oral or enteral feeding, the diarrhea will stop dramatically within 24 hours or less. If the agent is reintroduced, the diarrhea will reappear.
The diarrhea is of a moderate volume compared with that in secretory diarrhea.
Normally, the electrolyte conc. in stool is roughly twice its combined Na + & K+ conc. When this number is much ˂ total stool osmolality (usually approximately 290 mOsm/kg), osmotically active nonelectrolytes must be in stool, & OD is present. An osmotic gap of ˃ 100 mOsm/kg indicates OD.Ion(osmotic) gap = stool osmolality - [(stool Na + stool K) ×2]
• 2. secretory diarrhea:• occurs when a physiologic electrolyte secretory process is pathologically stimulated Increase in luminal electrolytes &, subsequently, a secondary increase in water occur.
• The electrolytes that have been implicated are Na, Cl, and perhaps HCO3.
• It is usually of large volume & persists even with fasting. The ion gap is 100 mOsm/kg or less & stool osmolality is normal.
• The prototype for a secretory diarrhea is cholera.

• 3.exudative diarrhea:
A break in the integrity of the mucosal surface of the intestine can result in H2O & electrolyte loss, driven by hydrostatic pressure in bd vessels & lymphatics. The exudate contains mucus, protein & blood cells.e.g. infectious(Salmonella, Shigella, amebiasis)
allergic, or ulcerative colitis.
4.diarrhea resulting from abnormal intestinal motility:
Increased, decreased, or disordered movement of intestine can lead to diarrhea.
Increased motility may cause diarrhea by allowing less time for the contact of intraluminal contents with absorptive surfaces.
Slowed transit and severely disordered motility lead to intraluminal stasis which leads to the development of bacterial overgrowth.
e.g. short-bowel syndrome, irritable bowel syndrome.
It denotes infections of GIT caused by bacterial, viral, or parasitic pathogens. Many of these infections are foodborne illnesses. The most common manifestations are diarrhea & vomiting, which can also be associated with systemic features such as abdominal pain & fever. It is common in children, transient & usually self-limited.
• USUALLY WITHOUT BLOOD IN STOOL
• Viral enteritis : rotavirus, caliciviruses, enteric adenovirus, astrovirus….• Enterotoxin : Escherichia coli, Klebsiella organisms, cholera, Clostridium perfringens, Staphylococcus organisms, Bacillus cereus, and Vibrio species
• Parasitic : Giardia, Cryptosporidium…..
• Extraintestinal infection( parenteral) : otitis media and UTI.
• Antibiotic-induced and Clostridium difficile toxin (without pseudomembranous colitis)
Causes of Acute Diarrhea
• COMMONLY ASSOCIATED WITH BLOOD IN STOOL
• Bacterial : Shigella, Salmonella, and Campylobacter organisms, Yersinia enterocolitica, invasive E coli, gonococcus (venereal spread), enteroadherent E coli,• enteroaggregative E coli, Aeromonas hydrophilia, and Plesiomonas shigelloides.
• Cytomegalovirus (especially in immunocompromised individuals)
• Amebic dysentery, Trichuris trichiura (whipworm)
• Hemolytic-uremic syndrome (enterohemorrhagic E coli—E coli O157:H7 and other Shiga toxin-producing E coli)
• Henoch-Schonlein purpura
• Pseudomembranous enterocolitis (C difficile toxin)
• Ulcerative or granulomatous colitis (acute presentation)
• Necrotizing enterocolitis (neonates)
Non inflammatory diarrhea
• Pathogenesis of Infectious Diarrhea:
enterotoxin production ,destruction of villus cells by viruses, adherence by parasites, & adherence and/or translocation by bacteria
bacteria that directly invade the intestine or produce cytotoxins with consequent fluid, protein, and cells (erythrocytes, leukocytes) that enter the intestinal lumen.
Inflammatory diarrhea
• Risk Factors for Gastroenteritis :
• Environmental contamination• increased exposure to enteropathogens
• young age
• immunodeficiency
• measles
• malnutrition
• lack of exclusive or predominant breast-feeding
vitamin A deficiency risk of dying from diarrhea, measles, and malaria is increased by 20-24%.
Zinc deficiency risk of mortality from diarrhea, pneumonia, and malaria is increased by 13-21%.
• Neonatal Diarrhea
Neonates with acute diarrhea must be considered differently from older infants & children because of:lower tolerance to the associated fluid shifts .
greater likelihood of severe infection or of a congenital anomaly.
Necrotizing enterocolitis(NEC):
gastric retention (frequently bilious), distention & occult or bright red bd in stool, should raise concern. Although this disease usually occurs in premature infants, it also may occur in full-term infants.
Abdominal XR: pneumatosis intestinalis, gas in the portal vein, or free intraperitoneal gas(pneumoperitoneum) supports Dx.
Epidemics of diarrhea associated with rotavirus, enteropathogenic E coli, salmonellae,other organisms, reported in nurseries.

pneumoperitoneum
If the onset of diarrhea is associated with initial feedings, then the clinician should consider congenital digestive defects especially sugar intolerance.Hirschsprung disease may produce acute diarrhea and enterocolitis in the neonatal period & considered in the infant who has not passed meconium in the first 24 hours.
• Bloody diarrhea that results from cow milk or soy protein intolerance may develop as early as the first few ds of life. Resolution & exacerbation on removal and reintroduction of cow milk or soy formula, as well as an atopic family Hx, are clues to Dx.
DDx of diarrhea in Older Infant and Child
Most episodes of acute diarrhea are transient & benign. First one should: assess the hydration status then to know the cause.It is usually the result of viral enteritis, typically occurring with low-grade fv, v & frequent watery stools. Generally, the stools without bd or WBC.
Enterotoxin-producing organisms (eg toxigenic E coli) are associated with watery stools and are without evidence of mucosal invasion (no high fever or bd in stool).

Diarrhea in association with extraintestinal infections, most notably otitis media and pyelonephritis, has been called parenteral diarrhea; its mechanism is obscure
Certain antibiotics, especially ampicillin, have been associated with transient diarrhea. Less common but of greater danger is antibiotic-associated pseudomembranous colitis(PMC) which may occur acutely or as a more chronic illness of 1 or 2 months' duration. C difficile toxin, the cause of most cases of PMC.
The presence of bd in stool, especially with symptoms of colonic involvement should make the clinician think of infection with :
Campylobacter (Up to 40% of individuals who have Guillain-Barre syndrome have evidence of a Campylobacter infection occurring before the onset of neurologic symptoms).
Shigella (Patients appear severely ill and may have meningismus or seizures. The stools tend to be foul smelling).
Salmonella organisms
C. difficile toxinYersinia enterocolitis .
E coli can produce diarrhea by several pathogenic mechanisms; the enteroadherent, enteroinvasive, enterohemorrhagic, and enteroaggregative .Amebiasis ( Entamoeba histolytica) can produce a picture of acute colitis.
Non infectious causes of bloody diarrhea:intussusception
immune deficienciesChronic inflammatory bowel disease (IBD)
Food-borne spread of organisms or toxins is an important cause of acute diarrheal illness.
• Clinical Evaluation of Diarrhea :
• HISTORY
• 1. Length of illness
• 2. Character of stools: frequency, looseness (watery vs mushy)& presence of gross blood
• 3. Oral intake: diet, quantity of fluids & solids taken
• 4. Presence of vomiting
• 5. Associated symptoms: fever, rash & arthralgia
• 6. Urine output: frequency and qualitative amount
• 7. Possible exposure to diarrheal illness, child-care center attendance
• PHYSICAL EXAMINATION
• 1. Hydration status: weight (stable or loss), mucosa (moist or dry), saliva & tears (present or absent), skin turgor (normal or poor), eyeballs & fontanelle (normal or sunken), & vital signs
• 2. Alertness
• 3. Infant: vigor of suck
Assessment of Degree of Dehydration:
Mild
ModerateSevere
Infant(wt loss)
5%
10%
15%
Adolescent
3%
6%
9%
Infants and young children
Thirsty; alert; restless
Thirsty; restless or lethargic but irritable or drowsyDrowsy; limp, cold, sweaty, cyanotic extremities; may be comatose
Older children
Thirsty; alert; restless
Thirsty; alert (usually)Usually conscious (but at reduced level), apprehensive; cold, sweaty, cyanotic extremities; wrinkled skin on fingers and toes; muscle cramps
Signs and Symptoms
Tachycardia
Absent
PresentPresent
Palpable pulses
Present
Present (weak)Decreased
Blood pressure
Normal
Orthostatic hypotensionHypotension
Cutaneous perfusion
Normal
Normal
Reduced and mottled
Skin turgor
Normal
Slight reductionReduced
Fontanel
Normal
Slightly depressedSunken
Mucous membrane
Moist
DryVery dry
Tears
Present
Present or absent
Absent
Respirations
Normal
Deep, may be rapidDeep and rapid
Urine output
Normal
OliguriaAnuria and severe oliguria

• LABORATORY (PERFORMED AS INDICATED)
• Stool exam: culture, ova and parasites, smear for WBC, C. difficile toxin assay, occult bd & reducing substances• 2. CBC: Hemoconcentration ↑ Hb & PCV
• blood urea nitrogen (BUN),serum creatinine & electrolytes
• 4. GUE:the urine SG is usually ↑ (≥1.025) in significant dehyd, but ↓ after rehyd.
• With dehydration, GUE may show hyaline and granular casts, a few WBC & RBC, and 30 to 100 mg/dL of proteinuria
• 5. If child is lethargic or has seizure, culture for sepsis: measure BUN, S. electrolyte, glucose & CSF.
Calculation for correction of dehydration
1.Deficit:
A child with dehydration has lost water; there is usually a concurrent loss of Na+ and K+
• Water deficit =%dehydration× weight
• Sodium deficit = Water deficit × 80 mEq/L
• Potassium deficit = Water deficit × 30 mEq/L
e.g. for a 10-kg child with severe dehydration:
deficit of water= 10/100×10=1 liter
2.Maintenace fluid(water):BODY WEIGHT
FLUID PER DAY
0-10 kg
100 mL/kg
11-20 kg
1,000 mL + 50 mL/kg for each kg >10 kg
>20 kg
1,500 mL + 20 mL/kg for each kg >20 kg♯
♯The maximum total fluid per day is normally 2,400 ml
3.Ongoing losses :
From diarrhea or vomiting or urine or skin & lungs should be replaced ml/ml
• Sources of Water losses:• Urine 60%
• Insensible losses (skin and lungs)35%
• Stool 5%
• Maintenance requirements of electrolytes:
• Sodium: 2 - 3 mEq/kg/day
• Potassium: 1 - 2 mEq/kg/day.
Fluid Management Of Dehydration:
1.Restore intravascular volume( fluid bolus or shoot):NS or Ringer's lactate : 20 mL/kg over 20 min (repeat until IVF restored, 3 ×)
2.Calculate 24-hr water needs
Calculate maintenance water
Calculate deficit water
3.Calculate 24-hr electrolyte needs
Calculate maintenance Na+ and K+
Calculate deficit Na+ and K+
4.Select an appropriate fluid (based on total water and electrolyte needs).
For a pt with isotonic dehydration, D5 half NS with 20 mEq/L KCl) usually an appropriate fluid.
For a child weighing ˂ 10 to 20 kg, with mild dehydration, a reduction of the Na concentration is usually reasonable (1/4 NS) because the Na+ deficit is small. K+ usually is not included in the IV fluids until the pt voids, unless significant hypok+ is present. So it will be:
D5 1/2NS+ 20 mEq/L KCl or D5 0.2NS + 20 mEq/L KCL
• solution• Glucose (g/l)
• Na+
• Mmol/l
• K+
• Ca+2
• Cl-
• Lactate
• D5W
• 50
• 0
• 0
• 0
• 0
• 0
• D10w
• 100
• 0
• 0
• 0
• 0
• 0
• NS
• 0
• 154
• 0
• 0
• 154
• 0
• ½ NS
• 0
• 77
• 0
• 0
• 77
• 0
• ¼ NS
• 0
• 38.5
• 0
• 0
• 38.5
• 0
• D5NS
• 50
• 154
• 0
• 0
• 154
• 0
• D5 ½ NS
• 50
• 77
• 0
• 0
• 77
• 0
• 0.2 NS
• 0
• 31
• 0
• 0
• 31
• 0
• 3%NaCl
• 0
• 513
• 0
• 0
• 513
• 0
• LR
• 0
• 130
• 4
• 3
• 109
• 28
•
• Administer half the calculated fluid during the first 8 hr, first subtracting any boluses from this amount. Administer the remainder over the next 16 hr
• 5.Replace ongoing losses as they occur.
• In all children, it is critical to carefully monitor vital signs, wt, UOP, and electrolytes to identify over- or underhydration, hypona, & other electrolyte disturbances, then adjust the rate or composition of the IV solution accordingly.