Tumors of the Pharynx
Tumors of the Nasopharynx.Pseudotumors: the commonest cause of a mass in this region and includes adenoid and antrochoanal polyp.
. Benign tumors: angiofibroma, hemangioma, chondroma, leiomyoma, fibroma.
. Malignant tumors : Squamous cell carcinoma, lymphoma, adenocarcinoma
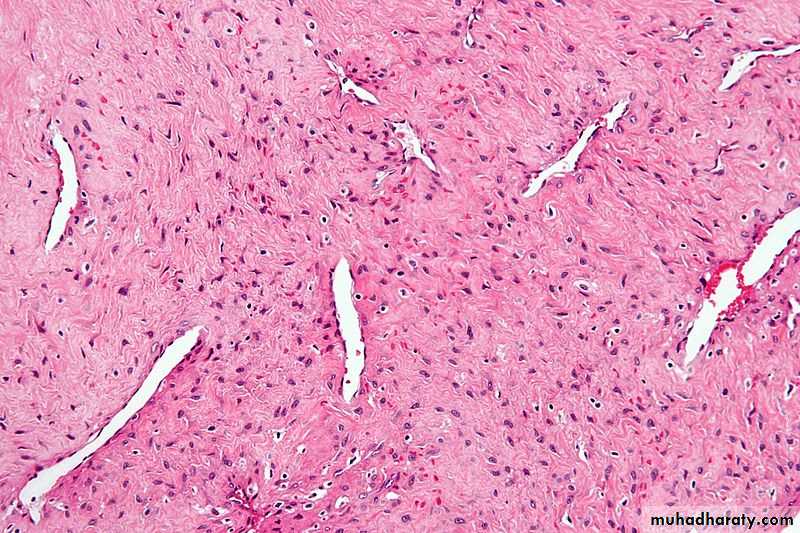
Angiofibroma
Benign vascular tumor arising in the nasopharynx of adolescent males and exhibiting strong tendency to bleed.It is exclusively a disease of males with mean age of 14 years.
Pathology:
Grossly: firm, spongy, lobulatedpinkish-white color
sharply demarcated
Microscopically: vascular spaces
fibrous tissue stroma
With increasing age the amount of fibrous tissues increase on the expense of the vascular tissues
Site of origin: sphenopalatine foramen present on the lateral wall of the nasal cavity. It then extends into the nasal cavity, paranasal sinuses, orbit and even intracranially.
Clinical presentations:
1- Nasal obstruction
2- Epistaxis: ranging from mild to severe life threatening.
3- Deafness: due to Eustachian tube orifice obstruction.
4- Proptosis: due extension into the orbit.
5- Headache and neurological manifestations: due to intracranial extension.
6- On exam.: pale patient, on posterior rhinoscopy (by mirror or endoscopy) a pinkish or red lobulated mass could be seen.
Investigations:
1- plain x-ray: soft tissue shadow and bone erosion2- tomography
3- CTS and MRI : site and extent of the tumor
4- angiography: shows a vascular blush in the nasopharynx and is useful to determine the feeding vessel
Biopsy is contraindicated
Treatment:
Mainly surgical: At least 3 units of blood should be preparedThere are different techniques used preoperatively to reduce the tumor size and vascularity:
1- Hormonal therapy: testosterone and /estrogen
2- Radiotherapy: also for inoperable intracranial extension or recurrent tumor
3- Embolization
Careful follow up is important because the tumor might recur.


NASOPHARYNX
Malignant tumorsSCC is the commonest, lymphoepithrlioma is a avariant of SCC. Other less common malignant tumors as lymphoma, sarcoma, salivary tumors.
Incidence :
Two peaks , at the 2nd decade and 5th decade
Male more than female 2:1
Chinese population more commonly affected by this tumor.
Aetiology:
1- Epstein-bar virus
2- chemicals : tobacco, wood-dust
3- diet : salted fish and nitrosamines
4- genetic predisposition, HLA linked
Clinical features:
1- Cervical lymphadenopathy: presented as a neck mass in 60% of patients.
2-Nasal symptoms: nasal obstruction, discharge and epistaxis in 40% of cases.
3- Audiological symptoms: deafness and tinnitus due to eustachian tube obstruction in 30% of cases.
4- Neurological : cranial nerves palsy and Horner’s syndrome in 20% cases.
5- Metastasis: local and distant.
Diagnosis:
Examination of the postnasal space by mirror or endoscopy( might be done under GA)Radiological: plain X-ray, CTS, and MRI
Biopsy: under local or general anesthesia
Treatment:
The main treatment is radiotherapy for both the nasopharynx and the neck
Surgery has limited role apart from taking biopsy and neck dissection for metastatic lymph nodes.
Tumors of the Oropharynx
Benign :Papilloma is the commonest; present as a painless warty mass and treated by surgical excision.
Malignant :
1- Squamous cell carcinoma :70%
2- Lymphoma : 25%
3- Salivary gland tumors :5%
Aetiology and incidence :of malignant tumors
Male more than female 5:1
6th and 7th decades
Tobacco and alcohol are the most important aetiological factors.
Other factors include: syphilis, dental sepsis, HPV(types 8 and 16), and premalignant lesions( leucoplakia and erythroplakia)
Pathology:
Site: tongue, palatine tonsil, hard palate and retromolar trigone
Gross appearance: exophytic, fungating or ulcerative lesion could be seen.
Microscopic appearance: squamous cell carcinoma in 75% of cases, with different grades of differentiation.
Spread: 1- direct to surrounding structures
2- lymph nodes: rich lymphatics
3- blood-stream: distant
Clinical features:
1- Sore throat: pain might be severe and radiates into the ear.
2- Dysphagia and odynophagia
3- Cervical lymphadenopathy: neck mass
4- Muffled (hot potato) speech.
5- Distant metastasis
Diagnosis:
1- Examination of the oropharynx: fungating, proliferative or ulcerative
2- Biopsy : under local or general anaesthesia and send for histopathology
3- Radiological: CTS and MRI
Treatment:
Radiotherapy , surgery and chemotherapy alone or in combination depending on the histology and extent of the tumor.Radiotherapy alone is the best choice for early SCC and lymphoma ( with or without chemotherapy)
For more advanced SCC: COMMANDO operation: combined mandibulectomy and oropharyngeal resection, with neck dissection for lymphadenopathy with or without postoperative radiotherapy.

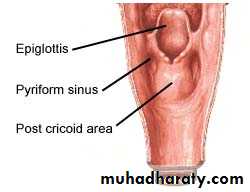
Tumors of the hypopharynx
Benign tumors are very rareMalignant tumors :
SCC is the commonest, in females this is usually in the postcricoid region while in males it is commonly in the pyriform fossa.
Aetiology:
1- Tobacco
2- Alcohol
3- Iron deficiency( Plummer-Vinson syndrome) associated with postcricoid carcinoma.
Clinical features:
1- Sore throat
2- Dysphagia and odynophagia
3- Hoarseness if the tumor extends to the larynx
4- Cevical lymphadenopathy
5- Weight loss in advanced cases
Diagnosis:
1- Examination : mirror or flexible endoscopy2- Radiological : plain lateral soft tissue of the neck might show widening of the prevertebral soft tissue. Also Ba swallow, CTS and MRI.
3- Endoscopy( rigid) and biopsy.
Treatment:
It is mainly surgical with or without radiotherapy for better control .
Surgery is according to the extent of the tumor either partial pharyngectomy or total pharyngectomy with laryngectomy.
Repair of the defect by myocutaneous flap or jejunal flap reconstruction .
Neck dissection for lymph node metastasis.
For more advanced tumors with downward spread into the esophagus , a complete pharyngo-laryngo-esophagectomy is required . Reconstruction is achieved by anastomosing the mobilized stomach to the base of the tongue.