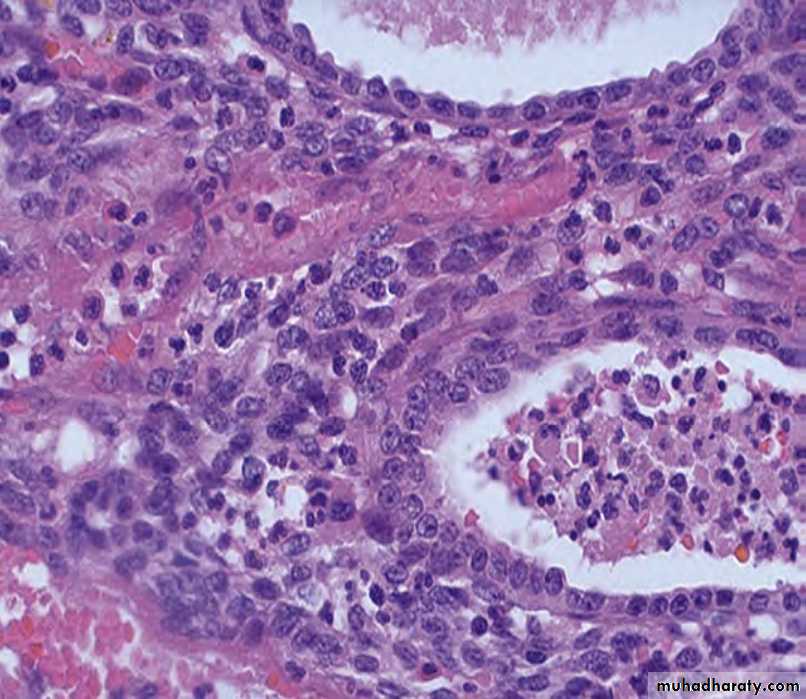
PATHOLOGY OF UTERINE BODY
ENDOMETRITISfever, abdominal pain, menstrual abnormalities, infertility and ectopic pregnancy
Causes:
1-Retained products of conception
subsequent to miscarriage or delivery.
2- foreign body such
as an intrauterine device.
N. gonorrhoeae or C. trachomatis
Chronic Vs acute endometritis
ADENOMYOSIS
Growth of the basal layer of the endometrium down into the myometrium.The uterine wall often becomes thickened and the uterus is enlarged and globular
menorrhagia, dysmenorrhea,
and pelvic pain
before the onset of menstruation.
ENDOMETRIOSIS
characterized by endometrial glands and stroma in a location outside the endomyometrium.
frequently multifocal
Commonly involve tissue in the pelvis
may seen in the umbilicus, lymph nodes, lungs, and even heart, skeletal muscle, or bone.
But How?
1-The regurgitation theory menstrual backflowthrough the fallopian tubes.
2- the metaplastic theory
3- vascular or lymphatic dissemination theory
Morphology:
Grossly : red-blue to yellow-brown nodules or implants. They vary in size from microscopic to 1 to 2 cmThe histologic diagnosis at all sites depends on finding two of the following three features within the lesions:
1-endometrial glands,
2- stroma, or
3- hemosiderin pigment.
endometriosis almost always contains functioning endometrium.
Gross Vs microscopic endometriosis
ABNORMAL UTERINE BLEEDING
Abnormal uterine bleeding include :
Menorrhagia (profuse or prolonged bleeding at the time of the period),
Metrorrhagia (irregular bleeding between the periods), or postmenopausal bleeding.
Common causes include endometrial polyps, leiomyomas, endometrial hyperplasia, endometrial carcinoma, and endometritis.
Dysfunctional uterine bleeding: is an abnormal bleeding from the uterus in the absence of an organic uterine lesion.
Causes of abnormal uterine bleeding
Inadequate luteal phase The corpus luteum may fail to mature normally or may regress prematurely leading to a relative lack of progesterone. The endometrium under these circumstances fails to show the expected secretory changes.Contraceptive-induced bleeding Older oral contraceptives containing synthetic estrogens and progestin induced a variety of endometrial responses, including decidua-like stroma and inactive, nonsecretory glands.
Endomyometrial disorders including chronic endometritis, endometrial polyps, and submucosal leiomyomas.
Failure of ovulation Anovulatory cycles can be due to:
(1) Hypothalamic pituitary axis, adrenal, or thyroid dysfunction;(2) Functional ovarian lesions producing excess estrogen.
(3) Malnutrition, obesity, or debilitating disease
(4) Severe physical or emotional stress.
Endometrial Hyperplasia
Due to an excess of estrogen relative to progestin, if sufficiently prolonged or marked.precursor of endometrial carcinoma.
The severity of hyperplasia is correlated with the level and duration of estrogen excess.
classified based on architectural crowding (simple versus complex) and the presence or absence of cytologic atypia.
The risk of developing carcinoma is related to the presence of cellular atypia.
In time, the hyperplasia may proliferate autonomously, no longer requiring estrogen
Simple hyperplasia Vs complex
Endometrial Carcinoma
One of the most frequent cancer occurring in the female genital tract.the ages of 55 and 65 years.
It comprise two distinct kinds : endometrioid and serous ca,
Endometrioid cancers arise in association with estrogen excess and endometrial hyperplasia in perimenopausal women.
serous cancers arise in the setting of endometrial atrophy in older postmenopausal women.
Endometrioid type
accounts for 80% of cases of endometrial carcinomas.Risk factors
obesity, DM, hypertension,infertility, and exposure to unopposed estrogen.
Mutations in mismatch repair genes and PTEN gene are early events in the stepwise development of endometrioid carcinoma.
TP53 mutations occur but are relatively uncommon
They include a range of histologic types, including those showing mucinous, tubal (ciliated), and squamous differentiation
The serous type endometrial carcinoma
less common,accounting for roughly 15% of tumors.
Nearly all cases have mutations in the TP53 tumor suppressor gene
mutations in DNA mismatch repair genes and PTEN are rare.
form small tufts and papillae.
exhibit much greater cytologic atypia.
behave aggressively.
Endometrial Polyps
sessile lesions
range from 0.5 to 3 cm in diameter.
Larger polyps may project from the endometrial mucosa into the uterine cavity.
Microscopy composed of endometrium resembling the basalis, with small muscular arteries.
The glands more often are cystically dilated.
commonly are detected around menopause.
Leiomyoma
the most common benign tumor in females.these tumors are monoclonal and are associated with several different recurrent chromosomal abnormalities, including rearrangements of chromosomes 6 and 12.
Estrogens and possibly oral contraceptives stimulate the growth of leiomyomas; these tumors shrink postmenopausally.
are typically sharply circumscribed,
firm gray-white masses with a characteristic whorled cut surface.
Microscopy :the tumors are characterized by bundles of smooth muscle cells mimicking the appearance of normal myometrium. Foci of fibrosis, calcification, and degenerative softening may be present.
Leiomyoma
LeiomyosarcomaAlmost always solitary and most often occur in postmenopausal women
soft, hemorrhagic, necrotic masses
The diagnostic features of overt leiomyosarcoma include tumor necrosis, cytologic atypia, and mitotic activity