


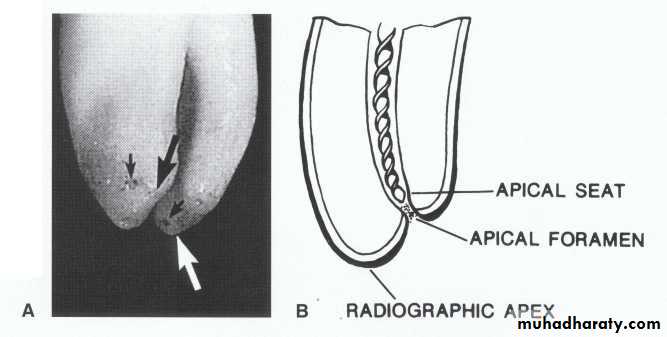
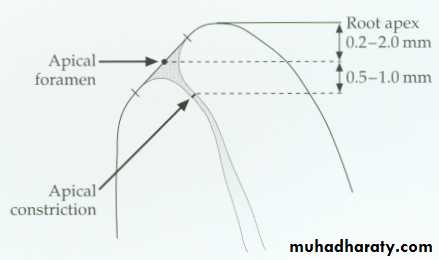
The average distance between the apical foramen and the
most apical part of the root is 0.2-2.0 mm. The constrictioncan be 0.5-1.0 mm from the apical foramen.
Anatomical situation for the anterior teeth
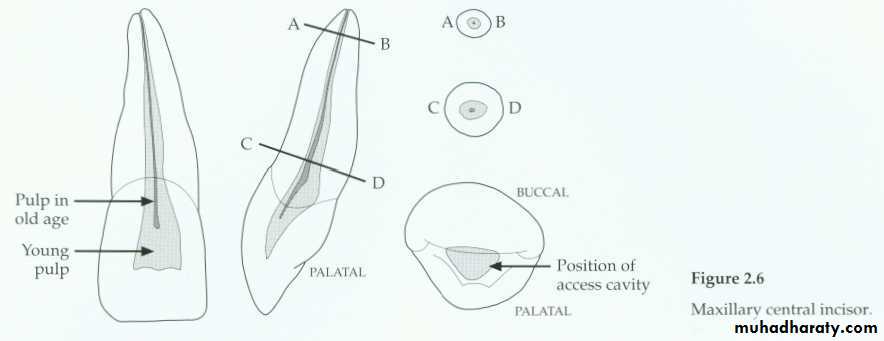
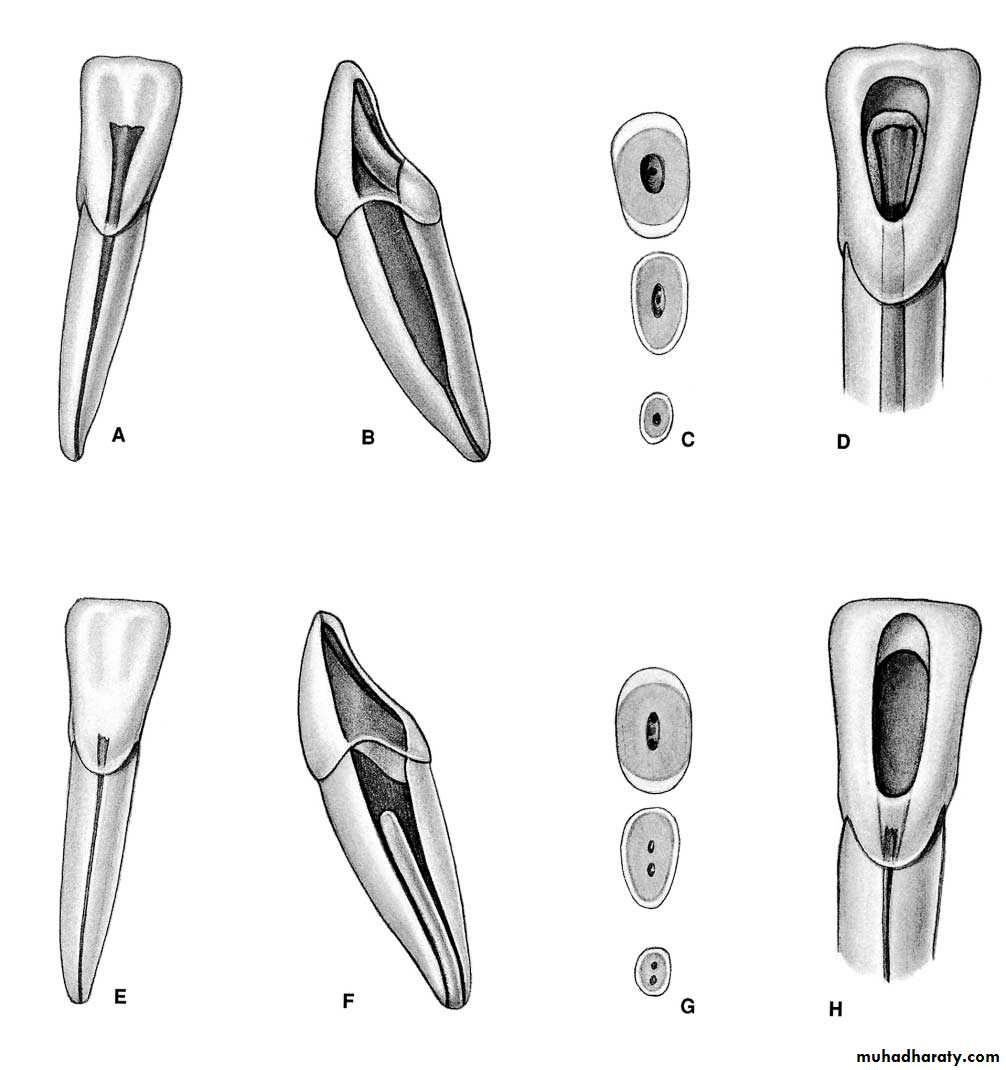
Max. central incisor
Mesial-axial inclination of the toothdistal
Single root-type I canal configurationCanal shape: Simple, large, conical, tapered toward the apex and the Pulp chamber gradually merging into the root canal.Slightly triangular or oval in shape at the cervical area of the root and tend to be round at the apical portion.
Apical foramen exists short of the apex to the labial direction.Average length:22mmIf the lingual shoulder not cut during access opening, it will lead to obstructed line during canal preparation.
Multiple canals are very rare; incidence of accessory & lateral canals is high.
young
oldApical-distal curvature
Beveld extension toward the incisal
distal

Notch in the middle of the incisal extent of the access. This notch allows more straight-line access for instruments and greatly helps eliminate cervical flexure that can cause "unexplained" instrument
breakage.
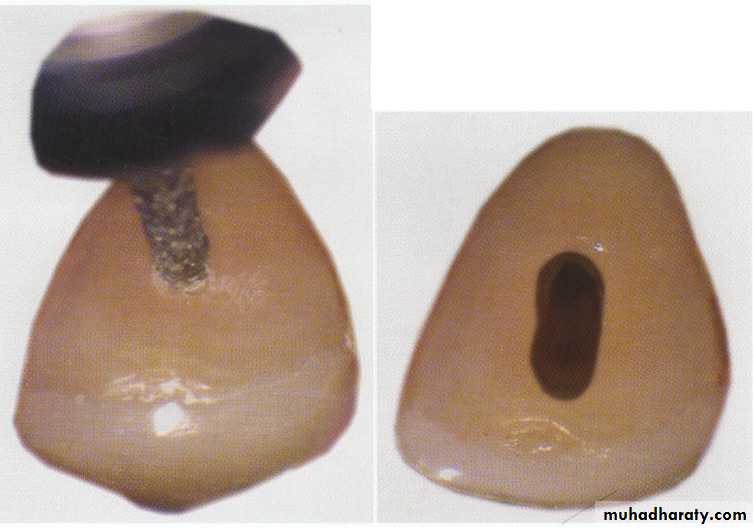
Access opening shape in the central & lateral are triangular
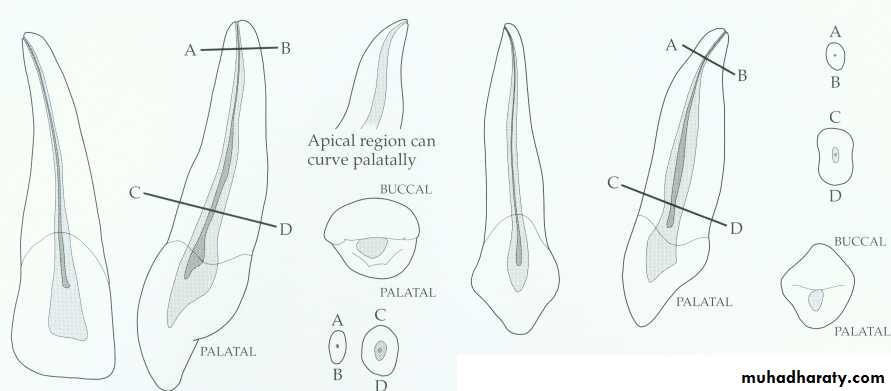
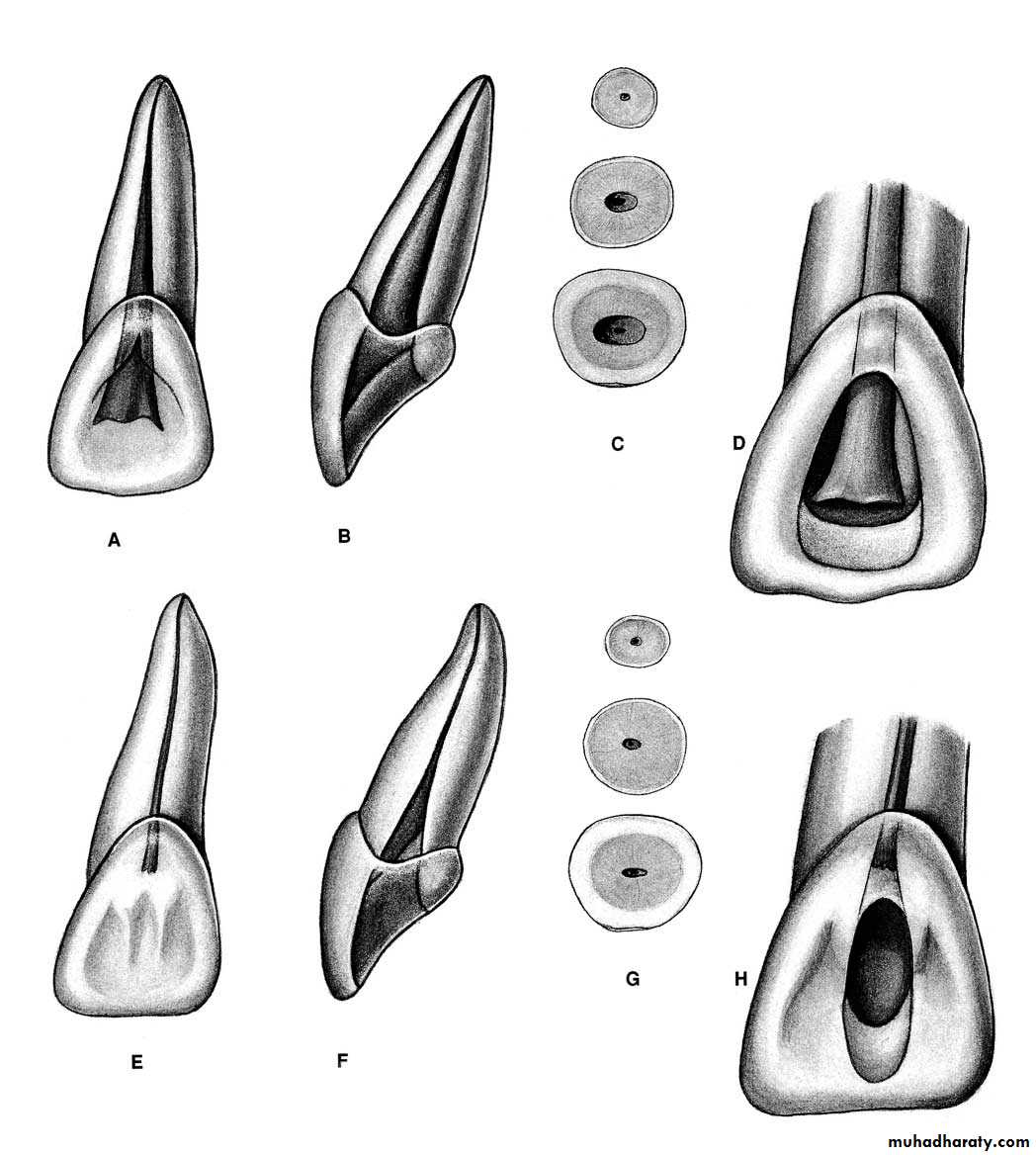
Maxillary lateral incisor.
• The long axis of crown not with the long axis of root so the direction of the access opening slightly distally to reach the pulp chamber.Single root-type I canal configurationCanal shape: Simple out line, conical in the apical third with pronounced constriction, narrower in diameter than central incisor,
most of them have curvature in the root disto-palataly (perforation or ledge formation)→ (small, flexible instrument with filing action not reaming action.
Oval at cervical area, round apicallyPulp chamber: Tend to be gradually merging to root canal, smaller than that for max. central.Average length 23mm
The main canal has pronounced constriction and curvature in the apical third which follow the curvature of the root in the apical. The importance of this curvature: the large non flexible size instruments should be avoided in the preparation of such canal,
because if such instruments used this will lead to either perforation or ledge formation. This critical situation curvature could be avoided through limiting the apical preparation to flexible sizes up to 25 and the use of
precurved instruments in case of using stainless steel instruments or we can use NiTi flex files also we have K-flex files. In addition to those 2 points, we should do thorough irrigation (very important).
The long axis of crown not with the long axis of root so the direction of the access opening slightly distally to reach the pulp chamber.
A curved canal is enlarged by alternate reaming and filing with copious irrigation
youngold
Maxillary canine.
Apical-distal curvatureThe longest tooth in the dental arch. Root slender from labial, bulky proximally.Canal shape: Huge ovoid pulp, wider labio-palatally than mesiodistally Mostly apical curvature in the root→
follow the previously mentioned points to overcome apical curvature of lateral incisor. Pulp chamber: Gradually margining with the root canal. The canal is conical at the apical third and wider in the middle and coronal part.Average length 27 mm
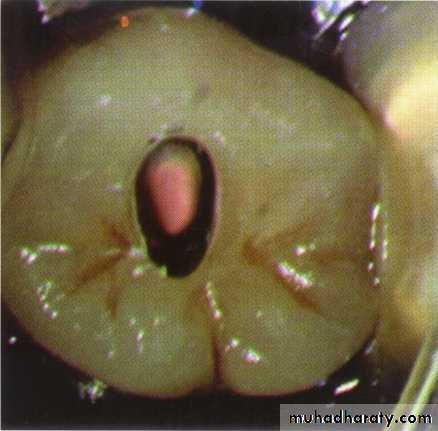
Access opening shape is oval in the canine while in the lateral or central the shape is triangular
Access opening shape in the canine is oval
Narrow mesio-distal widthLarge labio-lingually width
Distal-axial inclination of the tooth
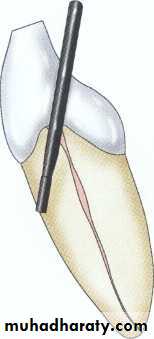
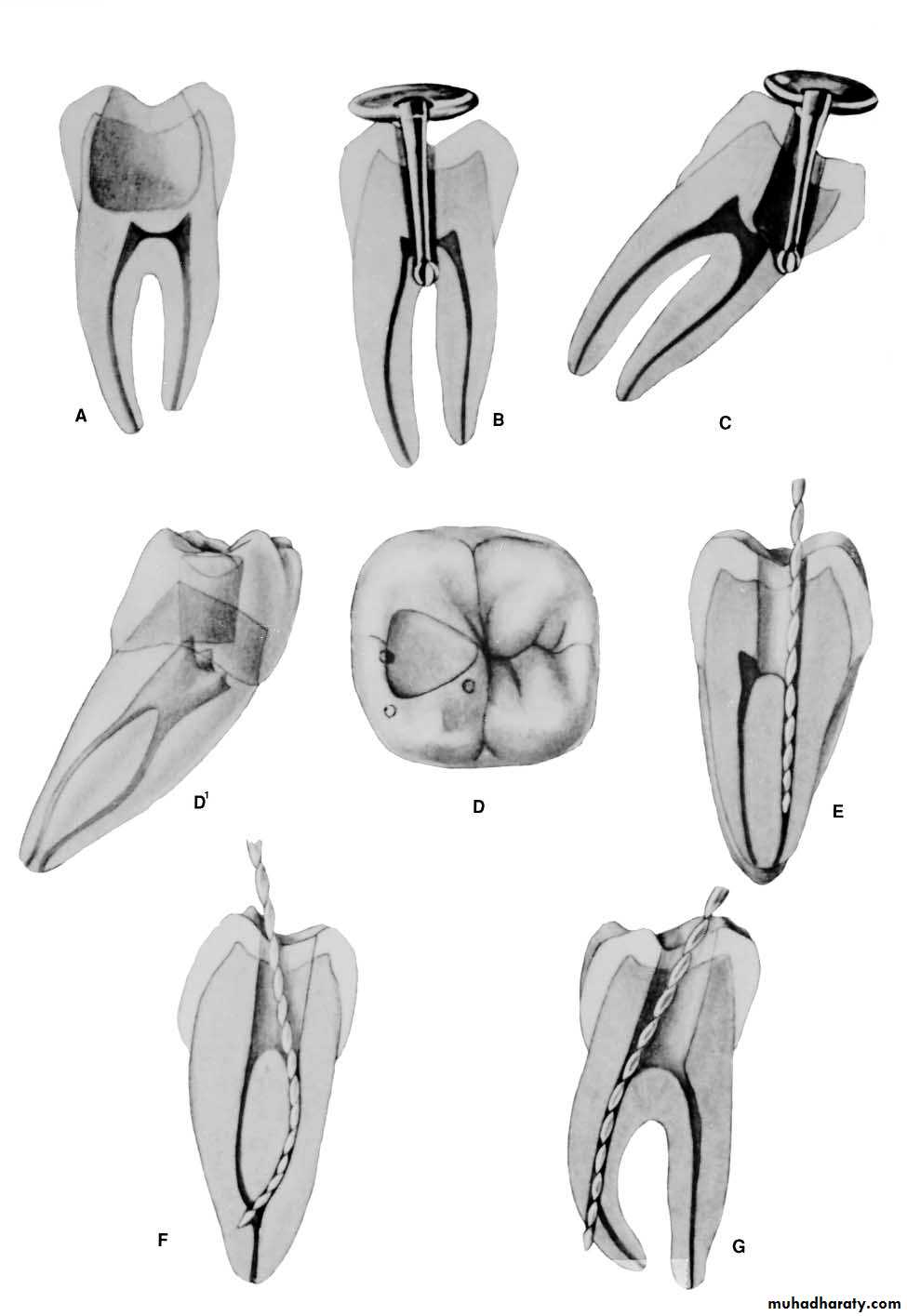
A, Initial access penetration occurs in the middle of the incisal-cervical dimension.
B, After locating the canal, the clinician extends the access incisally.
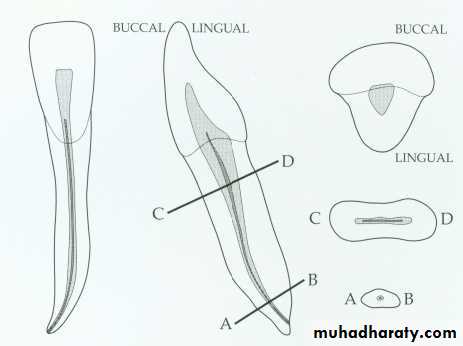
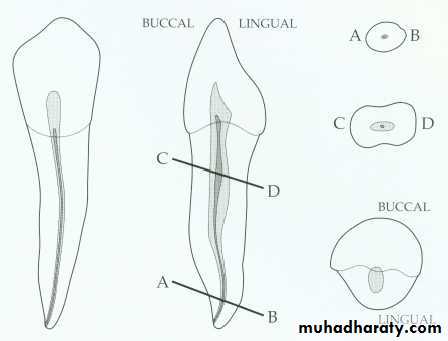
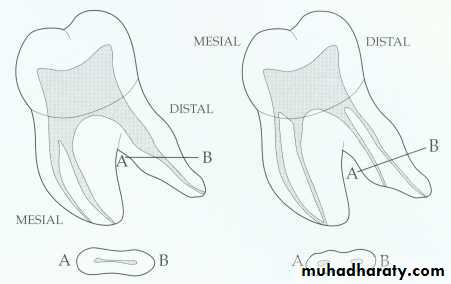
Mandibular incisors.

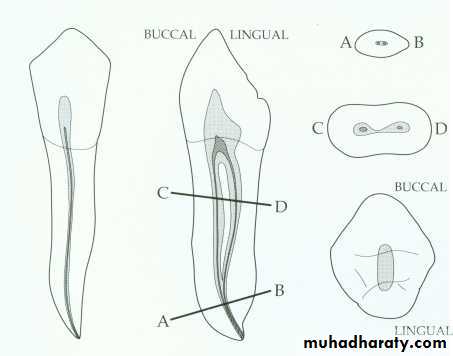
Mandibular incisor canal configurations.
*slight apical-distal curvature of the canal.*20 degree lingual-axial angulation of the tooth.* 30% presence of bifurcation of pulp into the labial &lingual canals* Axial inclination of the root calls for careful orientation &alignment of the bur to prevent gouging.*smaller canal orifices are more difficult to find.*labial & lingual canals are discovered by exploration with a fine curved file to both labial and lingual.
How you suspect 2 canals in preoperative radiograph: The pulp chamber merge gradually into the canal these constriction gradually occur in the x-ray with continuous tapering mean one canal but when there is narrow line of the root we suspect 2 canals then take other x-ray with little angulations.

incisor with two canals
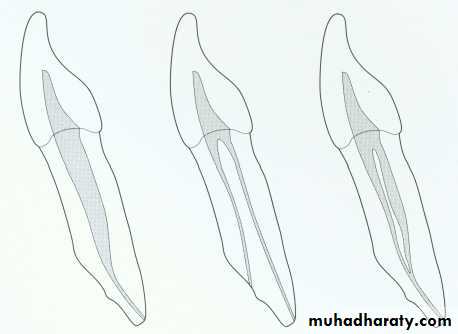
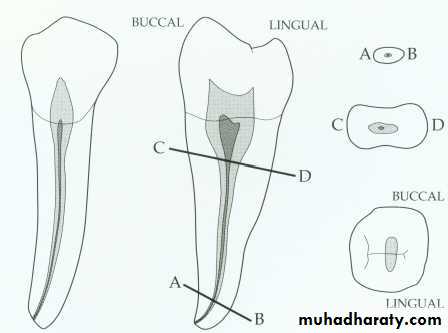
Mandibular canine.
Mandibular canine:Canal shape: The canal is somewhat ovoid at the cervical portion, round at the apical portion, narrow mesiodistally, apical labial curvature is present.Pulp camber: Gradually merging with root canal, average length: 23mm.Possibility of 2 canal7% one root-two canals5% two separate roots with two separated canals.

Access openings for the mandibular canine.
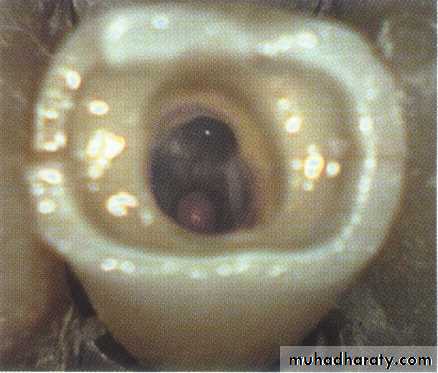
Root canal access: it is the initial step toward canal preparation.Why we remove the pulp contents: to remove the infected & necrotic materials in the pulp & to avoid the discoloration of the tooth.Access to ant teeth:Entrance is always gained through lingual surface of all ant. teeth just in the exact center of the tooth and just below the cingulum.Round bur No. 4 operated at right angle to long axis of the tooth, only the enamel is penetrated, once the head of the bur hidden in the tooth structure, stop drilling.
Switch the bur to be parallel to the long axis, keep drilling until entrance to pulp chamber is gained.Remove the pulp chamber roof working from inside the chamber to the outside (pulling motion) to eliminate the remnant of roof of pulp chamber.
Lingual shoulder is removed (working from inside to the outside) introduce the round bur just behind the shoulder to give continuous smooth flowing preparation then the entire tooth chamber is rounded then funneling is done of the canal outward.Finishing and funneling with fissure bur, final shape, funnels down toward the orifice of the canal flare outward.
pulp horns should be eliminated, a round bur No. 2 used laterally and incisally to eliminate necrotic tissues which may cause discoloration.
*extirpation of the pulp content using barbed broach.*Irrigation of the pulp chamber and the root canal
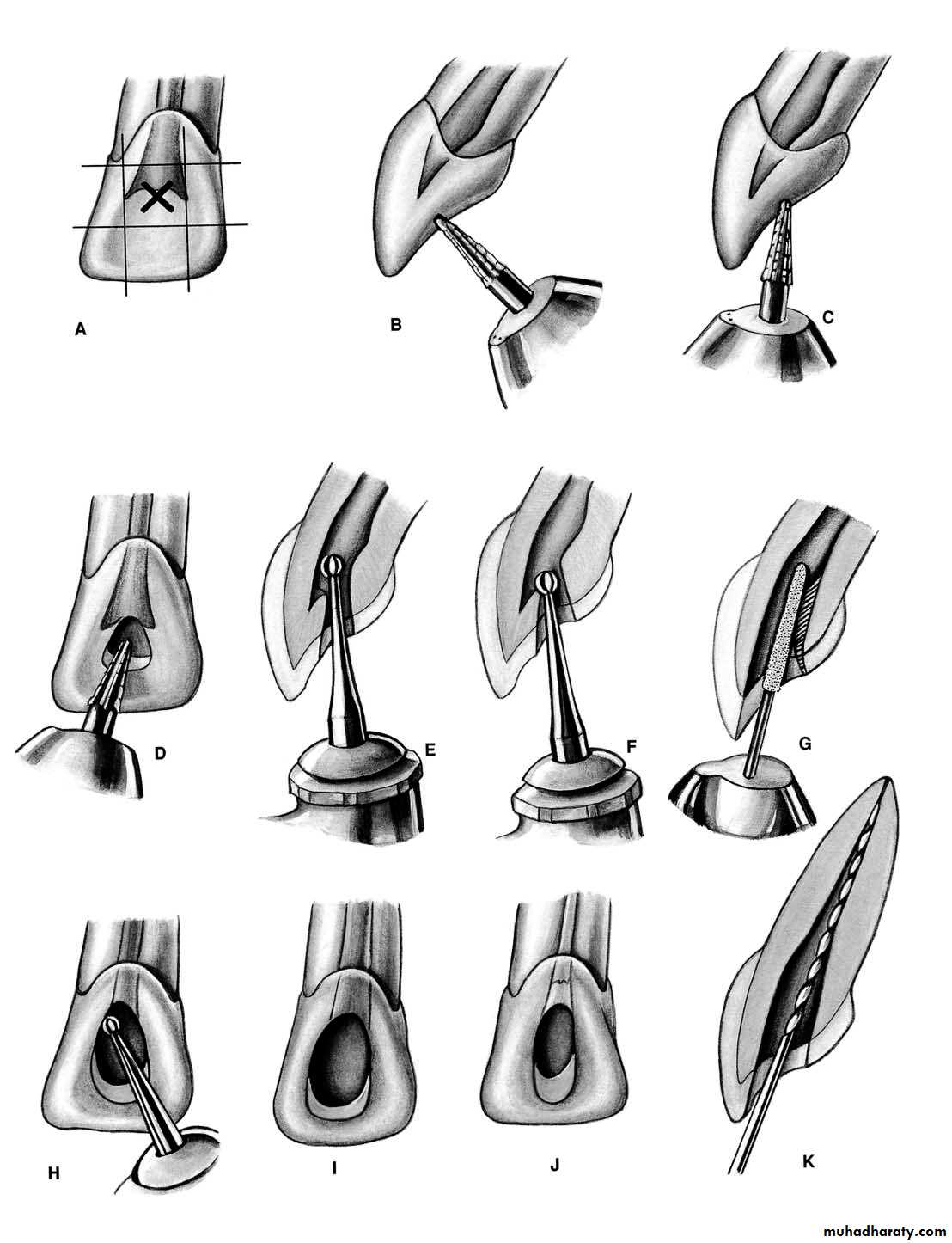
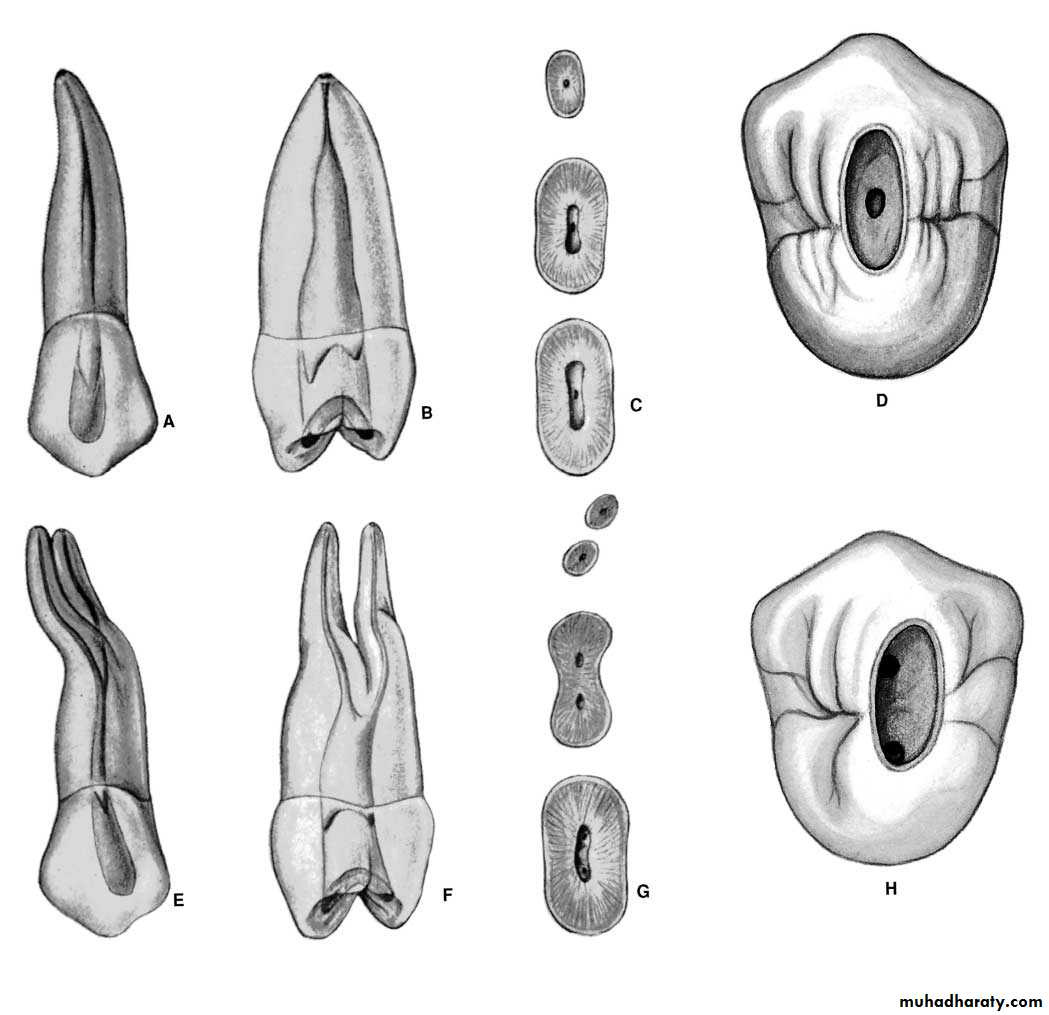
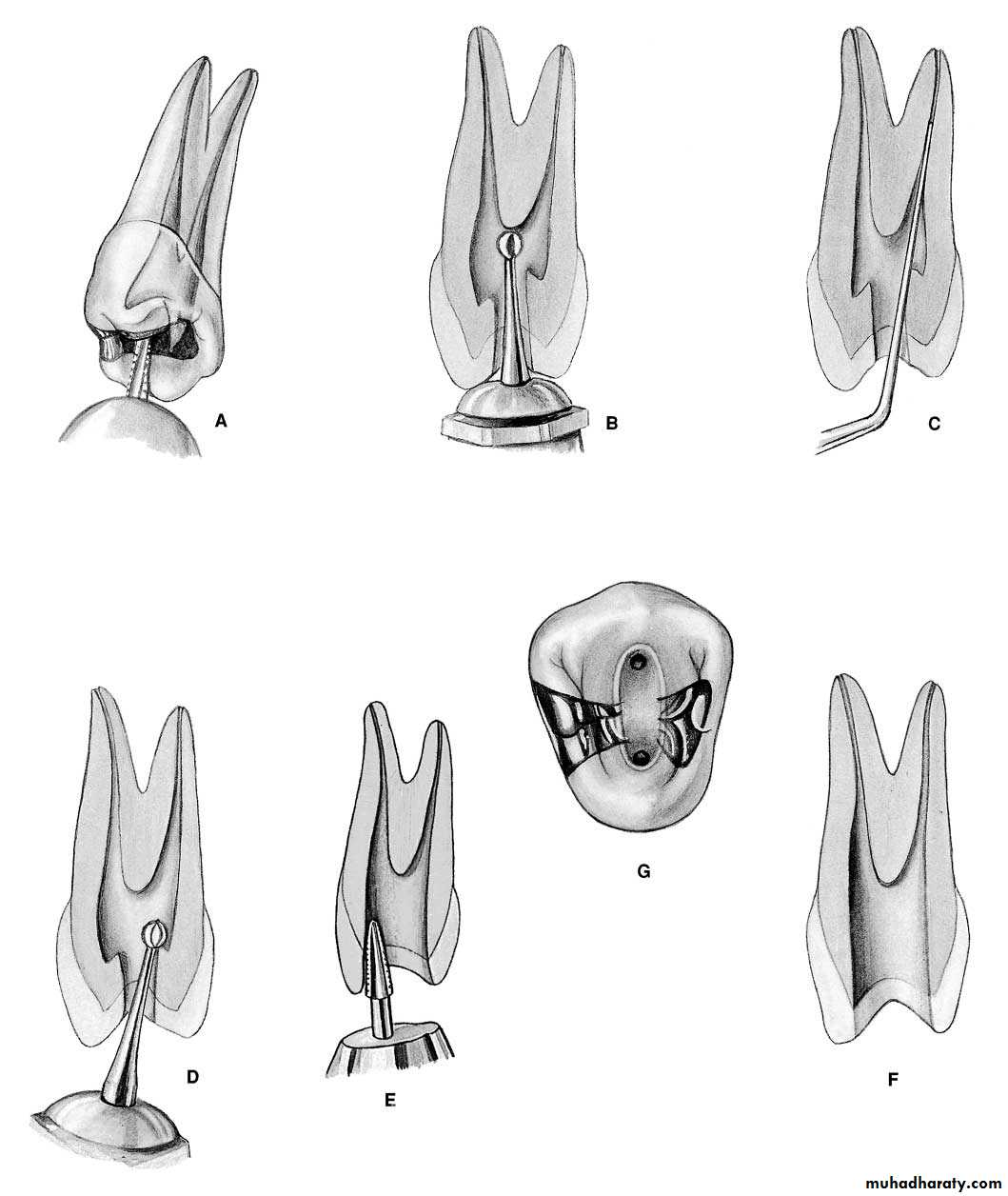
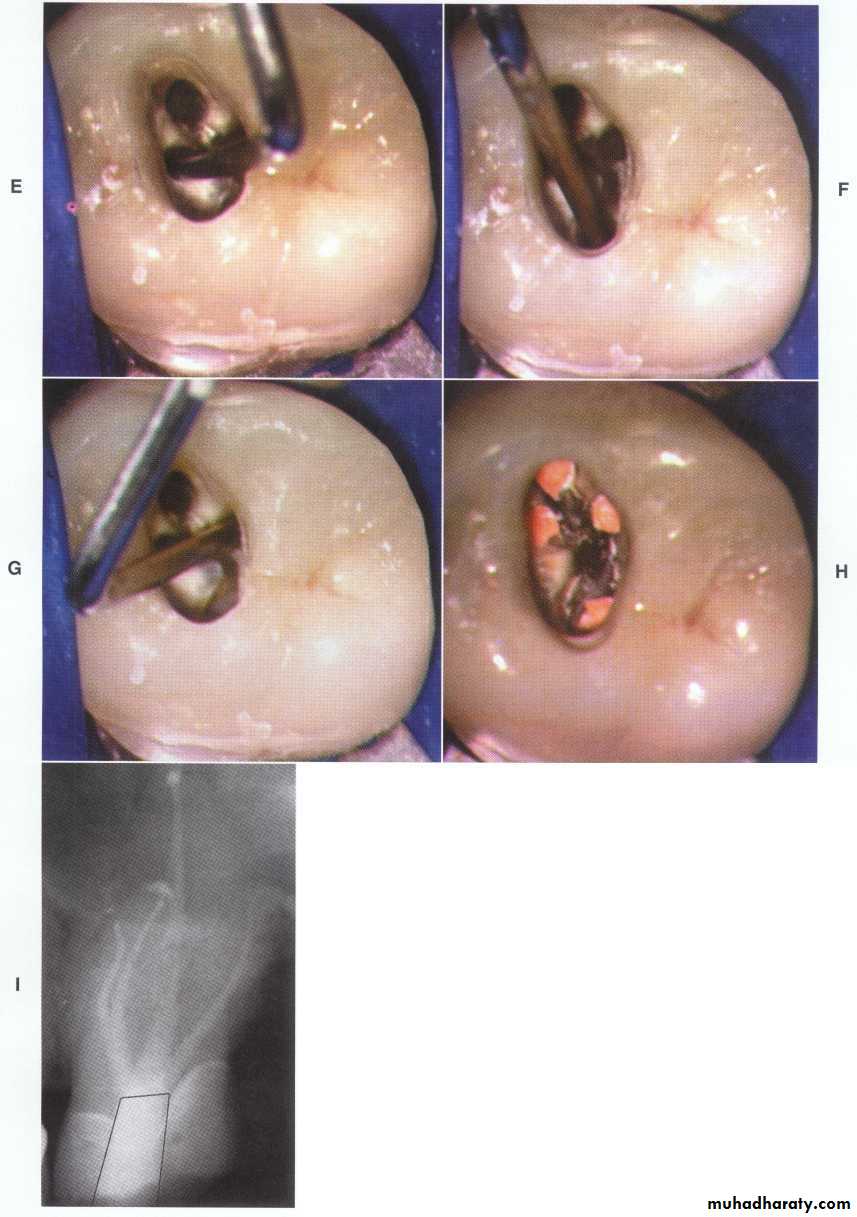
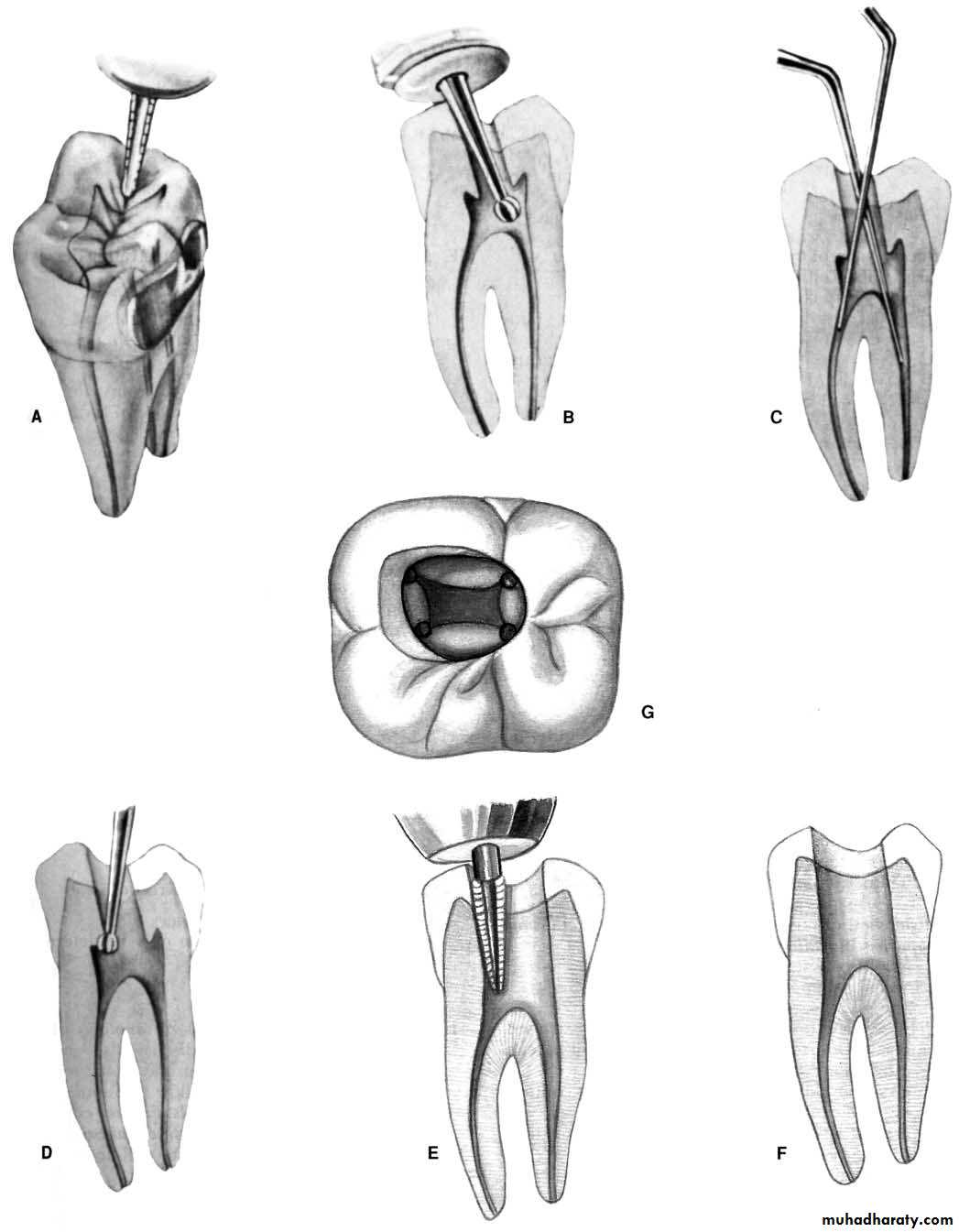
Error in access opening in max. ant teethA.PERFORATION: at the labiocervical caused by failure to complete convenience extension toward the incisal, prior to the entrance of the shaft of the bur.B.GOUGING: of the labial wall caused by failure torecognize the 29-degree lingual-axial angulation of the tooth.
C. GOUGING: of the distal wall caused by failure to recognize the 16-degree mesial-axial inclination of the tooth. D.PEAR-SHAPED PREPARATION: of the apical canal caused by failure to complete convenience extensions. The shaft of the instrument rides on the cavity margin and lingual “shoulder.” Inadequate débridement and obturation ensure failure.
E.DISCOLORATION: of the crown caused by failure to remove pulp debris. The access cavity is too far to the gingival with no incisal extension.F. LEDGE: formation at the apical-distal curve caused by using an uncurved instrument too large for the canal. The cavity is adequate.
G.PERFORATION: at the apical-distal curve caused by using too large an instrument through an inadequate preparation placed too far gingivally. H.LEDGE: formation at the apical-labial curve caused by failure to complete the convenience extension. The shaft of the instrument rides on the cavity margin and “shoulder.”
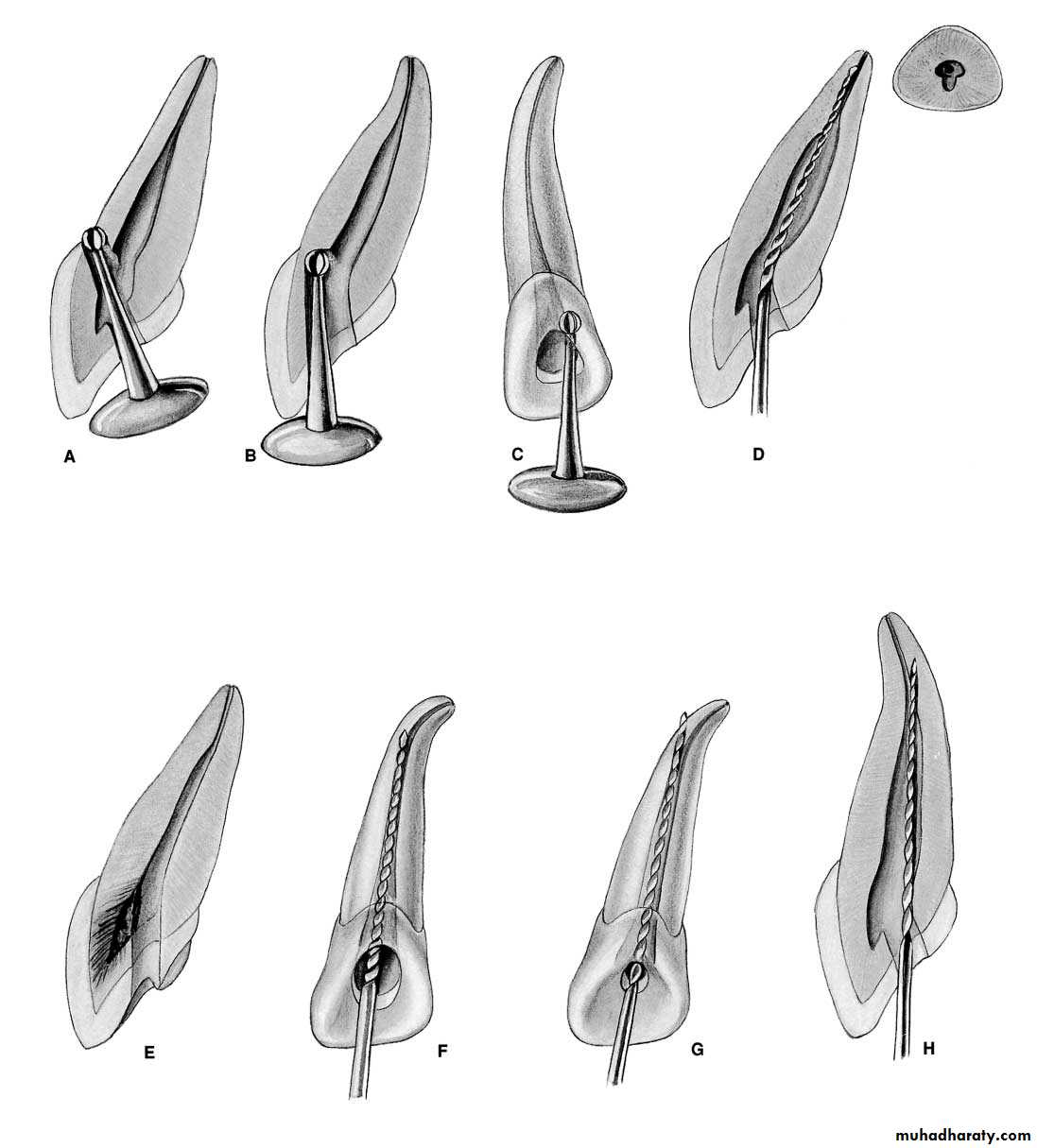
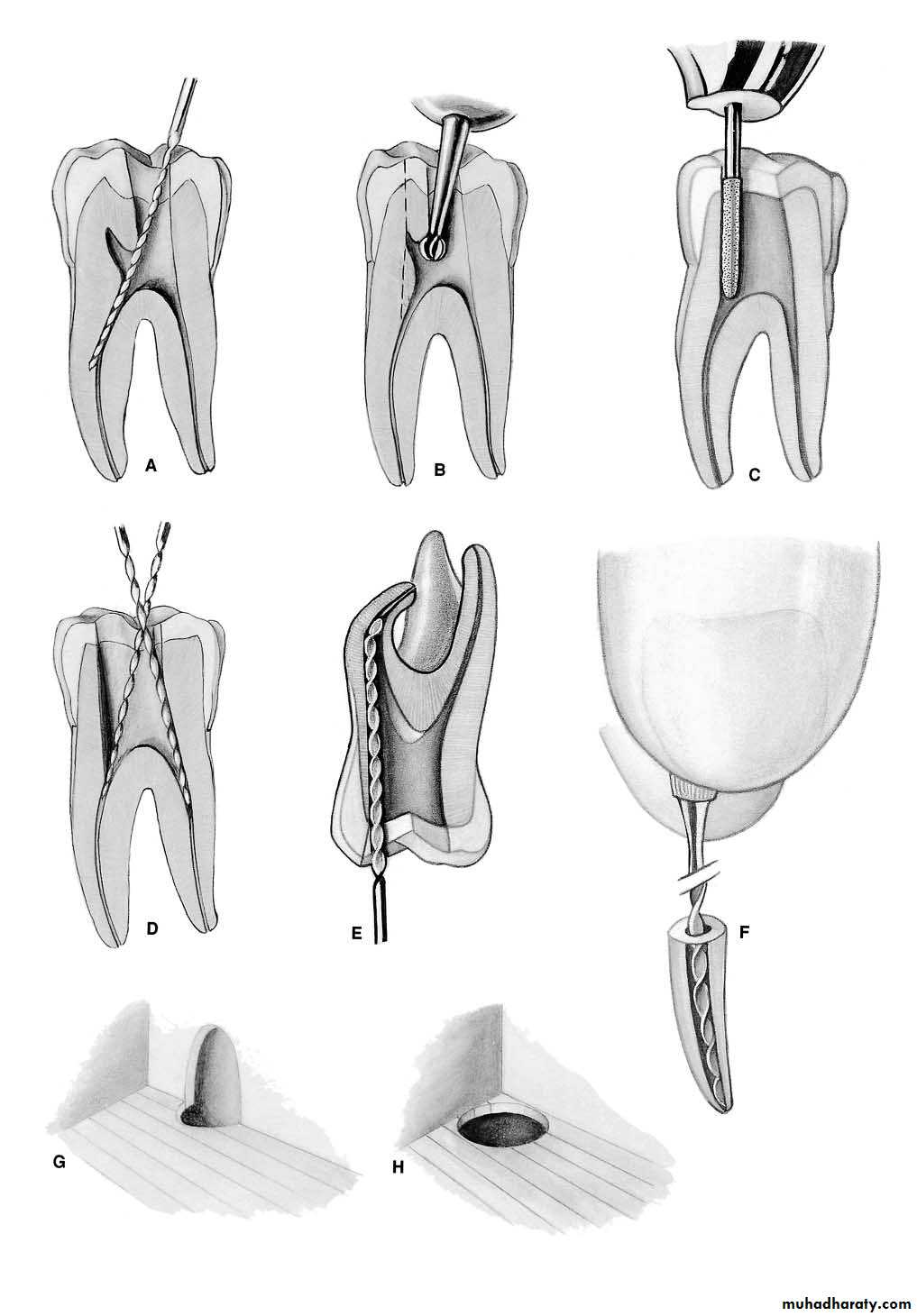
Error in access opening in man. ant. teeth
A.GOUGING: at the labiocervical caused by failure to complete convenience extension toward the incisal prior to entrance of the shaft of the bur. B.GOUGING: of the labial wall caused by failure to recognize the 20-degree lingual-axial angulation of the tooth.
C.GOUGING: of the distal wall caused by failure to recognize the 17-degree mesial-axial angulation of the tooth.D.FAILURE to explore: débride, or fill the second canal caused by inadequate incisogingival extension of the access cavity.
E. DISCOLORATION: of the crown caused by failure to remove pulp debris. The access cavity is too far to the gingival with no incisal extension. F.LEDGE: formation caused by complete loss of control of the instrument passing through the access cavity prepared in proximal restoration.
Anatomical situations for posterior teeth
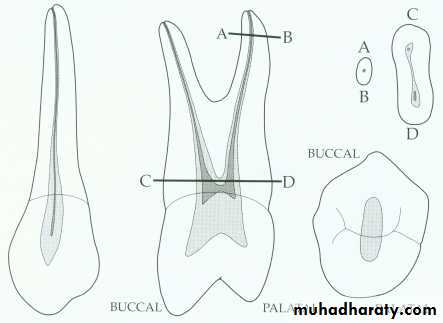
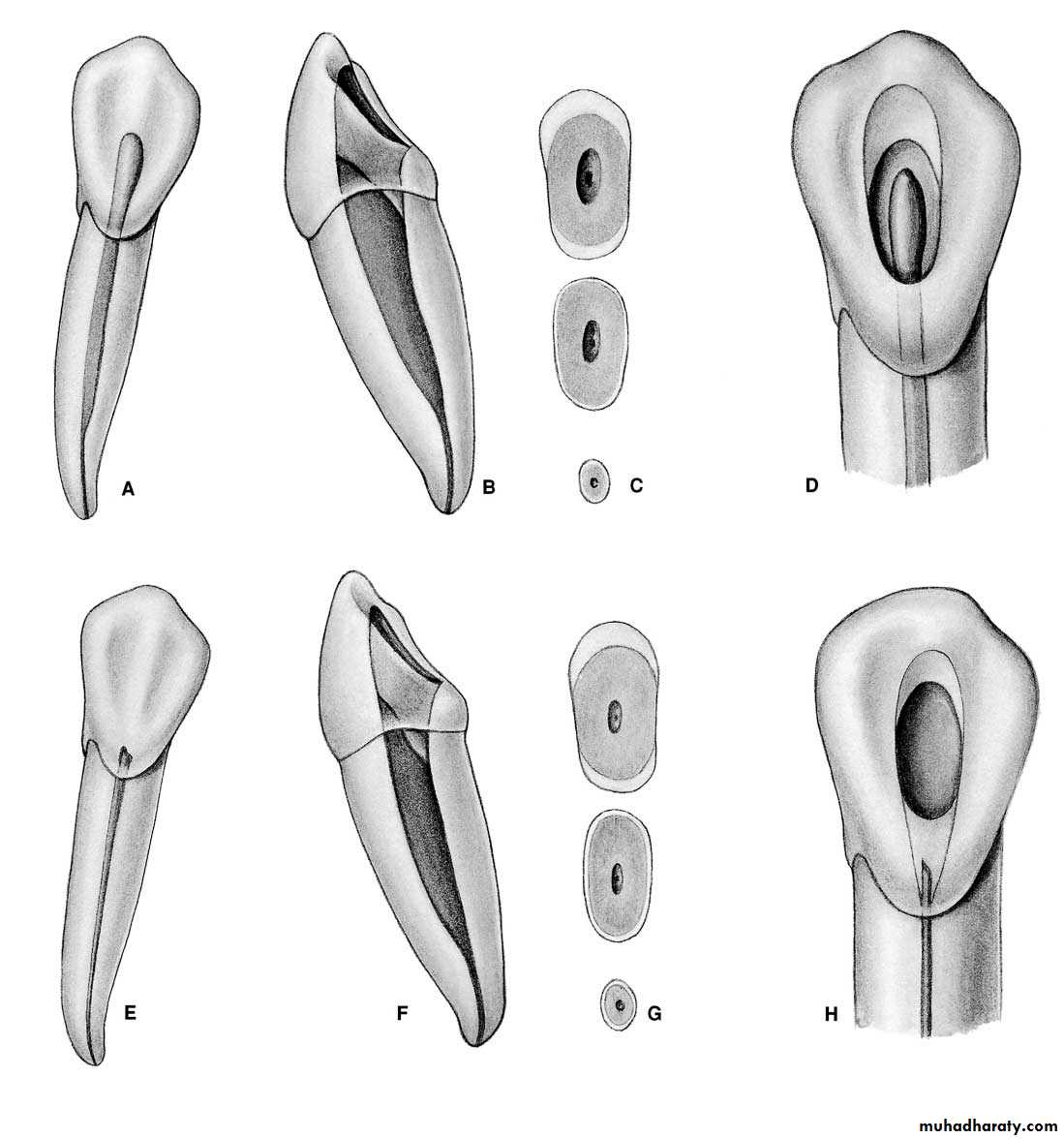
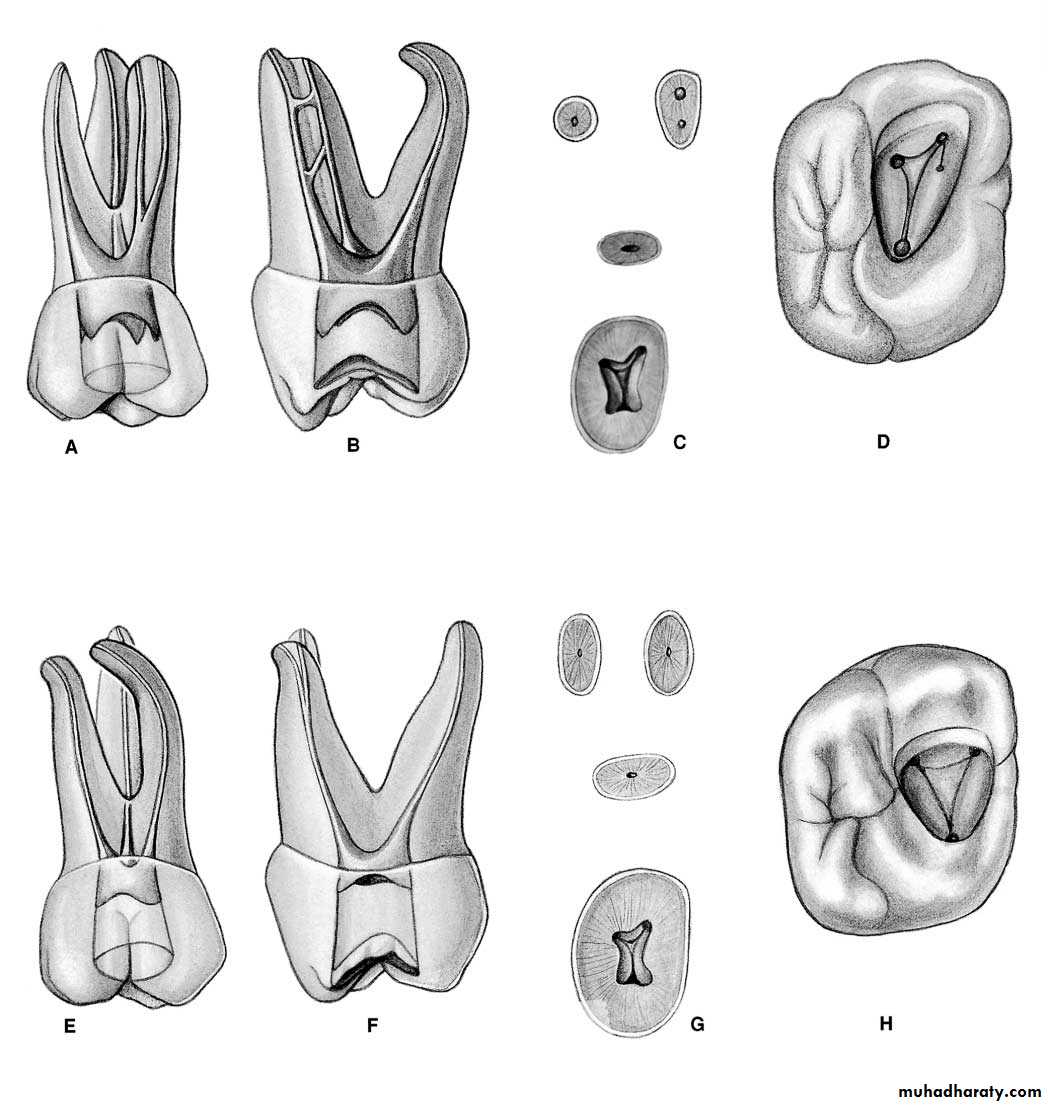
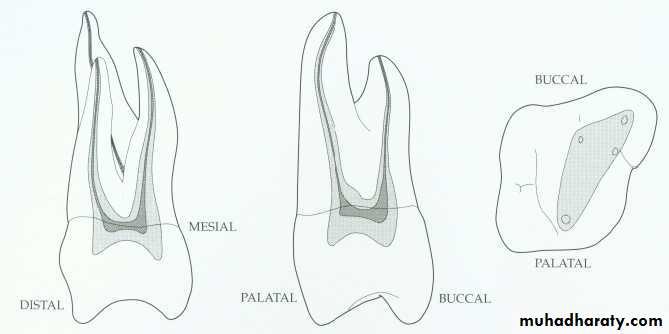
Maxillary first premolar.
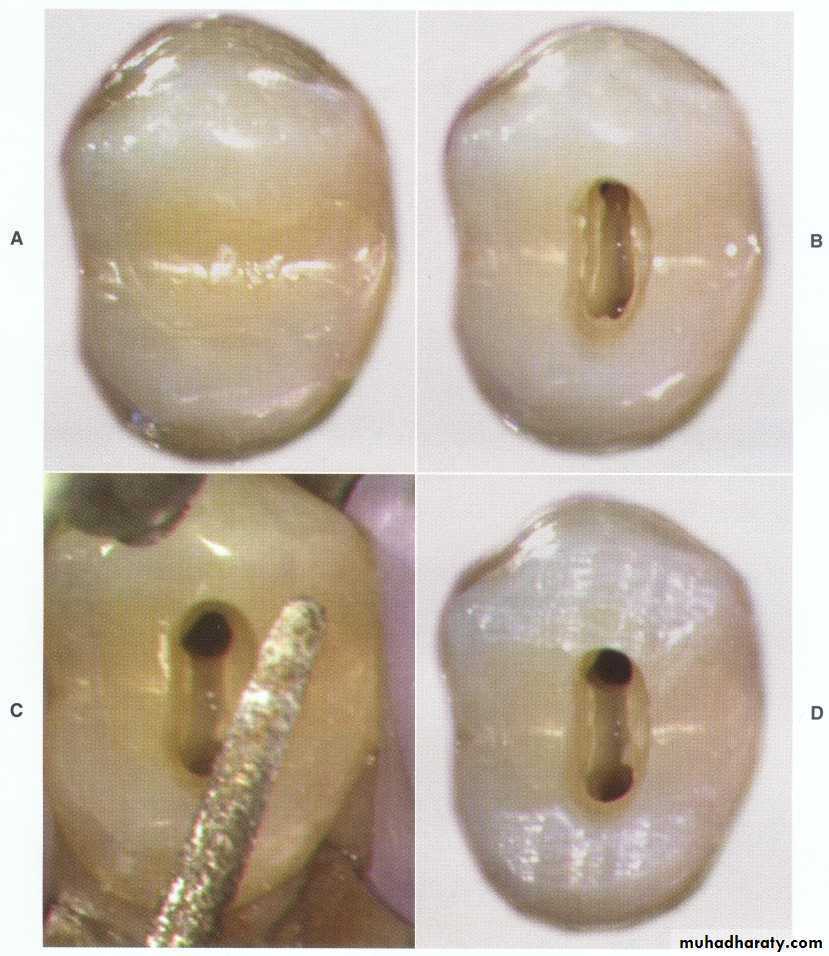
• Access opening ovoid, elongated bucco-palatally.
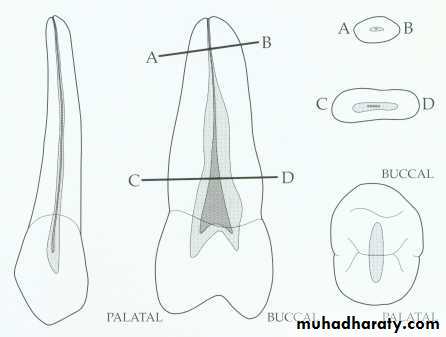
Maxillary 1st premolar:Canal shape: Wide in bucco-palatal direction, ovoid at mid-root, round at apical third.Canal orifice: Below and slightly central to cusps tips.Pulp horns: Should not be confused with true root canal orifice.
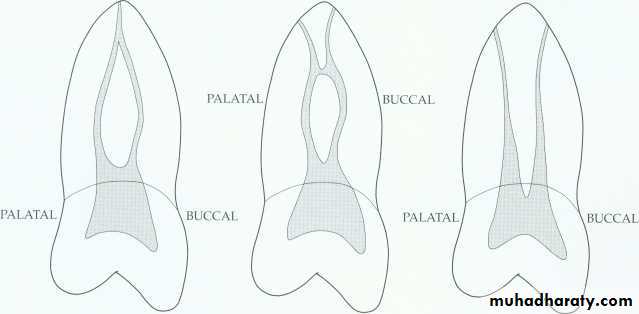
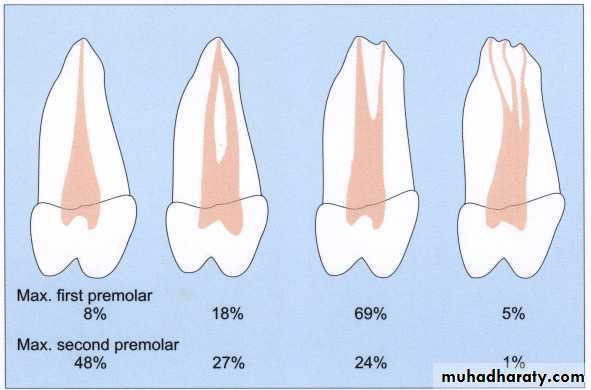
Access opening ovoid, elongated bucco-palatally.Multiple canal possibilities:20% single canal in single root, elliptical or figure 8 in shape, wider buccopalatally than mesiodistally, mistaken as two canals (sudden narrowing).
80% two canals, either single root with either one or two apical foramen or 2 separated roots (palatal larger)Average length: 21.5mmRarely 3 roots and 3 canals.
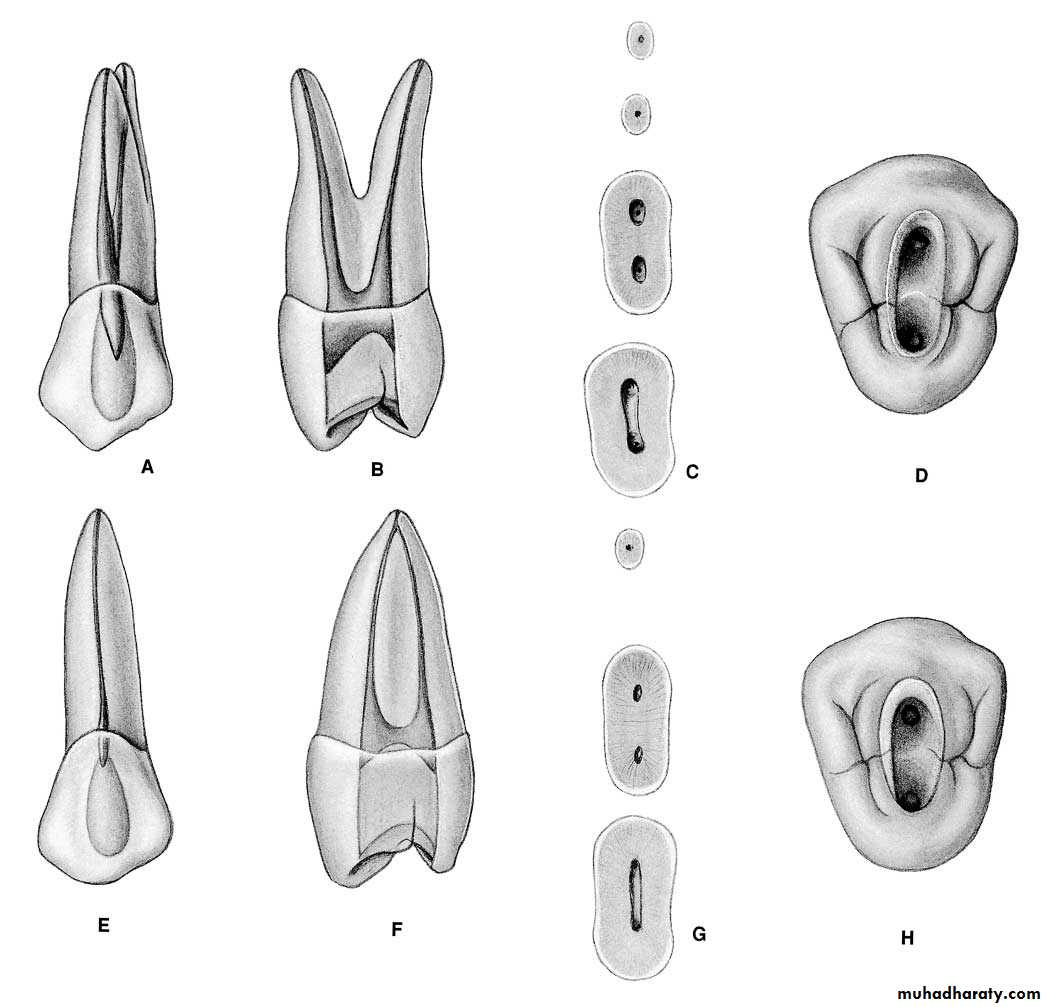
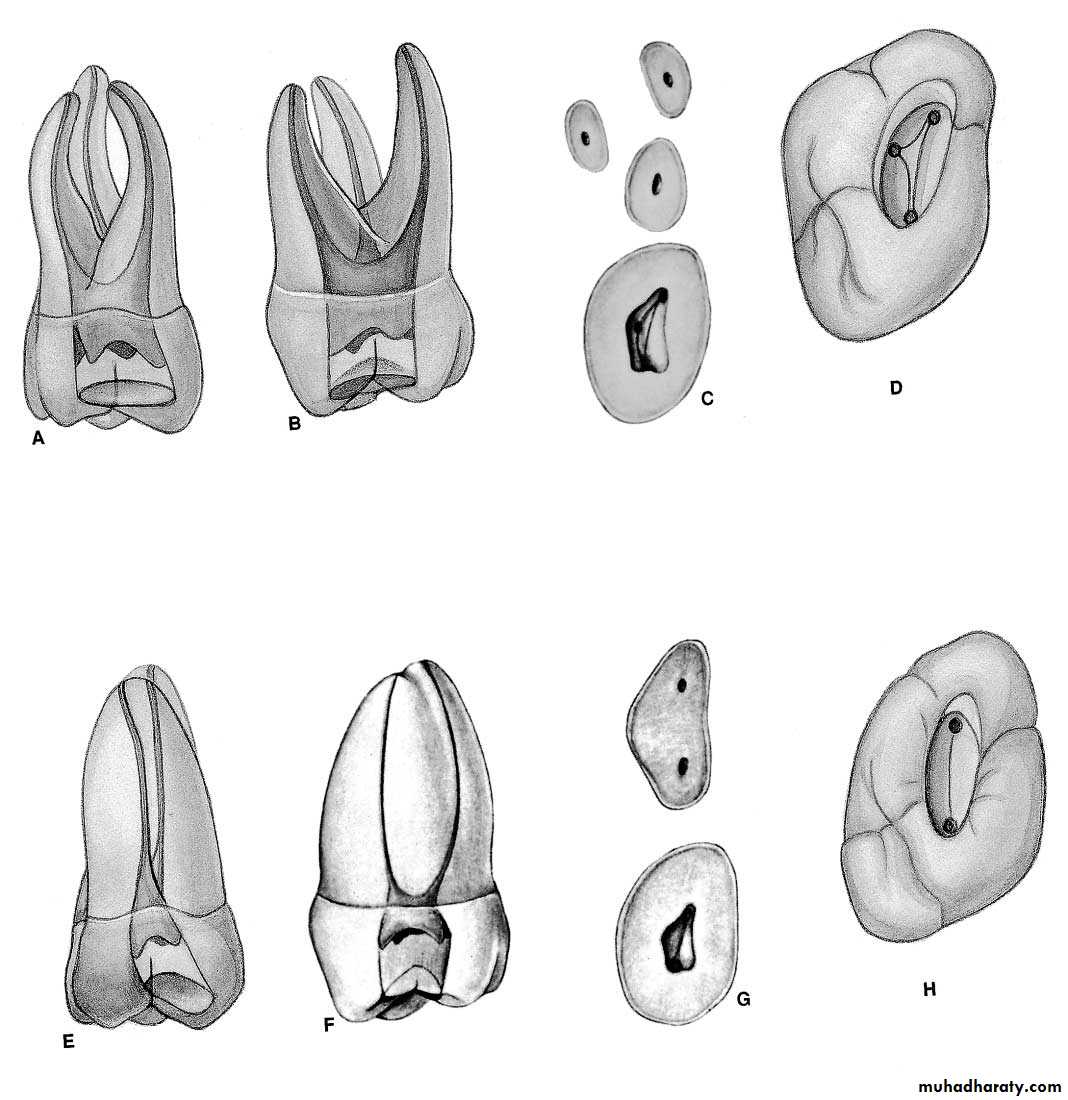
Maxillary second premolar.
Maxillary 2nd premolar: Mostly single rootCanal shape: Single canal, enormous and very wide cervical portion in bucco-palatal direction, mid root ovoid, apical round.Canal orifice: centrally located and often appears as a slot than as a single ovoid opening.Access opening: Ovoid, accessory and lateral canal common.Multiple canals possibilities: 40% 2 canals, 60% one canal, average length:21.5mm.
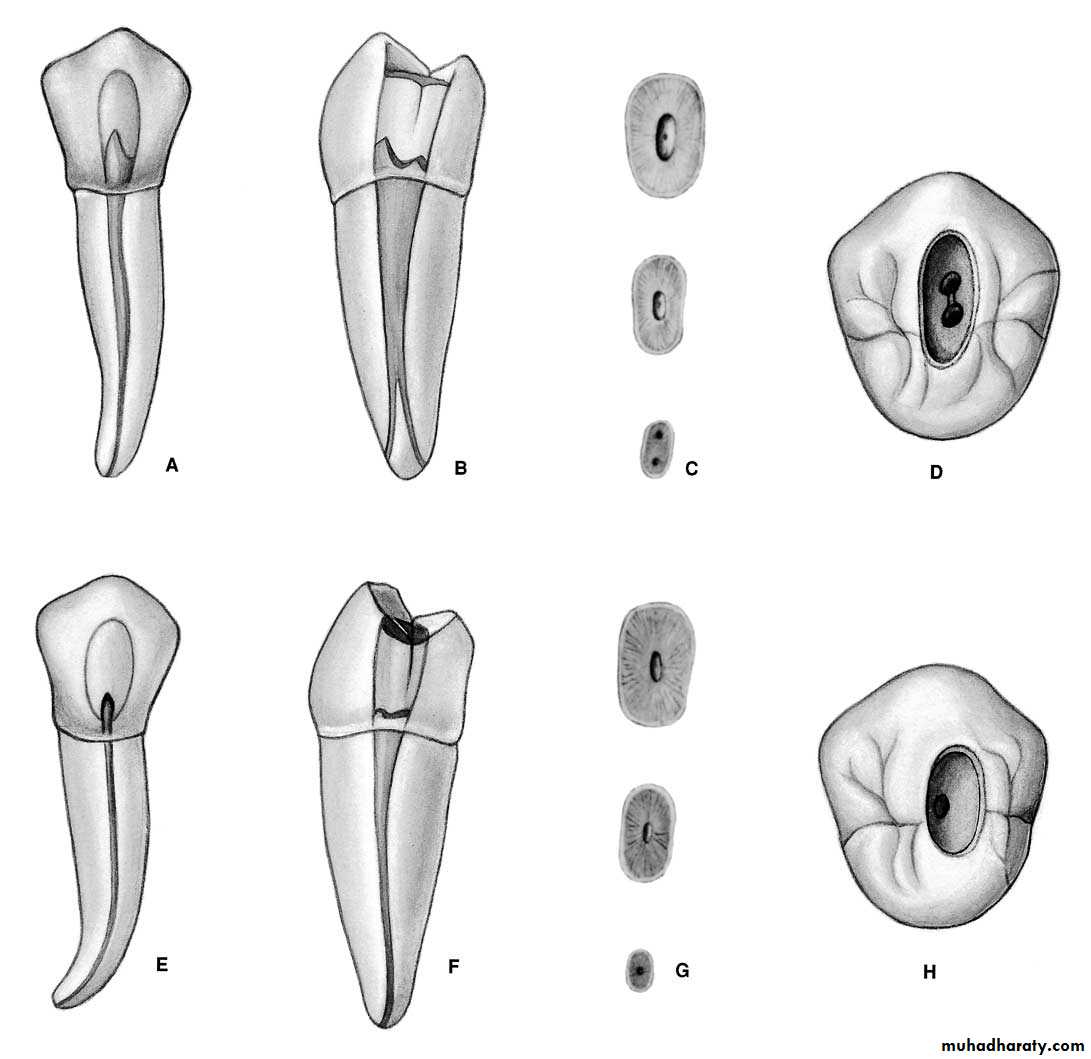
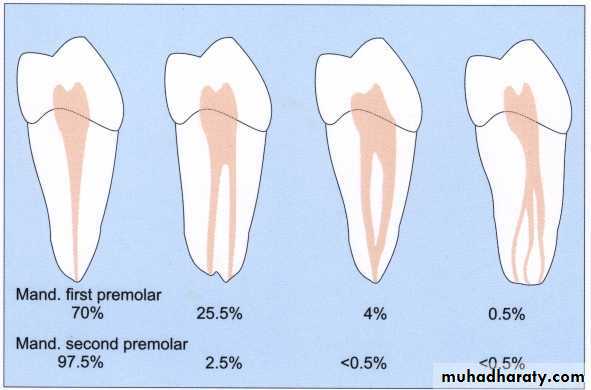
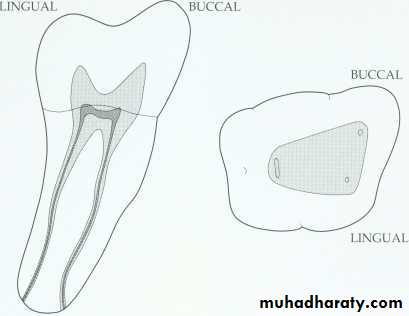
Mandibular first premolar.
Mandibular 1st premolar:Well developed buccal cusp and a small lingual cusp, the root is more rounded than 2nd premolar and shorter.Pulp chamber: Ovoid, buccal pulp horn higher.Canal shape: At cervical level, wide in bucco-lingual dimension, mid root continues ovoid, apical third round.Possibility of 2 canals is not uncommon, access opening, ovoid. Access made slightly buccally to the central groove. Because the tooth inclines
lingually so we might end up with lingual perforation at the neck if we keep drilling lingually and so removing unnecessary tooth structure.Average length: 21mm
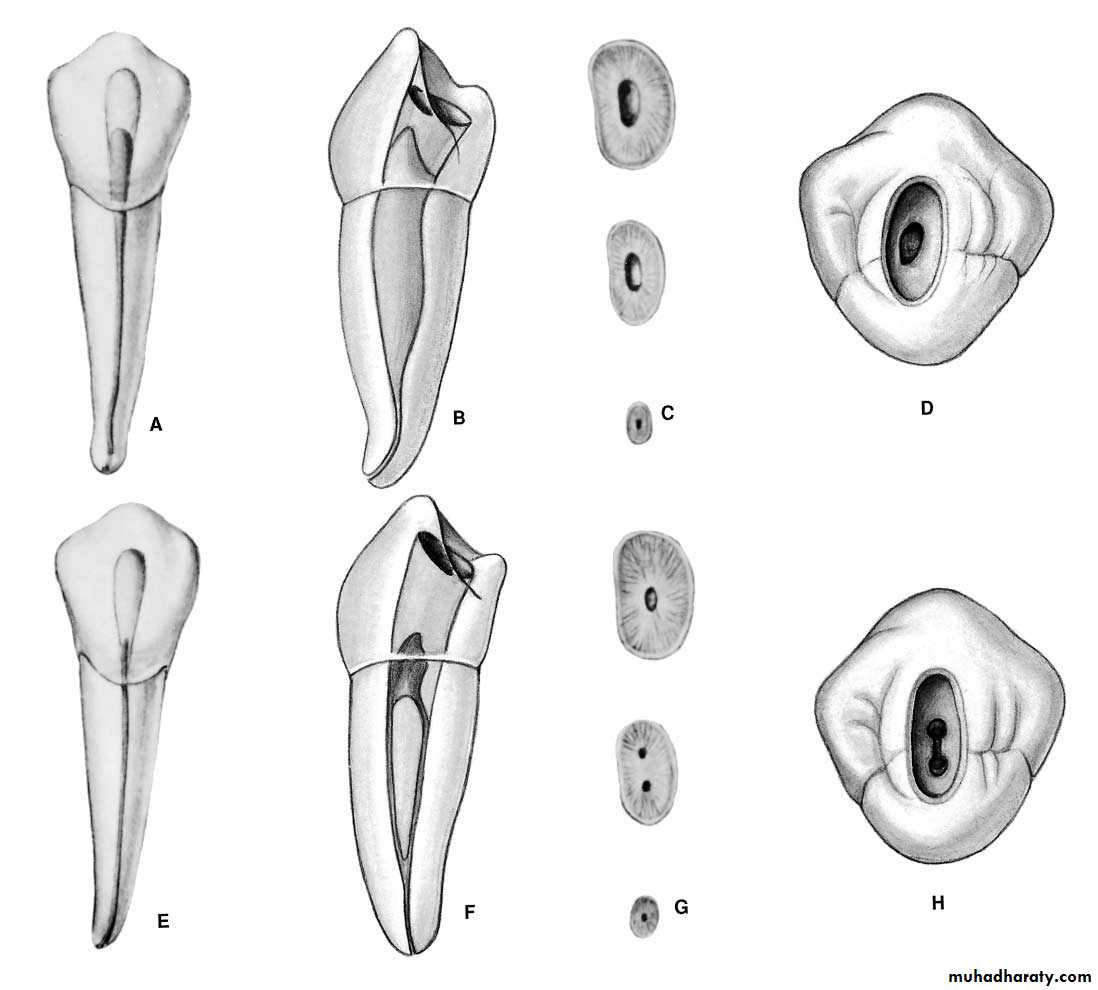
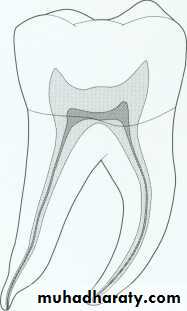
Mandibular second premolar.
Mandibular 2nd premolar:Well developed buccal cusp and much better formed lingual cups.Pulp chamber: Gradually merging with root canal.Canal orifice: At cervical, wide in bucco-lingual dimension, mid rootlevel, continuous to be elongated ovoid, apical third level generally round.Apical distal curvature: likely to be seen, access opening: ovoid funnel shaped, average length: 21mm.
Access opening slightly mesialy allowing adequate room to instrument & fill the curved apical third distally
Access opening technique for premolars:Entrance is always gained through occlusal surface of all posterior teeth.Initial penetration is made parallel to the long axis into the exact center of the central groove.
Round bur No.2 or 4 is used to open into pulp chamber, bur will be felt to drop when the pulp is reached, widen occlusal opening bucco-palatally to allow room for exploring, endo explorer used to locate orifices of canal, do not search for any canal orifice in un roofing pulp chamber.
Extend the cavity bucco-lingually by removing the roof of pulp chamber by round bur as mentioned working from inside the pulp chamber to the outside if the opposite is done we are sacrificing too much tooth structure.
Finishing of the cavity walls is done with a fissure bur to diverge to the access opening which should be ovoid, ovoid preparation reflects the anatomy of the pulp chamber and position of the buccal and lingual canal orifices. Access opening should be funneled downward and flared outward.
Access for lower premolars made slightly buccally to the central groove because the tooth inclines lingually so we might end up with lingual perforation at the neck if we keep drilling lingually and so removing unnecessary tooth structure.
Access for upper premolar: out line form less extensive for single canal case than with 2 canals case, buccal canal approached buccally, and palatal canal approached palatally if we have parallel canals. Sometimes the opposite occur and reference points will be the opposite, also when we have converging canals coronally i:e according to divergence of canals the approaching of canal will differ.
Put TF in the incremental technique i:e 2,3,4 layers until filling the cavity do not use blob technique (one increment) leave space between the cavity & TF.
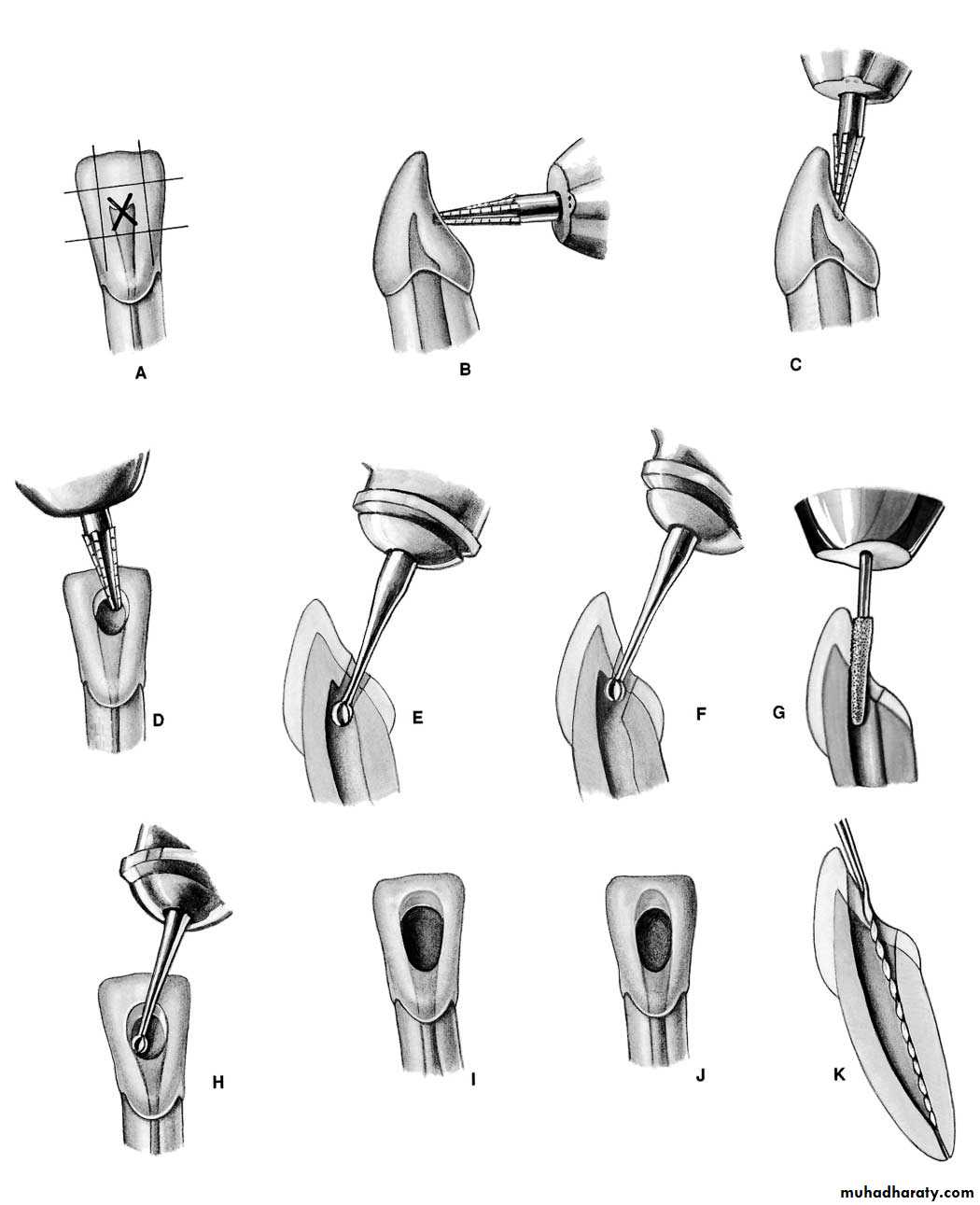
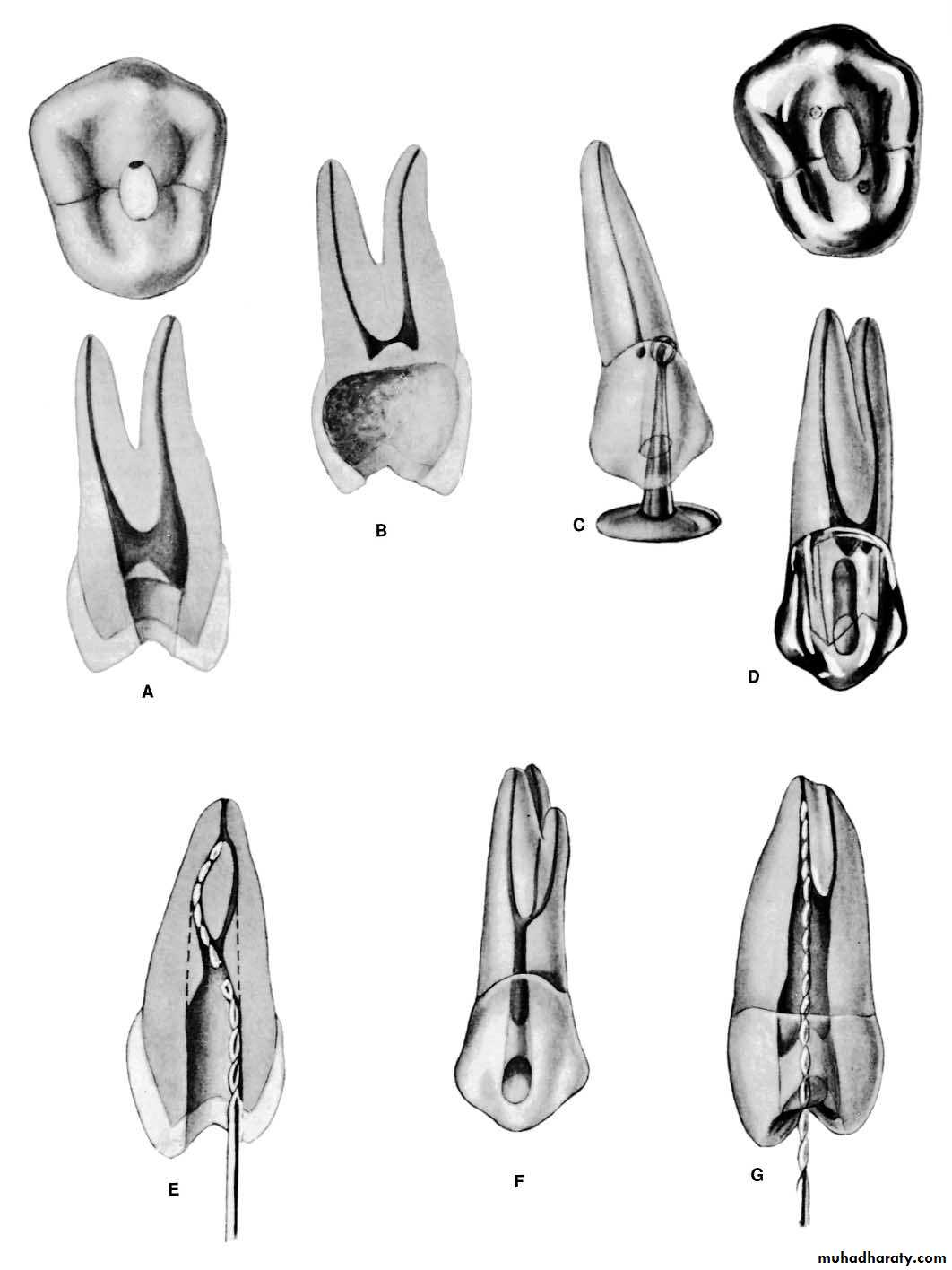
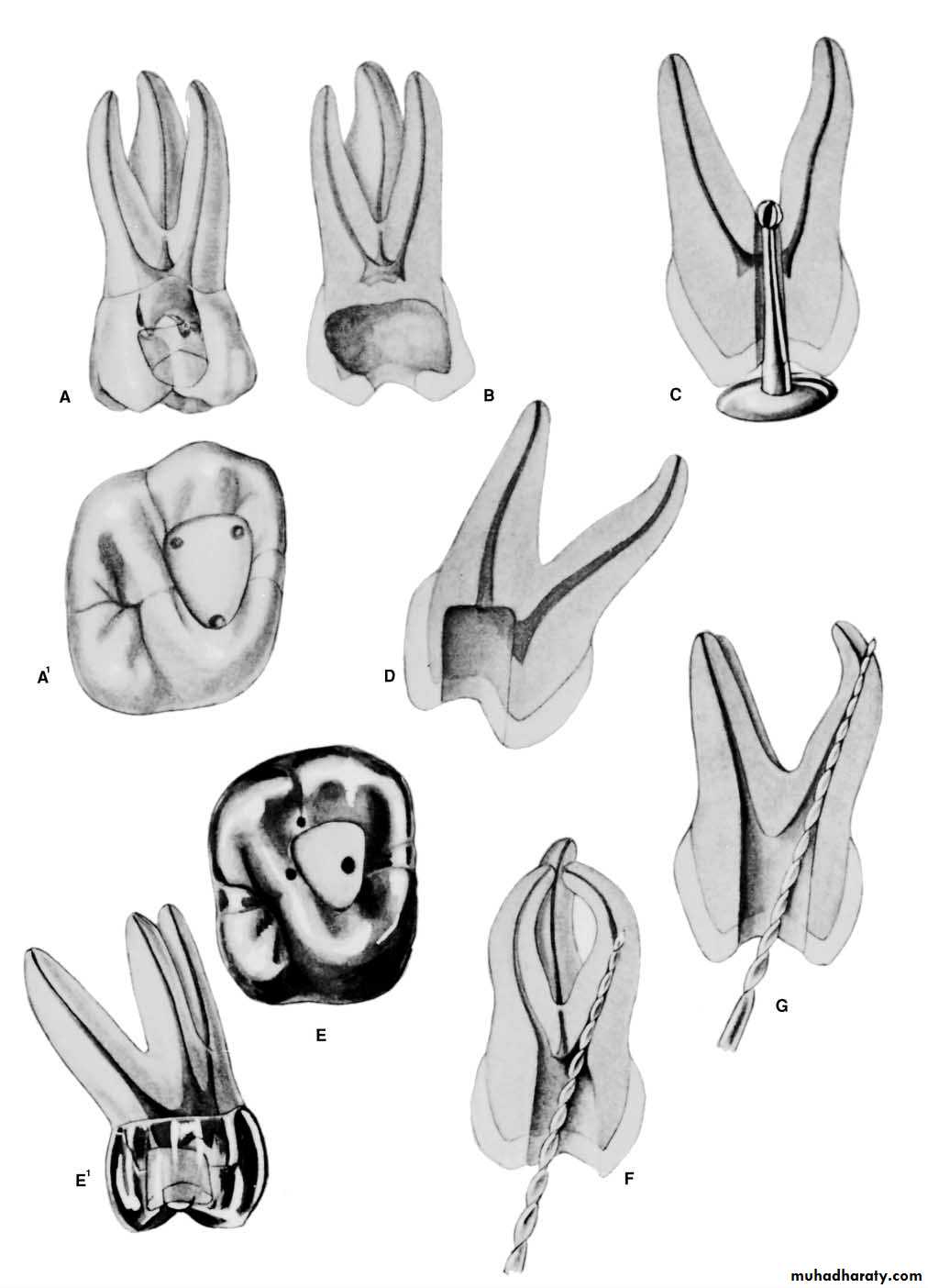
Maxillary Premolar TeethErrors in Cavity Preparation
A.UNDEREXTENDED: preparation exposing only pulp horns. Control of enlarging instruments is abdicated to cavity walls. The white color of the roof of the chamber is a clue to a shallow cavity. B.OVEREXTENDED: preparation from a fruitless search for a receded pulp. The enamel walls have been completely undermined. Gouging relates to failure to refer to the radiograph, which clearly indicates pulp recession.C.PERFORATION: at the mesiocervical indentation. Failure to observe the distal-axial inclination of the tooth led to bypassing receded pulp and perforation. The maxillary first premolar is one of the most commonly perforated teeth.
D.FAULTY ALIGNMENT: of the access cavity through full veneer restoration placed to “straighten” the crown of a rotated tooth. Careful examination of the radiograph would reveal the rotated body of the tooth.E.BROKEN INSTRUMENT: twisted off in a“cross-over” canal. This frequent occurrence may be obviated by extending the internal preparation to straighten the canals (dotted line).
F.FAILURE to explore: débride, and obturate the third canal of the maxillary first premolar (6% of the time). G.FAILURE to explore: débride, and obturate the second canal of the maxillary second premolar (24%of the time).
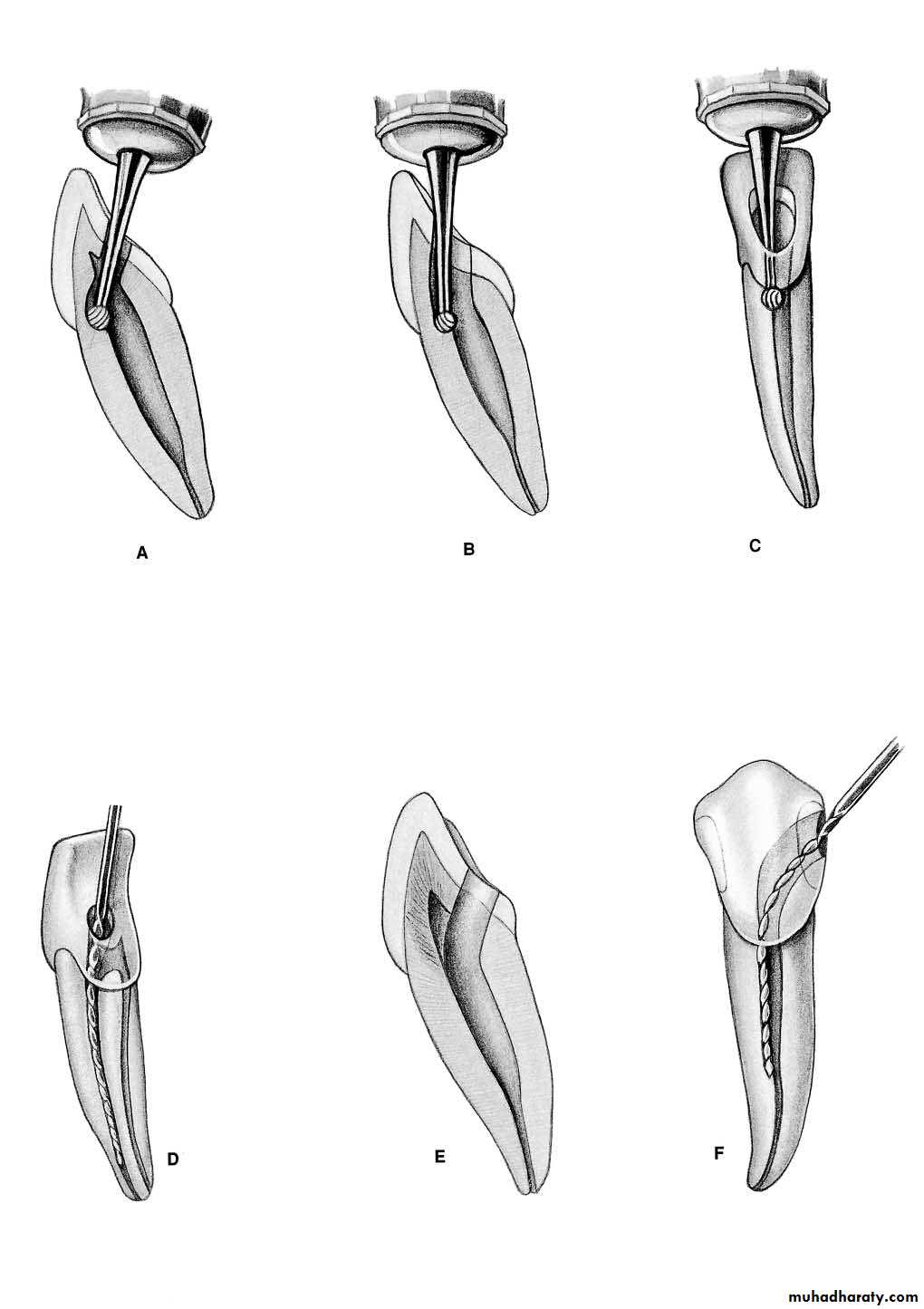
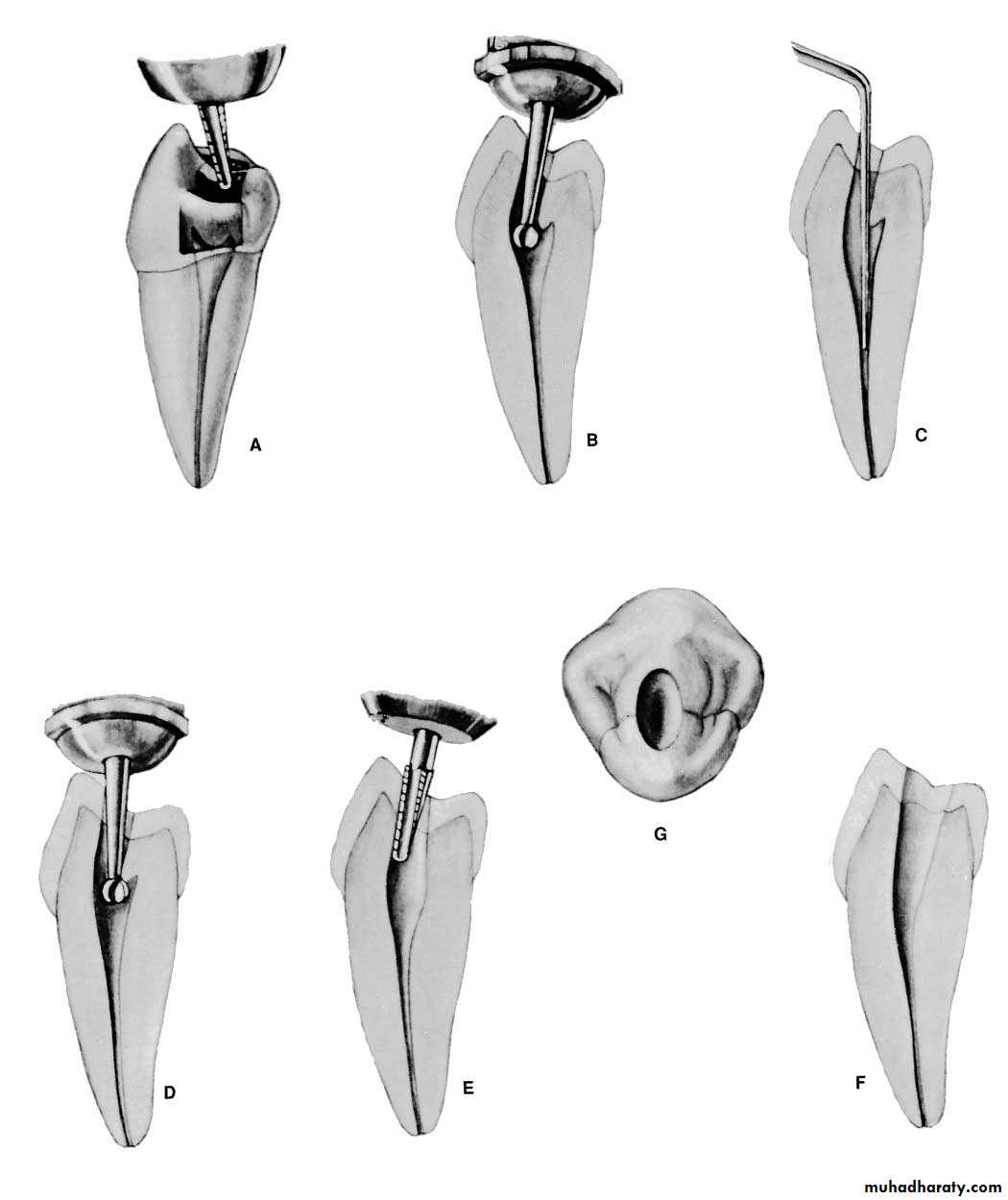
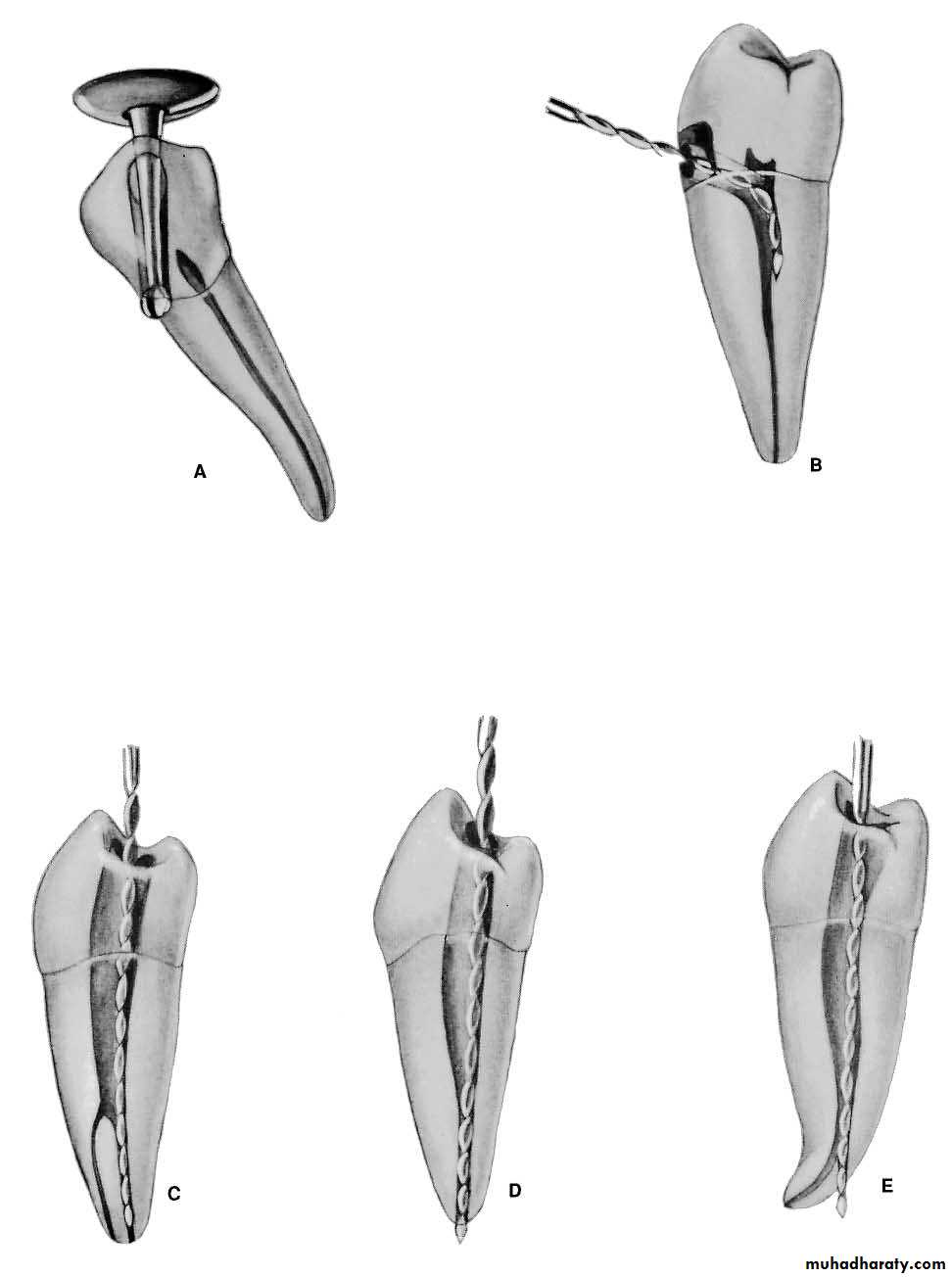
Mandibular Premolar TeethErrors in cavity Preparation
A.PERFORATION: at the distogingival caused by failure to recognize that the premolar has tilted to the distal.B.INCOMPLETE: preparation and possible instrument breakage caused by total loss of instrumentcontrol. Use only occlusal access, never buccal or proximal accessC.BIFURCATION of a canal completely missed, caused by failure to adequately explore the canal with a curved instrument.D.APICAL PERFORATION of an invitingly straight conical canal. Failure to establish the exact length of the tooth leads to trephination of the foramen.
E.PERFORATION: at the apical curvature caused by failure to recognize, by exploration, buccal curvature. A standard buccolingual radiograph will not show buccal or lingual curvature.
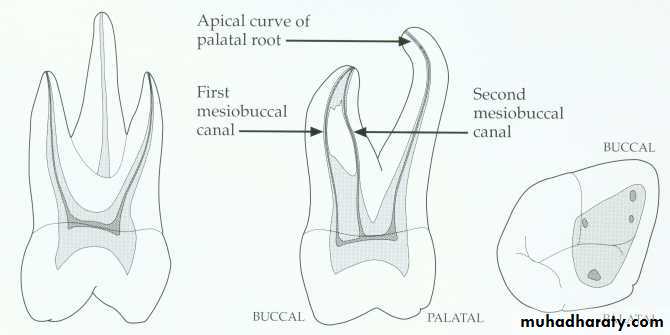
Maxillary first molar.
* Fourth canal (55-74% of teeth) located in the mesiobuccal root.Canal configuration is usually type II or type IV in mesiobuccal root
* The palatal and distobuccal roots usually present a type I configuration.* The length of this tooth is 22mm*Apical-buccal curvature of the palatal root.
* The palatal root slightly longer than the buccal roots.* The pulp chamber is quadrilateral in shape and wider buccopalatally than mesiodistally.* it has four pulp horns, the mesiobuccal is the longest and sharpest in outline.
* The distobuccal pulp horn is smaller than the mesiobuccal but larger than the two palatal pulp horns.* the floor of the pulp chamber is just apical to the cervix, rounded and convex towards the occlusal.
*the minor mesiobuccal canal if present lies on a line joining the main mesiobuccal and palatal canal orifices.*the distobuccal root is closer to the middle of the tooth than to the distal wall.
* The distobuccal canal is the shortest and finest of the three canals.* the palatal canal is the largest and longest of three canals and in 50% the canal curved buccally in apical third.
Maxillary second molar.
*the max. 2nd. molar is usually a smaller replica of the first molar.*the roots are less divergent and more fusion than max 1st molar.
*teeth with three canals and three apical foramina are prevalent and the average length is 21mm.
2 canal, buccal & palatal
Access opening to max. molars*the traditional access cavity outline for max. teeth is in mesial two thirds of the occlusal surface leaving the oblique ridge intact.*it is triangular with the base of the triangle towards the buccal & the apex palatally.*Initial penetration is made in the exact center of the mesial pit with the bur directed toward the lingual using No.4 or 6 round bur.* the depth of 9mm is the usual position of the floor of the pulp chamber working form inside toward outside.
*the walls should not be undercut but should flare occlusally to prevent the accidental forcing of the T.F into the pulp chamber during mastication and thus prevent occurring between visits
*final finish and funneling of cavity walls are compeleted with U shape fissure bur.
*Enlargement of buccal canals is accomplished by reaming and filling.*A dark cavity floor with lines connecting orifice is in marked contrast to white walls.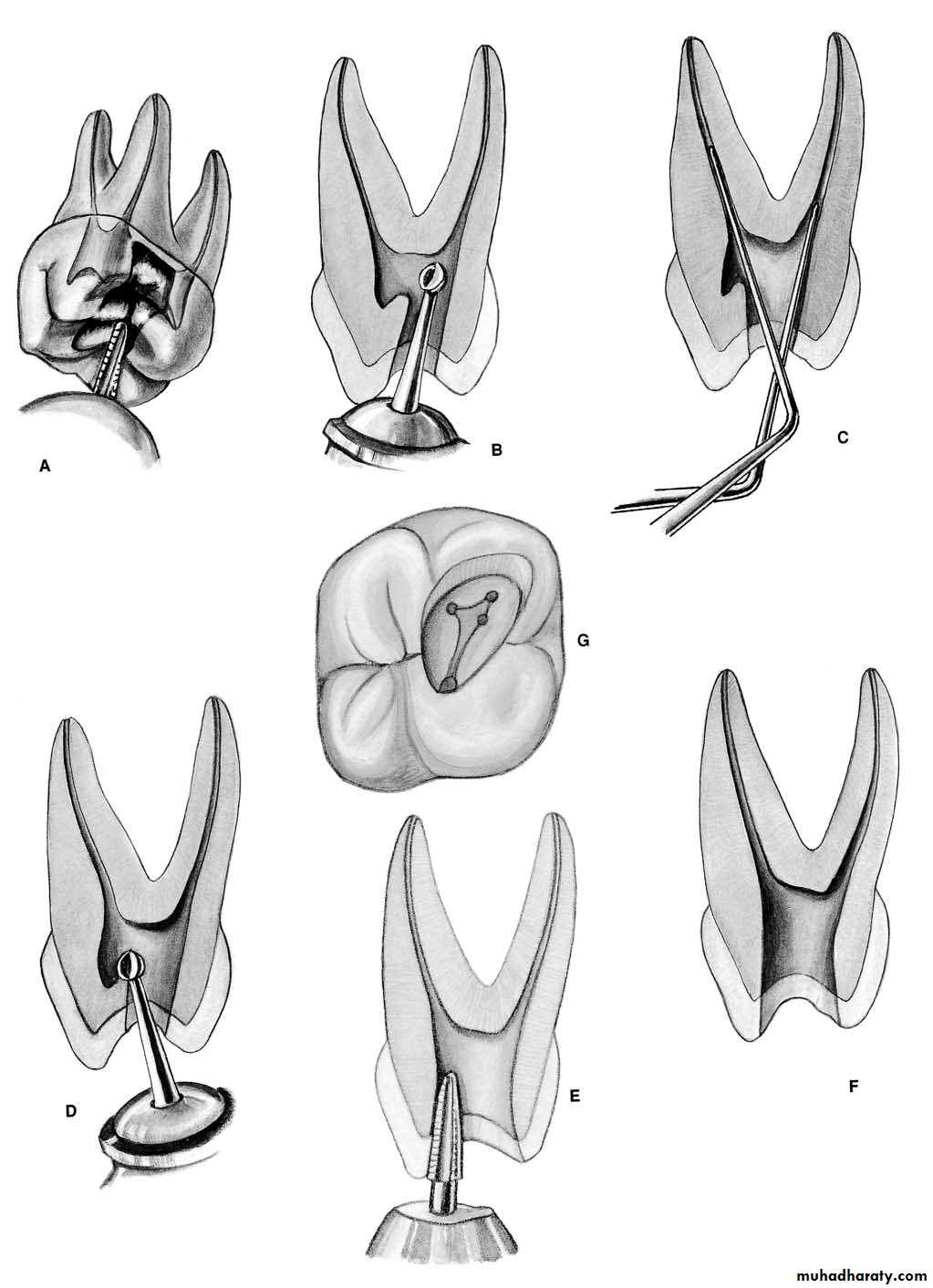

Maxillary Molar TeethErrors in cavity Preparation
A.UNDEREXTENDED preparation. Pulp horns have merely been “nicked,” and the entire roof of the pulp chamber remains. “White” color dentin of the roof is a clue to underextension→Instrument control is lost.B.OVEREXTENDED preparation undermining enamel walls. The crown is badly gouged owing to failure to observe pulp recession in the radiograph.C.PERFORATION into furca using a surgical-length bur and failing to realize that the narrow pulp chamber had been passed. Operator error in failure to compare the length of the bur to the depth of the pulp canal floor. Length should be marked on the bur shank with Dycal.
D.INADEQUATE: vertical preparation related to failure to recognize severe buccal inclination of an unopposed molar. E.DISORIENTED: occlusal outline form exposing only the palatal canal. A faulty cavity has been prepared in full crown, which was placed to “straighten” a rotated molar . Palpating for mesiobuccal root prominence would reveal the severity of the rotation.
F.LEDGE FORMATION: caused by using a large straight instrument in a curved canal.G.PERFORATION: of a palatal root commonly caused by assuming the canal to be straight and failing to explore and enlarge the canal with a fine curved instrument.
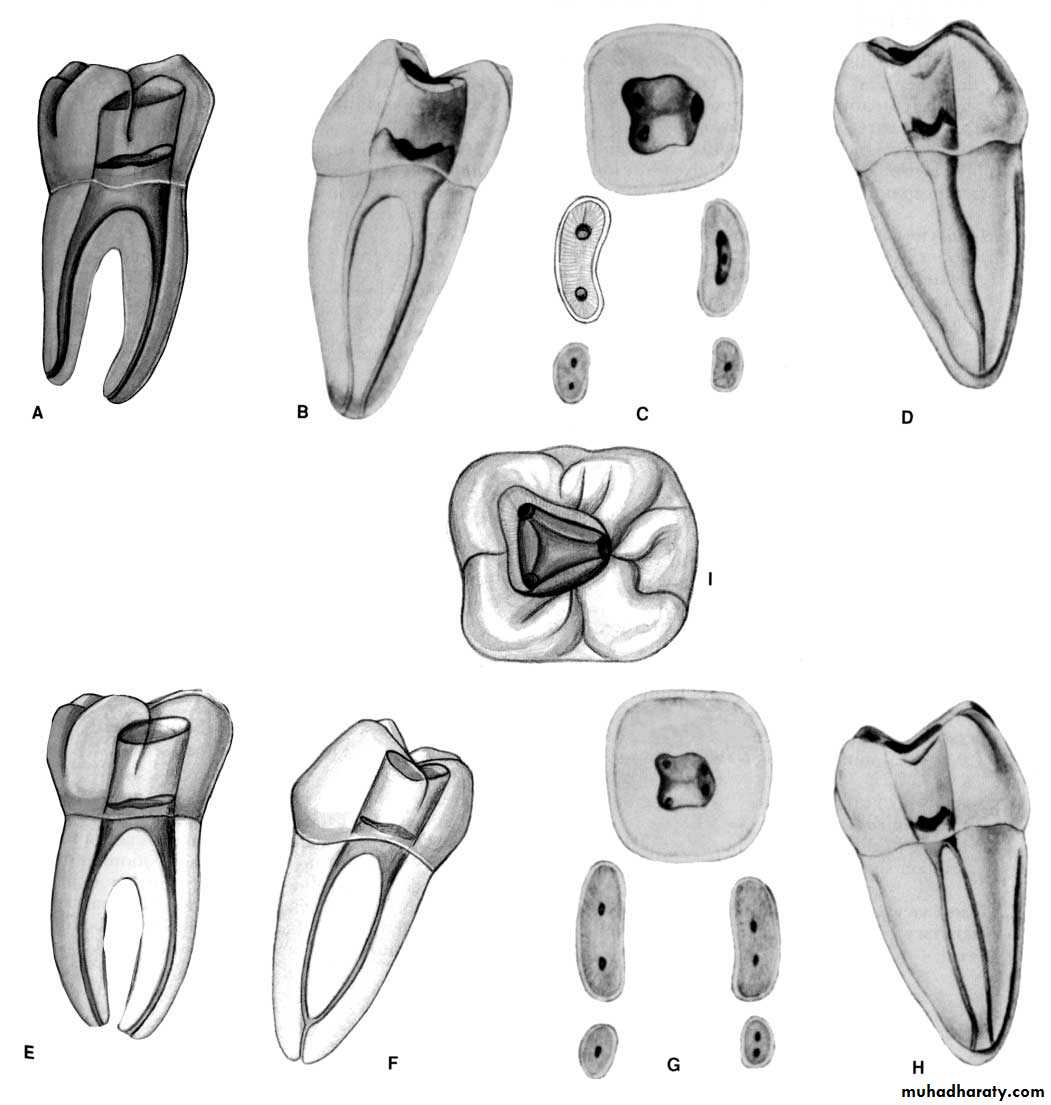
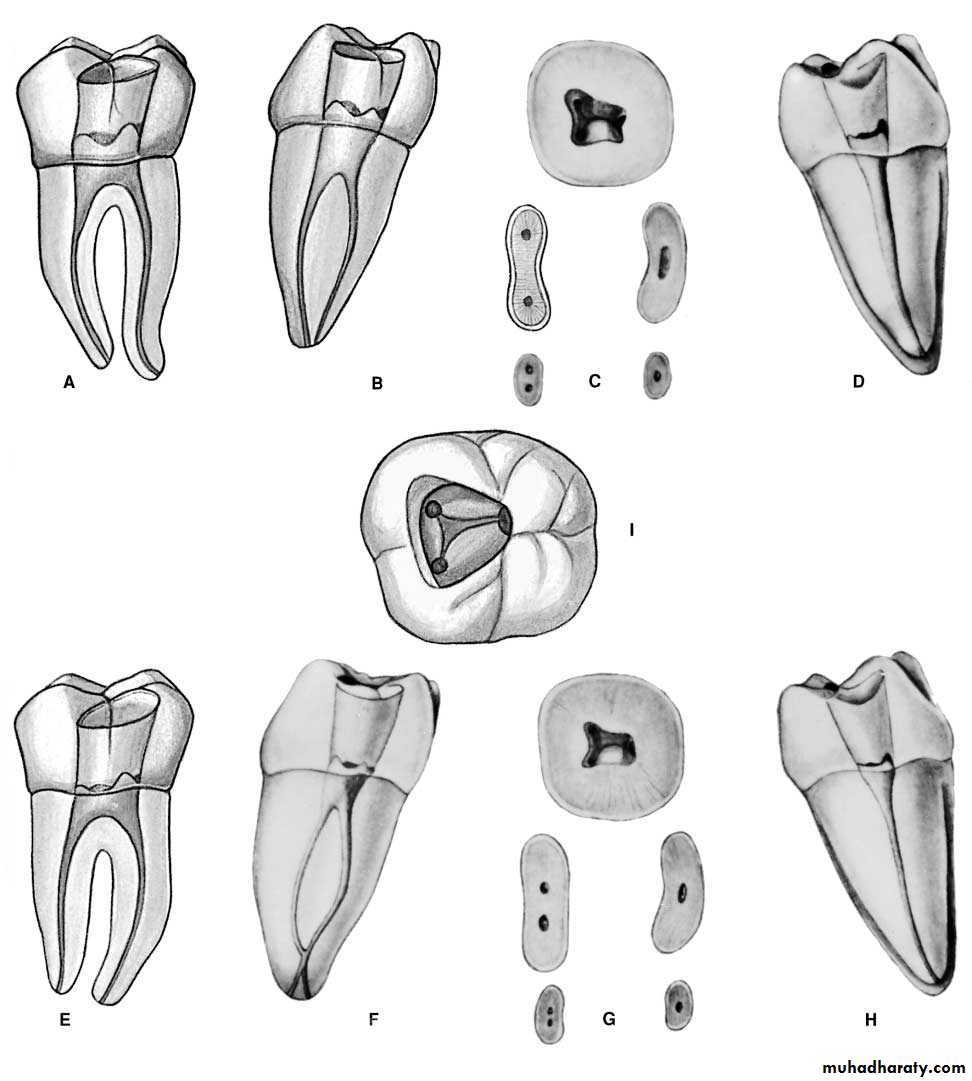
Mandibular first molar.
Distal root can have two canals
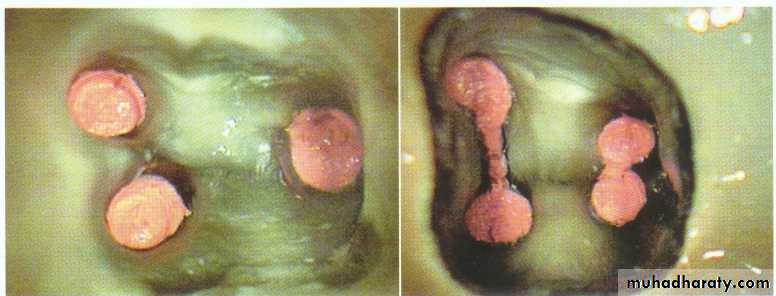
Mandibular first molar.* The Man 1st molar usually has two roots, mesial & distal.*Single mesial root with 2 canals.*the distal root is curved mesially.&mesial root curved distally.*the two-rooted molar usually has a canal configuration of three canals.
* The incidence of two distal canals has been reported as 38%.*the pulp chamber is wider mesially than it distally &may have five pulp horns.
*the lingual pulp horns being longer & more pointed.*the floor is rounded &convex toward the occlusal & lies just apical to the cervix.* mesiobuccal canal tend to be much finer than the mesiolingual.*the mesial root in 40-45% has only one apical foramen.
*when a 2nd distal canal is present on the distolingual aspect it tends to curve towards the buccal.*the average length is 21mm.
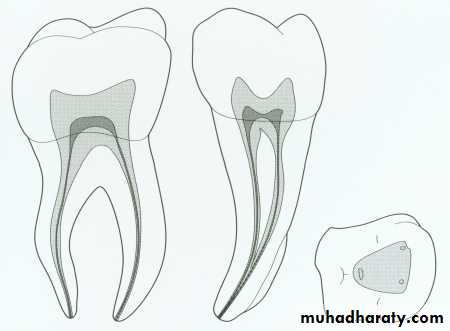
Mandibular second molar.
* Man 2nd molar presents as a smaller version of the man 1st molar.*the average length is 20mm.*the mesial root has two canal but the distal root usually has one canal.*the mesial canals tend to fuse in the apical third to give rise one main apical foramen.*32-33% of man2nd molars have tendency to fused roots.
Access cavity to mand. molar
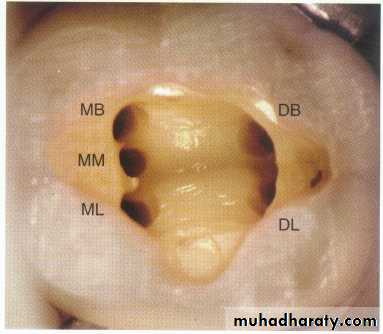
*Entrance is always gained through the occlusal surface.*Initial penetration is made in the exact center of the mesial pit with the bur directed toward the distal using round bur no.4 or6.The prevalence of the 2nd distal canal in mand 1st molars necessitates a rectangular outline.*care should be taken to remove the roof of the pulp chamber completely without causing damage to the floor of the pulp chamber
* the depth of 9mm is the usual position of the floor of the pulp chamber working form inside toward outside.*final finish and funneling of cavity walls are compeleted with U shape fissure bur.
*the walls of the access cavity should diverge towards the occlusal to resist masticatory forces and prevent dislogement of the T.F.* access cavity may require enlargement &/or modification.
Mandibular Molar TeethError in cavity Preparation
A.OVEREXTENDED: preparation underminingenamel walls. The crown is badly gouged owing to failure to observe pulp recession in the radiograph.B.PERFORATION :into furca caused by using alonger bur and failing to realize that the narrowpulp chamber had been passed. The bur should be measured against the radiograph and the depth to the pulpal floor marked on the shaft with Dycal.
C.PERFORATION: at the mesial-cervical caused by failure to orient the bur with the long axis of the molar severely tipped to the mesial.D.DISORIENTED: occlusal outline form exposing only the mesiobuccal canal. A faulty cavity has been prepared in full crown, which was placed to “straighten up” a lingually tipped molar .
E.FAILURE: to find a second distal canal owing to lack of exploration for a fourth canal.F.LEDGE FORMATION: caused by faulty exploration and using too large of an instrument.G.PERFORATION: of the curved distal root caused by using a large straight instrument in a severely curved canal.
Access opening difficulties.Calcified canalHard to find pulp chamber: (receded pulp, stop drilling and taking x-ray to prevent perforation, weakening tooth structure)Long axis of the tooth should be known to prevent perforation at the neck of the crown.
Entrance in molar teeth: Should be limited to the mesial half of the occlusal surface since pulp chamber located there, most of pulp chamber occupy mesial half of the crown, so there is no need to go so far distally→ sacrificing tooth structure.
Roof of the pulp chamber: should be removed completely to locate canal orifice and get direct access to canal instrumentation.Floor of the pulp chamber: Should be left untouched, its very important anatomical landmarks.
Narrow and conservative access opening: results of:Root canal debridement and obturation not sufficient.
Bending of instruments.Missed canal.Discoloration because of remnant of pulp chamber roof (pulp horn remains).
Establishment of a sound reference point: any where tooth structure or unsupported cusp should be eliminated because if not; fracture of cusp might happen during subsequent visit and at that time the reference point is lost and the working length established is lost.
Once you enter the pulp camber with bur before complete access opening the roof of the pulp chamber must be removed completely in order to be able to see well because the bleeding makes the vision to be difficult so we do so to stop the bleeding.
Shallow access opening and instrumentation through the pulp chamber or pulp horn, to know that it is not canal:Sever bleeding cannot be arrested.Color of dentine: floor-dark bluish, roof-white.
Anatomical land marks of the floor of pulp chamber, convex, grooves connecting canal orifices together.Distinguish level of floor and roof through the radiograph.
Obturation phase: the root canal system is filled with inert root canal material from dentinocemental junction to the canal orifice to provide hermetic seal.
So these phases communicate with each other, each phasesupport the other and any defect will lead to defect in root canal treatment.