Liver and Gallbladder
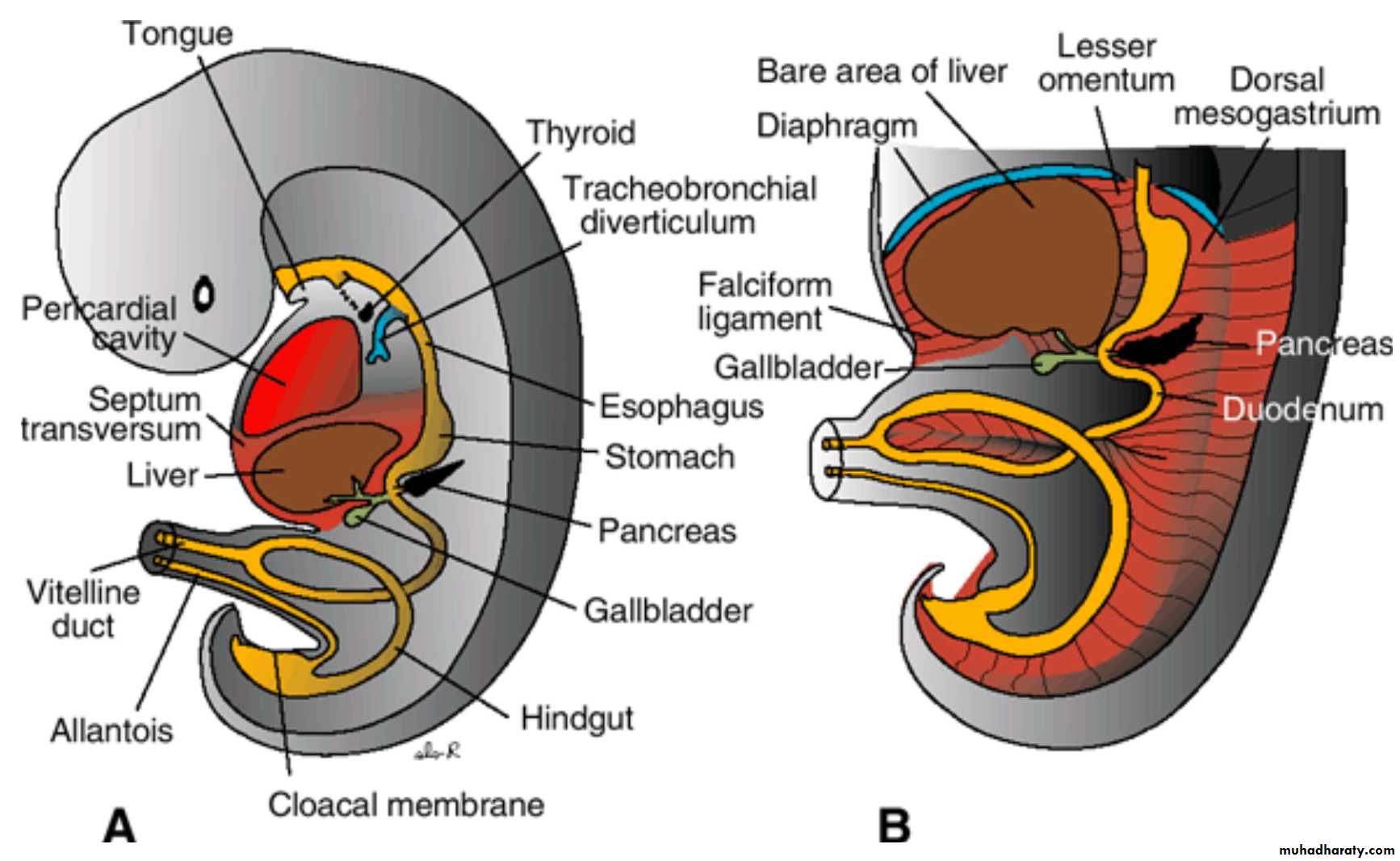
The liver primordium appears in the middle of the third week as an outgrowth of the endodermal epithelium at the distal end of the foregut ) the hepatic diverticulum, or liver bud)
The hepatic diverticulum consists of rapidly proliferating cells that penetrate the Septum transversum( the mesodermal plate between the pericardial cavity and the stalk of the yolk sac) .
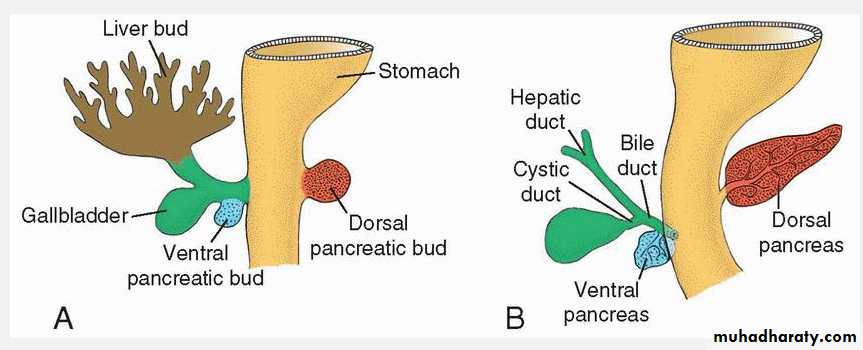
While hepatic cells continue to penetrate the septum, the connection between the hepatic diverticulum and the foregut (duodenum) narrows, forming the bile duct.
A small ventral outgrowth is formed by the bile duct, and this outgrowth gives rise to the gallbladder and the cystic duct
During further development, epithelial liver cords intermingle with the vitelline and umbilical veins, which form hepatic sinusoids. Liver cords differentiate into the parenchyma (liver cells) and form the lining of the biliary ducts. Hematopoietic cells, Kupffer cells, and connective tissue cells are derived from mesoderm of the septum transversum.
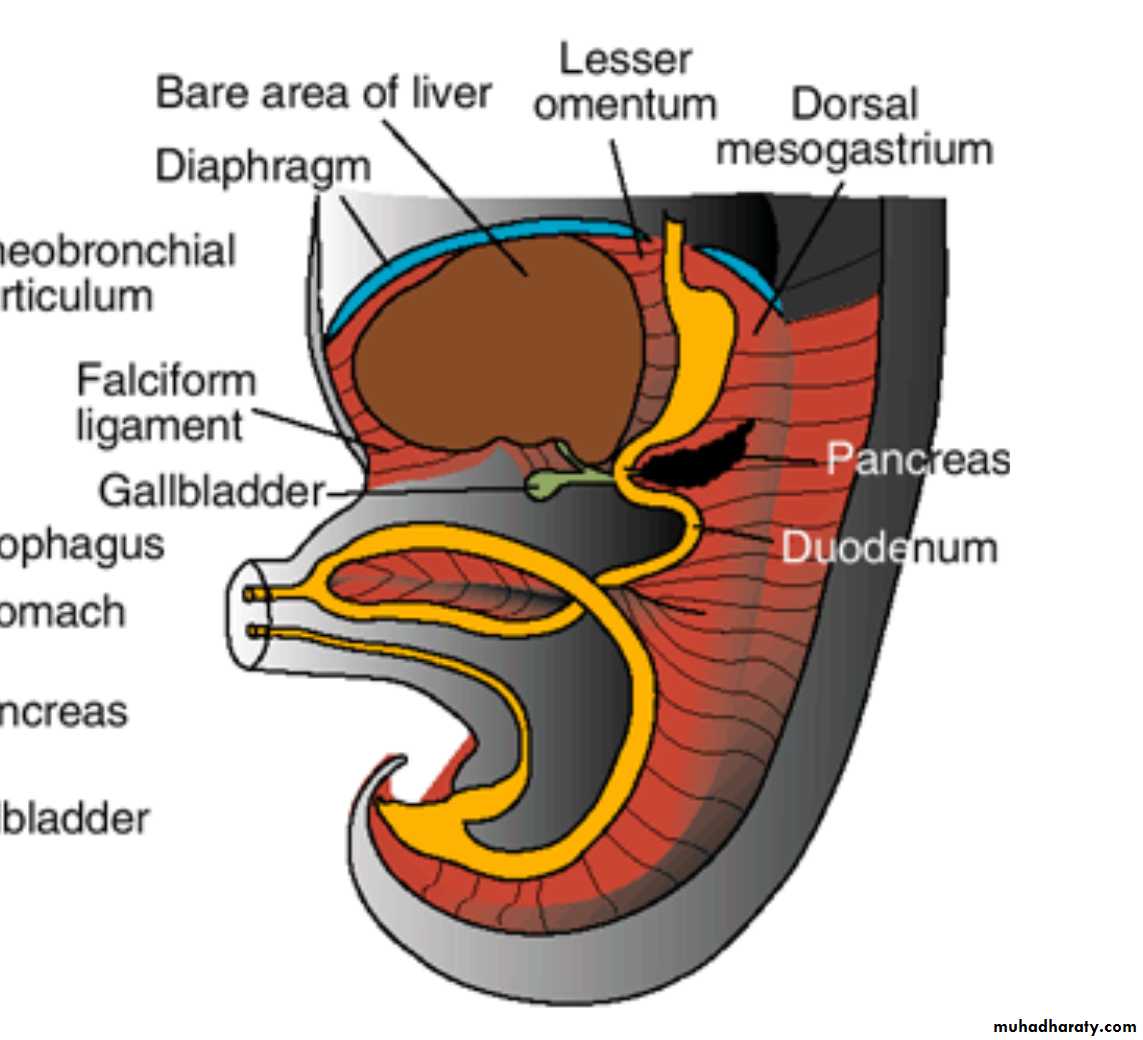
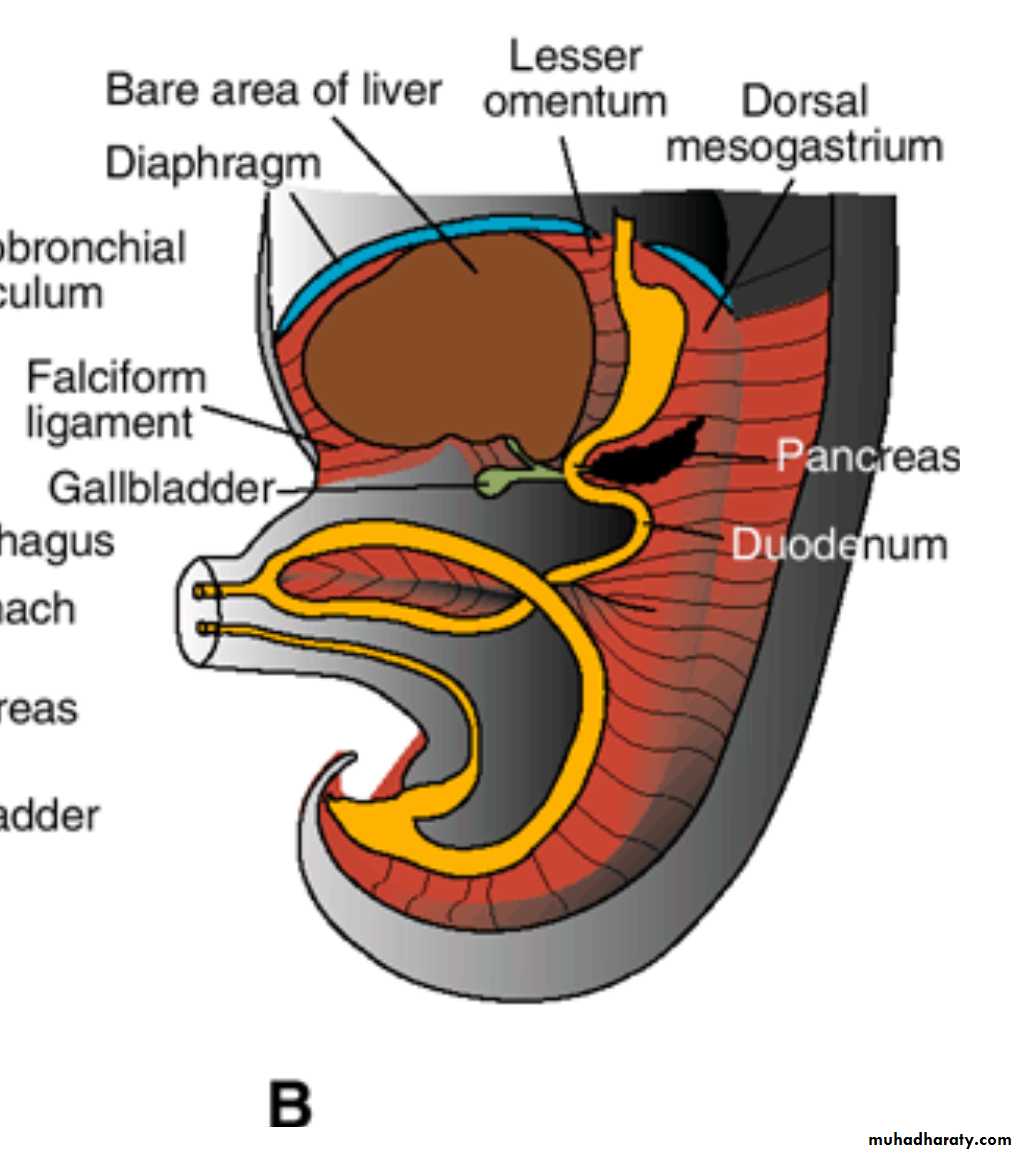
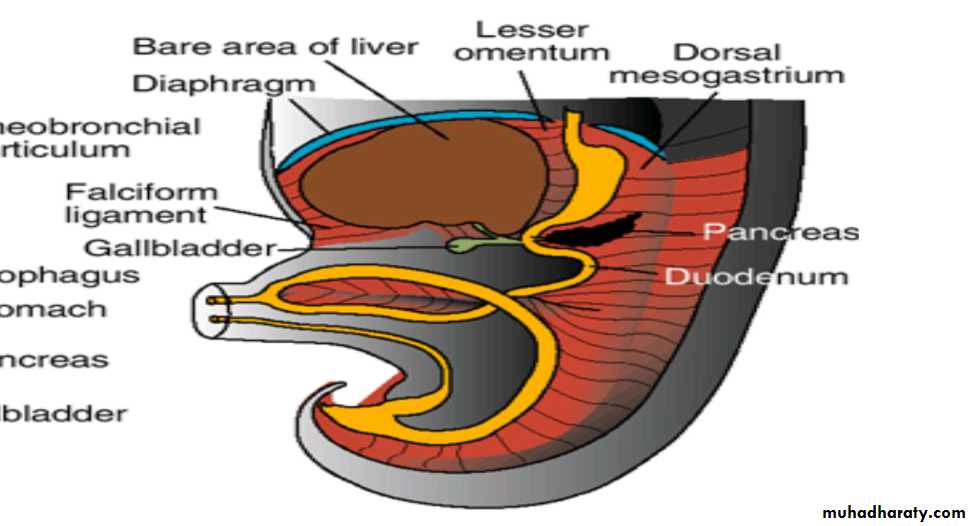
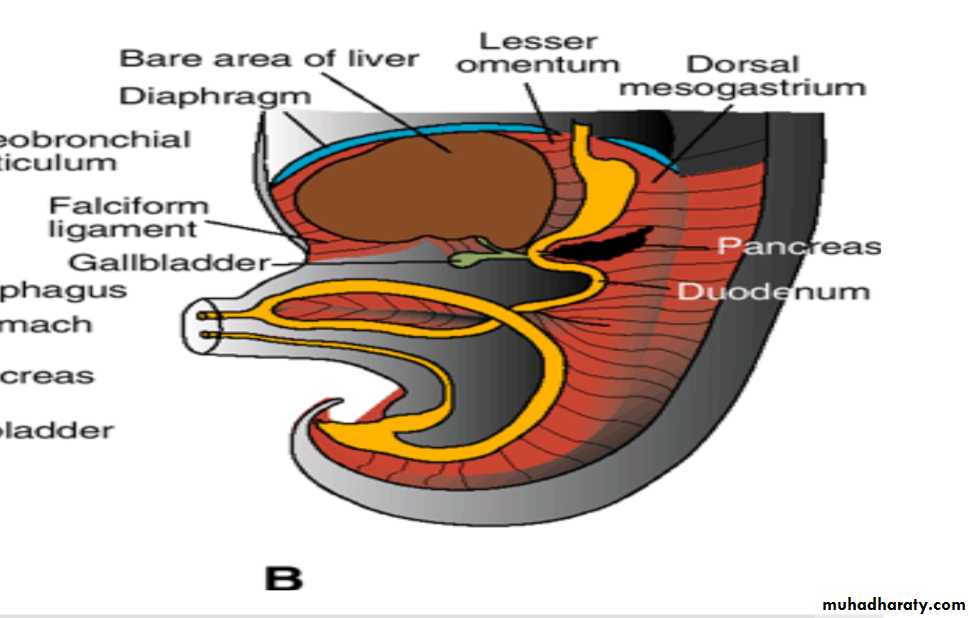
Mesoderm on the surface of the liver differentiates into visceral peritoneum except on its cranial surface , the liver remains in contact with the rest of the original septum transversum. This portion of the septum, which consists of densely packed mesoderm, will form the central tendon of the diaphragm.
The surface of the liver that is in contact with the future diaphragm is never covered by peritoneum; it is the bare area of the liver
Pancreas
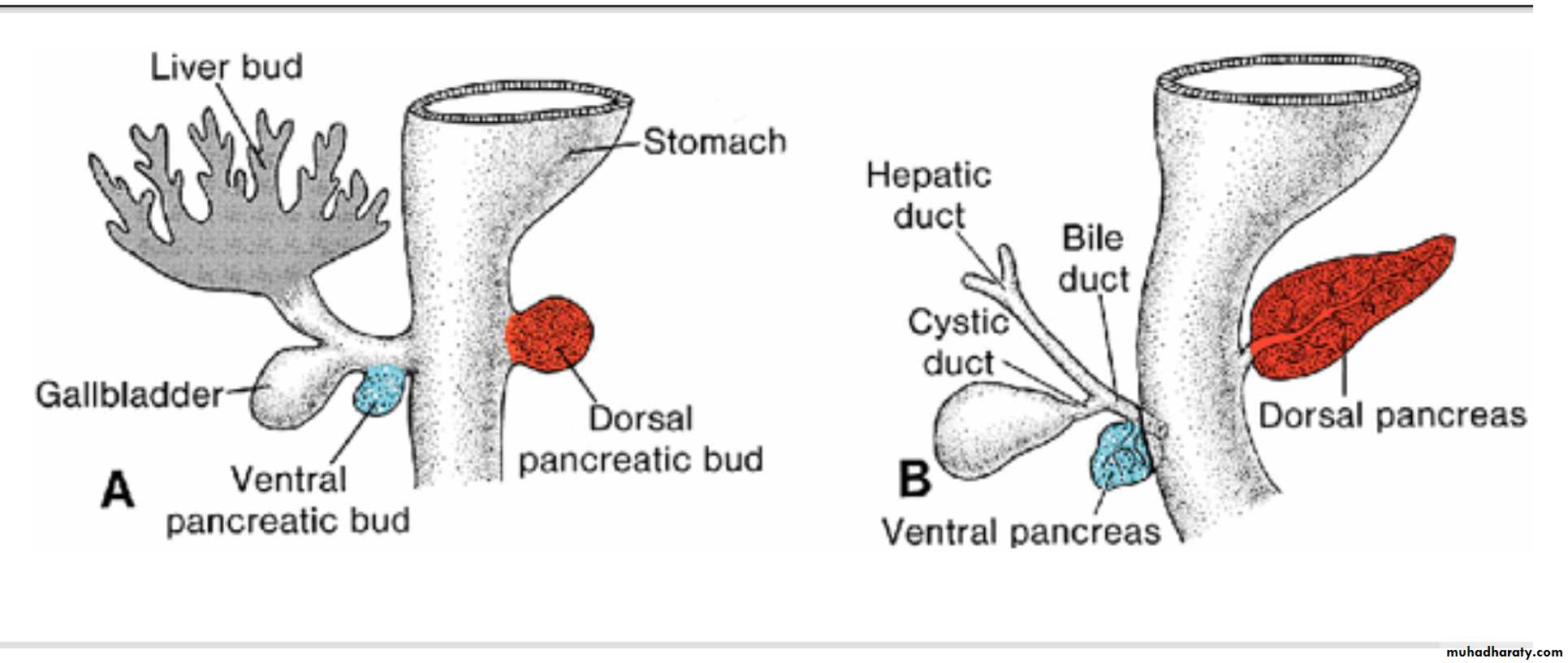
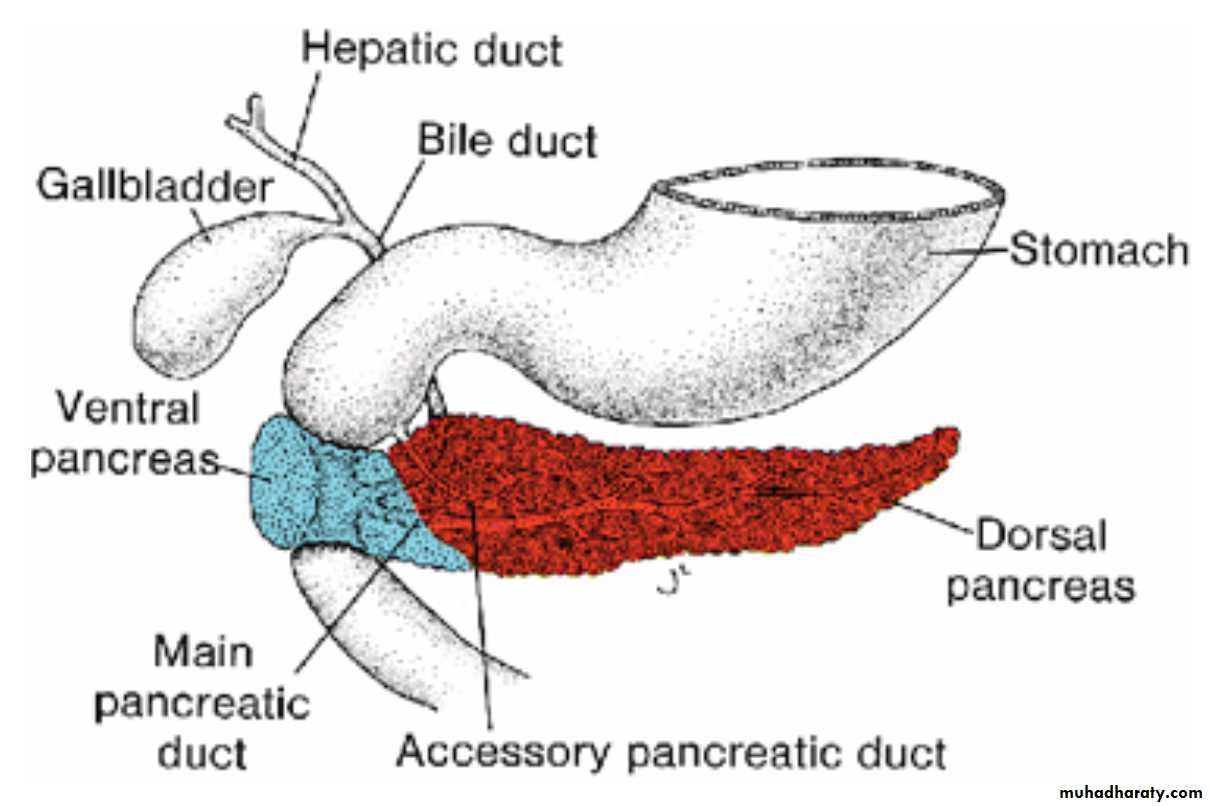
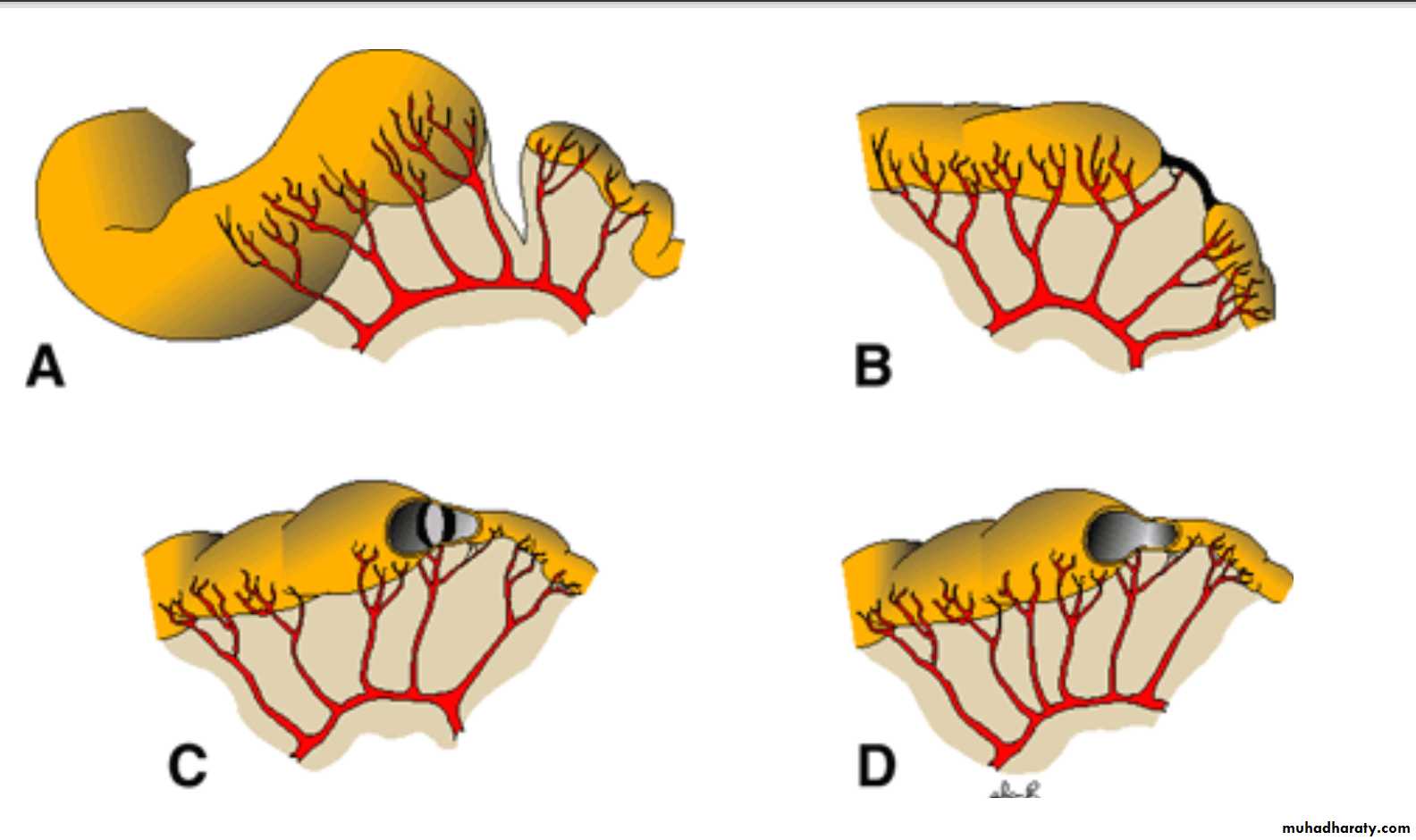
The pancreas is formed by two buds, dorsal and ventral, originating from the endodermal lining of the duodenum.
The dorsal pancreatic bud is in the dorsal mesentery, Tthe ventral pancreatic bud is close to the bile duct .
When the duodenum rotates to the right and becomes C-shaped, the ventral pancreatic bud moves dorsally in a manner similar to the shifting of the entrance of the bile duct.
Finally, the ventral bud comes to lie immediately below and behind the dorsal bud
The parenchyma and the duct systems of the dorsal and ventral pancreatic buds fuse
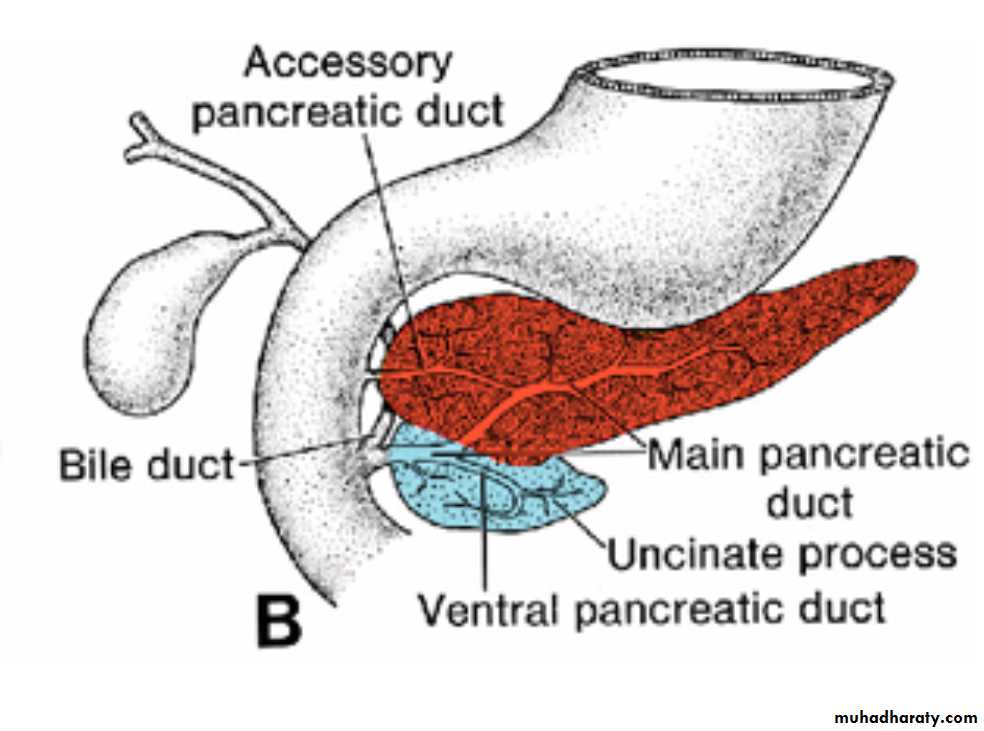
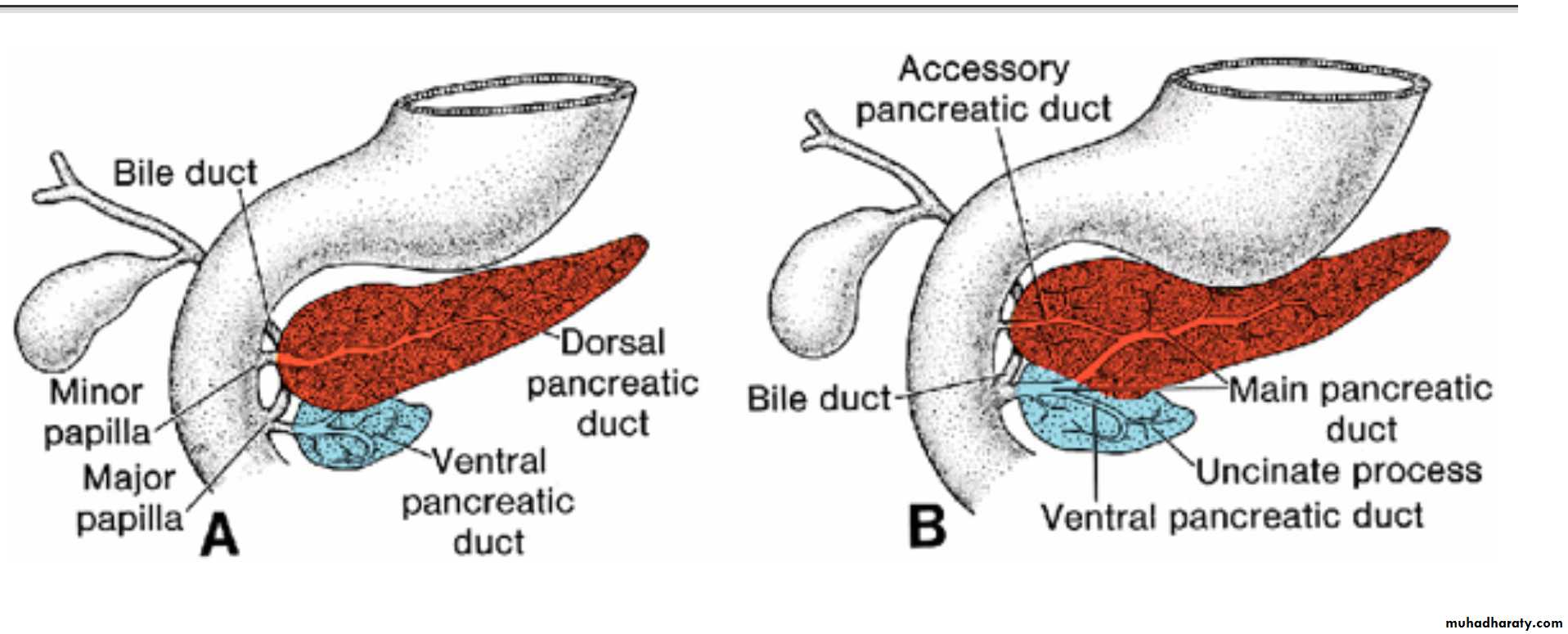
The ventral bud forms the uncinate process and inferior part of the head of the pancreas. The remaining part of the gland is derived from the dorsal bud.
The main pancreatic duct (of Wirsung) is formed by the distal part of the dorsal pancreatic duct and the entire ventral pancreatic duct
The proximal part of the dorsal pancreatic duct either is obliterated or persists as a small channel, the accessory pancreatic duct (of Santorini).
The main pancreatic duct, together with the bile duct, enters the duodenum at the site of the major papilla; the entrance of the accessory duct (when present) is at the site of the minor papilla.
In about 10% of cases the duct system fails to fuse, and the original double system persists.

In the third month of fetal life, pancreatic islets (of Langerhans) develop from paranchymal cells and scatter throughout the pancreas.
Insulin secretion begins at approximately the fifth month. Glucagon- and somatostatin-secreting cells also develop from parenchymal cells.
Splanchnic mesoderm surrounding the pancreatic buds forms the pancreatic connective tissue
Pancreatic Abnormalities
Annular pancreas. The ventral pancreas splits and forms a ring around the duodenum, occasionally resulting in duodenal stenosis.
Accessory pancreatic tissue .Most frequently, it lies in the mucosa of the stomach and in Meckel's diverticulum,
Midgut
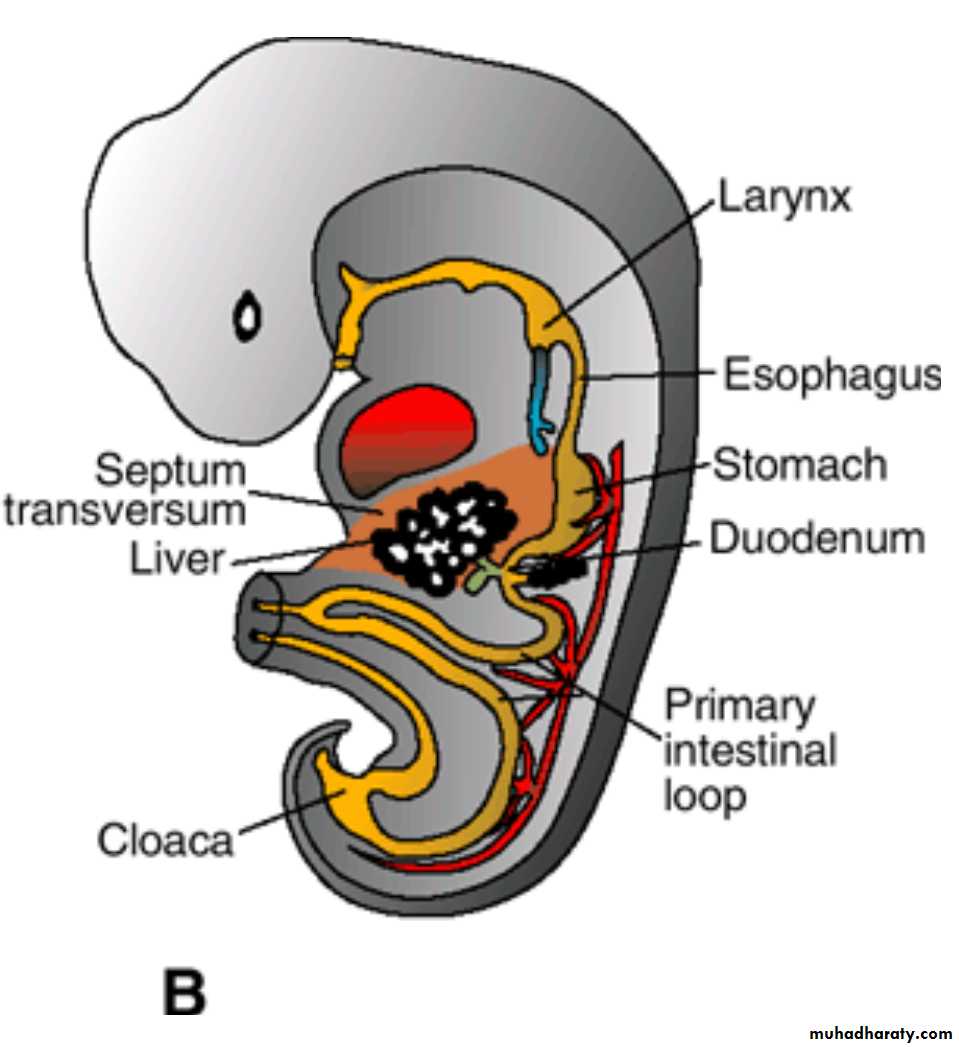
In the 5-week embryo, the midgut is
suspended from the dorsal abdominal wall by a short mesentery andcommunicates with the yolk sac by way of the Vitelline duct or yolk stalk .
The midgut
In the adult, it begins immediately distal to the entrance of the bile duct into the duodenum andterminates at the junction of the proximal two-thirds of the transverse colon with the distal third.
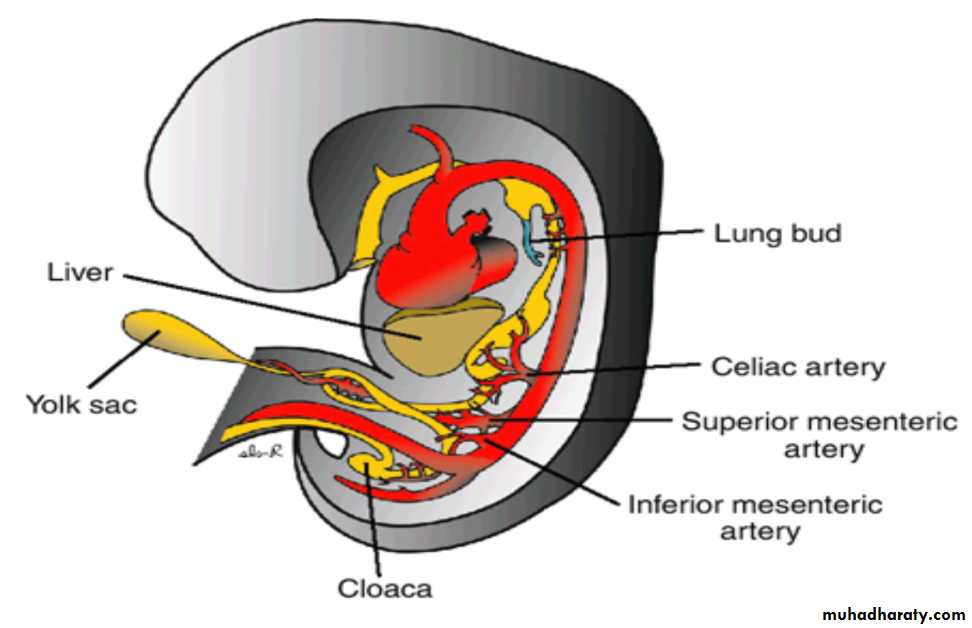
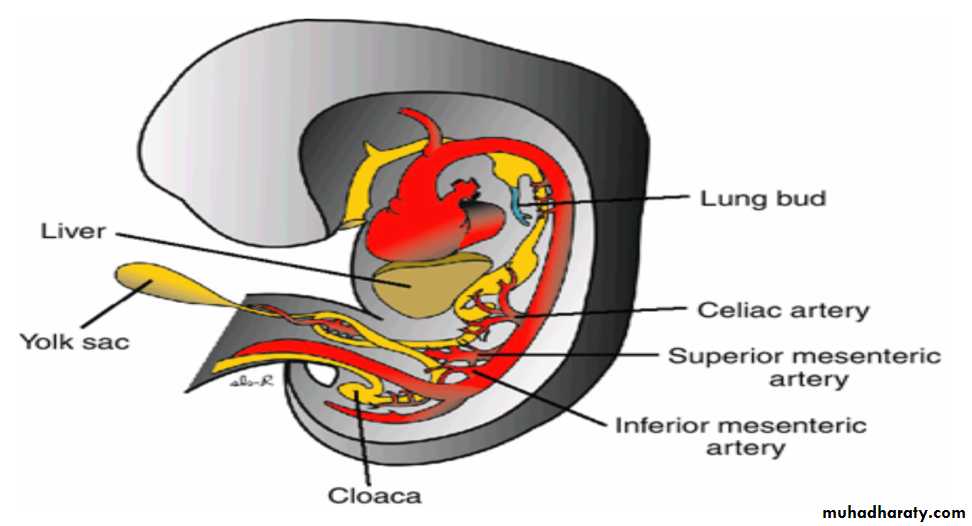
is supplied by the superior mesenteric artery.
Development of the midgut is characterized by
rapid elongation of the gut and its mesentery, resulting in formation of the Primary intestinal loop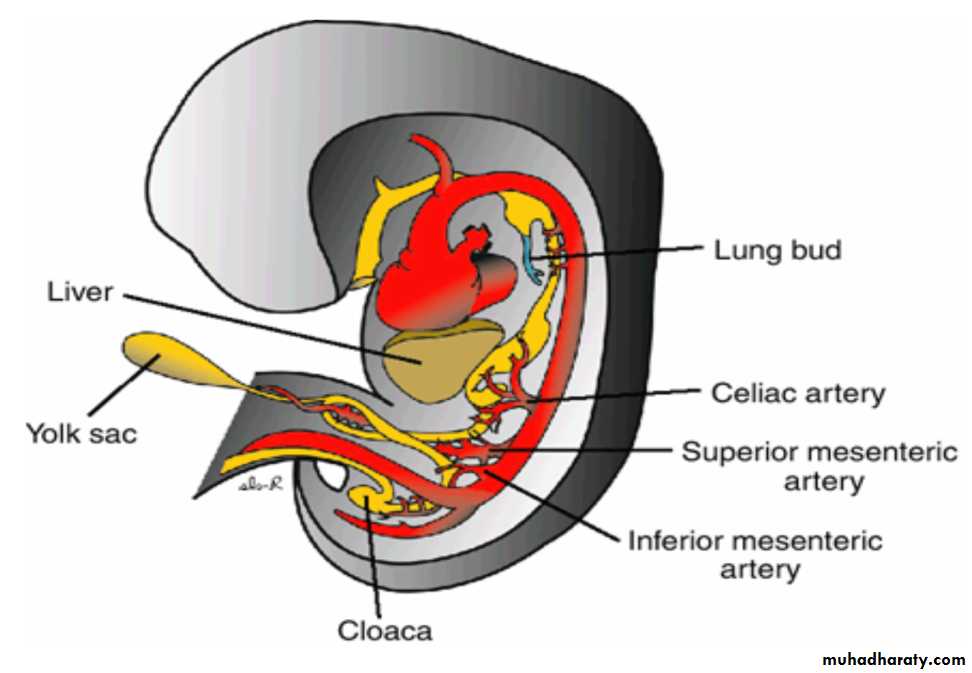
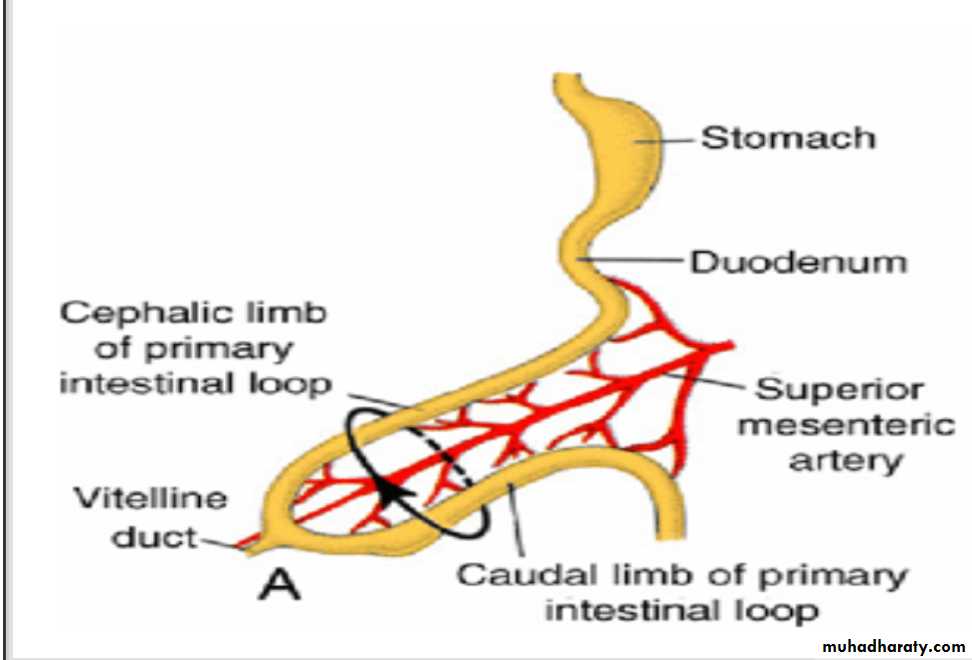
Primary intestinal loop
At its apex, the loop remains in open connection with the yolk sac by way of the narrow Vitelline duct.
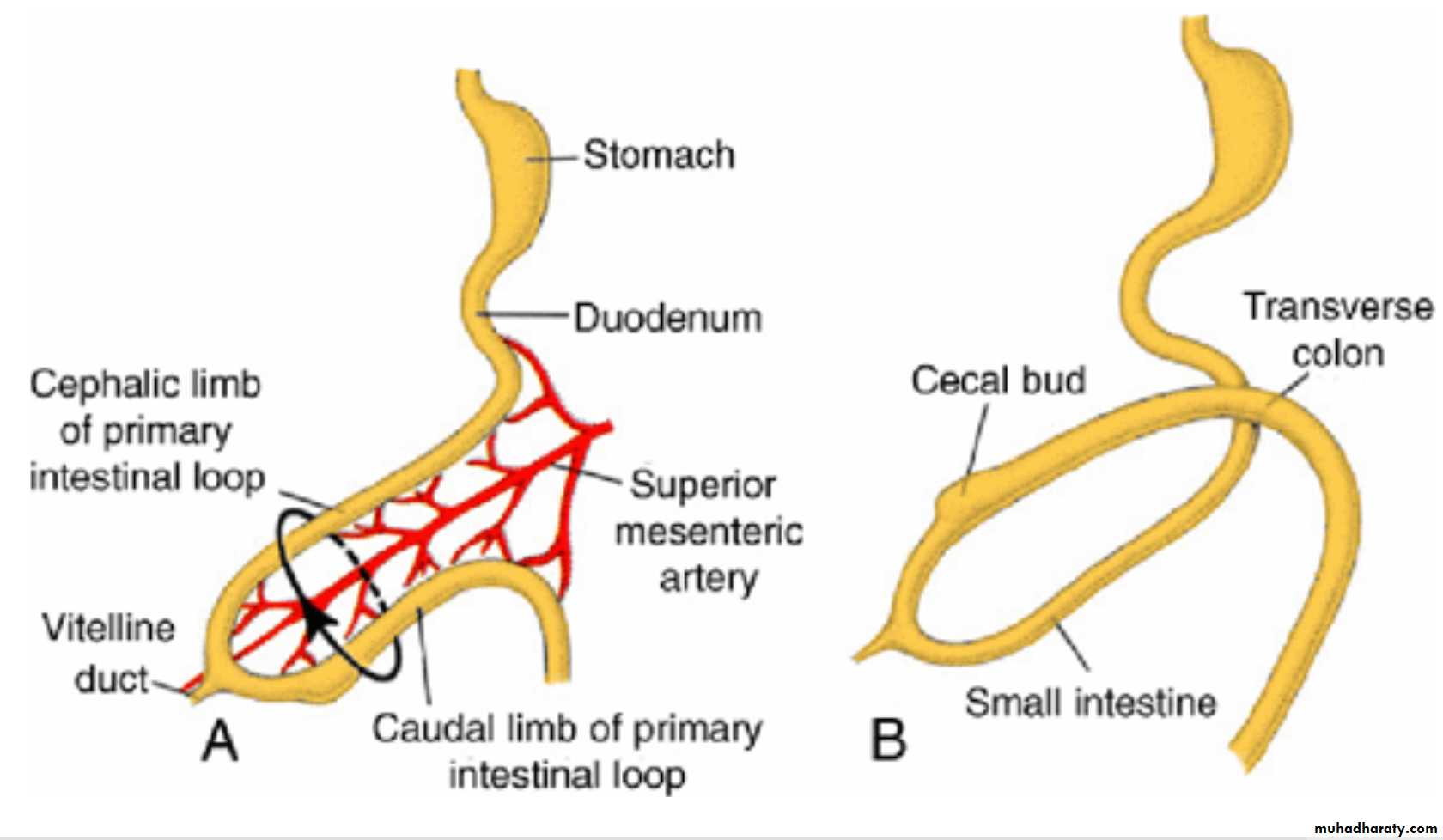
The cephalic limb of the loop develops into the distal part of the duodenum, the jejunum, and part of the ileum.
The caudal limb becomes the lower portion of the ileum, the cecum, the appendix, the ascending colon, and the proximal two-thirds of the transverse colon.
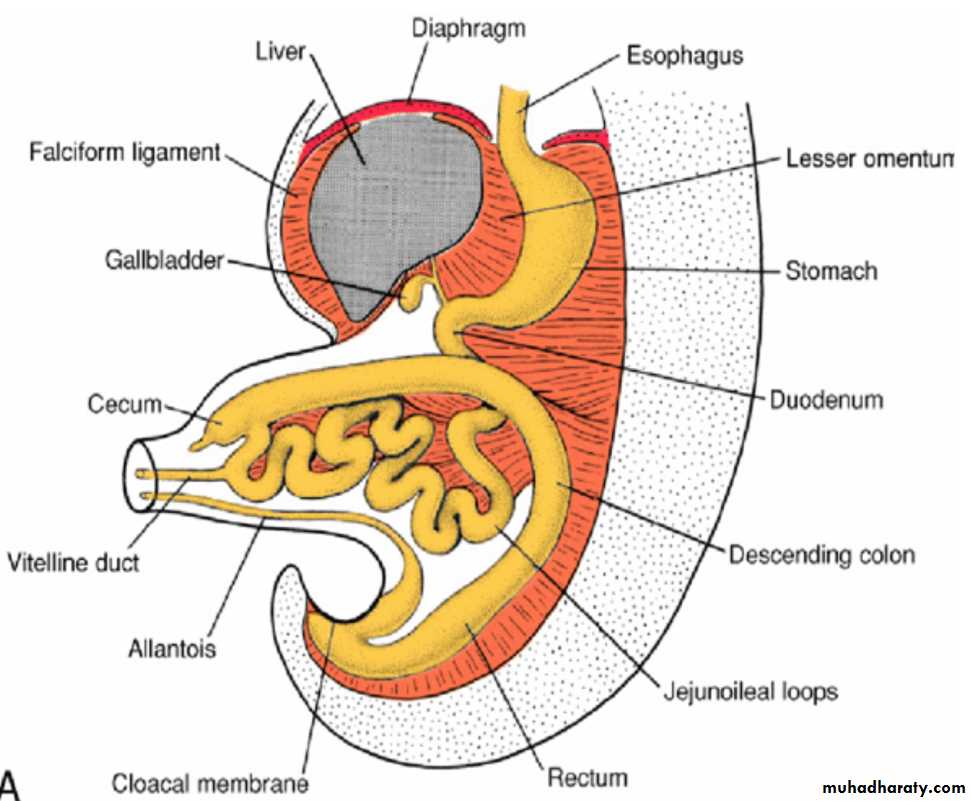
physiological umbilical herniation
during the sixth week of development, the abdominal cavity temporarily becomes too small to contain all the intestinal loops, and they enter the extraembryonic cavity in the umbilical cord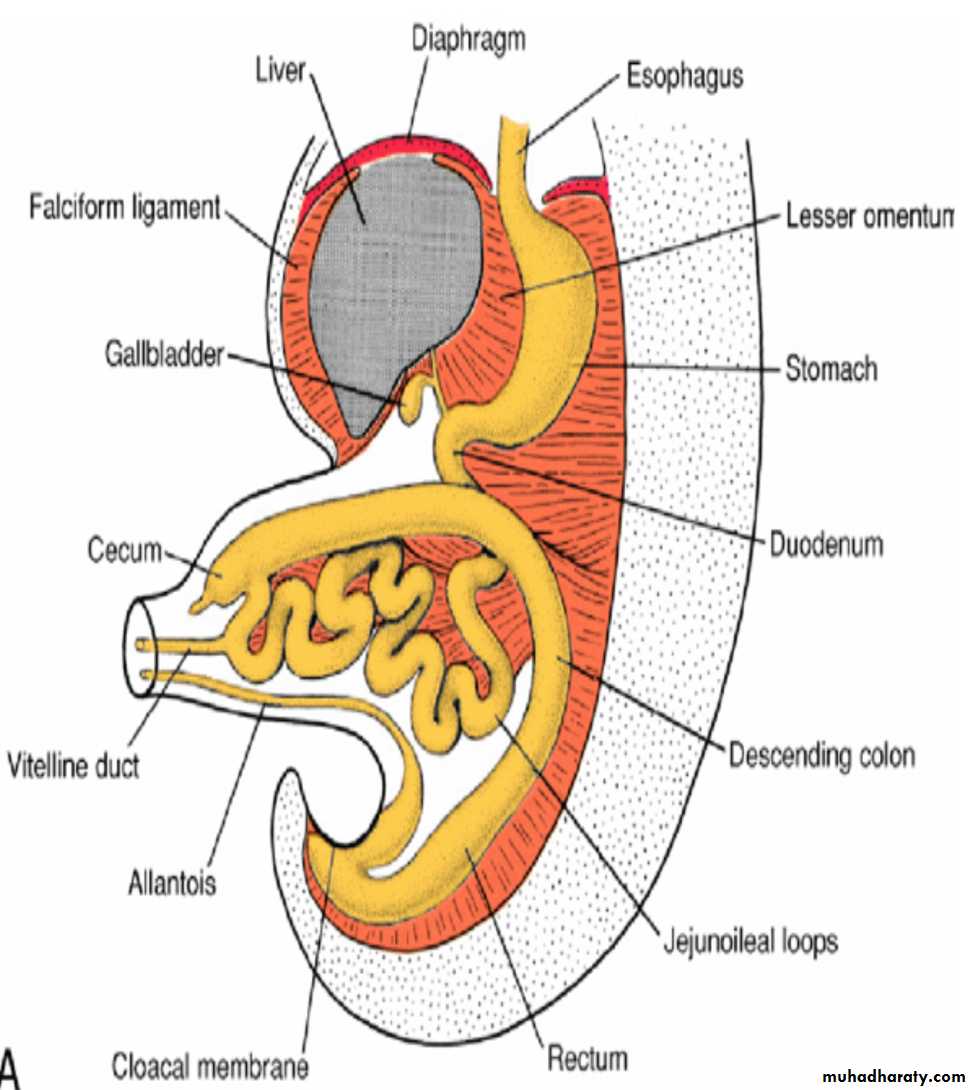
physiological umbilical herniation
is due torapid elongation, particularly of the cephalic limb &
rapid growth and expansion of the liver
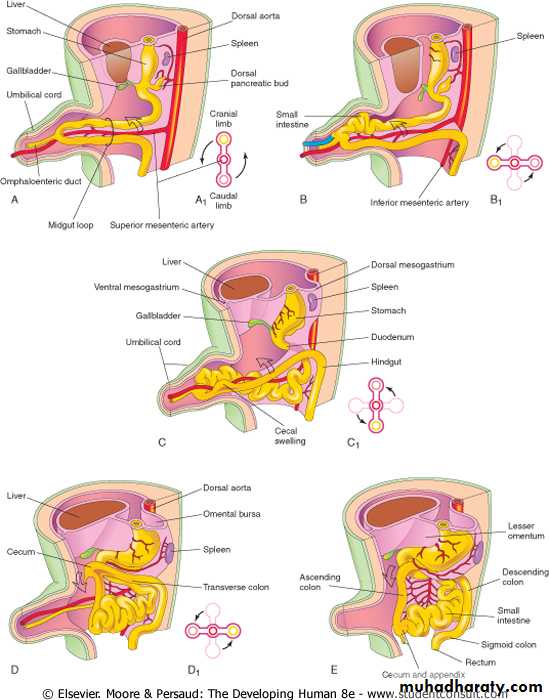
Rotation of the Midgut
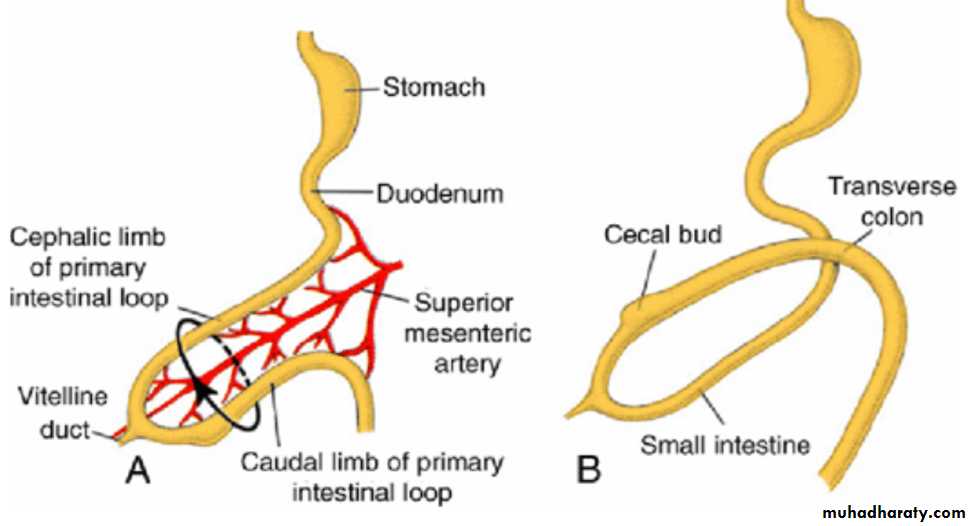
Coincident with growth in length, the primary intestinal loop rotates around an axis formed by the superior mesenteric artery
When viewed from the front, this rotation is counterclockwise, and it amounts to approximately 270° when it is complete
Even during rotation, elongation of the small intestinal loop continues, and the jejunum and ileum form a number of coiled loops
The large intestine likewise lengthens considerably but does not participate in the coiling phenomenon.
Rotation occurs during herniation (about 90°), as well as during return of the intestinal loops into the abdominal cavity (remaining 180°)
Retraction of Herniated Loops
During the 10th week, herniated intestinal loops begin to return to the abdominal cavity.It is thought that the following play important roles in this retraction
regression of the mesonephric kidney,
reduced growth of the liver, and
expansion of the abdominal cavity.
Retraction of Herniated Loops
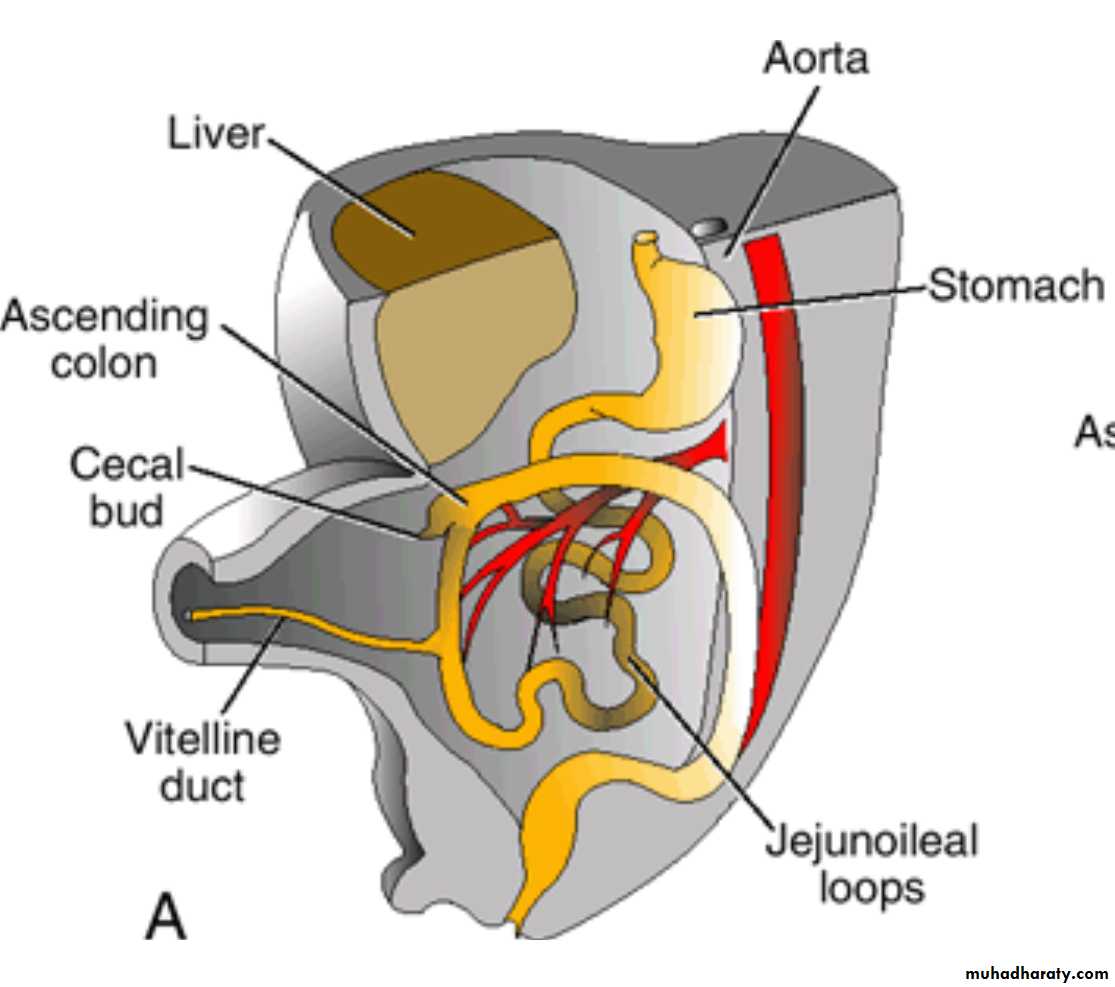
The proximal portion of the jejunum, the first part to reenter the abdominal cavity, comes to lie on the left side (The later returning loops gradually settle more and more to the right.
The cecal bud, which appears at about the sixth week as a small conical dilation of the caudal limb of the primary intestinal loop, is the last part of the gut to reenter the abdominal cavity.
Temporarily, the cecal bud lies in the right upper quadrant directly below the right lobe of the liver .
From here, it descends into the right iliac fossa, placing the ascending colon and hepatic flexure on the right side of the abdominal cavity
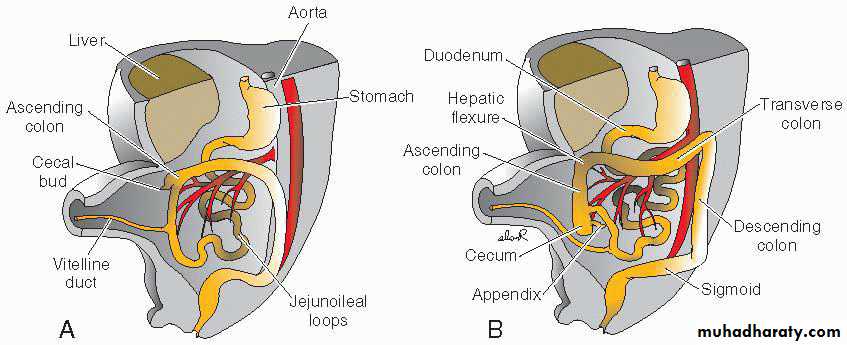
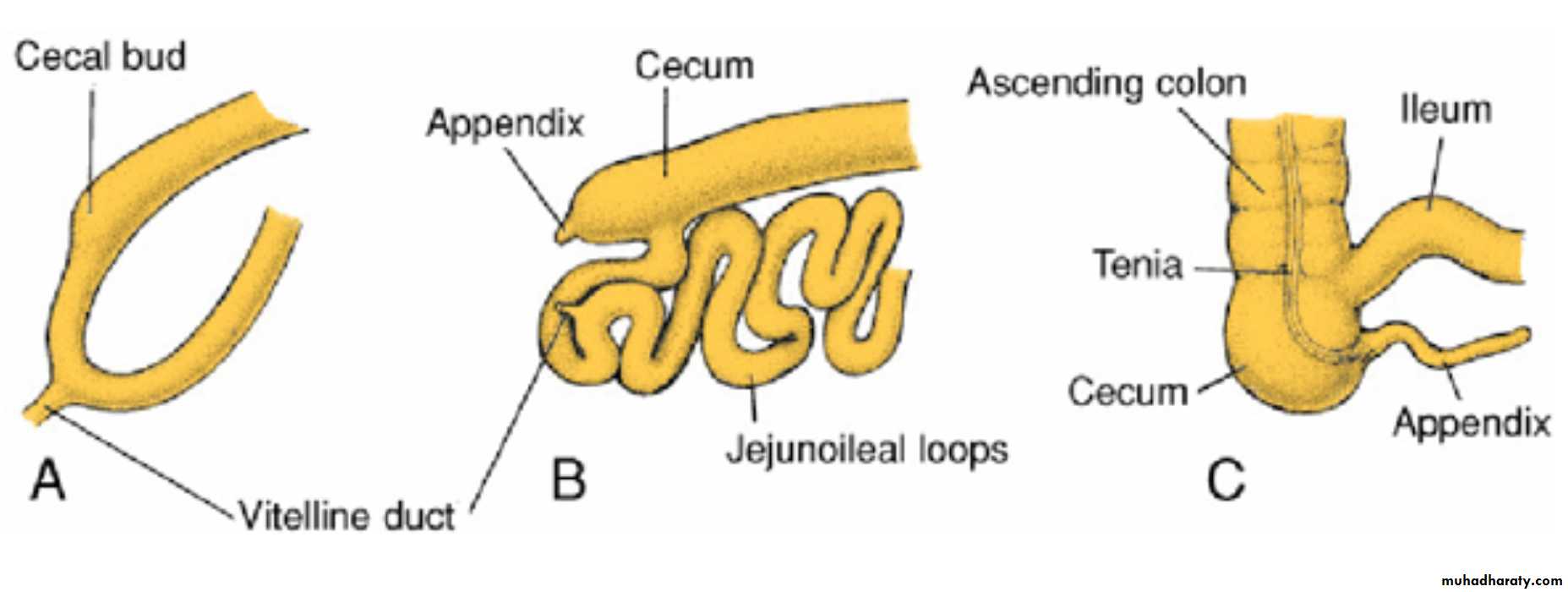
During this process the distal end of the cecal bud forms a narrow diverticulum, the appendix.
Since the appendix develops during descent of the colon, its final position frequently is posterior to the cecum or colon )retrocecal or retrocolic, respectively)
Various positions of the appendix
In about 50% of cases, the appendix is retrocecal or retrocolic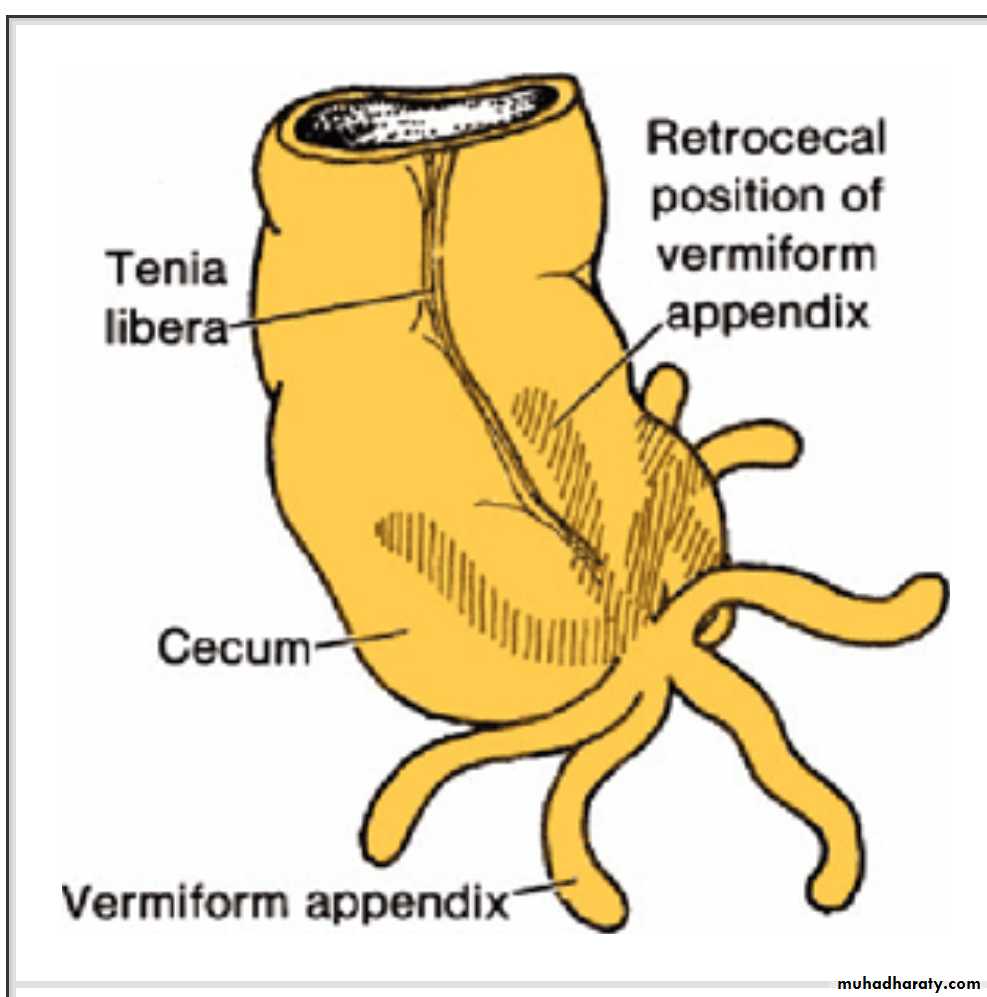
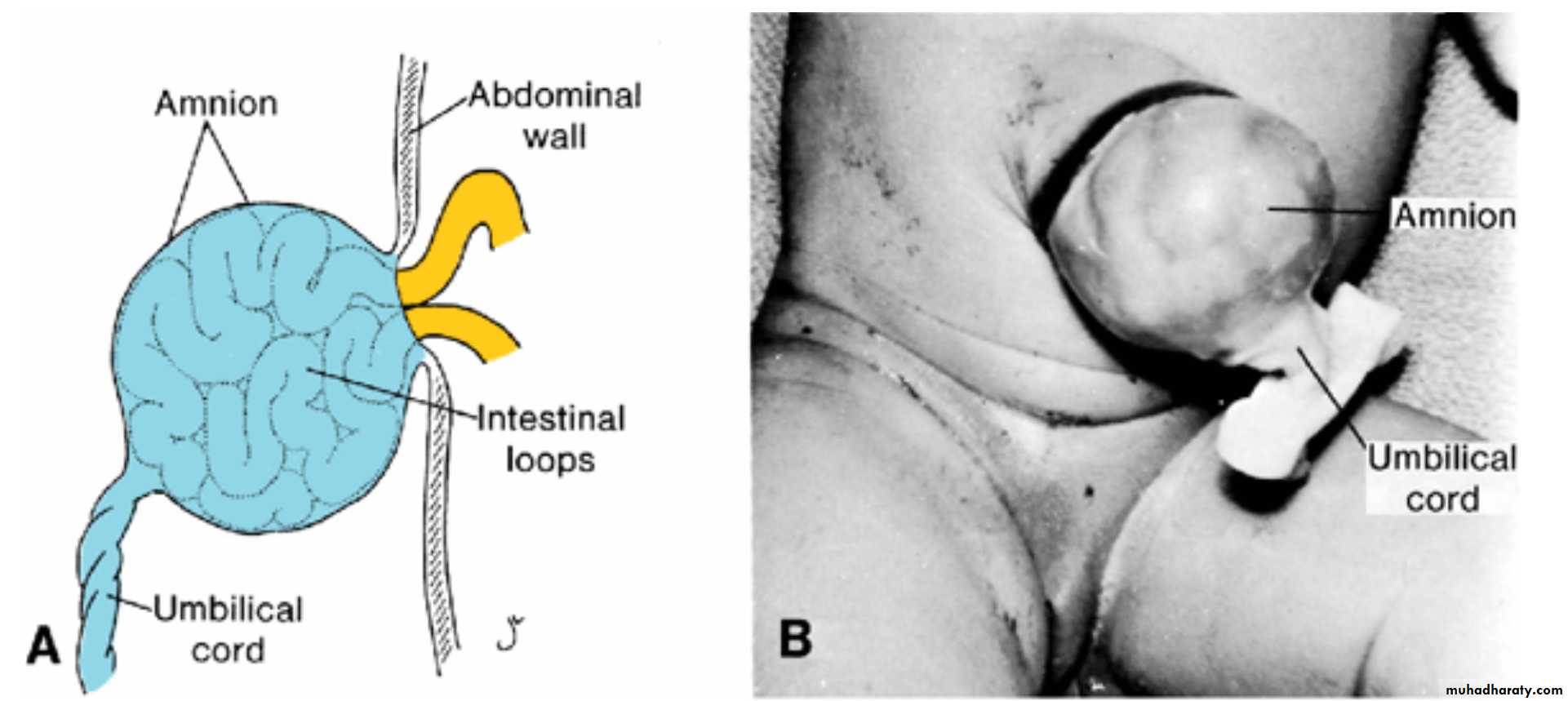
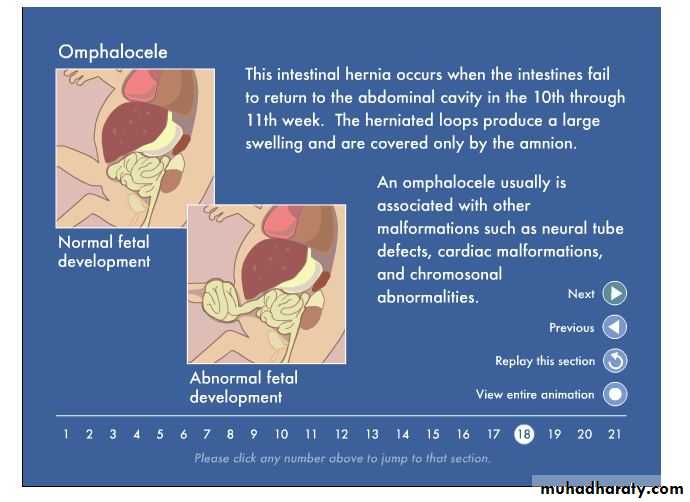
Omphalocele
failure of the intestinal loops to return to the body cavity after physiological herniation.The herniated loops are covered by amnion
is associated with a high rate of mortality and severe malformations, such as cardiac anomalies and neural tube defects .
Approximately 15% of live-born infants with omphalocele have chromosomal abnormalities.
Gastroschisis
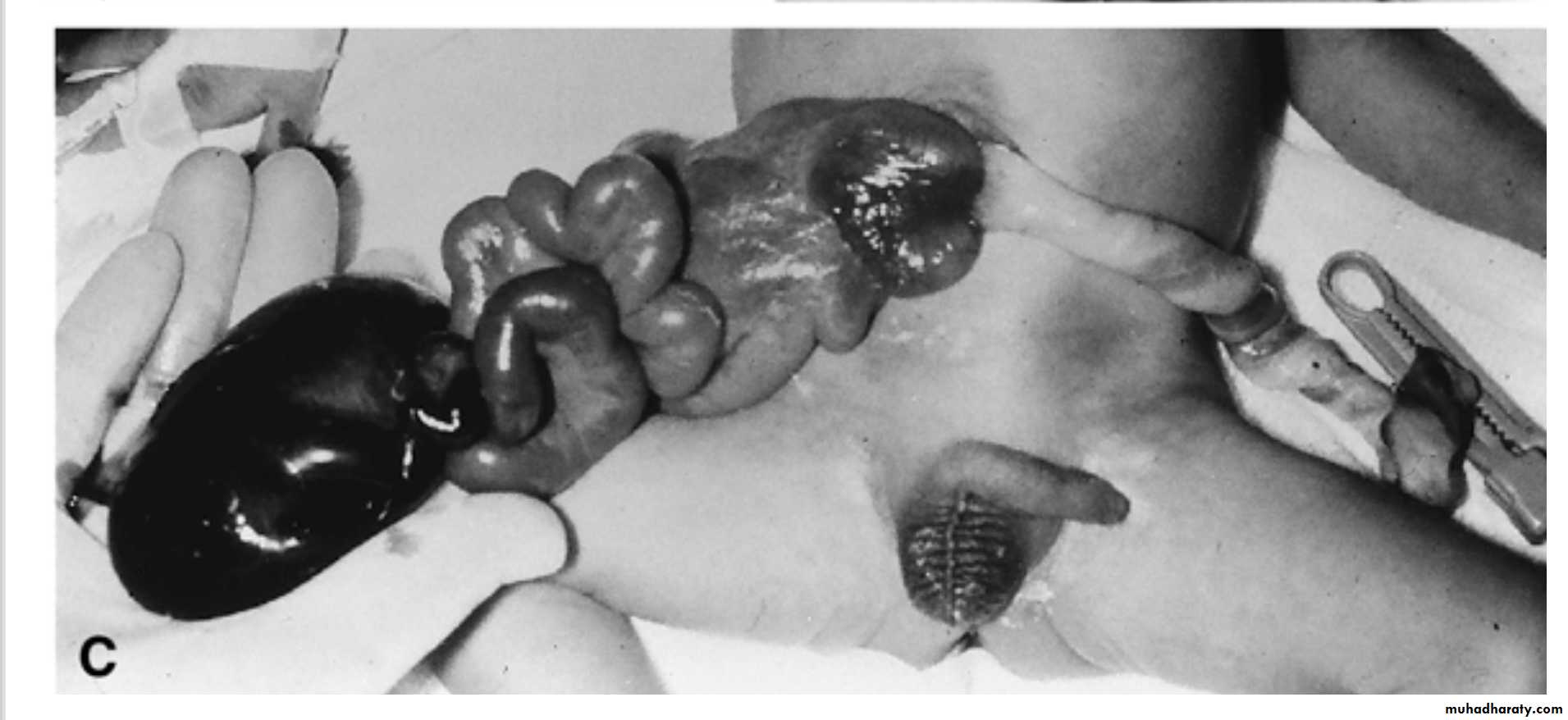
Loops of bowel return to the body cavity but herniate again through the body wall, usually to the right of the umbilicus in the region of the regressing right umbilical vein. Unlike omphalocele, the defect is not covered by amnion.
gastroschisis is not associated with chromosome abnormalities or other severe defects, so the survival rate is excellent
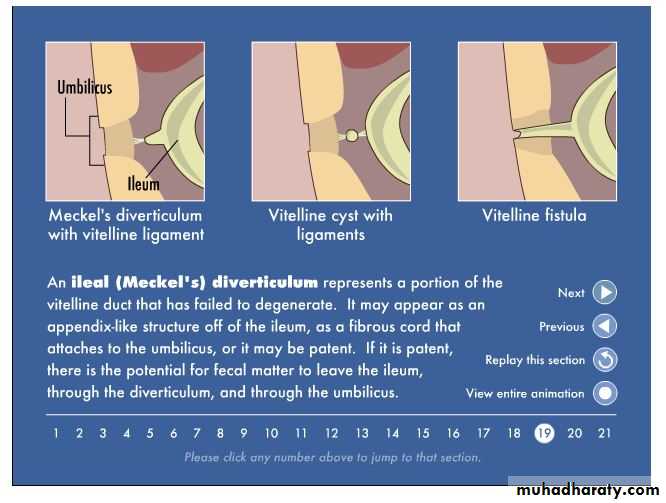
Remnants of the vitelline duct
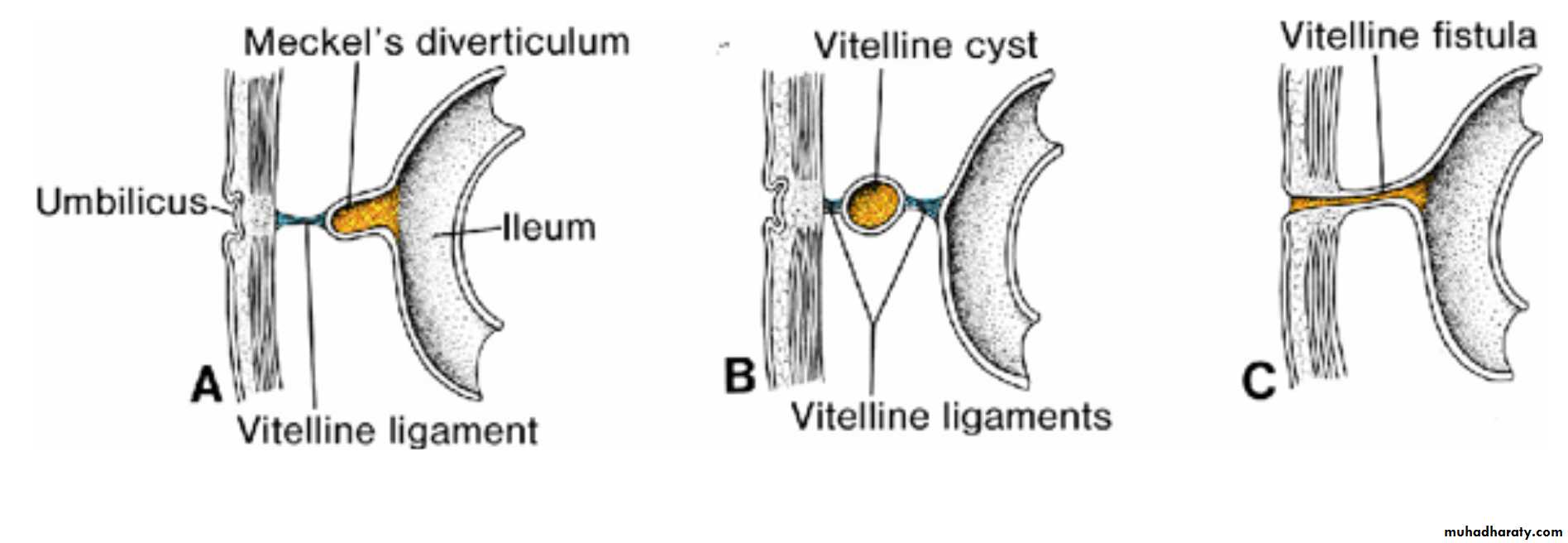
Meckel's, or ileal, diverticulum combined with fibrous cord (vitelline ligament).
B. Vitelline cyst attached to the umbilicus and wall of the ileum by vitelline ligaments.
C. Vitelline fistula connecting the lumen of the ileum with the umbilicus.
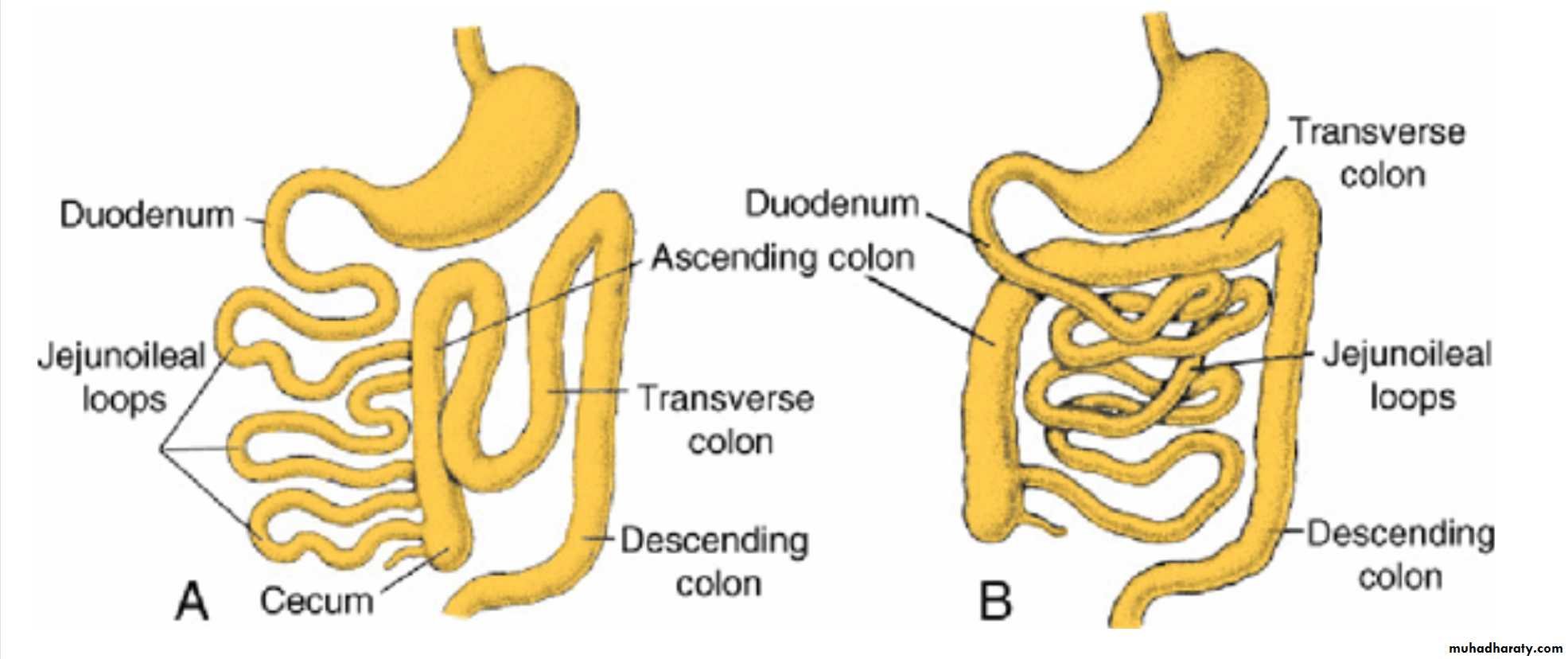
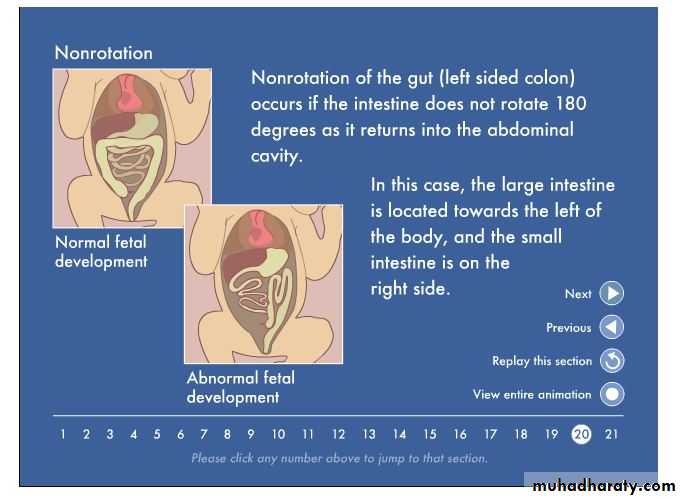
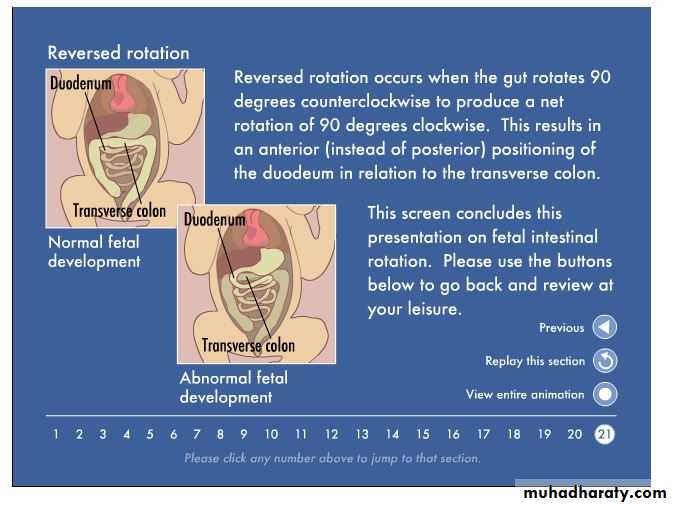
Abnormal rotation of the primary intestinal loop
(A) The colon is on the left side of the abdomen, and the small intestinal loops are on the right. The ileum enters the cecum from the right.(B) The primary intestinal loop is rotated 90° clockwise (reversed rotation). The transverse colon passes behind the duodenum.
Atresias and stenoses
may occur anywhere along the intestine. Most occur in the duodenum, fewest occur in the colon, and equal numbers occur in the jejunum and ileumMost are caused by vascular accidents; those in the upper duodenum may be caused by a lack of recanalization.
Atresias (A – C) occur in 95% of cases, and stenoses (D), in only 5%.
In 50% of cases a region of the bowel is lost(A), and in 20% a fibrous cord remains (B).In another 20%, there is narrowing, with a thin diaphragm separating the larger and smaller pieces of bowel
Stenoses and multiple atresias account for the remaining 10% of these defects, with a frequency of 5% each
Hindgut
The hindgutgives rise to the distal third of the transverse colon, the descending colon, the sigmoid, the rectum, and the upper part of the anal canal.
Its endoderm also forms the internal lining of the bladder and urethra
Cloaca
The terminal portion of the hindgut enters into the posterior region of the cloaca, the primitive anorectal canal;the allantois enters into the anterior portion, the primitive urogenital sinus .
The cloaca itself is an endoderm-lined cavity covered at its ventral boundary by surface ectoderm. This boundary between the endoderm and the ectoderm forms the cloacal membrane
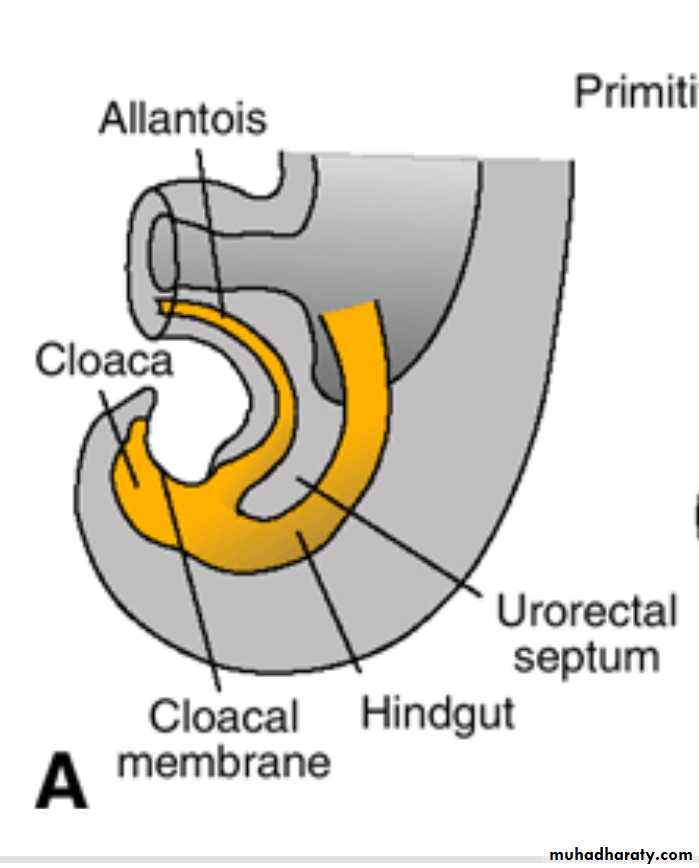
Urorectal septum
A layer of mesoderm, the Urorectal septum, separates the region between the allantois and hindgut. This septum is derived from the merging of mesoderm covering the yolk sac and surrounding the allantois .As the embryo grows and caudal folding continues, the tip of the urorectal septum comes to lie close to the cloacal membrane, although the two structures never make contact .
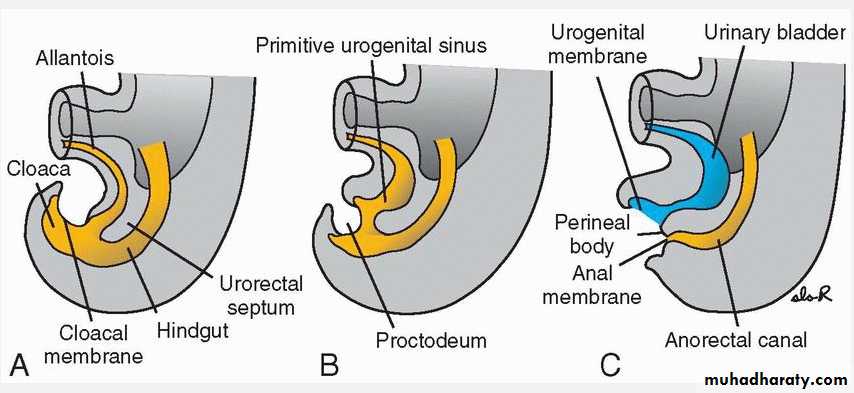
Rupturing of cloacal membrane
At the end of the seventh week, the cloacal membrane ruptures, creating the anal opening for the hindgut and a ventral opening for the urogenital sinus.Between the two, the tip of the urorectal septum forms the perineal body
At the end of 7th week , proliferation of ectoderm closes the caudalmost region of the anal canal. During the ninth week, this region recanalizes.
Thus:
the caudal part of the anal canal originates in the ectoderm, and it is supplied by the inferior rectal arteries, branches of the internal pudendal arteries.
The cranial part of the anal canal originates in the endoderm and is supplied by the superior rectal artery, a continuation of the inferior mesenteric artery, the artery of the hindgut.
The junction between the endodermal and ectodermal regions of the anal canal is delineated by the pectinate line, just below the anal columns. At this line, the epithelium changes from columnar to stratified squamous epithelium.
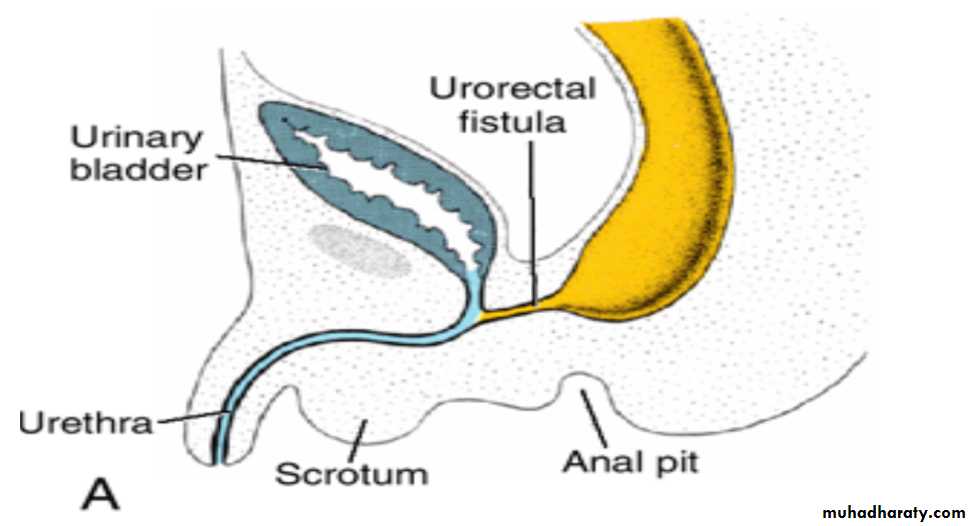
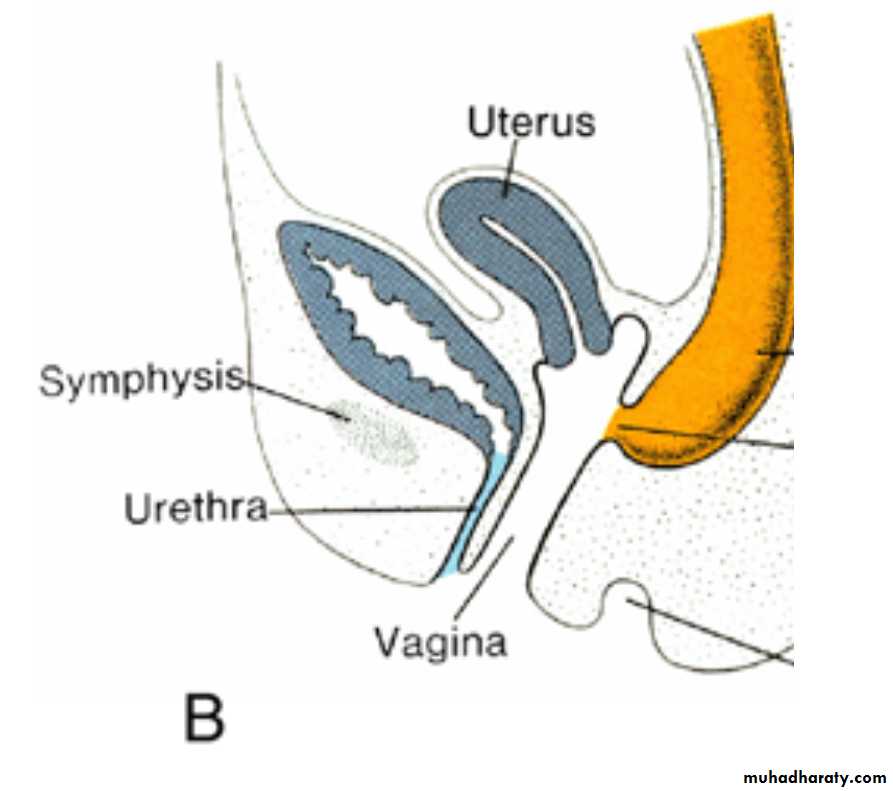
Rectourethral and rectovaginal fistulas
Rectourethral (A) and rectovaginal (B) fistulas that result from incomplete separation of the hindgut from the urogenital sinus by the urorectal septum.These defects may also arise if the cloaca is too small, which causes the opening of the hindgut to shift anteriorly.
Rectoanal atresias
Rectoperineal fistula (rectoanal atresia). These defects probably result from vascular accidents involving the caudal region of the hindgut, resulting in atresias and fistulas.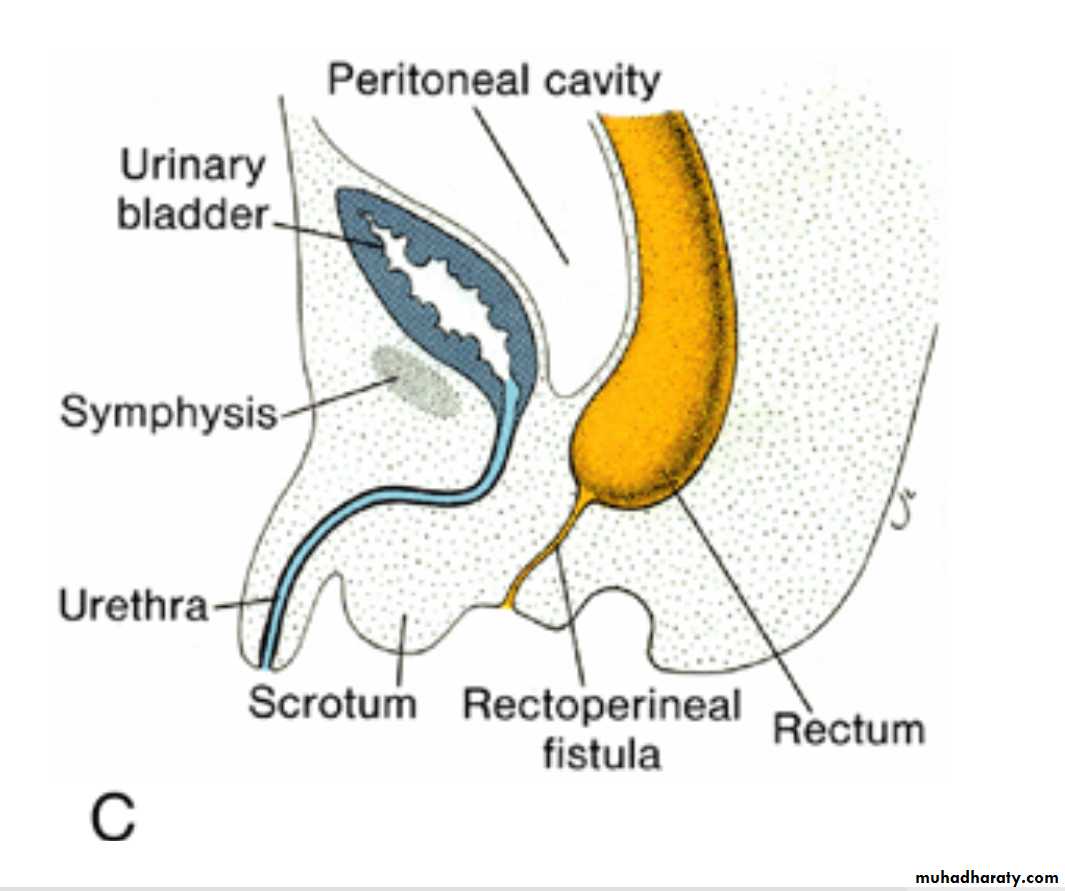
Imperforate anus
resulting from failure of the anal membrane to break down.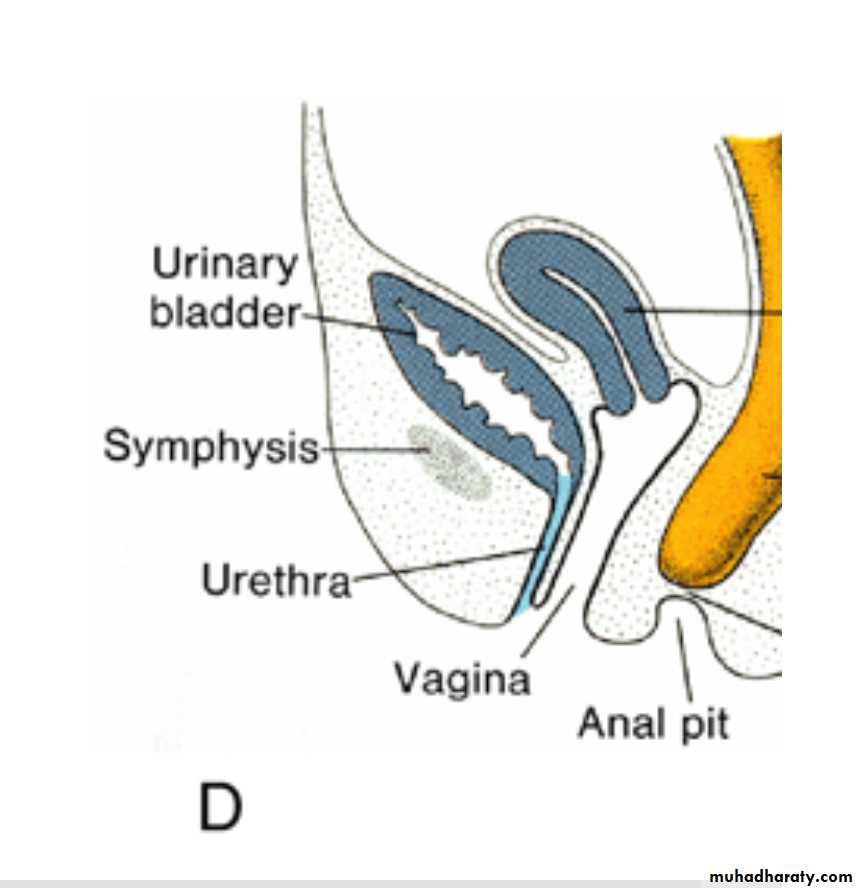
Congenital megacolon(aganglionic megacolon or Hirschsprung disease)
is due to an absence of parasympathetic ganglia in the bowel wall .These ganglia are derived from neural crest cells that migrate from the neural folds to the wall of the bowel.