Dr. Jabar Etaby Lecture one
GIARDIASIS (lambliasis)
Etiology: Giardia lamblia (flagellate)
Epidemiology: It has worldwide distribution and is not uncommon in South Carolina.
It is the most frequent protozoan intestinal disease in the US and the most common
identified cause of water-borne disease associated with breakdown of water
purification systems, outdoorsmanship, travel to endemic areas (Russia, India,
Rocky Mountains, etc.) and day care centers.
Morphology:
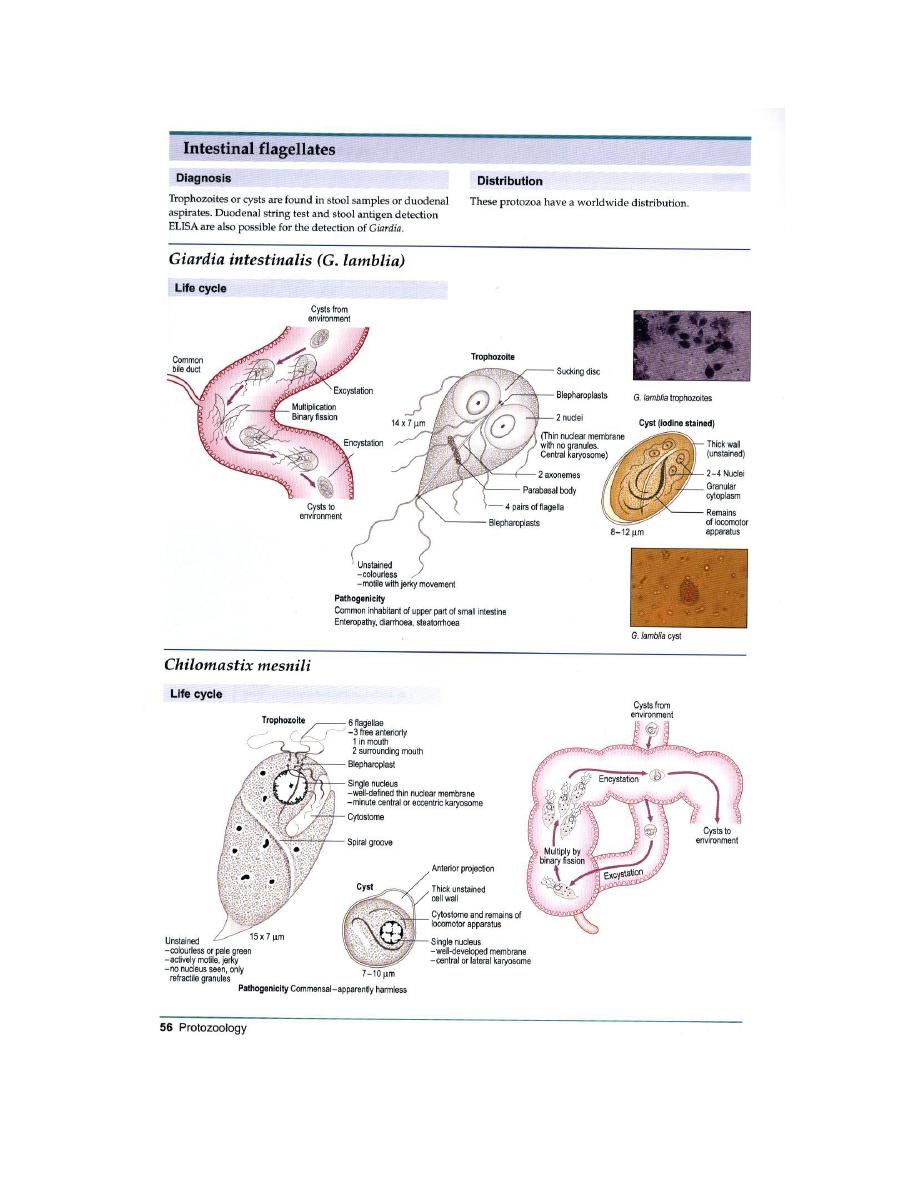
Trophozoite: It is12-15 µ, half pear shaped with 8 flagella and, 2 axostyles arranged
in a bilateral symmetry. There are two anteriorly located large suction discs. The
cytoplasm contains two 2 nuclei and two parabasal bodies (Figure 7).
Cyst: Giardia cysts are 9-12 µ ellipsoidal body with smooth well-defined wall. The
cytoplasm contains 4 nuclei and many structures of the trophozoite.
Life cycle : Infection occurs by ingestion of cysts, usually in contaminated
water. Decystation occurs in duodenum and trophozoites (trophs) colonize the
upper small intestine where they may swim freely or attach to the sub-mucosal
epithelium via the ventral suction disc. The free trophozoites encyst as they move

down stream and mitosis takes place during the encystment. The cysts are passed
in the stool. Man is the primary host although beavers, pigs and monkeys are also
infected and serve as reservoirs.
Life cycle of Giadia lamblia. Infection occurs by the ingestion
of cysts in contaminated water or food. In the small intestine,
excystation releases trophozoites that multiply by longitudinal
binary fission. The trophozoites remain in the lumen of the
proximal small bowel where they can be
Free or attached to the mucosa by a ventral sucking disk.
Encystation occurs when the parasites transit toward the
colon, and cysts are he stage found in normal (non diarrheal)
feces. The cysts are hardy, can survive several months in cold
water, and are responsible or transmission. Because the cysts
are infectious when passed in the stool or shortly afterward,
person-to-person transmission is possible. While animals are
infected with Giardia, their importance as a reservoir is unclear
Figure 6

Symptoms: The early symptoms include flatulence, abdominal distension, nausea
and foul-smelling bulky, explosive, often watery, diarrhea. The stool contains
excessive lipids but very rarely any blood or necrotic tissue. The more chronic stage
is associated with vitamin B
12
malabsorption, disaccharidase deficiency and lactose
intolerance.
Pathogenesis
The mechanisms by which
Giardia
causes diarrhea and
malabsorption have not been elucidated. There is no evidence that
Giardia
produces an enterotoxin or that it invades the intestinal
epithelial cells. Electron microscopy shows that the ventral disk
embeds the parasite into the epithelial microvillus layer and
“footprints” of formerly adherent trophozoites are visible on the
epithelial cell surface. However, even in a heavy infection, the surface
area covered and possibly damaged by the adherent trophozoites
cannot account for the symptoms. In humans, biopsy of the infected
gut shows little abnormality. In a European study in which over 500
biopsy specimens from
Giardia
-infected patients were observed,
slightly over 96% had normal looking mucosa and 3.7% had mild
villous shortening with a ismall amount of neutrophil and lymphocyte
infiltration. The lack of histologic abnormalities in the majority of
symptomatic patients has also been observed in other, smaller
studies. In one study in which patients with villous shortening and
inflammatory infiltration were followed with serial biopsies, these

abnormalities all resolved after the infection was eradicated.
In the murine models of giardiasis, similar findings of villous atrophy
and inflammatory infiltration of villous epithelium can be observed.
However as with humans, the findings are subtle and the
inflammatory changes mild.
Giardiasis
7
In conclusion, the cause of diarrhea and malabsorption in Giardia
infection is likely to be multifactorial, involving the host immune
response to the pathogen as well as, yet to be identifi ed, cytopathic
substances that the parasite may secrete.
Additionally, it has been suggested that
Giardia
may cause pathology
by alteration of the bile content or endogenous flora of the small
intestine which in turn could
affect the absorptive function of gut. These hypotheses must now be
formally tested before a more complete picture emerges.
Diagnosis
The traditional method of diagnosis is examination of stool for
trophozoites or cysts (stool O&P). Both fresh and fixed stool
specimens are usually examined. Cysts are normally found but motile
trophozoites can be observed in a fresh specimen of loose stool .
Because the parasites are normally found in the small intestine and
are shed intermittently, the sensitivity of one stool specimen is low, in
the range of 50 - 70%. However, examination of three specimens,
from three different days, increases the sensitivity to 85 - 90%; specifi
city is close to 100%.

This assay remains the most widely used method to diagnose
Giardia
infection and is the gold standard to which other newer assays are
usually compared. It is important to note that there can be a delay
between the onset of symptoms and the excretion of cysts so that a
negative stool sample in someone in whom giardiasis is suspected
warrants reanalysis at alater time.
Recently, new assays have been developed based on detection of
Giardia
antigens. The direct fluorescent antibody test (DFA), uses a
Giardia
-specifi c antibody conjugated to a fluorophore to stain stool
specimens. Because the parasites are labeled, much larger regions
of the slide can be scanned more quickly and the likelihood
of detecting the parasite is increased. On a single stool specimen the
sensitivity is between 96 - 100%. Other antigen-detection tests detect
soluble
Giardia
-specifi c proteins in the stool. There are two different
types of soluble-antigen-detection
Covering of the epithelium by the trophozoite and flattening of the mucosal surface
results in malabsorption of nutrients.
Immunology:
Some role for IgA and IgM. Increased incidence in immunodeficiency (e.g. AIDS).

Diagnosis:
Symptoms, history, epidemiology. Distinct from other dysentery due to lack of
mucus, and blood in the stool, lack of increased PMN leukocytes in the stool and
lack of high fever. Cysts in the stool and trophs in duodenal content
obtained using a string device (Enterotest
R
). Trophs must be distinguished from the
nonpathogenic flagellate Trichomona hominis, an asymmetrical flagellate with an
undulating membrane.
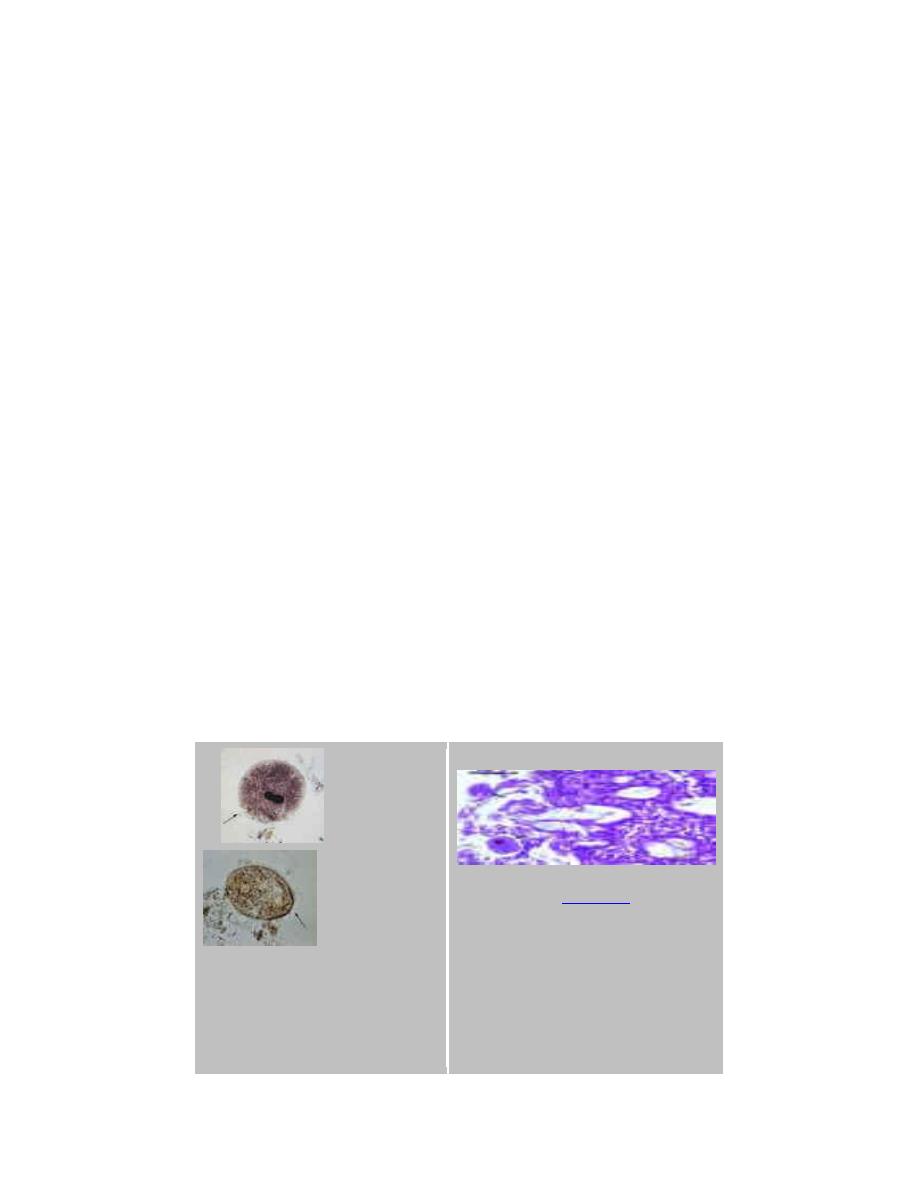
{kind=link}
Cysts of Giardia lamblia,stained
with iron- hematoxylin (A, B) and
in a wet mount (C; from a
patient seen in Haiti). Size: 8-12
µm in length. These cysts have
two nuclei each (more mature
ones will have four). CDC
{kind=link}
Giardia lamblia
{kind=link}
cyst. Chlorazol black. CDC/Dr.
George R. Healy
{kind=link}
cyst. Iodine stain. CDC
{kind=link}
Indirect fluorescent antibody
stain. Positive test.
CDC/Dr. Govinda S. Visvesvara
gsv1@cdc.gov
Giardia
{kind=link}
trophozoites in section of
intestine (H&E) ©
, Queensland University
of Technology clinical
parasitology collection. Used
with permission
{kind=link}
Indirect fluorescent antibody
stain. Negative test.
CDC/Dr. Govinda S. Visvesvara
gsv1@cdc.gov
Protozoa Infection in Human Intestine sp. (Giardia)
{kind=link}
l, University of Hawaii. Used with permission
Figure 7
Treatment: Metronidazole is the drug of choice.


Lecture Two DR. Jabar Etaby
OTHER INTESTINAL PROTOZOA
Blanatidium coli and Cryptosporidium (parvum) are both zoonotic protozoan
intestinal infections with some health significance. Isospora belli is an opportunistic
human parasite.
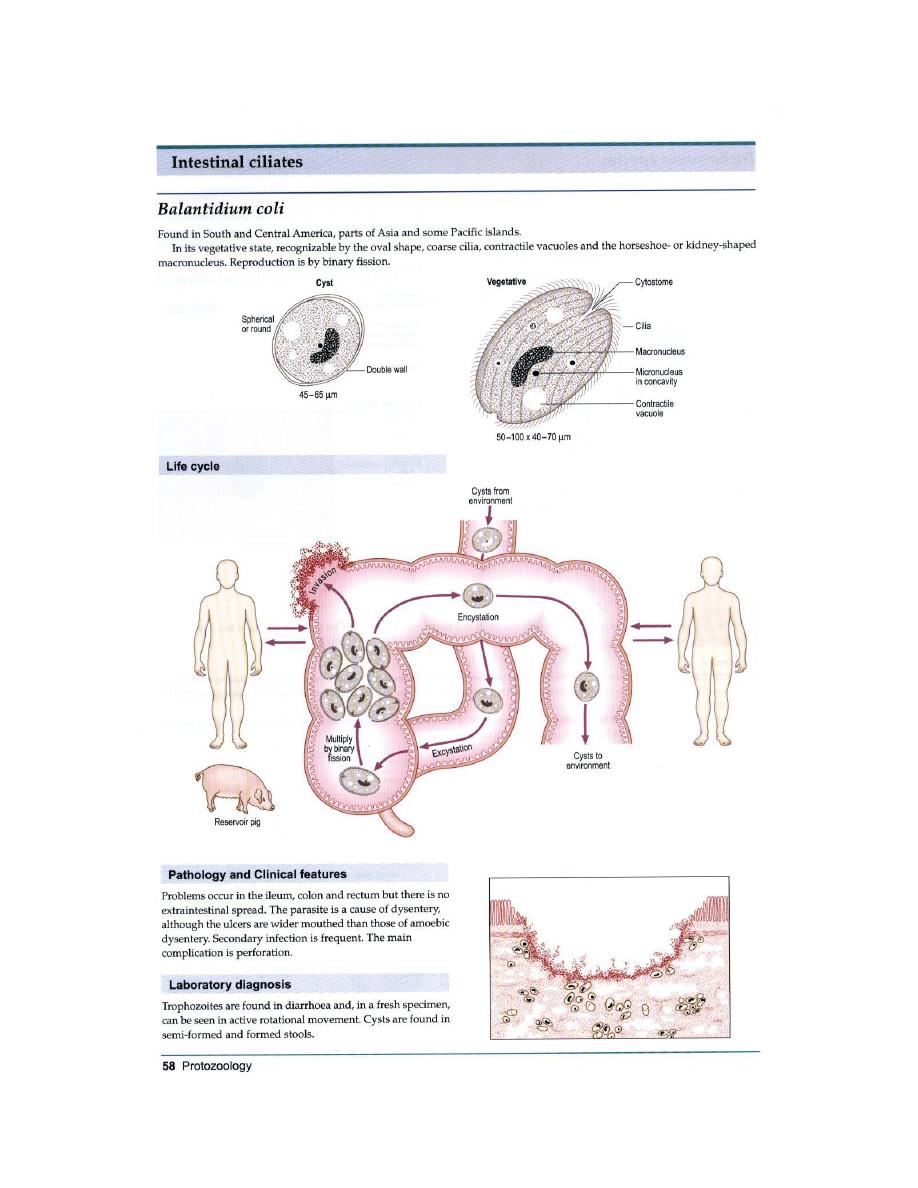
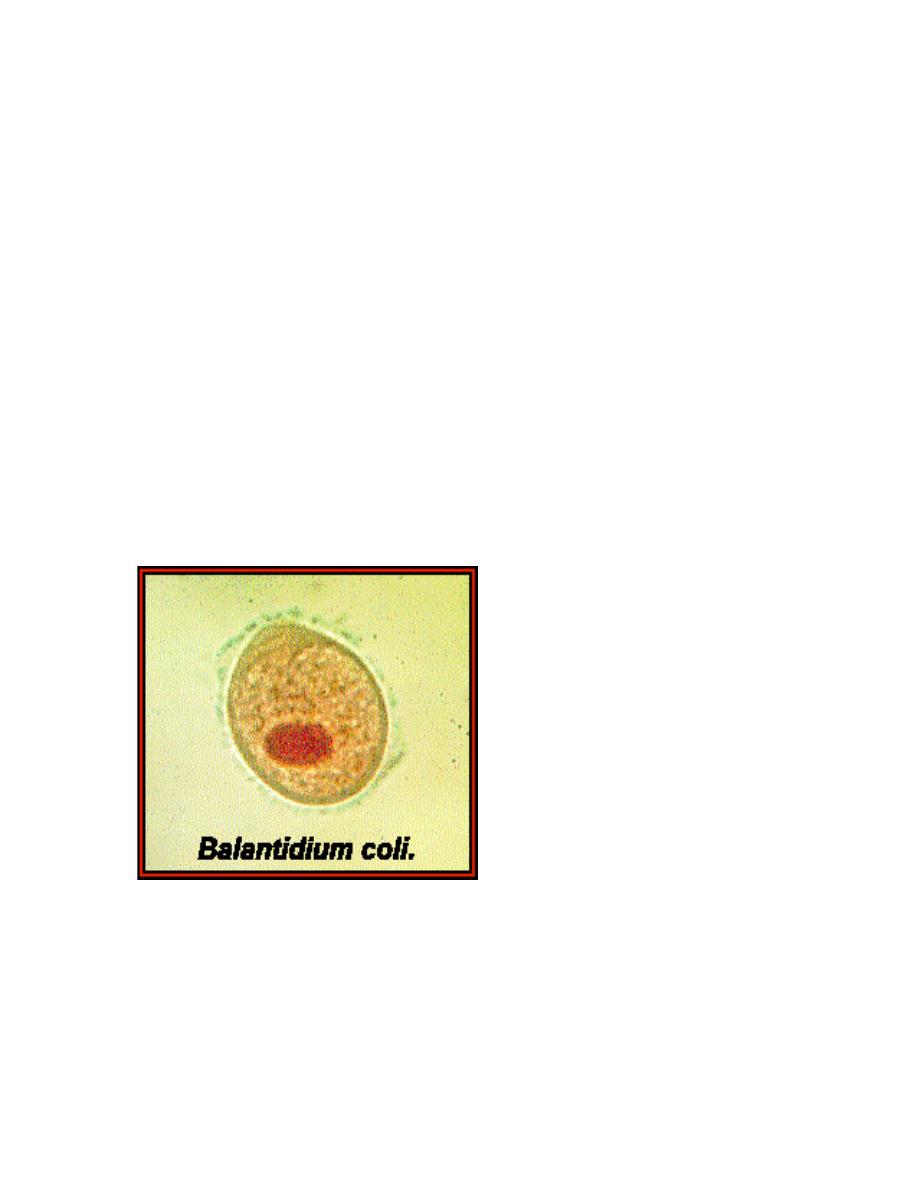
B. coli: This is a parasite primarily of cows, pigs and horses. The organism is a large
(100x60 µ) ciliate with a macro and a micronucleus (Figure 8). The infection occurs
primarily in farm workers and other rural dwellers by ingestion of cysts in fecal
material of farm animals. Man to man transmission is rare but possible. Symptoms
and pathogenesis of balantidiasis are similar to those seen in entamebiasis,
including intestinal epithelial erosion. However, liver, lung and brain abscesses are
not seen. Metronidazole and iodoquinol are effective.
A
B
{kind=link}
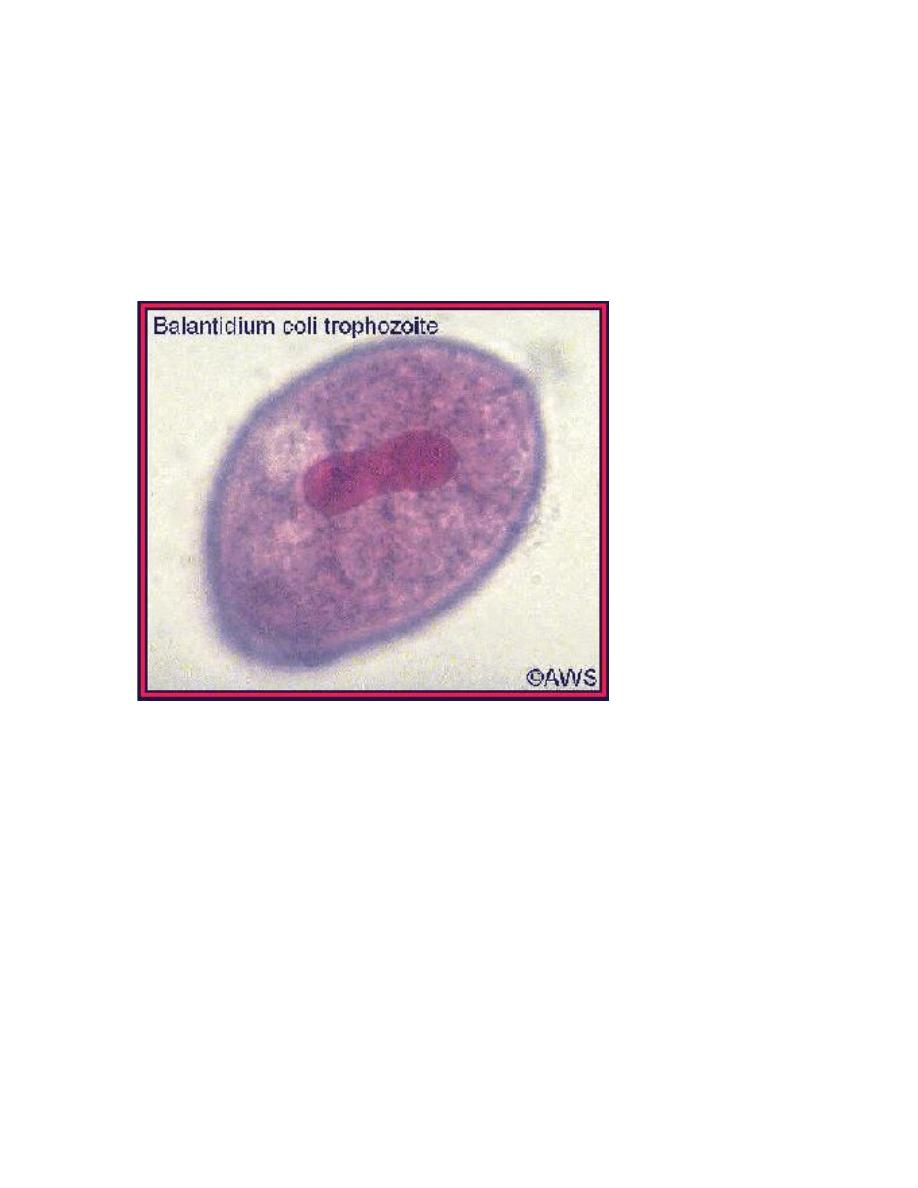
Balantidium coli
trophozoites. These
are characterized by: their
Bala
ntidium coli trophozoites in section of
intestine (H&E)
, Queensland
University of Technology clinical
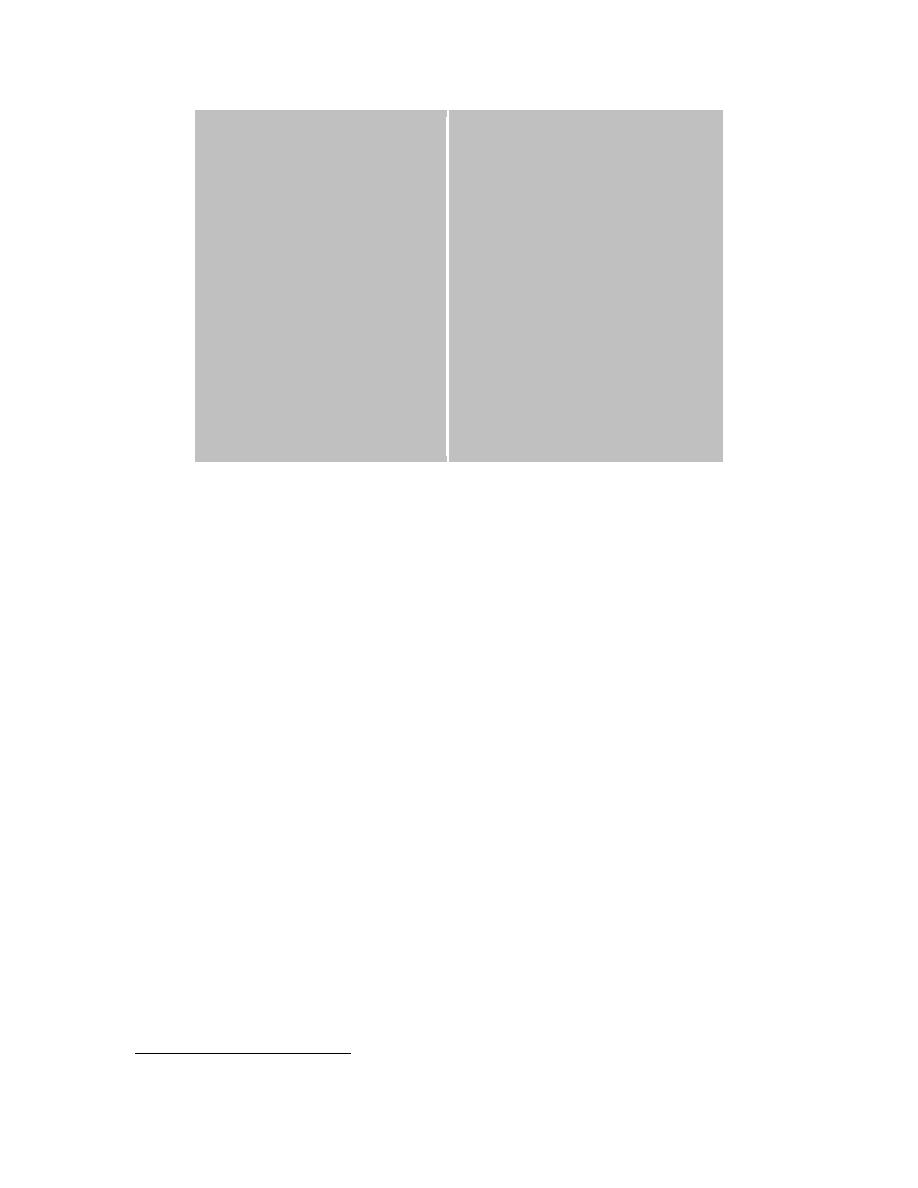
large size 40 µm to more
than 70 µm) the
presence of cilia on the cell
surface – particularly visible
in (B) a cytostome
(arrows) a bean shaped
macronucleus which is often
visible - see (A), and a
smaller, less conspicuous
micronucleus CDC
1
Balantidium coli
Balantidium coli is a parasite of many species of animals, including pigs,
rats, guinea pigs, humans, and many other
animals. It appears that the parasite can be transmitted readily among these
species, providing the appropriate conditions
are met (i.e., fecal contamination). Humans are infected when they ingest
cysts via food or water contaminated with fecal
material. In many respects this parasite resembles
Entamoeba histolytica
---
an important difference that can have a
1
significant impact of epidemiology is that trophozoites of B. coli will encyst
after being passed in stools, trophs of E.
histolytica will not. In humans this parasitic species resides most often in the
large intestine, and it can invade the mucosa
(or invade lesions caused by other organisms) causing serious pathology.
Ectopic (extra-intestinal) infections can also
occur. You can view a diagram of the life cycle
here
.
A trophozoite