RICKITS
Rickets is defined as decreased or defective bone mineralization in growing children.Osteomalacia is the same condition in adults.
Pathophysiology:
Bone consists of a protein matrix called osteoid and a mineral phase, principally composed of calcium and phosphate.
Rickets is a disease of growing bone that is caused by unmineralized matrix at the growth plates and occurs in children only before fusion of the epiphyses. Because growth plate cartilage and osteoid continue to expand but mineralization is inadequate, the growth plate thickens. There is also an increase in the circumference of the growth plate and the metaphysis, increasing bone width at the location of the growth plates and causing some of the classic clinical manifestations, such as widening of the wrists and ankles.
There is a general softening of the bones that causes them to bend easily when subject to forces such as weight bearing or muscle pull. This softening leads to a variety of bone deformities.
Etiology:
VITAMIN D DISORDERS
Nutritional vitamin D deficiency
Congenital vitamin D deficiency
Secondary vitamin D deficiency
Malabsorption
Chronic kidney disease
CALCIUM DEFICIENCY
Low intake
Premature infants (rickets of prematurity)
Malabsorption
Dietary inhibitors of calcium absorption
PHOSPHORUS DEFICIENCY
Inadequate intake
Premature infants (rickets of prematurity)
Aluminum-containing antacids
RENAL LOSSES
RTA
X-linked hypophosphatemic rickets
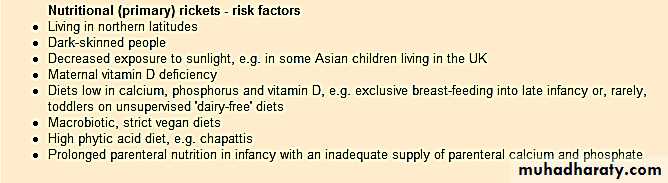
Risk factors for vitamin D deficiency
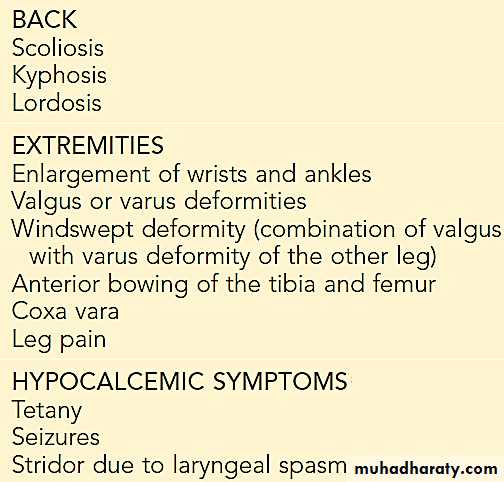
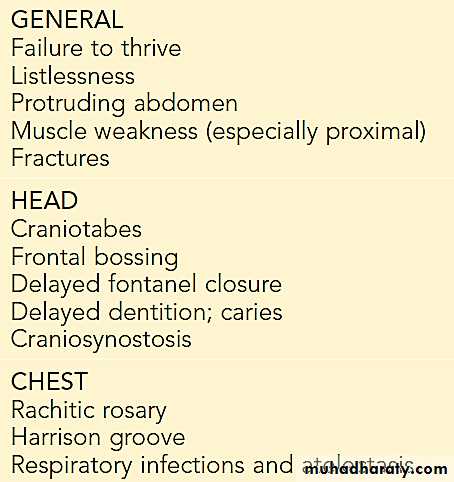
Clinical Features of Rickets
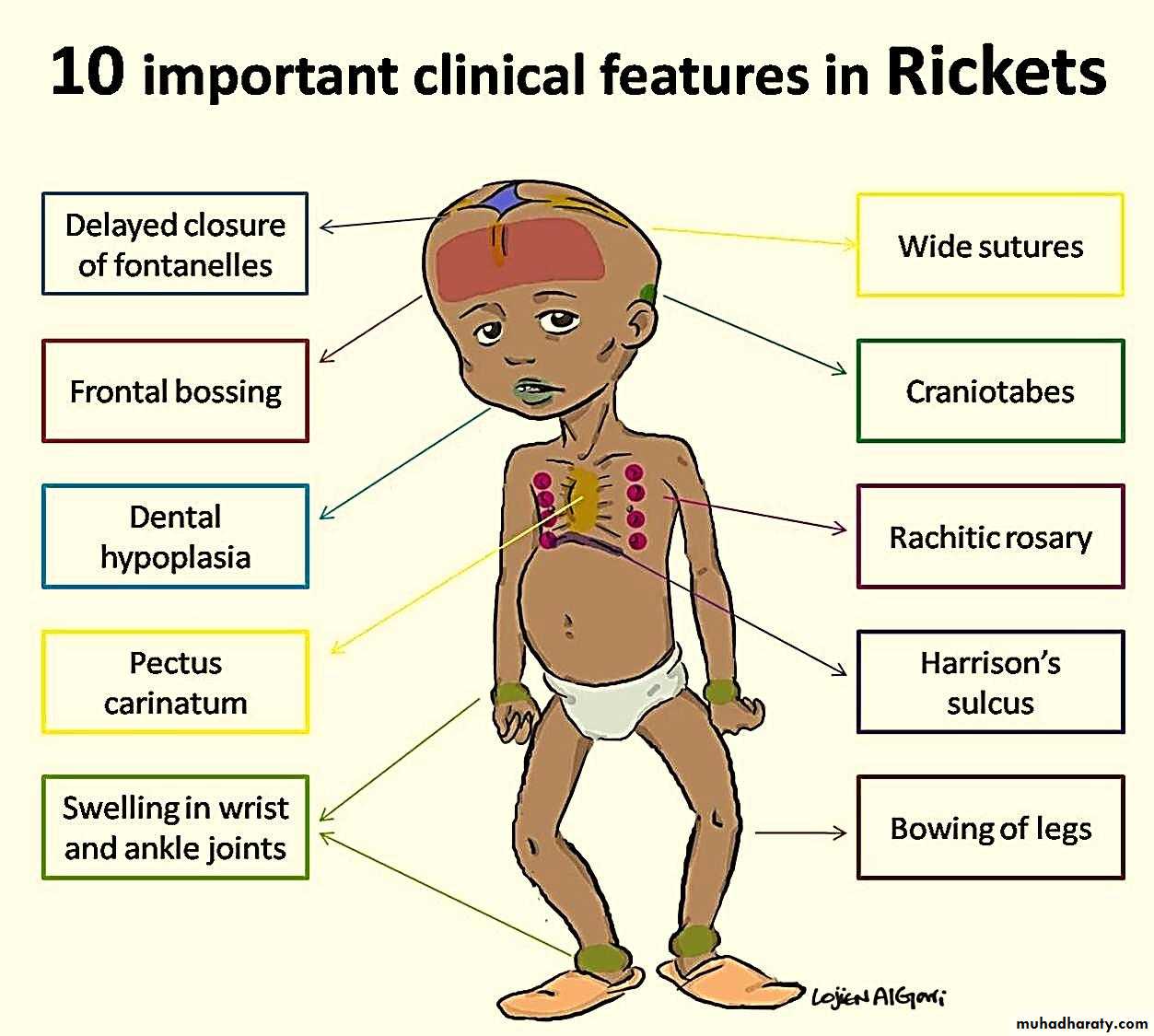
Craniotabes (softening of the cranial bones and can be detected by applying pressure at the occiput or over the parietal bones. The sensation is similar to the feel of pressing into a Ping-Pong ball and then releasing)

Diagnosis
Most cases of rickets are diagnosed based on the presence of classic radiographic abnormalities.The diagnosis is supported by physical examination findings and a history.
Laboratory test results that are consistent with a specific etiology.
Laboratory Tests
The initial laboratory tests in a child with rickets should include:
Serum calcium.
Serum phosphorus.
Alkaline phosphatase.
PTH.
25-hydroxyvitamin D.
1,25-dihydroxyvitamin D.
Creatinine.
Electrolytes
urinary excretion of calcium & inorganic phosphorus

Treatment
Children with nutritional vitamin D deficiency should receive vitamin D and adequate nutritional intake of calcium and phosphorus (usually provided by milk, formula, and other dairy products).There are 2 strategies for administration of vitamin D:
Stoss therapy, 300,000-600,000 IU of vitamin D are administered orally or intramuscularly as 2-4 doses over 1 day. Stoss therapy is ideal in situations where adherence to therapy is questionable.
The alternative is daily, high-dose vitamin D, with doses ranging from 2,000-5,000 IU/day over 4-6 wk.
Either strategy should be followed by daily vitamin D intake of:
400 IU/day if <1 yr old.
600 IU/day if >1 yr old.
Children who have symptomatic hypocalcemia: might need intravenous calcium acutely, followed by oral calcium supplements, which typically can be tapered over 2-6 wk in children who receive adequate dietary calcium.