PUJO& mega ureters
Dr.Mohammed BassilPelviureteric junction (PUJ)obstruction
A ureteropelvic junction (UPJ) obstruction can be thought of as a restriction to flow of urine, from the renal pelvis to the ureter, which, if left uncorrected, will lead to progressive renal deterioration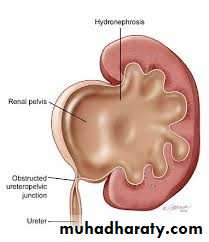
UPJ obstruction occurs in all pediatric age groups, but there tends to be a clustering in the neonatal period because of the detection of antenatal hydronephrosis and again later in life because of symptomatic occurrence. At one point about 25% of cases were discovered within the first year of life.
UPJ obstruction is the most common cause of significant dilation of the collecting system in the fetal kidney.
Pelviureteric junction (UPJ)obstruction
Pelviureteric junction (PUJ)obstruction
Obstruction occurs more commonly in boys than in girls.Left-sided lesions predominate, particularly in the neonate (approximately 67%).
Bilateral UPJ obstruction is present in 10% to 40% of cases.
and it has been known to affect members of more than one generation.
ETIOLOGY
Intrinsic:
interruption in the development of the circular musculature of the UPJ.
or an alteration of the collagen fibers and composition between and around the muscle cells (The muscle fibers become widely separated and attenuated, leading to a functional discontinuity of the muscular contractions and ultimately to insufficient emptying) .
a significant increase in the lamina muscularis and in the number of inner longitudinal muscular bundles of the UPJ complex of obstructed kidneys in infants younger than 1 year of age, compared with age-matched normal infants
ETIOLOGY
valvular mucosal folds.persistent fetal convolutions .
upper ureteral polyps.
Such folds that does not flatten out when the ureter is distended or stretched.
"östling's folds" are now considered folds that are not obstructive and disappear with a person's lineargrowth they are rarely seen in an older child or adult.ETIOLOGY
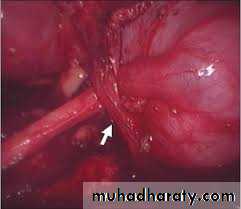
Extrinsic:An aberrant, accessory, or early-branching lower-pole vessel is the most common cause of extrinsic UPJ obstruction. These vessels pass anteriorly to the UPJ or proximal ureter and contribute to mechanical obstruction.
ETIOLOGY
an aberrant or accessory renal artery to the lower pole of the kidney is present and the ureter courses behind it, the ureter may angulate at both the UPJ and the point at which it traverses over the vessel as the pelvis fills and bulges anteriorly. Further angulation of the ureter occurs as it becomes adherent to the UPJ secondary to an inflammatory process. A two-point obstruction ensues, with kinking of the ureter at the UPJ and at the point where the ureter drapes over the vessel.
Secondary Ureteral Pelvic Junction Obstruction
UPJ obstruction may also be seen with severe vesicoureteral reflux (VUR); these conditions coexist in 10% of cases. The ureter elongates and develops a tortuous course in response to the obstructive element of reflux. A kink may develop in the UPJ area, a point of relative fixation, and may cause obstruction secondarily . In such a situation the obstructive lesion needs to be corrected initially, even though the VUR contributed to the initial problem.Associated Anomalies
UPJ obstruction is the most common anomaly encountered in the opposite kidney; it occurs in 10% to 40% of cases.Renal dysplasia and multicystic dysplastic kidney are the next most frequently observed contralateral lesions.
In addition, unilateral renal agenesis has been noted in almost 5% of children.
UPJ obstruction may also occur in either the upper or the lower half (usually the latter) of a duplicated collecting system,or of a horseshoe or ectopic kidney.
VUR has been found in as many as 40% of affected children.
UPJ obstruction was noted in 21% of children with the VATER (vertebral defects, imperforate anus, tracheoesophageal fistula, and radial and renal dysplasia) association.
PRESENTATION
most infants are asymptomatic and most children are discovered because of their symptoms. infants were discovered to have UPJ obstruction because of a palpable mass.infants who present with failure to thrive, feeding difficulties, sepsis secondary to urinary tract infection, or pain or hematuria related to nephrolithiasis. Urinary tract infection is the presenting sign in 30% of affected children beyond the neonatal period.
PRESENTATION
In the older child, episodic flank or upper abdominal pain, sometimes associated with nausea and vomiting due to intermittent UPJ obstruction, is a prominent symptom.cyclic vomiting alone is caused by intermittent UPJ obstruction.
Hematuria, which is seen in 25% of children, may occur after minor abdominal trauma.
This hematuria is believed to be caused by disruption and rupture of mucosal vessels in the dilated collecting system.
PRESENTATION
In the young adult, episodic flank or abdominal pain, particularly during diuresis, is a common manifestation. Occasionally, a patient with the UPJ obstruction presents with hypertension. The pathophysiology is thought to be a functional ischemia with reduced blood flow caused by the enlarged collecting system that produces a renin-mediated hypertension .
DIAGNOSIS
Ultrasonography; is the standard method for identifying hydronephrosis in infancy. Postnatal ultrasound imaging is usually deferred until day 3 of life, to allow for improvement in the relative oliguria, which could lead to underestimation of the degree of hydronephrosis.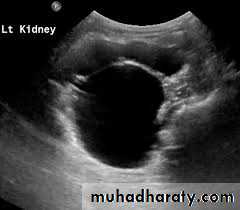
DIAGNOSIS
If prenatal US has shown a large or bilateral hydronephrosis, a follow-uprenal tract ultrasound scan should be performed soon after birth. If there
is a prenatal unilateral hydronephrosis (and the bladder is normal), the
scan is deferred until days 3–7 (to allow normal physiological diuresis to
occur, which may spontaneously improve or resolve hydronephrosis).
If upper tract obstruction persists, a voiding cystourethrogram (VCUG)
is indicated (to rule out VUR and examine for posterior urethral valves),
and a renogram can assess individual renal function and drainage (DTPA,
MAG-3).
DIAGNOSIS
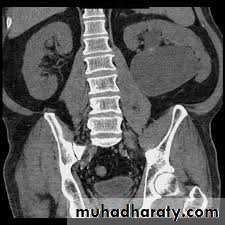
IVU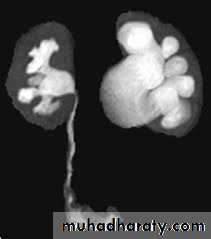
DIAGNOSIS
CT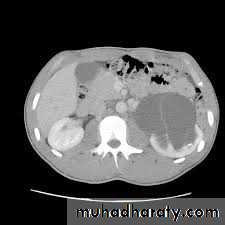
Treatment
Children may be observed with US and renogram if they remain stable andhave good renal function and no other complications (such as persistent infection or stones).
If children are symptomatic or have a signifi cant hydronephrosis with impaired renal function (<40%), pyeloplasty is recommended
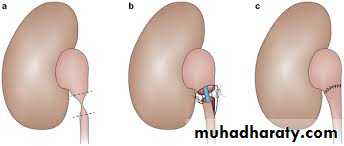
PYELOPLASTY

MEGAURETEr
DefinitionMGU is a nonspecific term implying a spectrum of anomalies associated with pathologically excessive ureteral diameter
Children up to 12 year-ureteral width>7mm
Older children ureteral width>10mm

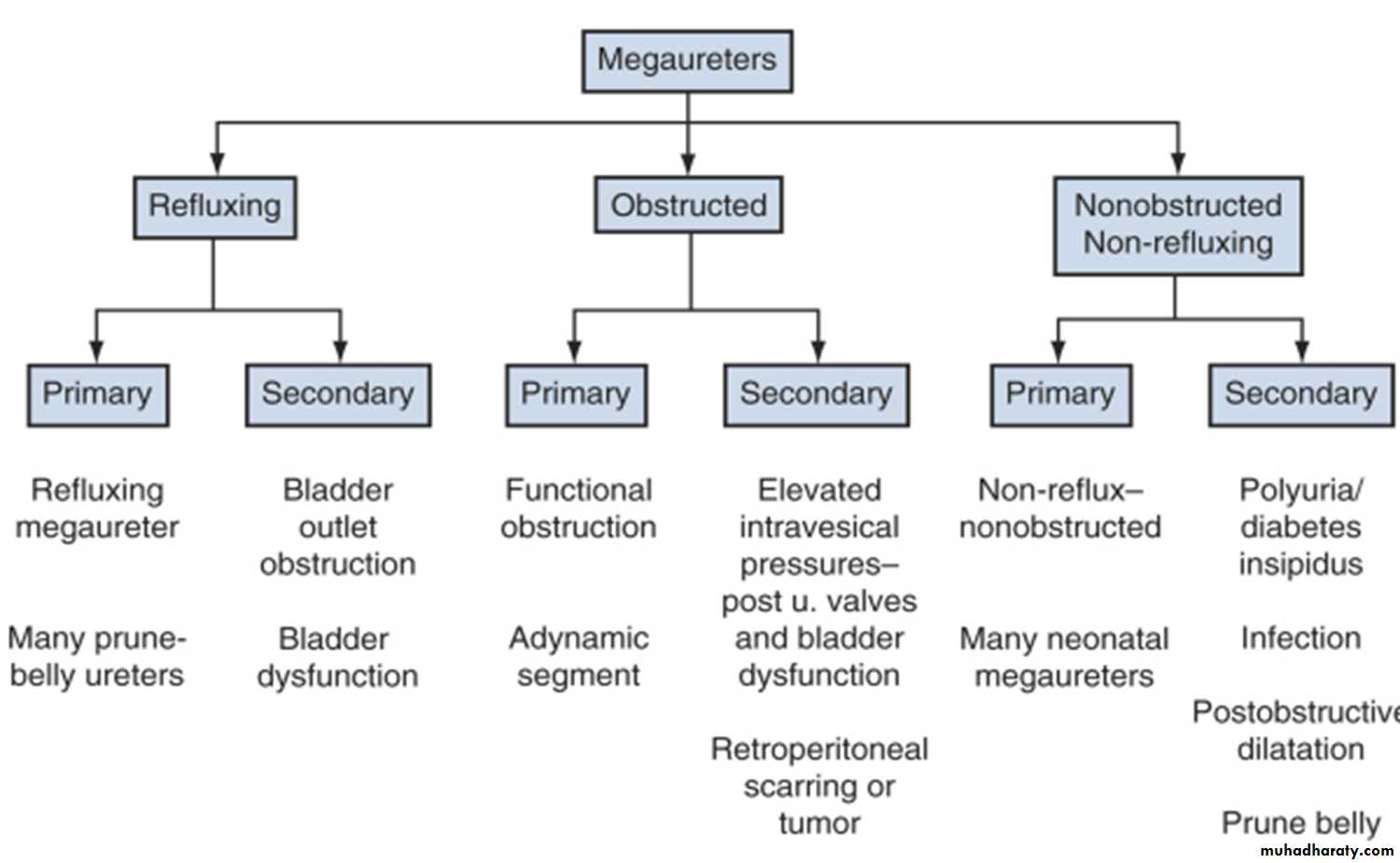
Classification
presentation
Bilateral in approximately 25% of patients .In up to 10% to 15% of children the contralateral kidney may be absent or dysplastic .
UTIs, abdominal pain, or hematuria.
The diagnosis may be made later in life in some asymptomatic patients.
Pathophysiology
The distal end of the ureter, as it becomes intramural and subsequently submucosal, rearranges the muscular layers in its wall. All layers become longitudinally oriented, and the ureteral adventitia fuses to the bladder trigone .
Primary Obstructive Megaureter
the precise etiology of primary obstructive MGU remains unclear, it is generally agreed that the most common finding is an aperistaltic juxtavesical (adynamic) ureteral segment that prevents urine from flowing at an acceptable rate. , and functional obstruction results
Operative exposure a dynamic segment
Secondary obstructive MGU
most commonly occurs with neurogenic and non-neurogenic voiding dysfunction or infravesical obstruction such as PUVs.ureteroceles, ureteral ectopia, bladder diverticula, postreimplantation fibrosis, and external compression by retroperitoneal tumors, masses, or aberrant vessels

Primary and Secondary Refluxing Megaureter
Primary
male more than female
Often bilateral
Often associated with renal scarring, atrophy,or dysplasia, secondary puj obstruction due to kinking
Secondary
bladder or urethral pathology
Ureterocele ,stricture, radiation
Primary Nonobstructive, Nonrefluxing Megaureter
Most newborn MGUs fall in this category To establish this diagnosis, VUR, UVJ obstruction, and secondary causes of dilatation must be ruled out. Clinically, this may not be straight forward in all casesSecondary Nonobstructive, Nonrefluxing Megaureter
-UTI-Nephropathies and other medical conditions
include lithium toxicity, diabetes insipidus or mellitus, sickle cell nephropathy, and psychogenic polydipsia.

DIAGNOSIS
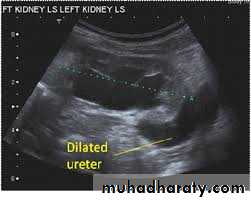
DIAGNOSIS

DIAGNOSIS

TREATMENT
