INFLAMATORY BOWEL DISEASE
done byDr. layth Q
INFLAMATORY BOWEL DISEASE
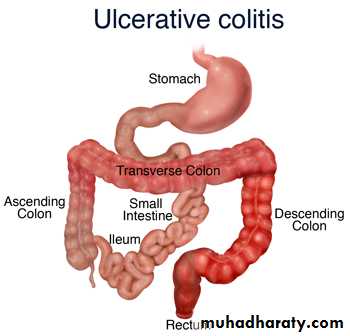
The term reserved for idiopathic intestinal inflammation as ulcerative colitis and Crohn's disease.ULCERATIVE COLITIS
It is disease of rectum and colon with extra intestinal manifestation .The incidence is 10per 100000.in UK
Aetiology
The cause is unknownGenetic contribution as 10-20-per cent of patients have first degree relative with inflammatory bowel disease .
UC more common in Caucasian than Afro-Caribbean orAsian population.
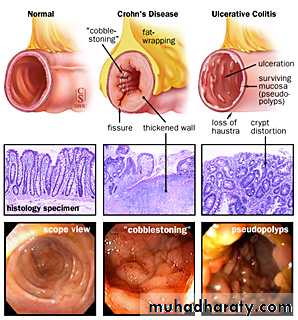
pathologyAll cases start at rectum and extends proximally in continuity
Colonic inflammation is diffuse,confluent and superficial, primarily affecting the mucosa and sub mucosa.Chronic mucosal ulceration is associated with formation of granulation tissue and regeneration ,leading to a polyp like pseudopolyposis,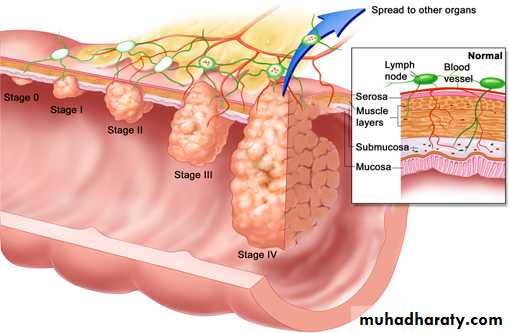
Structuring in UC is very unusual and urgent assessment because of the possibility of coexisting carcinoma.A small proportion of patients with colonic dysplasia may develop irregular mucosal swelling (dysplasia-associated lesions,DALMs),highly predictive of coexisting of carcinoma.
Histological examination reveals inflammatory cells in lamina propria,walls of crypts,and there are crypt abscesses.There is depletion of goblet cell mucin .
With time,precancerous changes can develop (dysplasia).It increases with time and ranging from 2-18-per cent at 30 years Dysplasia classified into low or high grade dysplasia.High grade dysplasia is absolute indication of colectomy as 40 per cent of colectomy specimens of high grade have evidence of colorectal cancer.
Symptoms
Depends on extent of the disease and the presence of complications .If confined to rectum usually no systemic upset and the extra alimentary manifestation are rare. The main symptoms will be rectal bleeding , and mucous discharge.
Colitis always associated with bloody diarrhoea and urgency.pain is unusual. The more extensive the disease the more likely extra intestinal manifestation are to occur .
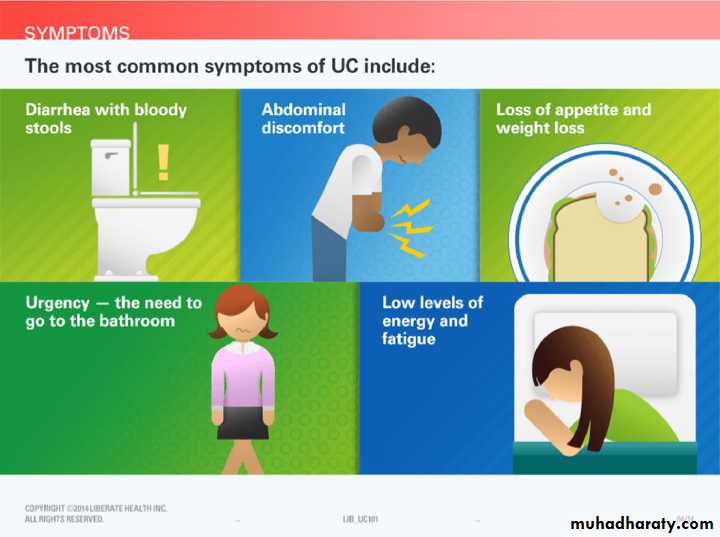
Extensive colitis associated with systemic illness like, malaise,loss of appetite and fever .Bloody diarrhoea resulting in anaemia and hypo proteinemia and electrolyte disturbance .Approximately30 percent extending to sigmoid colon and spread to splenic flexure
Complications of ulcerative colitis
AcuteToxic dilatation
PerforationHemorrhage
Chronic
Cancer
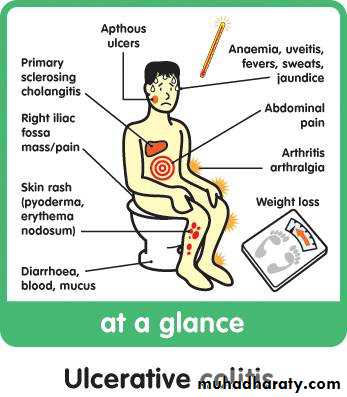
Extra- alimentary manefestations ,like skin lesions,eye problems and liver dis.Classifications of colitiis severity.
Bowel motion and presence of illness.Mild: four stools with or without bleeding daily .
Moderate disease:more than four stools with few systematic illness,abdominal pain,inflammatory markers,including ESR and C- reactive protein ( CRP) are often raised .Severe disease : more than six bloody stools,fever,tachycardia,anaemia, and raised inflammatory markers.Hypoalbuminaemia is common .
Fulminant disease: more than ten bowel movements daily,fever,tachycardia bleeding ,Hypoalbuminaemia,abdominal tenderness and distension,blood transfusion requirement ,progressive colonic dilatation ( toxic megacolon) . This is a significant finding and indication for immediate surgery if colonic perforation is to be avoided.
Extra intestinal manefestations:
Arthritis,sacroiliitis,ankylosing spondylitis more common than general population and associated with HLA-B27
Sclerosing cholangitis is associated with UC can progress to cirrhosis and heptocellular failure and at more great risk of development of large bowel cancer
Skin lesions: erythema nodosum and pyoderma gangrenosum.
Eyes: affected with uveitis and episcleritisCancer risk in colitis
Risk increases with duration.Ten years from the diagnosis is around 1 percent.Twenty years increases to 10-15/. . Twenty per cent at 30years.Carcinoma is more likely to occur if the whole colon is involved or if the disease started early in life .Colonoscopy with multiple biopsies is advised to detect dysplasia .Investigations:
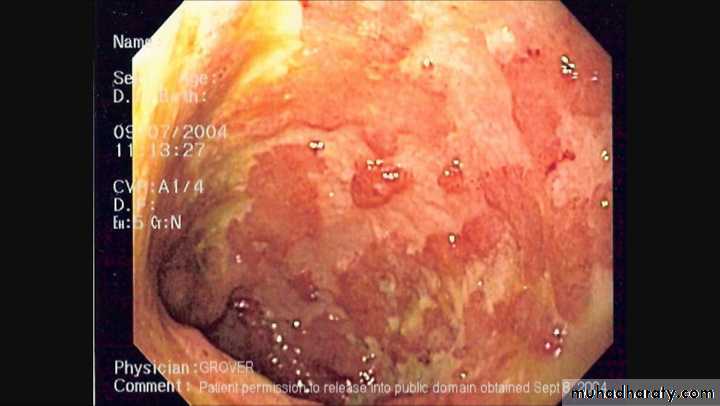
Endoscopy and biopsy by sigmoidoscopy or colonoscopy.Radiology plain film may be valuable in toxic megacolon.Barium enema has been replaced by computed tomography. CT finding may show thickening of colonic wall .
Bacteriology:stool send for microbiology to exclude infective causes.
treatment
Principles of management of UC:Many patients maintained for years on medical therapy.
Toxic dilatation suspected with sever abdominal pain .Colitis patients at risk of cancer especially pan colitis.
Multidisciplinary approach,gastroenterologist,nurses,as well as surgeon.Medical treatment : therapy based on anti inflammatory agents .5- aminosalicyclic acid and corticosteroids either topically or systemically.The immunosuppressive drugs azathioprine and cyclosporine maintain remission as steroid sparing agents.More recently monoclonal antibodies,(infliximab)
Acute colitis severe type require hospitalisation in addition to steroids ,medical therapy ,supportive treatment ,fluid and electrolyte balance. The multidisciplinary approach,lastly to surgical option.
indication for surgery
Fulminating disease failing to respond to medical therapyChronic disease with anaemia,frequent stools,urgency and tenesmus
Steroid dependant
Inability of the patient to tolerate medical therapy.
Neoplastic change
Extra intestinal manefestations
Rarely,severe haemorrhage or stenosis causing obstruction.
Operative treatment for UC:
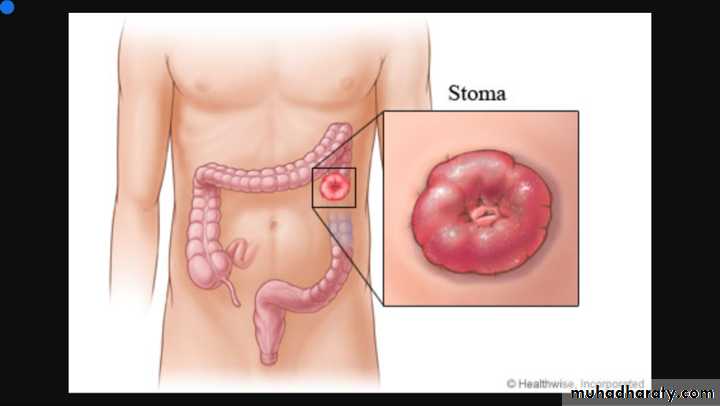
Emergency---is subtotal colectomy and end ileostomy.the recto sigmoid is left
Long and brought as mucous fistula or closed just beneath the skinElective surgery----- the indications for it include:
Failure of medical treatment/ steroid dependance.Growth retardation
Extra intestinal diseaseMalignancy
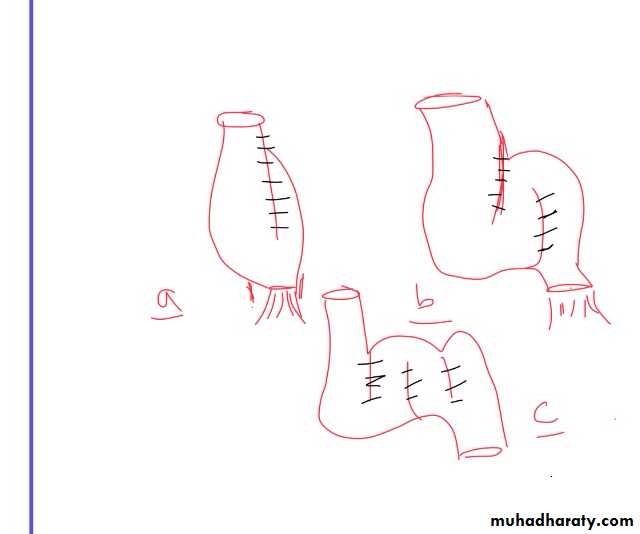
In elective setting FOUR operations:• .subtotal colectomy and ileostomy
• .proctocolectomy and permanent ileostomy.
• .restorative proctocolectomy with ileoanal pouch.
• .subtotal colectomy and ileorectal anastamosis.
INFECTIONS OF SMALL AND LARGE INTESTINE
Yersinia.,amebiasis,salmonella,typhoid and paratyphoid,tuberculosis,actinomycosis,and clostridium difficile.
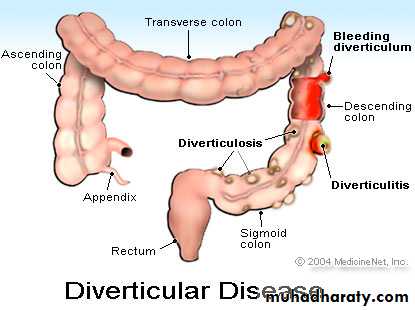
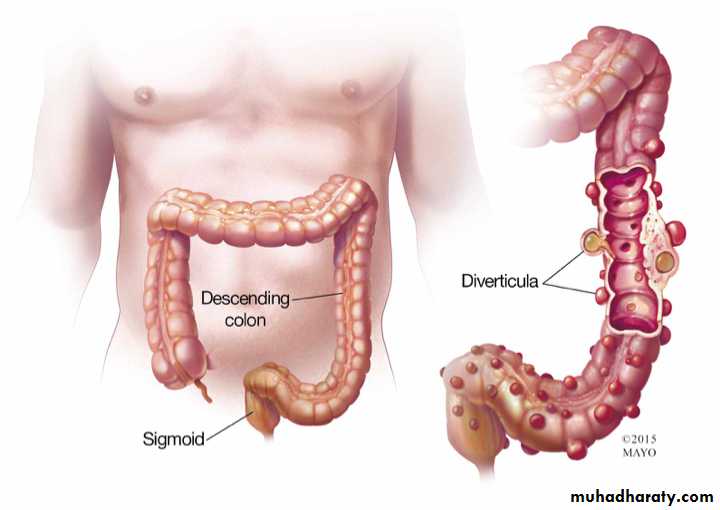
Diverticulitis disease of the large intestine:
done byDr. layth Q
Found around 75% of over seventy year olds in western world.Mostly affect sigmoid colon, but can occur in the caecum or the whole colon ( but not the rectum). Diverticula are most often asymptomatic( diverticulosis) and found incidentally,but can present clinically with sepsis or haemorrhage.
Aetiology: western diet deficient in dietary fibre
Complications of diverticulitis disease:
1. Diverticulitis2. Perforations , leading to peri colic abscess,occasionally generalised peritonitis.
3. Intestinal obstruction lead to fibrosis can cause stenosis or loops of small bowel
adhere to inflamed sigmoid.
4.Haemorrhage ,diverticulitis may cause haemorrhage.
5. Fistula,colovesical,colocutanous,colovajnal,enterocutaneous.
Classification of contamination:
The major of sepsis impact on the outcome in acute diverticulitis. The most commonly used system of classification is: Hinchey
classification of complicated diverticulitis.
GradeI .Mesenteric or pelvic abscess.
I l.pelvic abscess.
I l l.purulent peritonitis
I v.faecal peritonitis.
Radiology:Plain chests and abdominal radiograph can demonstrate pneumoperitonium.
Spiral CT,identifying the bowel wall.
On identifying of abscess in stable patient ,drainage maybe carried out per cutaneously.
Barium enemas and colonoscopy,avoided in acute cases.How can be used after the attack has settled to exclude a co existing carcinoma.
Colovesical fistula evaluated with cystoscopy and biopsy in addition .
The differential diagnosis for colovesical fistula includes:
CancerRadiation injury
Crohn's disease
Tuberculosis
Actinomycosis .
Management
Conservative
Nothing by mouth ,rest to the bowel.I.v.fluid and antibiotics for gram negative bacilli and anaerobes.
CT.scan can confirm the diagnosis and assess the complications.
Principles of surgical management:
*Hartman's procedure ,safest option in emergency surgery** primary anastamosis in selected patients
*** elective resection
**** colovesical fistula requires resection.
Tumours of the large intestine
done byDr layth Q
Benign:
Polyp,is protrusion of the mucosa.Classification of intestinal polyps:
Inflammatory. Inflammatory polyps ( pseudopolyposis in ulcerative colitis)
Meta plastic. Meta plastic or hyperplastic polyps
Hammartomatous. Peutz- jet hers polyp
Juvenile polyp
Neoplastic. Adenoma. Tubular,tubulovillous,villus
Adenocarcinoma,carcinoid tumour
Adenomatous polyp:
Varies from tubular to villus.may be solitary and the cause of rectal bleeding or sometimes villous and the cause of hypo Kalaemia and Hypoalbuminaemia .the risk of malignancy increases with their size .Adenomatous polyp:
Varies from tubular to villus.may be solitary and the cause of rectal bleeding or sometimes villous and the cause of hypo Kalaemia and Hypoalbuminaemia .the risk of malignancy increases with their sizeFamilial adenomatous polyposis: defined to have more than 100 polyps and multiple extra intestinal manifestation like endodermal( adenomas of duodenum,stomach) or ectodermal like epidermoid cysts ,brain tumours . And mesodermal like desmoid,dental problems,or osteomas.
Gardener's syndrome: familial polyps with epidermoid cyst and desmoid tumours.
Features of familial adenomatous polyposis:Autosomal dominant
More than 100 colonic adenomas
Prophylactic surgery
Polyps and malignant tumours can develop in the duodenum and small bowel.::
Treatment
Colectomy with ileorectal anastamosis
Restorative proctocolectomy with ileal pouch
Total removal with end ileostomy.
Lynch syndrome: characterised by increased risk of colorectal cancer and also cancer of endometrium,ovary,stomach and small intestine.
Malignant:
Epidemiology in UK colorectal cancer is the second most common cause of cancer death .Aetiology: the accepted model arises from adenomatous polyps after genetic mutation influenced by environmental factors . The p53 gene mutated in carcinomas.
Linkage between diet and colon cancer
Ulcerative colitis
Suggested after cholecystectomy increase risk
Also increased risk after ureterosigmoidostom
Pathology:
MacroscopicFour types; annular,tubular,ulcer,cauliflower.
Microscopic
It is adenocarcinoma originating in the colonic epithelium
Surgical Treatment
done byDr.layth Q
Pre operative preparation
Mechanical preparation,In colonic cancer there is good evidence that there is no benefit of pre operative preparation .While rectal cancer suggest mechanical bowel preparation is still appropriate .
The antiembolic stocking ,prophylactic subcutaneous low molecular weight heparin .
*single dose of proper antiembiotic to reduce wound infection and sepsis .
*In all cases where stoma seem most likely careful pre operative counselling
Operations:
Designed to remove the primary tumour and draining locoregional lymph nodes .
Right hemicolectomy for right sided cancer .
Extended right hemicolectomy for ca of transverse colon and splenic flexure ,to remove in addition the whole transverse colon and splenic flexure .Left hemicolectomy ,for descending colon and sigmoid cancers.
Laparoscopic surgery for colonic cancer nowadays
Emergency surgery:
In UK 20% of colonic cancer patients presents as emergency,the majority with obstruction .In right sided cancer ,usually possible to do primary anastomoses during the operation of right hemicolectomy .while if there is perforation and the patient is unstable ,advisable to bring out an ileo/ colostomy rather than anastamosing bowel .
Left sided cancer,resection and anastamosis,with proximal colostomy if leaking is a possibility.But if facilities are present,an obstructing left sided lesion can be treated with an expanding metal stent.This has the advantage of converting an emergency operation with high chance of stoma to situation which can be managed semi electively with a resection and anastamosis.
PROGNOSIS:
Five year survival 50%.Patients with Duke 's A ===>90% have disease free five years .( disease confined to the bowel wall.)
Spread of the disease out side the bowel wall reduces five year survival to60%.
Patients with lymph nodes metastasis five year survival 30%.
Colorectal cancer follow up
Surveillance colonoscopy to detect synchronous and metachronous bowel tumoursUS,CT scan for liver metastasis
CEA ( carcinoembryonic antigen
RECTUM
done byDr layth Q
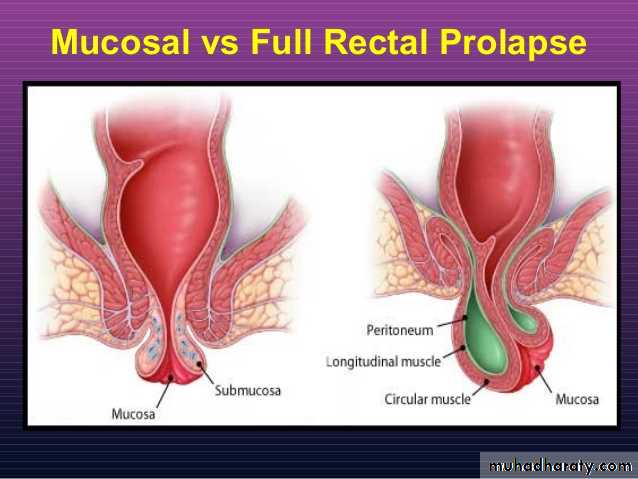
prolapse
Prolapse: tow types,
Mucosal
Full thickness ,whole layers .
The mucosal ( partial thickness) can be palpated by finger and thumb ,in children can be treated conservatively.
While in adult, full thickness associated with incontinance

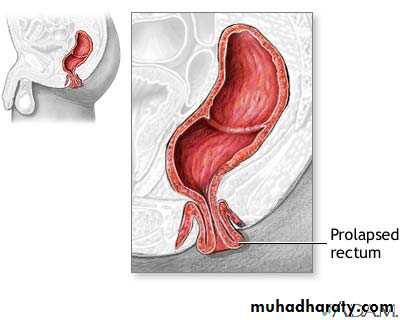
Surgery is necessary. The operation is performed either via the perineum,or the abdomen.
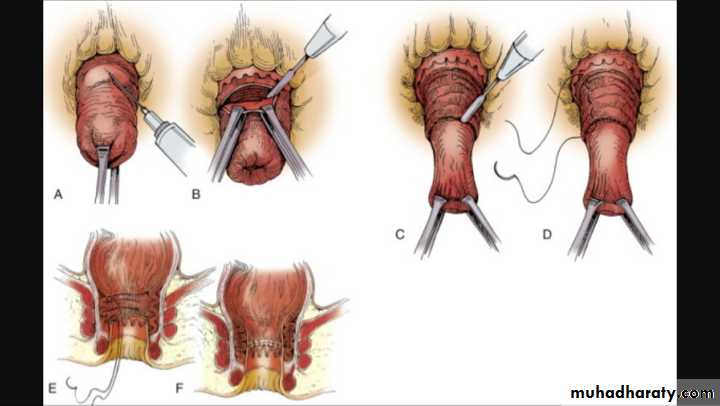
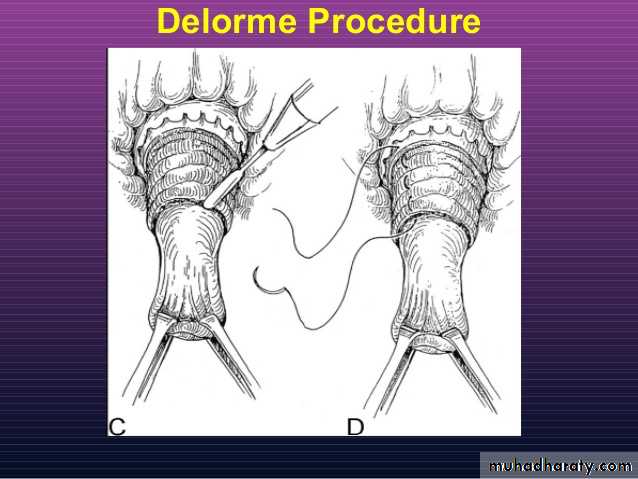
Delorme's operation for rectal prolapse,performed by removal of excessive mucosa and inserting interrupted sutures in the underlying muscle to be plicated.
Rectal tumors
Done byDr Layth Q
Benign tumour
Villous adenomasThese have a characteristic frond-like appearance. They may be very large, and occasionally fill the entire rectum. These tumours have an enhanced tendency to become malignant – a change that can sometimes be detected by palpation with the finger; any hard area should be assumed to be malignant and should be biopsied. Rarely, the profuse mucous discharge from these tumours, which is rich in potassium

Familial adenomatous polyposis
Hyperplastic polypsThese are small, pinkish, sessile polyps, 2–4 mm in diameter and frequently multiple. They are common and generally harmless.
Inflammatory pseudopolyps
Juvenile polyp
CARCINOMAS
Origin:the adenoma–carcinoma sequence)
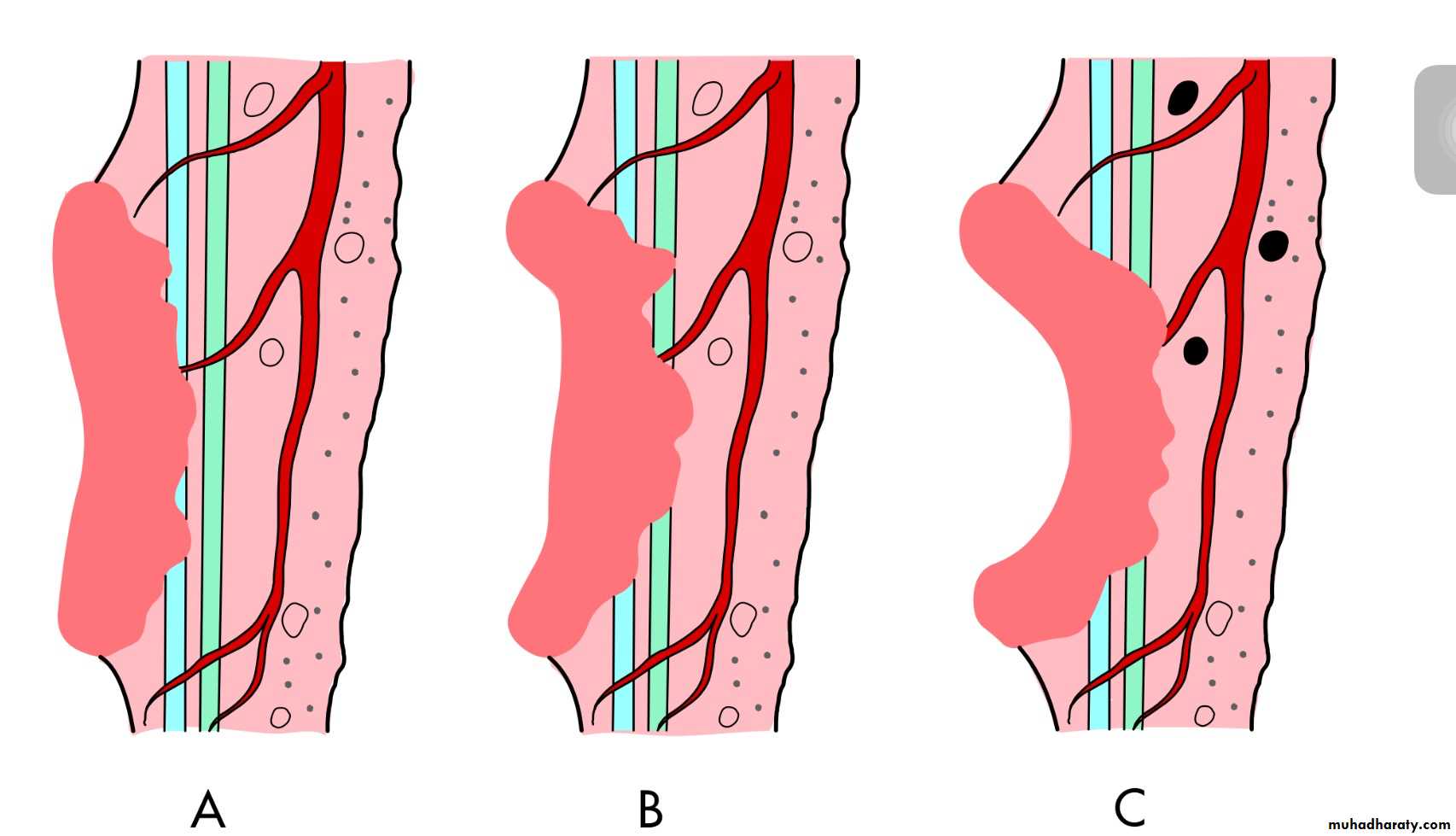
Types of carcinoma spread
Local spread
Local spread occurs circumferentially rather than in a longitudi- nal direction. After the muscular coat has been penetrated, the growth spreads into the surrounding mesorectum, but is initially limited by the mesorectal fascia
Lymphatic spread
Lymphatic spread from a carcinoma of the rectum above the peritoneal reflection occurs almost exclusively in an upward direction
Venous spread
Peritoneal dissemination
Stages of progressionDukes classified carcinoma of the rectum
TNM staging
Histological grading• Low grade, well-differentiated 11 per cent prognosis good;
• Average grade, 64 per cent prognosis fair;
• High grade, undifferentiated tumours 25 per cent prognosis
poor.
Clinical feature
Early symptoms of rectal cancer
■ Bleeding per rectum
■ Tenesmus
■ Early morning
Investigations
1. Abdominal examination2. Rectal examination
3.Proctosigmoidoscopy
4.biopsy
5. Colonoscopy
Treatment
Surgery
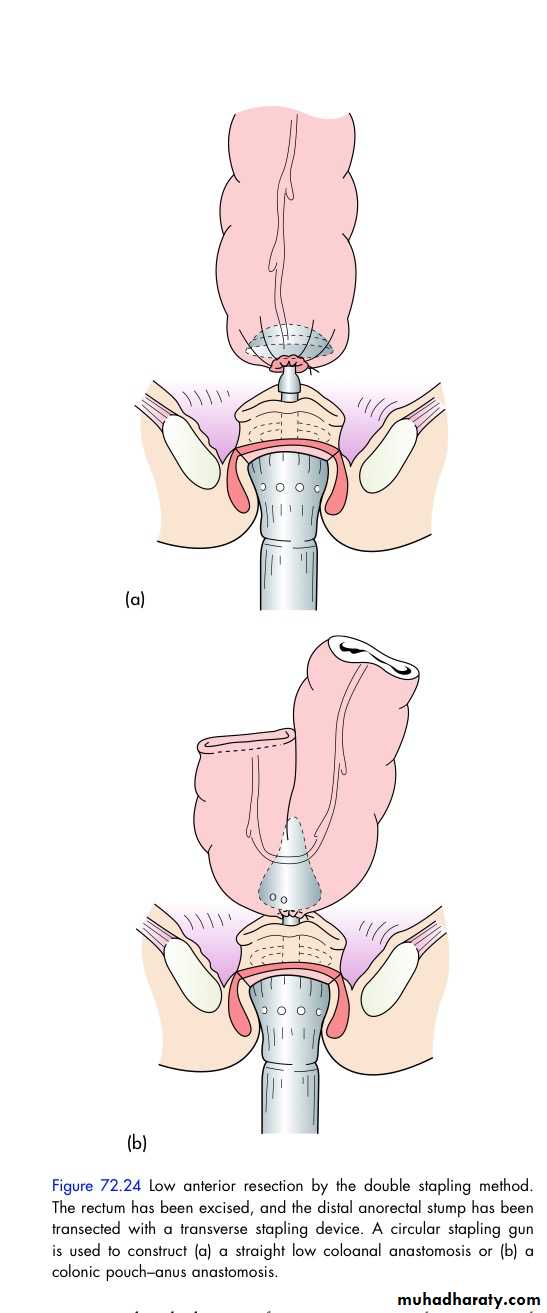
Anterior resection
Abdominoperineal resection
Endoluminal stenting
Palliative colostomy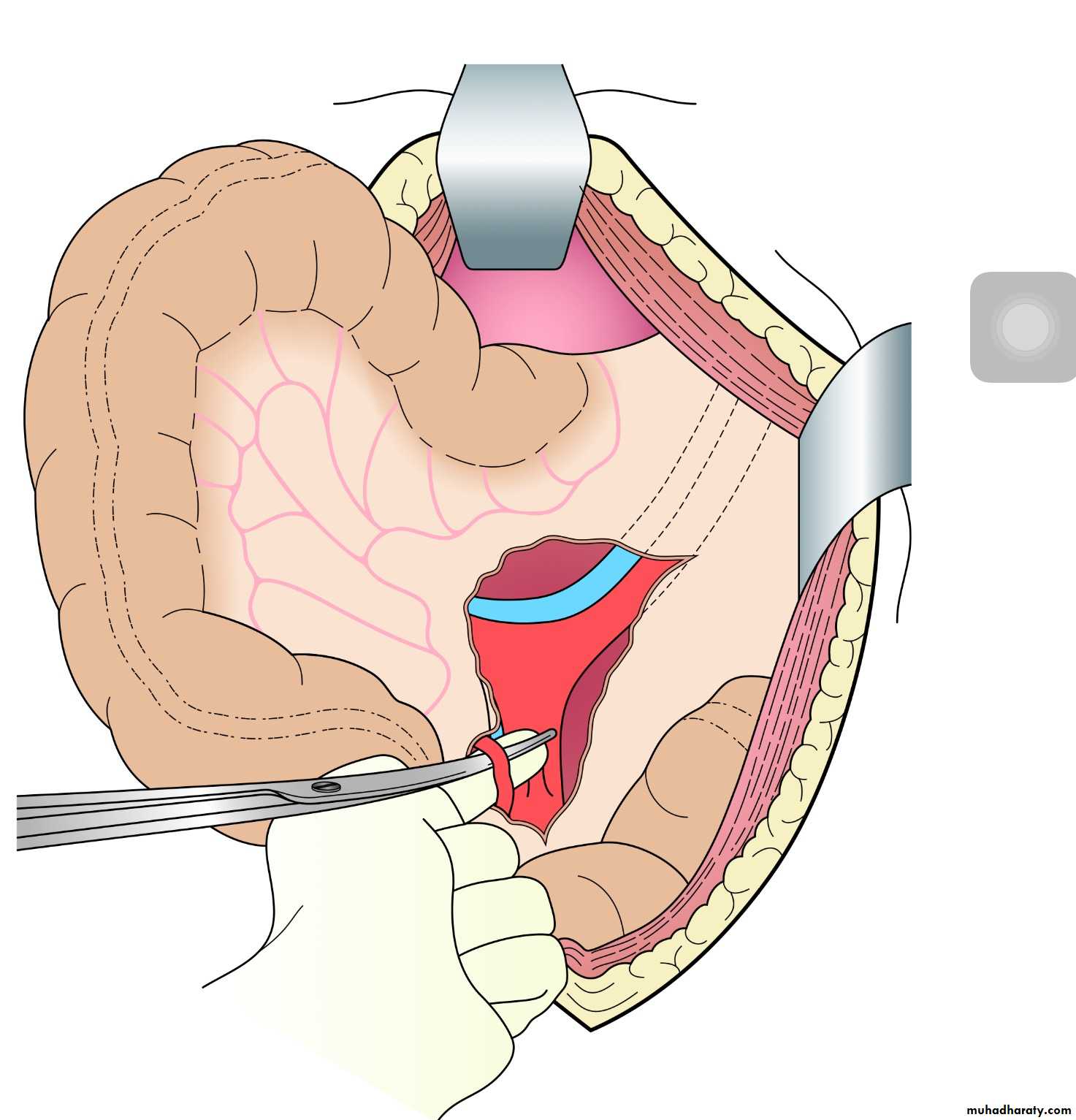
Summary
Radiotherapy
ChemotherapyCarcinoid tumour
Carcinoid tumour originates in the submucosa, with the mucous membrane over it being intact. Consequently, it seldom pro- duces evidence of its presence in the early stages, when it presents as a small plaque-like elevation. The incidence of clini- cal malignancy, i.e. the occurrence of metastases, is 10 per cent.Further reading 1235
This is much less than that for carcinoid tumour of the small intestine, but it is greater than that for carcinoid tumour of the appendix. Multiple primary carcinoid tumours of the rectum are not infrequent. The neoplasm is of slow progression, and usually metastasises late. Large carcinoids (over 2 cm) are almost always malignant.
Treatment
Local excision is sufficient treatment for small carcinoids. Resection of the rectum is advisable if the growth is more than 2.5 cm in diameter, if recurrence follows local excision or if the growth is fixed to the perirectal tissues. Even when metastases are present, resection may prolong life
Thanks for your attention