
Onchocerca volvulus ( Blinding
filariasis; river blindness)
Microfilaria of Onchocerca volvulus,
from skin snip from a patient seen
in Guatemala. Wet preparation

Some important characteristics of
the microfilariae of this species are
shown here: no sheath present; the
tail is tapered and is sharply angled
at the end Onchocerca volvulus .

Epidemiology: In Africa onchocerciasis
is prevalent throughout the eastern,
central and western Africa, where it is
the major cause of blindness. In the
Americas it is found in Guatemala,
Mexico, Colombia and Venezuela. The
disease is confined to neighborhoods of
low elevation with rapidly flowing small
streams where black flies breed. Man is
the only host.

Morphology: Adult female onchocerca
measure 50 cm x 300 µm, male worms
are much smaller.
Infective larvae of O. volvulus are
500 µm x 25 µm

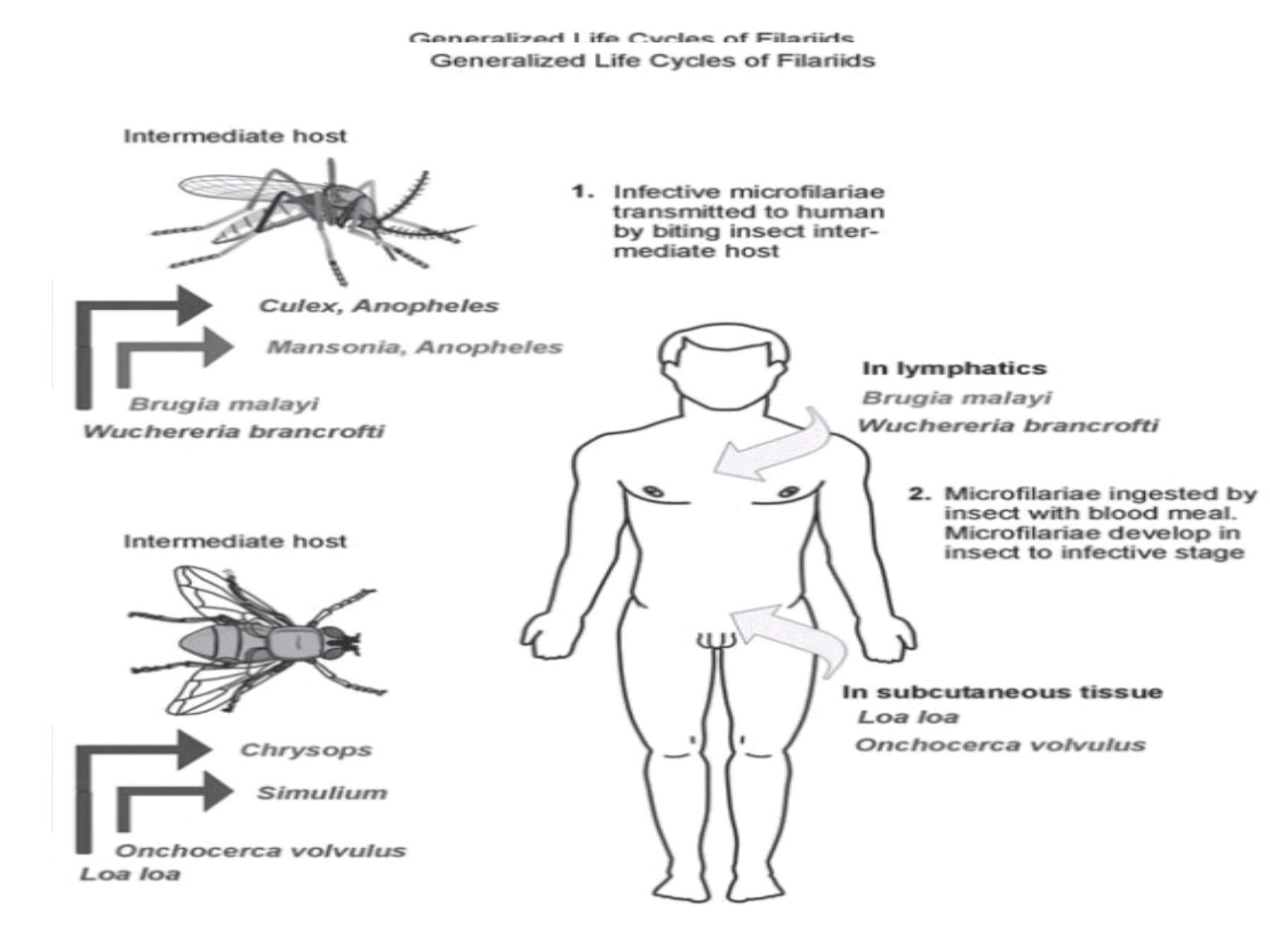
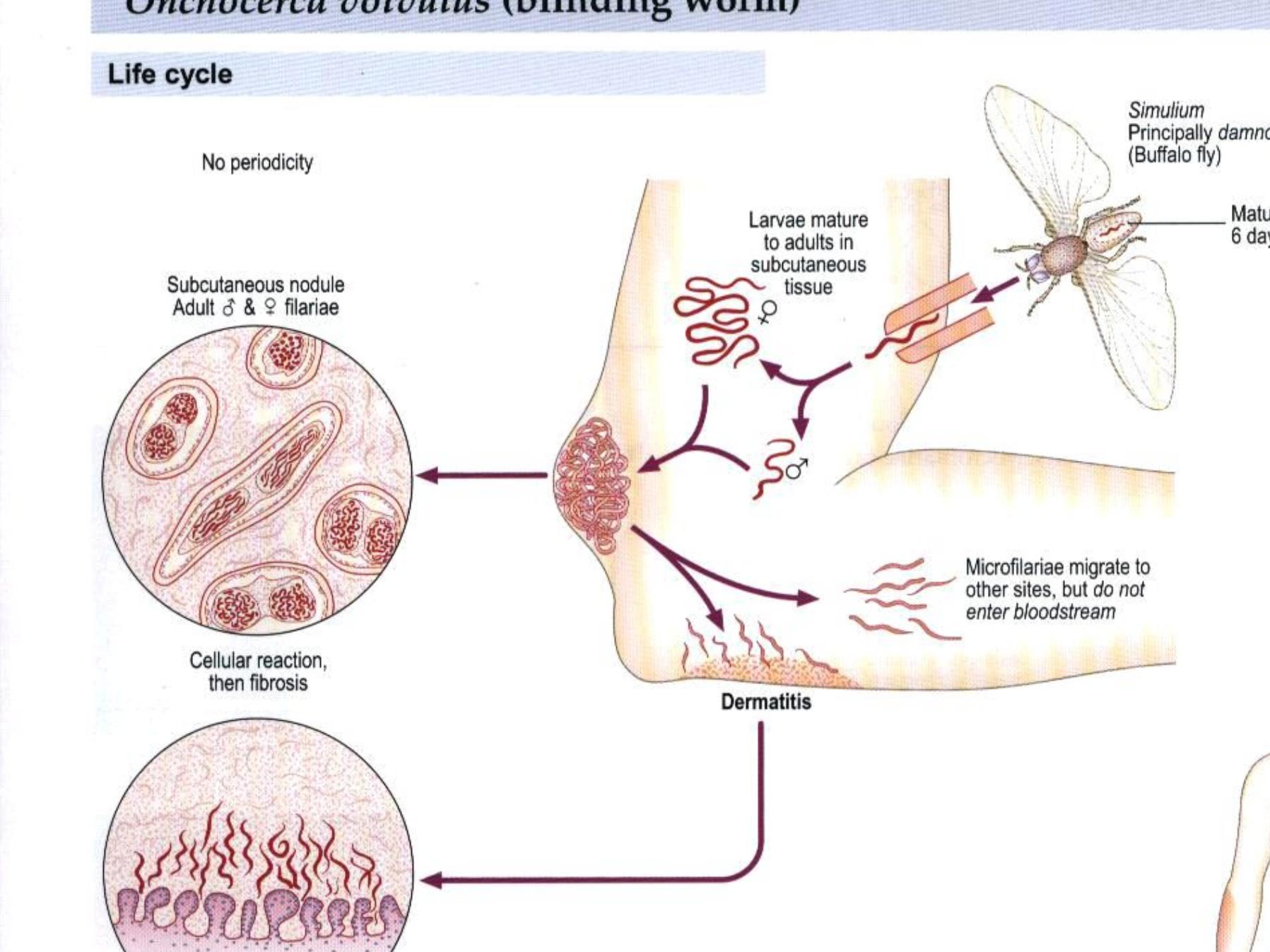
L ife cycle: Infective larvae are injected
into human skin by the female black fly .
(Simulium damnosum) where they develop
into adult worms in 8-10 months.

The adults usually inhabit as group of
worms (2-3 females and 1-2 males)
tightly coiled.
The gravid female releases
microfilarial larvae, which are usually
distributed in the skin.

They are picked up by the black fly
during a blood meal. The larvae
migrate from the gut of the black fly to
the thoracic muscle where they
develop into infective larvae in 6-8
days. These larvae migrate to the head
of the fly and then are transmitted to a
second host.

Diagnosis: Diagnosis is based on
symptoms, history of exposure to
black flies and presence of
microfilaria in nodules.
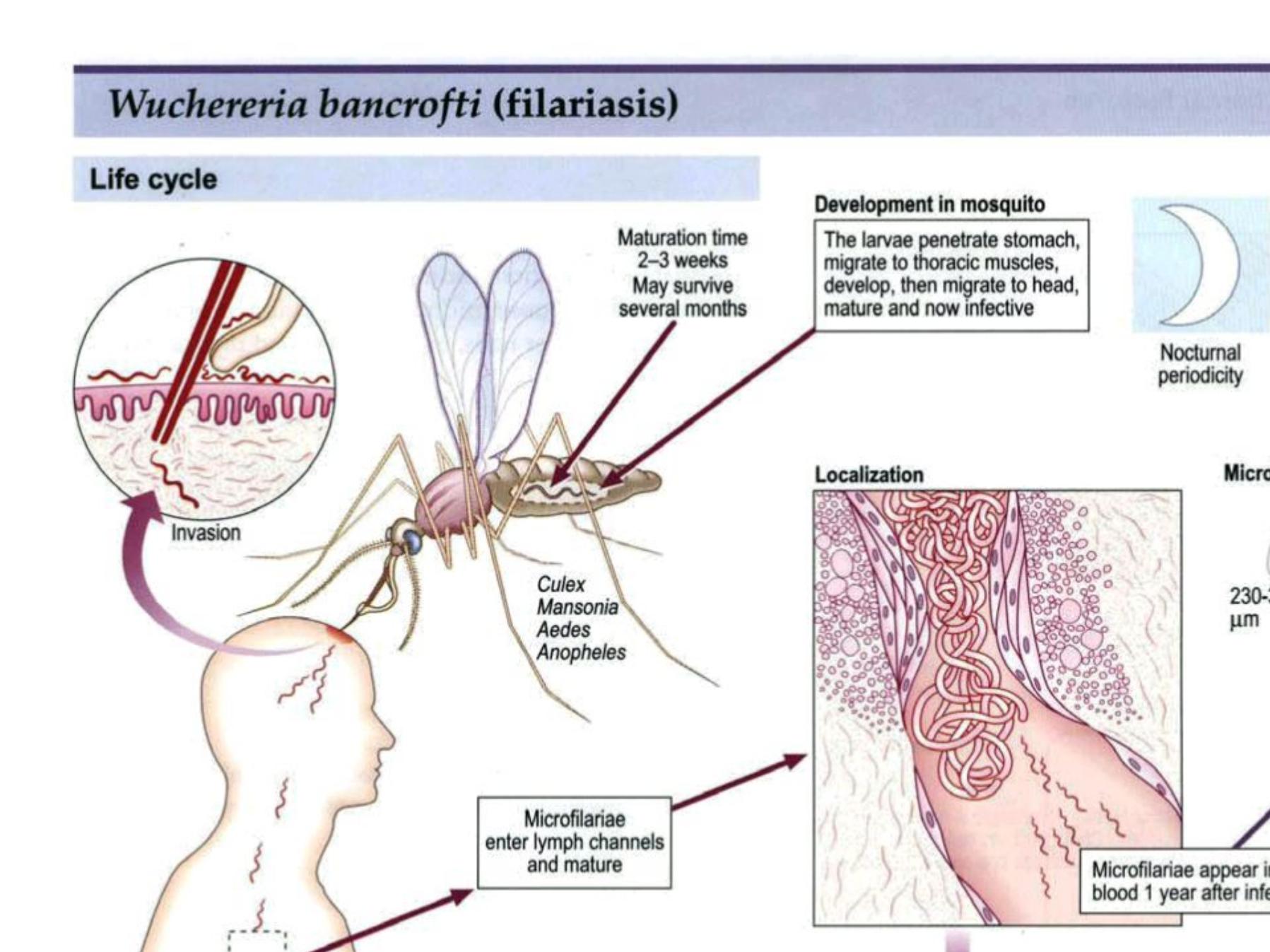

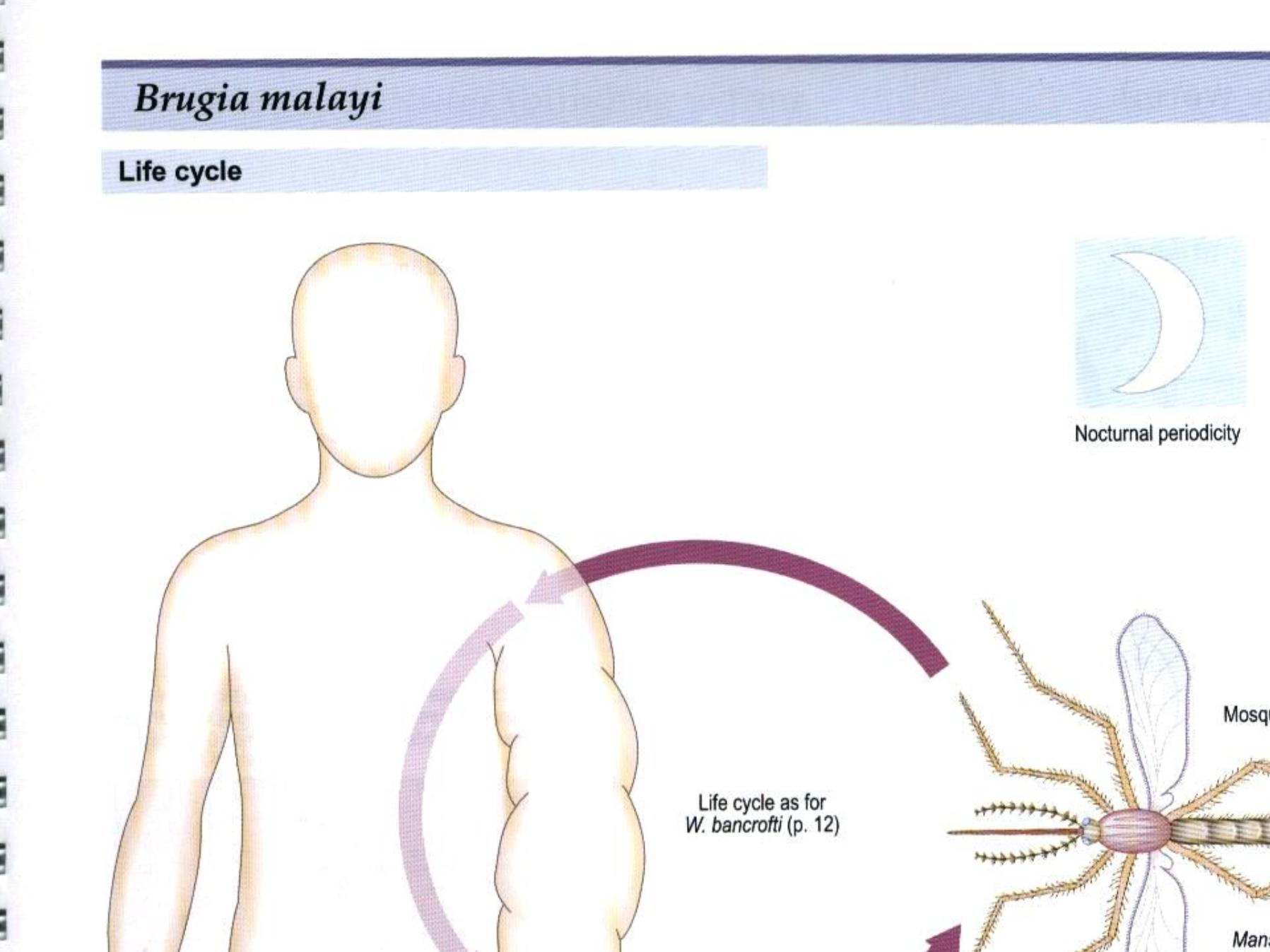
Epidemiology: W. bancrofti is strictly a
human pathogen and is
distributed in tropical areas worldwide,
whereas B. malayi infects
a number of wild and domestic animals
and is restricted to South-East Asia.
Mosquitoes are vectors for both
parasites.

Morphology: These two organisms are
very similar in morphology and the
disease they cause . Adult female W.
bancrofti found in lymph nodes and
lymphatic channels are 10 cm x 250 µm
whereas males are
only half the size. Microfilaria found in
blood are only 260 µm x 10 µm.
Adult B. malayi are only half the size and its
microfilaria are only slightly
smaller than W. bancrofti.

Life cycle: Filariform larvae enter the human
body during the mosquito bite
and migrate to tissues. There they may take
up to a year to mature and
produce microfilaria which migrate to
lymphatics and, at night,
enter the blood circulation. Mosquitos are
infected during the blood meal .
The microfilaria grow 4-5 fold in mosquito in
10-14 days and become infective for man.

Symptoms: Symptoms include
lymphadenitis and recurrent high fever,
every 8-10 weeks, which lasts 3-7 days.
There is progressively
lymphadenitis due to inflammatory
response to the parasite lodged in the
lymphatic channels and tissues. As the
worm dies, the reaction continues and
produces a fibro-proliferative granuloma
which obstructs lymph channels and
causes lymphedema and elephantiasis .

The stretched skin is
susceptible to traumatic injury and
infections. Microfilaria cause
eosinophilia and some splenomegaly.
Not all infections lead to elephantiasis.
Prognosis, in the absence of
elephantiasis, is good.

Diagnosis: Diagnosis is based on
history of mosquito bite in endemic
areas,
clinical findings, and presence of
microfilaria in blood samples collected
at night.
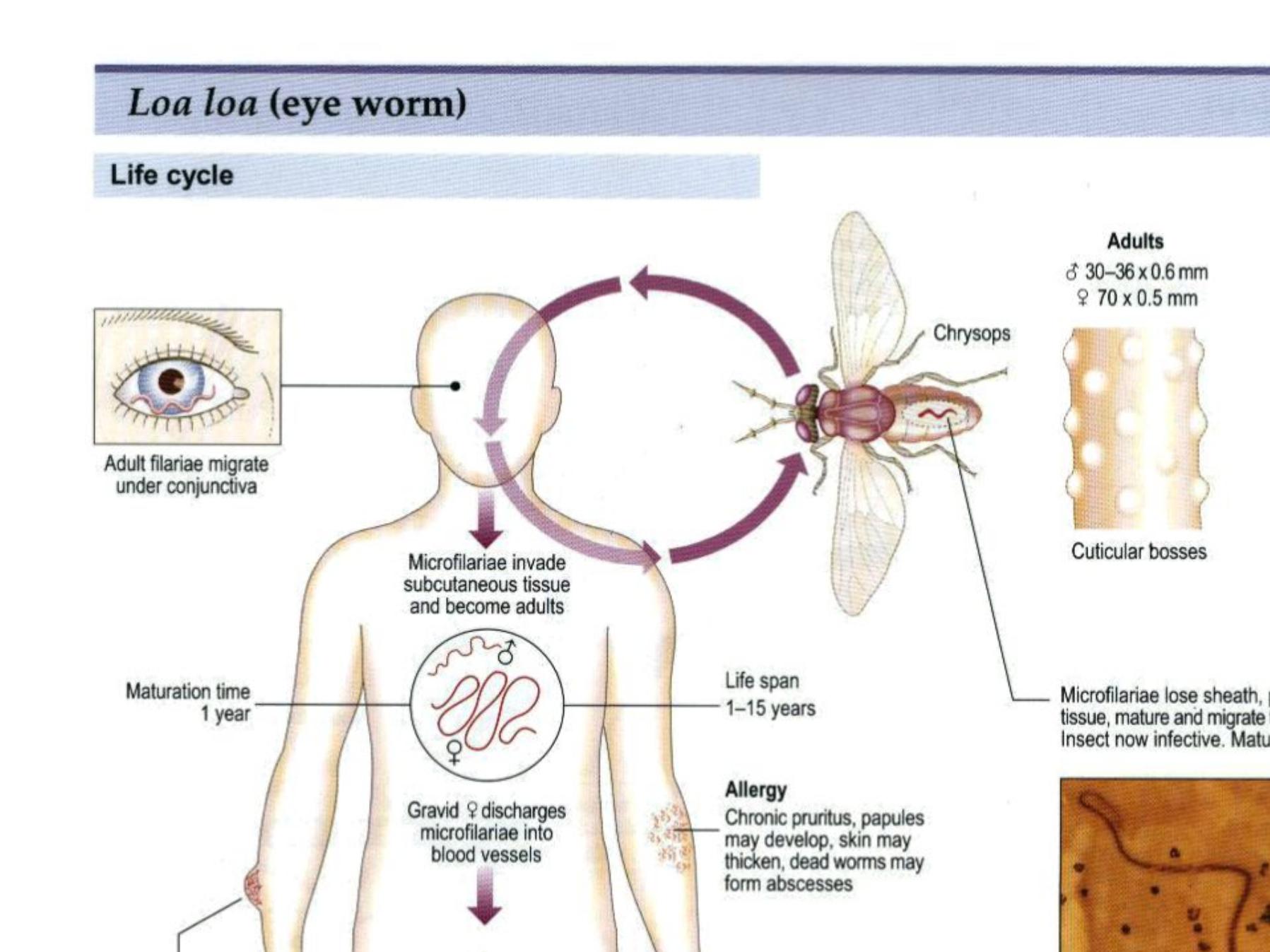

L oa loa (eye worm)
Loasis is limited to the areas of African
equatorial rain forest. The incidence in
endemic areas varies greatly (8-75
percent). The larger, female organism are
60 mm x 500 µm; males are 35 x 300 µm
in size. The circulating microfilaria are
300 µm x 7 µm; the infective larvae in the
fly are 200 µm x 30 µm.

The life cycle of
Loa loa is identical to that of onchocerca
except that the vector for this worm is
the deer fly. The infection results in
subcutaneous (Calabar) swelling,
measuring 5-10 cm in diameter, marked
by erythema and angioedema, usually in
the extremities. The organism migrates
under the skin at a rate of up to an inch
every two minutes.

Consequently, the swelling appears
spontaneously, persists for 4-7 days
and
disappears, and is known as fugitive
or Calabar swelling. The worm usually
causes
no serious problems, except when
passing through the orbital
conjunctiva

or the
nose bridge. The diagnosis is based
on symptoms, history of deer fly
bite and
presence of eosinophilia. Recovery
of worm from the conjunctiva is
confirmatory.
Treatment and control are the
same as those for onchocerciasis.
